Embed Size (px)
DESCRIPTION
Jean-Luc Harousseau, M.D., Professor of Hematology, Head, Dept. of Clinical Hematology, Director of the Cancer Center Rene Gauducheau, University of Nantes, France - Impact of Novel Therapies in the Management of Multiple Myeloma Presented at New Frontiers in the Management of Solid and Liquid Tumors hosted by the John Theurer Cancer Center at Hackensack University Medical Center. jtcancercenter.org/CME
Citation preview
Impact of Novel Therapies In Multiple Myeloma
Jean-Luc Harousseau
Intergroupe Francophone du Myélome

Impact of novel agents in younger patients

VAD TD VD RD TAD PAD VTD
Summary of novel agent induction trials (randomized studies)
Post-inductionPost-transplant
≥ VGPR rates post-induction and post-transplant
Harousseau et al. ASH/ASCO symposium during ASH 2008Rajkumar et al. ASCO 2008 (Abstract 8504); ASH/ASCO symposium during ASH 2008
Lokhorst et al. Haematologica 2008;93:124–7Sonneveld et al. ASH 2008 (abstract 653); IMW (abstract 152) Cavo et al. ASH 2008 (abstract 158); IMW 2009 (abstract 451)
*Post-transplant data not available
15-16%
30-35%
39% 33% 45%62%
42%
44-50%45-55%
57%49%
71%
76%
*

IFM 2005-01Impact of achieving at least VGPR after
induction ≥ VGPR vs PR
β2 mic (3mg/L)
t(4;14) ± del (17p)
≥ VGPR vs PR
RR
1.54
1.32
1.44
p. Value
0.01
0.23
0.038
median
≥ VGPRN=117
41m
PRN=145
33m
PFS
p=0.0015

VAD vs Vel/Dex induction for t(4;14) patients OS
treatment VAD Vel/Dex pvalue (logrank)
Patients 106 107
0.0004Deaths 70 20
Median OS (years) [IC 95%]
2.87[1.76 ; 3.48]
---*[3.60 ; ---*]
Vel/Dex
VADp=.0004
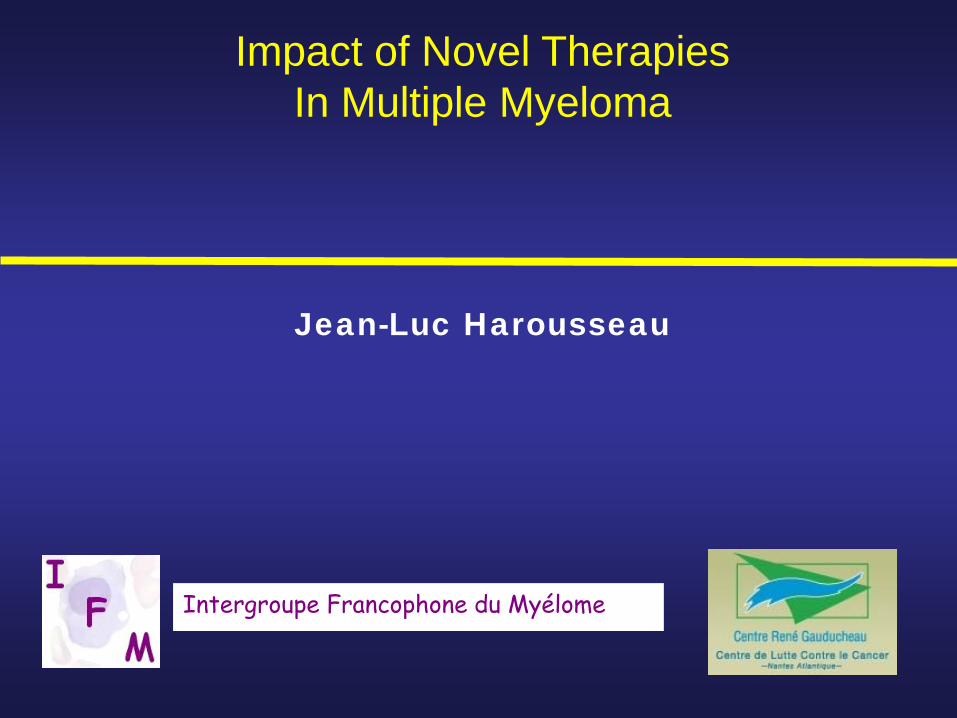
t(4;14) with BortezomibEFS of 507 patients treated with Vel/Dex induction
t(4 ;14) neg pos pvalue (logrank)
Patients 396 106
0.0178Relapses 141 43
Median EFS (years) [IC 95%]
2.90[2.74 ; 3.53]
2.32[1.49 ; 2.95]
p<.02
t(4;14) pos
t(4;14) neg
Avet-Loiseau et al., JCO online

Impact of Novel Agentsin the ASCT paradigm
Induction Treatment • Impact of CR/VGPR after Induction• Induction with BTZ appears to partly overcome poor prognosis
related to t(4,14)• The impact of 3-4 cycles of Len/Dex is less clear (no randomized
study)• Triple combinations appears more effective
( VCD,PAD, VTD…VRD) with VGPR rates up to50% before and 75% after ASCT
VTD is currently the best induction regimen andits neurotoxicity is reduced by lower doses (Moreau ASCO 2010)
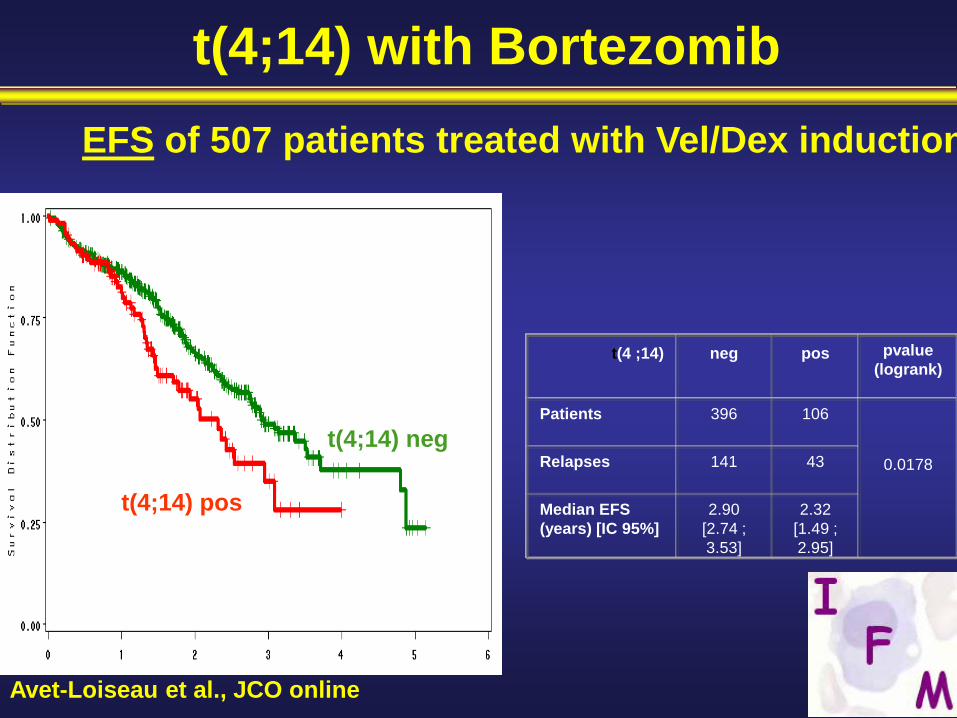
Stage 1-3, <70 yearsTherapy at least 2 cycles Stable Disease or better≤1 year from Rx initiation2 x 106 CD34 cells/kg
Placebo
Lenalidomide*10 mg/d with ↑↓ (5–15 mg)
RestagingDays 90–100
Registration
CALGB trial
CRPRSD
Stratification based on Diagnostic B2M and IMiD Use during Induction
Mel 200
ASCT
*
Randomization

Median Follow up is 12 monthsCALGB 100104, Nov 2009
Median TTP: Not yet reached
Median TTP 25.5 mo

IFM 2005-02: Study design
Arm A=Placebo(N=307)
until relapse
Patients < 65 years, with non-progressive disease, ≤ 6 months after ASCT in first line
Arm B=Lenalidomide
(N=307)10-15 mg/d until
relapsePrimary end-point: PFS.Secondary end-points: CR rate, TTP, OS, feasibility of long-term lenalidomide….
bConsolidation:Lenalidomide alone 25 mg/day p.o.
days 1-21 of every 28 days for 2 months
Randomization: stratified according to Beta-2m, del13, VGPR

IFM 2005-02 : PFS from randomization0.
000.
250.
500.
751.
00
0 6 12 18 24 30 36
Placebo Revlimid
p<10-7
P < 10-7

Impact of Novel Agentsin the ASCT paradigm
Best Intensive Approach
• Induction- 3 or 4 courses of VTD (RVD ?)
• Maintenance with Lenalidomide

Questions for the near future
• Will longer PFS with lenalidomide maintenance translate into longer OS ? Survival after relapse ?
• Optimal duration of maintenance ?- until progression- fixed duration- until best response (immunophenotypic remission?)
• Role of consolidation ?- maintenance with/without consolidation- novel agents or second TX ?

PRE POST p value
CR (IF -) 13 % 19 % <0.0001
≥ VGPR 58 % 68 % <0.0001
ATTAL ASCO 2010
IFM 2005 02 : Response during consolidation(n= 572)

Consolidation with VTD• Patients: (n=39) with ≥VGPR after ASCT• Treatment:
– 4 cycles VTD, started within 6 months• Bortezomib: 1.6 mg/m2, days 1, 8, 15, 22• Thalidomide: initial dose 50 mg/day, with increments up to 200 mg• Dex: 20 mg/day, days 1-4, 8-11, 15-18
• Results: at 32 month median follow up CR increased from 15% post-auto to 49% post-conso, MR from 3% to 18%
Ladetto et al. JCO 2010
• Six patients achieved molecular remission; none had clinical relapse
• 50 month PFS: 100% for patients with MR vs 62% for patients with no MR
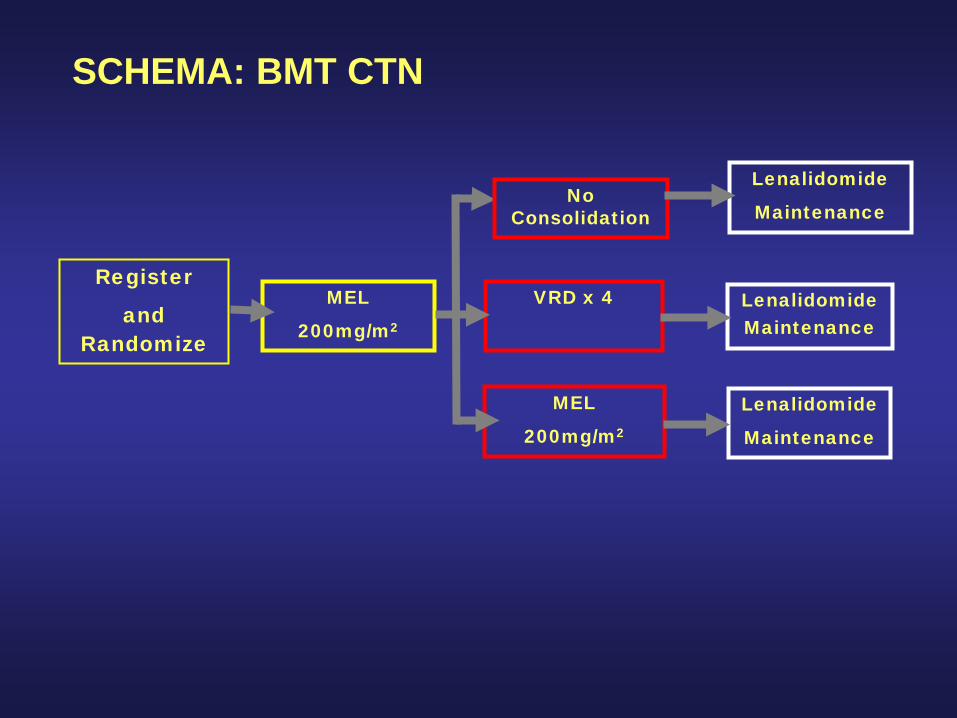
SCHEMA: BMT CTN
Register
and Randomize
MEL
200mg/m2
Lenalidomide
Maintenance
VRD x 4
MEL
200mg/m2
Lenalidomide Maintenance
Lenalidomide
Maintenance
No Consolidation

Questions for the near future
Key Question• With novel agents (MPT,MPV,Rd,RVD) it is
now possible to achieve up to 30%CR and up to 70% VGPR
• In published trials median PFS are comparable to those achieved in the past with ASCT (24-28 months)
• With prolonged treatment the CR/VGPR rate continues to increase (especially with Len which is well tolerated and administered orally)

Phase I/II study on RVD innewly diagnosed MM
• Overall response rate (66pts) 100%• CR 29 % (37 % for 35pts in the Phase II part)• CR+ VGPR 67% (74% in Phase II part)• 2-yr PFS 68% (no difference in 41 pts with ASCT) • 2-yr OS 95%
Up to eight 21-day cycles *
1 2 4 5 8 9 11 12 14 21
Lenalidomide
Bz Bz Bz Bz
Dex Dex Dex Dex
MPD Len 25mg Vel 1.3mg Dex 20mg in Phase II (35 pts)
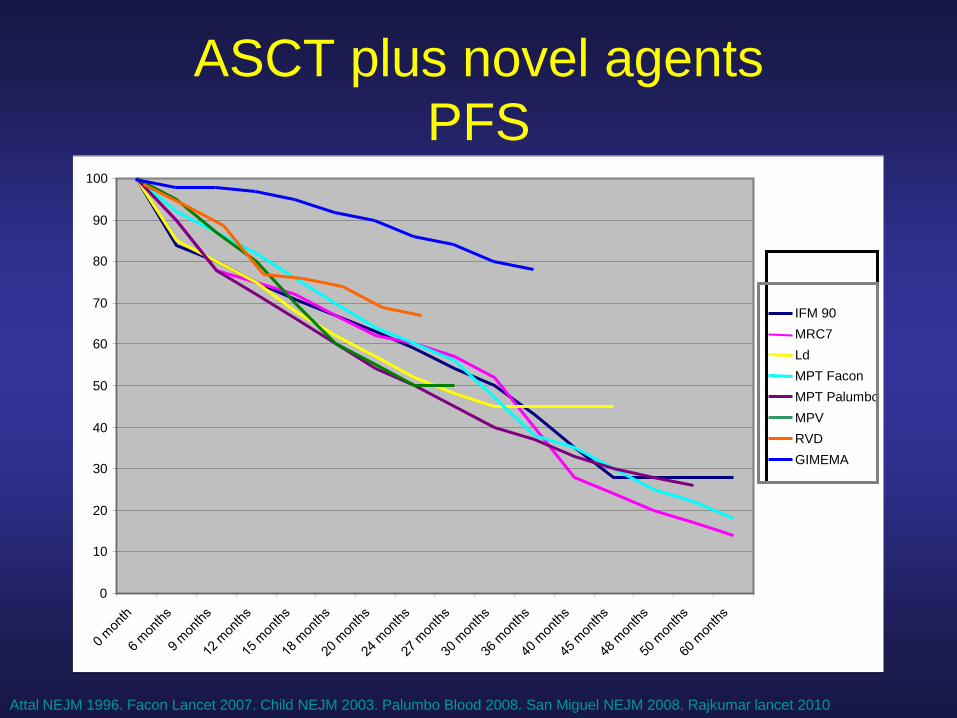
ASCT plus novel agentsPFS
0
10
20
30
40
50
60
70
80
90
100
IFM 90MRC7LdMPT FaconMPT PalumboMPVRVDGIMEMA
Attal NEJM 1996. Facon Lancet 2007. Child NEJM 2003. Palumbo Blood 2008. San Miguel NEJM 2008. Rajkumar lancet 2010

IFM/DFCI Trial
VRD x 3
SC collection
VRD x 5 Mel 200 + ASCT
VRD x 2
Rev 1 year Rev 1 year
(HDM + ASCT atrelapse)
Impact of novel agents in elderly patients

Frontline therapy in elderly patients
• MP is no longer the standard of care
• New standards- MPT > MP (1,2,3)
- MPV > MP (4)
- Len/dex > Len /dex (5)
• Maintenance therapy prolongs PFS- Low-dose lenalidomide (MM015 Palumbo ASH 2009)- Velcade-based combinations (Mateos ASH 2009, BoccadoroASCO 2010)
• Weekly velcade is better tolerated than bi-weeklyVMPT-VT vs VMP (Mateos ASH 2009, Boccadoro ASCO 2010)
Facon Lancet Oncol 2007, Palumbo Blood 2008, Hulin JCO 2009San Miguel NEJM 2008, Rajkumar Lancet Oncology 2010

MPR-R vs MPR47% reduced risk in PFS
MPR-RMPR
Median PFSNot reached13.2 months
HR 0.530 95% CI 0.350–0.802Log-rank p = 0.002
100
75
50
25
00 5
PFS duration (months)10 15 20 25 30
Patie
nts
with
out e
vent
(%)
Number at riskMPR-R 152 115 70 36 11 2 1MPR 153 122 78 20 5 1 1 Palumbo A, et al. Blood. 2009;114:[abstract 613]; updated data presented at ASH 2009.

VMPT-VT vs VMP
VMP VMPT-VT P-value
Nb of pts 257 254
Med age 71 71
CR 24% 38% 0.008
CR+VGPR 50% 59% 0.03
3-yr PFS 40% 54% 0.006
3-yr OS 84% 86% 0.6

Frontline therapy in elderly patients
• MP is no longer the standard of care
• New standards- MPT > MP (1,2,3)
- MPV > MP (4)
- Len/dex > Len /dex (5)
• Maintenance therapy prolongs PFS- Low-dose lenalidomide (MM015 Palumbo ASH 2009)- Velcade-based combinations (Mateos ASH 2009, BoccadoroASCO 2010)

Questions for the near future
- Will better PFS obtained with maintenance translate into longer OS ?
- Is maintenance necessary after all induction treatments (MPT, MPV, Ld) ?
- Optimal duration of maintenance ?- Role of alkylating agents
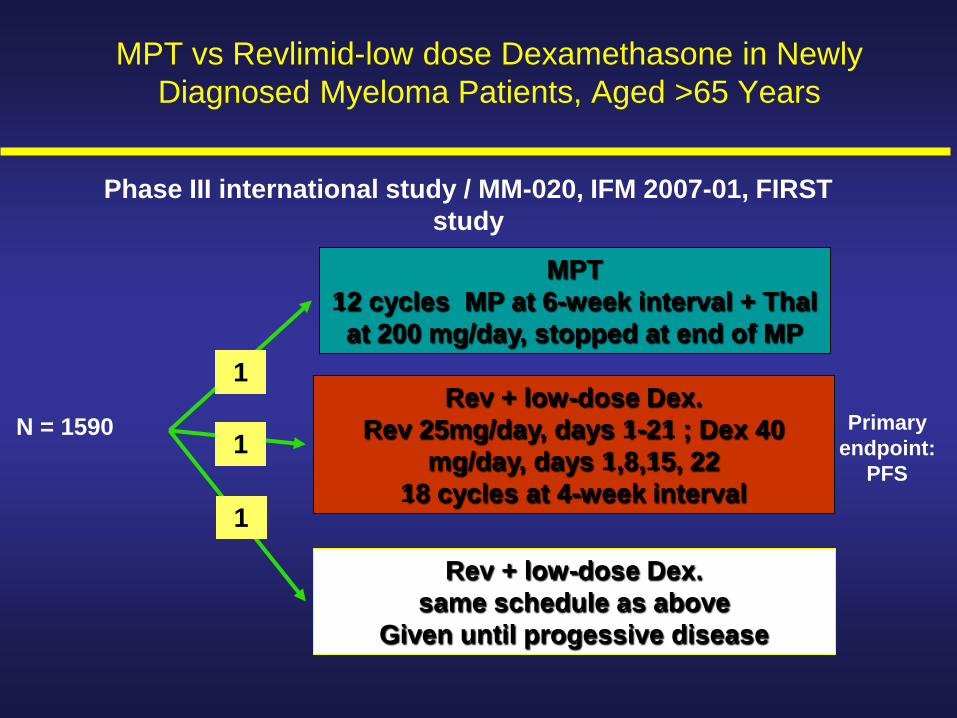
MPT 12 cycles MP at 6-week interval + Thal at 200 mg/day, stopped at end of MP
Rev + low-dose Dex.Rev 25mg/day, days 1-21 ; Dex 40
mg/day, days 1,8,15, 2218 cycles at 4-week interval
Rev + low-dose Dex.same schedule as above
Given until progessive disease
N = 1590 Primary endpoint:
PFS
1
1
1
MPT vs Revlimid-low dose Dexamethasone in Newly Diagnosed Myeloma Patients, Aged >65 Years
Phase III international study / MM-020, IFM 2007-01, FIRST study
General Questions
1) Role of novel agents in poor-risk cytogenetics

General Questions
1 Role of novel agents in poor-risk cytogenetics2 Which level of CR is needed to achieve long-term
remission?

78726660544842363024181260
1,0
,9
,8
,7
,6
,5
,4
,3
,2
,1
0,0
Impact of immunophenotypingat 3 months post-ASCTR
elap
se-fr
ee s
urvi
val
— <0.01% MM-PC
— ≥ 1% MM-PC
Months from immunophenotypical analysis
Updated Paiva et al Blood 2008
RFS
p=0.0001
40m
23m
— 0.01% to 1% MM-PC NR

General questions
1 Role of novel agents in poor-risk cytogenetics2 Which level of CR is needed to achieve long-term
remission?3 Which treatment at relapse when novel agents have
been used upfront ?

Pomalidomide
Lenalidomide
NNHO O
O
NH2
Structurally similar but functionally different, both qualitatively and quantitatively
NN
O
O
O
O
Thalidomide Pomalidomide (CC-4047)
N
O
O
NH
O
O
NH2
Teo SK, et al. Drug Discov Today. 2005;10:107-14.

Phase II of Pom/Dex in patients refractory to Lenalidomide
• 35 patients - Median age 62 y - 15 pts with mSMART high-risk- Median number of prior Tt 6- 100% Len , 100% Btz , 77% SCT
• Best response- VGPR 5 (14%)- PR 6 (17%)- MR 8 (23%)
• Median PFS 8 months Lacy M ASCO 2010

Carfilzomib
Carfilzomib is the first in a new class of selective and irreversible proteasome inhibitors that are associated with prolonged target suppression, improved antitumor activity
and low neurotoxicity
Tetrapeptide

0
50
100 CRVGPRPRMRSD
ORR:57%
ORR:18%
ORR:35.5%
AllSubjects(N = 31)
BortezomibNaive
(N = 14)
BortezomibExposed(N = 17)
PDNE (TLS)
14%
29%
36%
14%
7%
6%
18%
18%
59%45%
26%
6.5%3%
10%
3%
6.5%
% o
f sub
ject
s
90% of responses occurred by the end of Cycle 2
Phase II study of Carfilzomib

0
50
100 CRVGPRPRMRSD
ORR:57%
ORR:18%
ORR:35.5%
AllSubjects(N = 31)
BortezomibNaive
(N = 14)
BortezomibExposed(N = 17)
PDNE (TLS)
14%
29%
36%
14%
7%
6%
18%
18%
59%45%
26%
6.5%3%
10%
3%
6.5%
% o
f sub
ject
s
90% of responses occurred by the end of Cycle 2
PX-171-004: Response Summary

37
Panobinostat + Bortezomib Best ResponseDose escalation B2207 study in Relapsed MM pts
Clinical benefit (≥ MR) in 13/17 at cohort 3 and 6 levelN
umbe
r of p
atie
nts
PAN mgBTZ mg/m2
101.0
20 1.0
201.3
301.3
251.3
201.3
PAN panobinostat; BTZ bortezomib
CR, IF-negative CR; VGPR, very good PR; PR, partial response; MR, minor response; SD, stable disease; PD, progress. disease; NA, no assessment
0123456789
10
Co.1 Co. 2 Co. 3 Co. 4 Co. 5 Co. 6
NAPDSDMRPRVGPRCR

Panobinostat + Bortezomib EfficacyResponses including in Bortezomib-Refractory Patients
0102030405060708090
100
All (n=47) BTZ refractory (n=15)
MR
PR
VGPR
CR
Res
pons
e ra
te (%
)

39
Total Patients (%)Lenalidomide-Naїve
Patients (%)
Total (intent to treat)
28 22
ORR (≥ PR) 23 (82) 21 (95)
CR 1 (4) 1 (5)
VGPR 7 (25) 6 (27)
PR15 (54) 14 (64)
SD 4 (14) 1 (5)
PD 1 (4) 0
Phase 1b Elotuzumab plus Len/dexLonial ASCO 2010

General questions
1 Role of novel agents in poor-risk cytogenetics2 Which level of CR is needed to achieve long-term
remission?3 Which treatment at relapse when novel agents have
been used upfront ?4 What is the best strategy ?
- all active agents upfront ?- sequential use of active agents ?

General Questions
SEARCHING FOR CURE …

General Questions
SEARCHING FOR CURE
… OR TREATING MM LIKE A CHRONIC DISEASE
General Questions
SEARCHING FOR CURE
… OR TREATING MM LIKE A CHRONIC DISEASE
The answer to this question may depend on your definition of cure !!