IMAGING CASE REPORT
Gnathodiaphyseal dysplasiaTE Herman, MJ Siegel and K Sargar
Journal of Perinatology (2014) 34, 412–414; doi:10.1038/jp.2013.178
CASE PRESENTATIONA 3350 g infant was born at term to a 33-year old gravida 2, para 1mother by cesarean section due to the sonographic finding offractures and bowing of long bones in utero, raising the possibilityof osteogenesis imperfecta. However, amniocentesis had beenperformed and tissue was negative for collagen 1A1 or 1Amutations associated with osteogenesis imperfecta. After deliverythe child was in no respiratory distress and was discharged home.The child was noted to have bulging cheeks and swollen gingva.There were no cafe au lait spots or other skin lesions and thesclerae were white. A skeletal survey (Figure 1) and a head and
neck CT (Figure 2) were performed after referral to the geneticsclinic. Expansile lytic lesions of the mandible and maxilla werefound as well as osteopenic long bones. Biopsy of the mandibularlytic lesion was subsequently performed.
DISCUSSIONThe biopsy of the mandible demonstrated a fibro-osseous benignlesion with psammomatous bodies or calcospherites, but withoutgiant cells. A radical debulking procedure of the mandibularand maxillary lesions further defined the jaw lesion as a cemeno-ossifying fibrous lesion characteristic of autosomal dominantgnathodiaphyseal dysplasia (GDD). GDD is a osteodysplasiacharacterized by cemento-ossifying fibroma with psammomatousbodies in the mandible and maxilla, abnormal long bones with
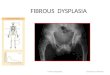
Figure 1. Skeletal-survey films. (a, b) Frontal and lateral views of chest and abdomen together. The bones are significantly osteopenic withcompression deformities of vertebral bodies at the thoracolumbar junction. (c) AP skull radiograph. No significant Wormian bones, poorlymineralized and with poorly delineated mandibular lucencies. (d, e) Frontal views of femurs, lateral right femur. There is lateral bowing of thefemurs with fractures at the apex of the bowing, best seen on the lateral view of the right femur.
Mallinckrodt Institute of Radiology, Washington University School of Medicine, St Louis, MO, USA. Correspondence: Dr TE Herman, Mallinckrodt Institute of Radiology,Washington University School of Medicine, 510 South Kingshighway Blvd., St Louis, MO 63110, USA.E-mail: [email protected] 17 September 2013; revised 4 November 2013; accepted 18 November 2013
Journal of Perinatology (2014) 34, 412–414& 2014 Nature America, Inc. All rights reserved 0743-8346/14
www.nature.com/jp

increased osseous fragility, anterior bowing particularly of thetibiae and fibulae and diaphyseal sclerosis with overall osteope-nia.1,2 GDD was first described in a large Japanese kindred3 andhas a characteristic autosomal dominant inheritance pattern. Thedisease was found to be linked to mutations in the transmem-brane protein 16E in the locus 11p14.3-15.1.3,4 Characteristicallythe disease has presented in early childhood with jaw lesions.These jaw lesions usually present with pain, swelling anddischarge. Mandibular and maxillary purulent osteomyelitis mayalso occur and teeth may fall out with poor healing after dentalextraction. However, fractures often following trivial trauma andbowing in these patients have developed subsequent to the jawlesions in the second decade of life between 12 and 14 years ofage, in contrast to our patient, who presented in utero with bowedbones. In one family with probable GDD, a high grade femoralosteogenic sarcoma developed at 12 years of age.5 The cognitivedevelopment of patients with GDD is normal.
The differential diagnoses of jaw and long-bone lesions isprimarily polyostotic fibrous dysplasia, with enicrinopathy, theMcCune–Albright syndrome. This was excluded in this case bythe pathologic appearance of the jaw lesions, the radiographicappearance of the long-bone lesions and the absence ofcharacteristic GNAS1 gene mutations.6 The jaw lesions can bedistinguished pathologically from those occurring in cherubism.Cherubism7,8 is a autosomal dominant disease with fibro-osseouslesions of the mandible. However, the lesions are not usuallypresent until 2 years of age and the condition has a benign course,often with resolution at puberty. It is not associated with long-bone lesions, or osseous fragility. The jaw lesions of cherubism,although not pathognomonic do contain characteristic giant cells.
The differential diagnosis of bowed long bones with osseousfragility and fractures after minimal trauma includes osteogenesisimperfecta and related conditions. These were the conditionsconsidered prenatally in this patient because of the bowed longbones. Osteogenesis imperfecta particularly types II and III presentwith osteopenia and perinatal or infantile fractures. However,because of the absence of detectable mutations in the precursorsof type I collagen, this diagnosis was essentially excluded.1 Thereare several rare genetic conditions also present as severe osseousfragility and recurrent fractures, several of which may havecraniofacial abnormalities. These conditions are Bruck syndrome,familial calvarial doughnut lesions with osteoporosis, osteoporosispseudoglioma syndrome and gnathodiaphyseal dysplasia. Brucksyndrome is an autosomal recessive condition with skeletalchanges resembling osteogenesis imperfecta and congenitalcontractures of large joints (arthrogryposis).9 However, this condi-tion is not associated with craniofacial abnormalities. Familialcalvarial doughnut lesions with osteoporosis is an autosomal
dominant condition in which features of bone fragility likeosteogenesis imperfecta occur, and are associated with scleroticround lesions of the calvaria, elevated alkaline phosphatase anddental caries. Several of these patients have been reported to havemandibular fibrous dysplasia.10 Osteoporosis pseudogliomasyndrome is an autosomal recessive condition often confusedwith osteogenesis imperfecta but is associated with a progressiveretinal dysplasia leading to blindness and phthisis bulbi.11
Figure 2. Axial CT scans of the facial bones. (a) Maxilla, (b) mandible. Expansile lytic lesions of the mandible and the maxilla.
Figure 3. Frontal radiographs lower extremities. Midfemoral healingfractures are present, now internally fixed by the Fassier–Duval nails.In the distal tibial metaphyses sclerotic bands are seen from theongoing pamidronate therapy.
Gnathodiaphyseal dysplasiaTE Herman et al
413
& 2014 Nature America, Inc. Journal of Perinatology (2014), 412 – 414

Additional ocular findings may include microcornea, clouding ofthe cornea and lens and iris–lens adhesions.4
In the patient reported here with genetically proven GDD, thechild was treated with pamidronate due to the early onset offractures. However, due to the persistent femoral fractures, thepatient at 23 months of age had placement of Fassier–Duvalmedullary rods for stabilization (Figure 3). In addition, the patienthas had two subsequent mandibular debulking proceduresperformed with some difficulty due to his difficult endotrachealintubation, stridor and excessive oral secretions.
CONFLICT OF INTERESTThe authors declare no conflict of interest.
REFERENCES1 Tsutsumi S, Kamata N, Vokes TJ, Maruoka Y, Nakakuki K, Enomoto S et al. The
novel gene encoding aputative transmembrane protine is mutated in gnatho-diaphyseal dysplasia (GDD). Am J Hum Genet 2004; 74: 1255–1261.
2 Ahluwalia J, Ly JQ, Norman E, Costello RF, Beall DP. Gnathodiaphyseal dysplasia.Clin Imaging 2007; 31: 67–69.
3 Tsutsumi S, Kamata N, Maruoka Y, Ando M, Tezuka O, Enomoto S et al. Autosomaldominant gnathodiaphyseal dysplasia maps to chromosome 11p14.3-15.1. J Boneand Miner Res 2003; 18: 413–418.
4 Roginsky VV, Ivanov AL, Khonsari Rh. Recurrent gnathodiaphyseal dysplasia in twoRussian Brothers. Int J Oral Maxillo fac Surg 2010; 39: 397–401.
5 Rossbach HC, Letson D, Lacson A, Ruas E, Salazar P. Familial gigantiformcementoma with brittle bone disease: pathologic fractures and osteosarcoma.Pediatr Blood Cancer 2005; 44: 3490–3496.
6 Riminucci M, Collins MT, Corsi A, Boyde A, Murphye MD, Wientroub S et al.Gnathodiaphyseal dysplasia: a syndrome of fibro-osseous lesions of jaw bones,bone fragility and long bone bowing. J Bone Miner Res 2001; 16: 1710–1718.
7 Kumar R, Madewell JE, Lindell MM, Swischuk LE. Fibrous lesions of bones.RadioGraphics 1990; 10: 237–256.
8 Penarrocha M, Bonet J, Minguez JM, Bagan JV, Vera F, Minguez I. Cherubism: aclinical, radiographic and histopathologic comparison of 7 cases. J Oral MaxillofacSurgy 2006; 64: 924–930.
9 Ha-Vinh R, Alanay Y, Bank R, Campos-Xavier A, Zankl A, Superti-Furga A et al.Phenotpyic and molecular characterization of Bruck syndrome caused by arecessive mutation in PLOD2. Am J Med Genet A 2004; 131A: 115–120.
10 Jaakkola E, Laine CM, Mayranpaa MK, Falck A, Ignatius J, Makitie O. Calvarialdoughnut lesions and osteoporosis: a new 3-generation family and review.Am J Med Genet 2009; 149: 2371–2377.
11 Tuysuz B, Bursali A, Alp Z, Suyugul N, Laine CM, Makitie O. Osteoprosis-pseu-doglioma syndrome: three novel mutations in the LRP5 gene and response tobisphosonate therapy. Hormone Res Pediatr 2012; 77: 115–120.
Gnathodiaphyseal dysplasiaTE Herman et al
414
Journal of Perinatology (2014), 412 – 414 & 2014 Nature America, Inc.
Recommended