Impact of Novel Therapies In Multiple Myeloma
Jean-Luc Harousseau
Intergroupe Francophone du Myélome

Impact of novel agents in younger patients

VAD TD VD RD TAD PAD VTD
Summary of novel agent induction trials (randomized studies)
Post-inductionPost-transplant
≥ VGPR rates post-induction and post-transplant
Harousseau et al. ASH/ASCO symposium during ASH 2008Rajkumar et al. ASCO 2008 (Abstract 8504); ASH/ASCO symposium during ASH 2008
Lokhorst et al. Haematologica 2008;93:124–7Sonneveld et al. ASH 2008 (abstract 653); IMW (abstract 152) Cavo et al. ASH 2008 (abstract 158); IMW 2009 (abstract 451)
*Post-transplant data not available
15-16%
30-35%
39% 33% 45%62%
42%
44-50%45-55%
57%49%
71%
76%
*

IFM 2005-01Impact of achieving at least VGPR after
induction ≥ VGPR vs PR
β2 mic (3mg/L)
t(4;14) ± del (17p)
≥ VGPR vs PR
RR
1.54
1.32
1.44
p. Value
0.01
0.23
0.038
median
≥ VGPRN=117
41m
PRN=145
33m
PFS
p=0.0015

VAD vs Vel/Dex induction for t(4;14) patients OS
treatment VAD Vel/Dex pvalue (logrank)
Patients 106 107
0.0004Deaths 70 20
Median OS (years) [IC 95%]
2.87[1.76 ; 3.48]
---*[3.60 ; ---*]
Vel/Dex
VADp=.0004
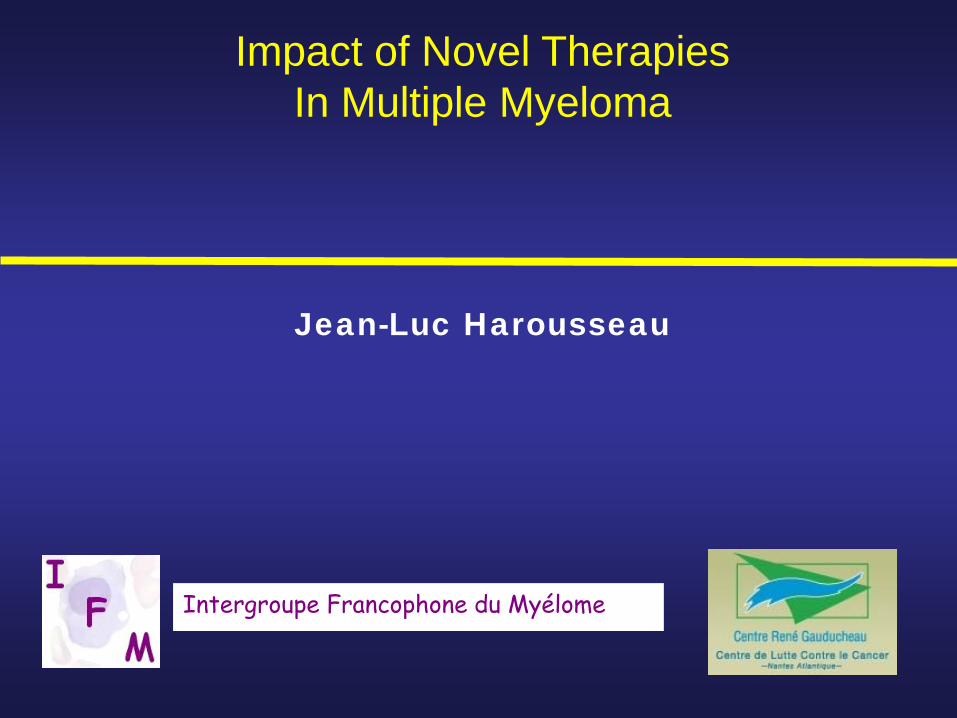
t(4;14) with BortezomibEFS of 507 patients treated with Vel/Dex induction
t(4 ;14) neg pos pvalue (logrank)
Patients 396 106
0.0178Relapses 141 43
Median EFS (years) [IC 95%]
2.90[2.74 ; 3.53]
2.32[1.49 ; 2.95]
p<.02
t(4;14) pos
t(4;14) neg
Avet-Loiseau et al., JCO online

Impact of Novel Agentsin the ASCT paradigm
Induction Treatment • Impact of CR/VGPR after Induction• Induction with BTZ appears to partly overcome poor prognosis
related to t(4,14)• The impact of 3-4 cycles of Len/Dex is less clear (no randomized
study)• Triple combinations appears more effective
( VCD,PAD, VTD…VRD) with VGPR rates up to50% before and 75% after ASCT
VTD is currently the best induction regimen andits neurotoxicity is reduced by lower doses (Moreau ASCO 2010)
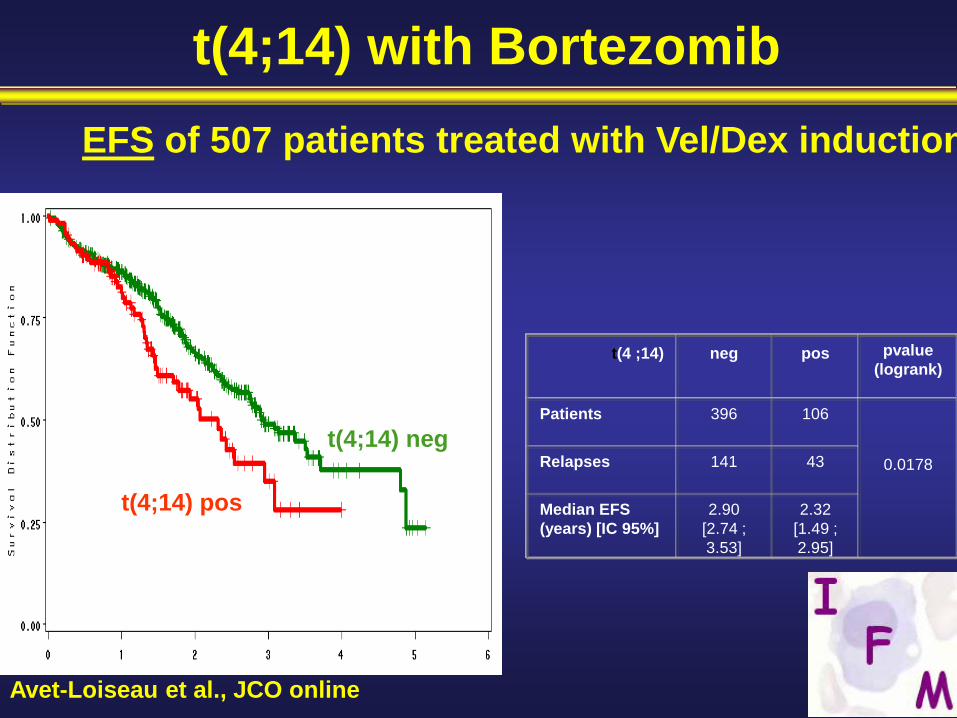
Stage 1-3, <70 yearsTherapy at least 2 cycles Stable Disease or better≤1 year from Rx initiation2 x 106 CD34 cells/kg
Placebo
Lenalidomide*10 mg/d with ↑↓ (5–15 mg)
RestagingDays 90–100
Registration
CALGB trial
CRPRSD
Stratification based on Diagnostic B2M and IMiD Use during Induction
Mel 200
ASCT
*
Randomization

Median Follow up is 12 monthsCALGB 100104, Nov 2009
Median TTP: Not yet reached
Median TTP 25.5 mo

IFM 2005-02: Study design
Arm A=Placebo(N=307)
until relapse
Patients < 65 years, with non-progressive disease, ≤ 6 months after ASCT in first line
Arm B=Lenalidomide
(N=307)10-15 mg/d until
relapsePrimary end-point: PFS.Secondary end-points: CR rate, TTP, OS, feasibility of long-term lenalidomide….
bConsolidation:Lenalidomide alone 25 mg/day p.o.
days 1-21 of every 28 days for 2 months
Randomization: stratified according to Beta-2m, del13, VGPR

IFM 2005-02 : PFS from randomization0.
000.
250.
500.
751.
00
0 6 12 18 24 30 36
Placebo Revlimid
p<10-7
P < 10-7

Impact of Novel Agentsin the ASCT paradigm
Best Intensive Approach
• Induction- 3 or 4 courses of VTD (RVD ?)
• Maintenance with Lenalidomide

Questions for the near future
• Will longer PFS with lenalidomide maintenance translate into longer OS ? Survival after relapse ?
• Optimal duration of maintenance ?- until progression- fixed duration- until best response (immunophenotypic remission?)
• Role of consolidation ?- maintenance with/without consolidation- novel agents or second TX ?

PRE POST p value
CR (IF -) 13 % 19 % <0.0001
≥ VGPR 58 % 68 % <0.0001
ATTAL ASCO 2010
IFM 2005 02 : Response during consolidation(n= 572)

Consolidation with VTD• Patients: (n=39) with ≥VGPR after ASCT• Treatment:
– 4 cycles VTD, started within 6 months• Bortezomib: 1.6 mg/m2, days 1, 8, 15, 22• Thalidomide: initial dose 50 mg/day, with increments up to 200 mg• Dex: 20 mg/day, days 1-4, 8-11, 15-18
• Results: at 32 month median follow up CR increased from 15% post-auto to 49% post-conso, MR from 3% to 18%
Ladetto et al. JCO 2010
• Six patients achieved molecular remission; none had clinical relapse
• 50 month PFS: 100% for patients with MR vs 62% for patients with no MR
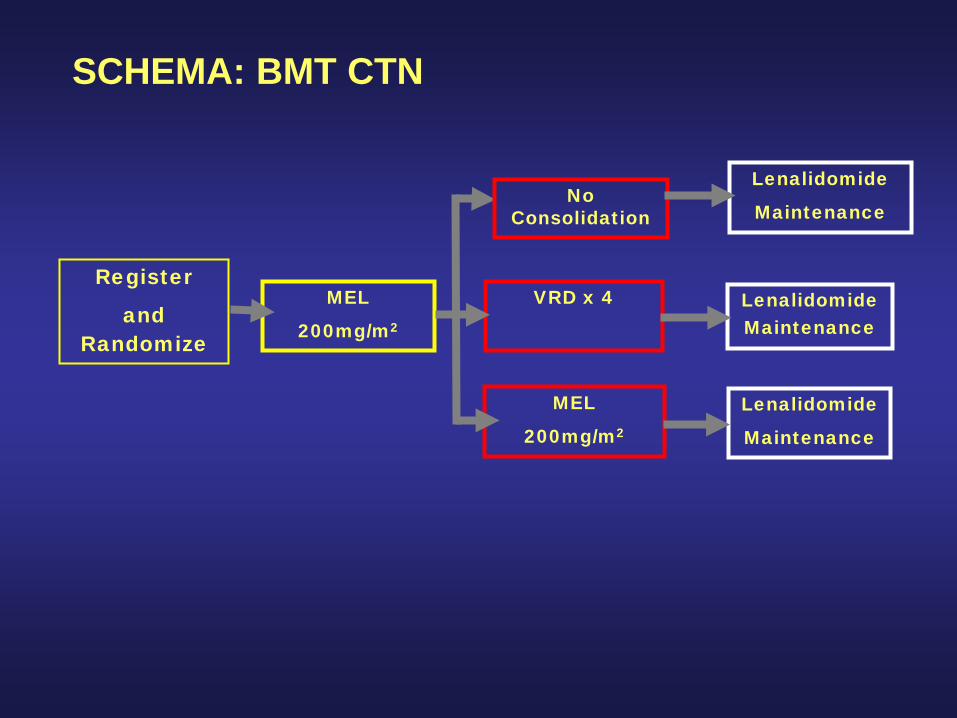
SCHEMA: BMT CTN
Register
and Randomize
MEL
200mg/m2
Lenalidomide
Maintenance
VRD x 4
MEL
200mg/m2
Lenalidomide Maintenance
Lenalidomide
Maintenance
No Consolidation

Questions for the near future
Key Question• With novel agents (MPT,MPV,Rd,RVD) it is
now possible to achieve up to 30%CR and up to 70% VGPR
• In published trials median PFS are comparable to those achieved in the past with ASCT (24-28 months)
• With prolonged treatment the CR/VGPR rate continues to increase (especially with Len which is well tolerated and administered orally)

Phase I/II study on RVD innewly diagnosed MM
• Overall response rate (66pts) 100%• CR 29 % (37 % for 35pts in the Phase II part)• CR+ VGPR 67% (74% in Phase II part)• 2-yr PFS 68% (no difference in 41 pts with ASCT) • 2-yr OS 95%
Up to eight 21-day cycles *
1 2 4 5 8 9 11 12 14 21
Lenalidomide
Bz Bz Bz Bz
Dex Dex Dex Dex
MPD Len 25mg Vel 1.3mg Dex 20mg in Phase II (35 pts)
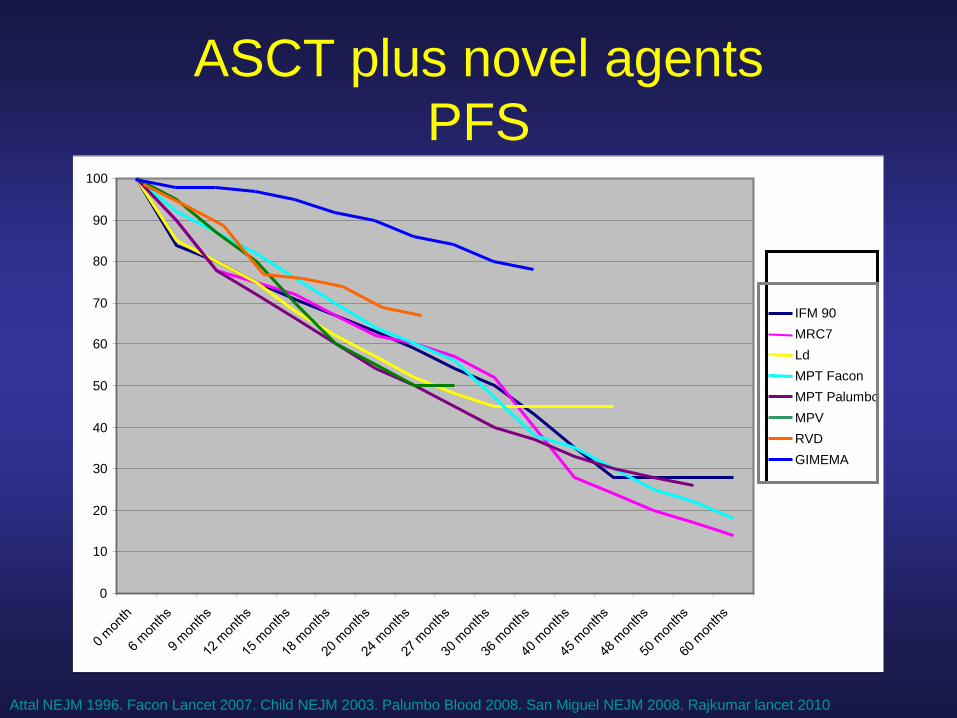
ASCT plus novel agentsPFS
0
10
20
30
40
50
60
70
80
90
100
IFM 90MRC7LdMPT FaconMPT PalumboMPVRVDGIMEMA
Attal NEJM 1996. Facon Lancet 2007. Child NEJM 2003. Palumbo Blood 2008. San Miguel NEJM 2008. Rajkumar lancet 2010

IFM/DFCI Trial
VRD x 3
SC collection
VRD x 5 Mel 200 + ASCT
VRD x 2
Rev 1 year Rev 1 year
(HDM + ASCT atrelapse)
Impact of novel agents in elderly patients

Frontline therapy in elderly patients
• MP is no longer the standard of care
• New standards- MPT > MP (1,2,3)
- MPV > MP (4)
- Len/dex > Len /dex (5)
• Maintenance therapy prolongs PFS- Low-dose lenalidomide (MM015 Palumbo ASH 2009)- Velcade-based combinations (Mateos ASH 2009, BoccadoroASCO 2010)
• Weekly velcade is better tolerated than bi-weeklyVMPT-VT vs VMP (Mateos ASH 2009, Boccadoro ASCO 2010)
Facon Lancet Oncol 2007, Palumbo Blood 2008, Hulin JCO 2009San Miguel NEJM 2008, Rajkumar Lancet Oncology 2010

MPR-R vs MPR47% reduced risk in PFS
MPR-RMPR
Median PFSNot reached13.2 months
HR 0.530 95% CI 0.350–0.802Log-rank p = 0.002
100
75
50
25
00 5
PFS duration (months)10 15 20 25 30
Patie
nts
with
out e
vent
(%)
Number at riskMPR-R 152 115 70 36 11 2 1MPR 153 122 78 20 5 1 1 Palumbo A, et al. Blood. 2009;114:[abstract 613]; updated data presented at ASH 2009.

VMPT-VT vs VMP
VMP VMPT-VT P-value
Nb of pts 257 254
Med age 71 71
CR 24% 38% 0.008
CR+VGPR 50% 59% 0.03
3-yr PFS 40% 54% 0.006
3-yr OS 84% 86% 0.6

Frontline therapy in elderly patients
• MP is no longer the standard of care
• New standards- MPT > MP (1,2,3)
- MPV > MP (4)
- Len/dex > Len /dex (5)
• Maintenance therapy prolongs PFS- Low-dose lenalidomide (MM015 Palumbo ASH 2009)- Velcade-based combinations (Mateos ASH 2009, BoccadoroASCO 2010)

Questions for the near future
- Will better PFS obtained with maintenance translate into longer OS ?
- Is maintenance necessary after all induction treatments (MPT, MPV, Ld) ?
- Optimal duration of maintenance ?- Role of alkylating agents
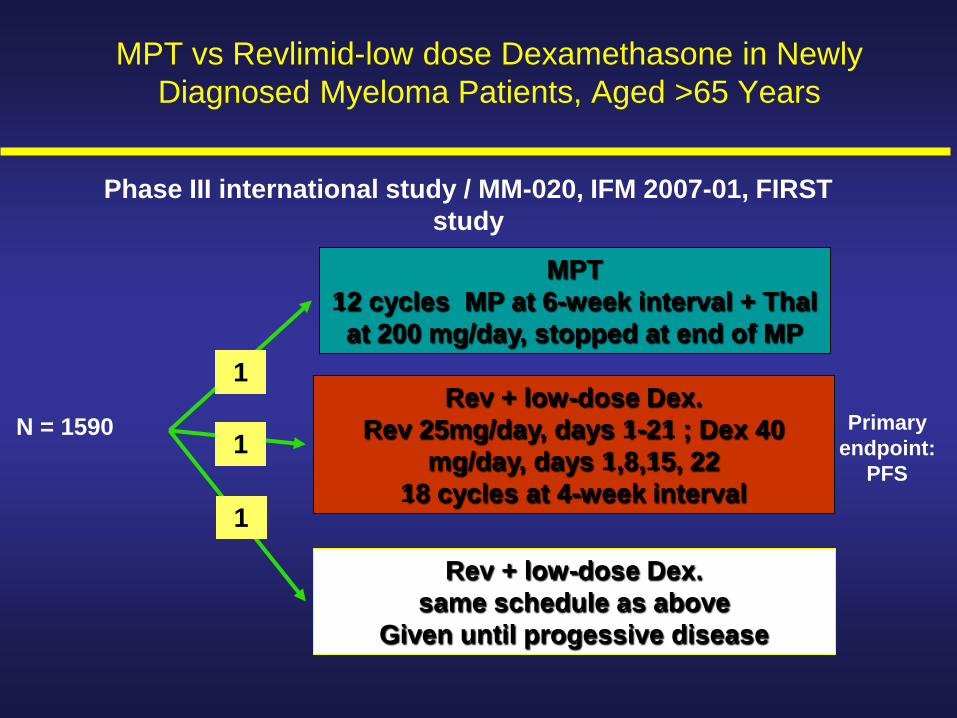
MPT 12 cycles MP at 6-week interval + Thal at 200 mg/day, stopped at end of MP
Rev + low-dose Dex.Rev 25mg/day, days 1-21 ; Dex 40
mg/day, days 1,8,15, 2218 cycles at 4-week interval
Rev + low-dose Dex.same schedule as above
Given until progessive disease
N = 1590 Primary endpoint:
PFS
1
1
1
MPT vs Revlimid-low dose Dexamethasone in Newly Diagnosed Myeloma Patients, Aged >65 Years
Phase III international study / MM-020, IFM 2007-01, FIRST study
General Questions
1) Role of novel agents in poor-risk cytogenetics

General Questions
1 Role of novel agents in poor-risk cytogenetics2 Which level of CR is needed to achieve long-term
remission?

78726660544842363024181260
1,0
,9
,8
,7
,6
,5
,4
,3
,2
,1
0,0
Impact of immunophenotypingat 3 months post-ASCTR
elap
se-fr
ee s
urvi
val
— <0.01% MM-PC
— ≥ 1% MM-PC
Months from immunophenotypical analysis
Updated Paiva et al Blood 2008
RFS
p=0.0001
40m
23m
— 0.01% to 1% MM-PC NR

General questions
1 Role of novel agents in poor-risk cytogenetics2 Which level of CR is needed to achieve long-term
remission?3 Which treatment at relapse when novel agents have
been used upfront ?

Pomalidomide
Lenalidomide
NNHO O
O
NH2
Structurally similar but functionally different, both qualitatively and quantitatively
NN
O
O
O
O
Thalidomide Pomalidomide (CC-4047)
N
O
O
NH
O
O
NH2
Teo SK, et al. Drug Discov Today. 2005;10:107-14.

Phase II of Pom/Dex in patients refractory to Lenalidomide
• 35 patients - Median age 62 y - 15 pts with mSMART high-risk- Median number of prior Tt 6- 100% Len , 100% Btz , 77% SCT
• Best response- VGPR 5 (14%)- PR 6 (17%)- MR 8 (23%)
• Median PFS 8 months Lacy M ASCO 2010

Carfilzomib
Carfilzomib is the first in a new class of selective and irreversible proteasome inhibitors that are associated with prolonged target suppression, improved antitumor activity
and low neurotoxicity
Tetrapeptide

0
50
100 CRVGPRPRMRSD
ORR:57%
ORR:18%
ORR:35.5%
AllSubjects(N = 31)
BortezomibNaive
(N = 14)
BortezomibExposed(N = 17)
PDNE (TLS)
14%
29%
36%
14%
7%
6%
18%
18%
59%45%
26%
6.5%3%
10%
3%
6.5%
% o
f sub
ject
s
90% of responses occurred by the end of Cycle 2
Phase II study of Carfilzomib

0
50
100 CRVGPRPRMRSD
ORR:57%
ORR:18%
ORR:35.5%
AllSubjects(N = 31)
BortezomibNaive
(N = 14)
BortezomibExposed(N = 17)
PDNE (TLS)
14%
29%
36%
14%
7%
6%
18%
18%
59%45%
26%
6.5%3%
10%
3%
6.5%
% o
f sub
ject
s
90% of responses occurred by the end of Cycle 2
PX-171-004: Response Summary

37
Panobinostat + Bortezomib Best ResponseDose escalation B2207 study in Relapsed MM pts
Clinical benefit (≥ MR) in 13/17 at cohort 3 and 6 levelN
umbe
r of p
atie
nts
PAN mgBTZ mg/m2
101.0
20 1.0
201.3
301.3
251.3
201.3
PAN panobinostat; BTZ bortezomib
CR, IF-negative CR; VGPR, very good PR; PR, partial response; MR, minor response; SD, stable disease; PD, progress. disease; NA, no assessment
0123456789
10
Co.1 Co. 2 Co. 3 Co. 4 Co. 5 Co. 6
NAPDSDMRPRVGPRCR

Panobinostat + Bortezomib EfficacyResponses including in Bortezomib-Refractory Patients
0102030405060708090
100
All (n=47) BTZ refractory (n=15)
MR
PR
VGPR
CR
Res
pons
e ra
te (%
)

39
Total Patients (%)Lenalidomide-Naїve
Patients (%)
Total (intent to treat)
28 22
ORR (≥ PR) 23 (82) 21 (95)
CR 1 (4) 1 (5)
VGPR 7 (25) 6 (27)
PR15 (54) 14 (64)
SD 4 (14) 1 (5)
PD 1 (4) 0
Phase 1b Elotuzumab plus Len/dexLonial ASCO 2010

General questions
1 Role of novel agents in poor-risk cytogenetics2 Which level of CR is needed to achieve long-term
remission?3 Which treatment at relapse when novel agents have
been used upfront ?4 What is the best strategy ?
- all active agents upfront ?- sequential use of active agents ?

General Questions
SEARCHING FOR CURE …

General Questions
SEARCHING FOR CURE
… OR TREATING MM LIKE A CHRONIC DISEASE
General Questions
SEARCHING FOR CURE
… OR TREATING MM LIKE A CHRONIC DISEASE
The answer to this question may depend on your definition of cure !!
Recommended