American College of Rheumatology Guidelines for
Screening, Treatment, and Management of Lupus Nephritis
Dr. Amit Agrawal

Disease Burden
• 35% of adults with SLE have clinical evidence of nephritis at the time of diagnosis.
• 50–60% developing nephritis during the first 10 years of disease.
• Higher in men than in women.• Survival with SLE - 95% at 5 years • 92% at 10 years • Lupus nephritis reduces survival 88% at 10 years

Case definition
• Persistent proteinuria 0.5 gm per day• Or greater than 3+ by dipstickAnd/or• Cellular casts including red blood cells,
hemoglobin, granular, tubular, or mixed

• Spot urine protein/creatinine ratio of >0.5Active Urinary Sediment:• >5 RBCs/hpf• >5WBCs/hpf in the absence of infection• cellular casts limited to RBC or WBC casts

Renal Biopsy
• All patients with clinical evidence of active LN, previously untreated, undergo renal biopsy (unless strongly contraindicated) so that glomerular disease can be classified by current ISN/RPS classification
• Evaluated for activity and chronicity and for tubular and vascular changes



Principles of treatment
• Class I and Class II- do not require immunosuppressive treatment.
• Class III And Class IV aggressive therapy with glucocorticoids and immunosuppressive agents
• Class V when combined with class III or IV should be treated in the same manner as class III or IV
• Class VI requires preparation for renal replacement therapy rather than immunosuppression

• All SLE patients with nephritis be treated with a background HCQ unless there is a contraindication
Rationale:• Lower rates of Flare• Reduced renal damage• Less clotting events

• LN patients with proteinuria >0.5 gm per 24 hours should have blockade of the renin–angiotensin system, which drives intraglomerular pressure
Rationale:• Reduces proteinuria by 30%, and • Significantly delays doubling of serum
creatinine • Delays progression to end-stage renal disease

• Control of hypertension, with a target of <130/80 mm Hg
• Statin therapy be introduced in patients with low-density lipoprotein cholesterol >100 mg/dl


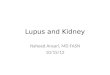
Class V Management



Class I LN (minimal-mesangial LN)
• Treatment as dictated by the extrarenal clinical manifestations of lupus
RATIONALE:• Class I LN has no clinical kidney
manifestations.• Class I LN is not associated with long-term
impairment of kidney function

Class II LN (mesangial-proliferative LN)
• Treat patients with class II LN and proteinuria <1 g/d as dictated by the extrarenal clinical manifestations of lupus. • Class II LN with proteinuria >3 g/d be treated
with corticosteroids or CNIs as described for MCD.
RATIONALE: There are no evidence-based data on the
treatment of class II LN.

Class III LN (focal LN) and class IV LN (diffuse LN)
• Initial therapy with corticosteroids , combined with either cyclophosphamide or MMF
• if patients have worsening LN (rising SCr, worsening proteinuria) during the first 3 months of treatment, a change be made to an alternative recommended initial therapy, or a repeat kidney biopsy be performed to guide further treatment

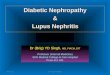
Regimens for initial therapy in class III/class IV LN


Other Initial Regimens
• Azathioprine• Cyclosporine• Combination of tacrolimus and MMF
(sometimes called ‘‘multitarget’’ therapy).

Important considerations
• Lifetime maximum of 36 g cyclophosphamide in patients with systemic lupus.
• The dose of cyclophosphamide should be decreased by 20%(CrCl 25–50 ml/min) or 30% (10–25 ml/min)

Choice of Initial Therapy
• In severe class III/IV LN, a cyclophosphamide-containing protocol for initial therapy may be preferred.
• In patients with less severe proliferative LN, an initial regimen not containing cyclophosphamide should be considered.

Class III LN and class IV LNmaintenance therapy
• Patients with class III and IV LN receive maintenance therapy with
• Azathioprine (1.5–2.5 mg/kg/d) or • MMF (1–2 g/d in divided doses), and • low-dose oral corticosteroids

• CNIs with low-dose cortico-steroids be used for maintenance therapy in patients who are intolerant of MMF and azathioprine.
• After complete remission is achieved, maintenance therapy be continued for at least 1 year before consideration is given to tapering the immunosuppression.

• If complete remission has not been achieved after 12 months of maintenance therapy, consider performing a repeat kidney biopsy before determining if a change in therapy is indicated.
• While maintenance therapy is being tapered, if kidney function deteriorates and/or proteinuria worsens, treatment be increased to the previous level of immunosuppression that controlled the LN.

Duration of Therapy
• There is no evidence to help determine the duration of maintenance therapy.
• The average duration of immunosuppression was 3.5 years in seven RCTs.
• Immunosuppressive therapy should usually be slowly tapered after patients have been in complete remission for a year.

• Immunosuppression should be continued for patients who achieve only a partial remission.
• The strategy of trying to convert a partial remission to a complete remission by increasing corticosteroids or using alternative immunosuppressive agents is not supported by evidence.

Predictors of Response to Treatment of Class III/IV LN
Predictors for not achieving remission:• SCr at the start of treatment• Magnitude of increase in SCr during relapse• Delay in starting therapy for more than 3
months after a clinical diagnosis of LN.• Severity of proteinuria• Failure to achieve complete remission a major
risk factor for kidney relapse.

Monitoring Therapy of Class III/IV LN
• Proteinuria • SCr• Urine sediment• C3 and C4,• Anti–double-stranded DNA antibodies

Class V LN (membranous LN)
• Patients with class V LN,normal kidney function, and non–nephrotic-range proteinuria be treated with antiproteinuric and antihypertensive medications, and only receive corticosteroids and immunosup-pressives as dictated by the extrarenal man-ifestations of systemic lupus.

• Pure class V LN and persistent nephrotic proteinuria be treated with corticosteroids plus an additional immunosuppressive agent:
• cyclophosphamide • CNI • MMF • Azathioprine

General treatment of LN
• All patients with LN of any class are treated with hydroxychloroquine(maximum daily dose of 6–6.5 mg/kg ideal body weight), unless they have a specific contraindication to this drug.

Class VI LN (advanced sclerosis LN)
• Treated with corticosteroids and immuno-suppressives only as dictated by the extrarenal manifestations of systemic lupus.

Relapse of LN
• Relapse of LN after complete or partial remission be treated with the initial therapy followed by the maintenance therapy that was effective in inducing the original remission
• If resuming the original therapy would put the patient at risk for excessive lifetime cyclophosphamide exposure, then we suggest a non cyclophosphamide based initial regimen be used.

• Consider a repeat kidney biopsy during relapse if there is suspicion that the histologic class of LN has changed, or there is uncertainty whether a rising SCr and/or worsening proteinuria represents disease activity or chronicity.


Treatment of resistant disease
• In patients with worsening SCr and/or protei-nuria after completing one of the initial treatment regimens, consider performing a repeat kidney biopsy to distinguish active LN from scarring.
• Treat patients with worsening SCr and/or proteinuria who continue to have active LN on biopsy with one of the alternative initial treat-ment regimens.

• Nonresponders who have failed more than one of the recommended initial regimens may be considered for treatment with rituximab, i.v.immunoglobulin, or CNIs.

Systemic lupus and thrombotic microangiopathy
• The antiphospholipid anti-body syndrome (APS) involving the kidney in systemic lupus patients, with or without LN,be treated by anticoagulation target INR 2–3.
• Patients with systemic lupus and thrombotic thrombocytopenic purpura (TTP) receive plasma exchange as for patients with TTP without systemic lupus.
Recommended