Embed Size (px)
Citation preview

Lupus Nephritis: Points To Remember
Mohamed A. Fouda, MD
Consultant Nephrologist
Urology & Nephrology CenterMansoura - Egypt
17 February 2017

Disease Burden
35% of adults with SLE have clinical evidence of nephritis at the time of diagnosis.
50–60% developing nephritis during the first 10 years of disease.
Survival with SLE - 95% at 5 years.
92% at 10 years.
Lupus nephritis reduces survival 88% at 10 years

Clinical Definitions


Indications For Renal Biopsy According to Several Committees Recommendations
Guideline recommendation
EULAR/ERA-EDTA ACR SEMI-SEN Dutch Working Party on
First renal biopsy
Proteinuriareproducible proteinuria
≥ 0.5 g/24 h
confirmed
proteinuria > 1.0
g/24 h
confirmed proteinuria
> 0.5 g/24 h
proteinuria > 0.5
g/24 h
Active urine sediment
(haematuria and/or
cellular casts)
May be considered yes yes no
Abnormal renal function May be considered yes yes with persistent elevation of serum creatinine > 30% and exclusion of other causes of renal impairment; with positive antiphospholipidantibodieswith extra-renal involvement/presence of anti-dsDNAantibodies/low C3, C4
Other proteinuria > 0.5 g/24 h plus haematuria (> 5 RBCs per hpf)proteinuria > 0.5 g/24 h pluscellular casts

Guideline recommendation
EULAR/ERA-EDTA ACR SEMI-SEN Dutch Working Party on
Repeat renal
biopsy
worsening or refractoriness to immunosuppressive or biological treatment (failure to decrease proteinuria by ≥50%, persistent proteinuria beyond 1 year and/or worsening of GFR)
at relapse
progression in histological class, change in biopsy chronicity and activity indices
no response totreatment
deteriorating renal function
additional or increased
proteinuria, nephrotic
syndrome or active urine
sediment, especially if the
first biopsy was in non-
proliferative class–
Increased serum
creatinine or unexplained
evolution
kidney failure– refractory
to immunosuppressive
treatment
uncertainty about the
level of activity/chronicity
of renal damage in
therapeutic decisions
suspected other
nephropathy
persistence of
proteinuria
after reaching a
partial
response,
despite optimal
supportive
treatment
including salt
restriction and
treatment with
ACEi or ARBs
failure to
respond (either
complete or
partial
response) at 12
months after
the start of the
initial induction
treatment

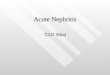
Discordance Between Biopsy and Clinical
Activity in Lupus Nephritis
SLE patients with first
clin. episode of LN
(n=69)
Induction
therapy
Complete
clinical
remission
Complete
histological
remission
33%persistent
histological activity
62%persistent
clinical activityBiopsy #1
Biopsy #2
Malvar et al. Nephrol Dial Transplant ,2015

Biopsy #1 :
Biopsy #2:
It is important to pay attention to the balance between
active (A) and chronic (c) lesions
Cellular crescents(50%), segmental sclerosis (5%),
normal (45%)
Fibrocellular crescents(5%), segmental sclerosis (40%),
global sclerosis (40%), normal (15%)
Class (A /C)
Class (A /C)

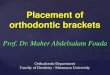
6 Month Clinical Response and Long-term Renal Function
SLE patients (n=69)at first presentation of LN ; all proliferative.
Induction: Steroids +MMF or CYC .
Complete renal response was defined as proteinuria >500 mg/d
and stable/improved SCr) .
CKD is defined as SCr < 1 mg /dl or proteinuria <500mg /d at last follow up .
100%
CRR39%
PRR/NRR61%
CRR 41%CKD14%ESRD11%FLARE 11%DIED 3.7%LOST 19%
CRR 61%CKD 26%ESRD 0%FLARE 2.4%DIED 0%LOST 10 %
Long- term kidney survival was similar whether a patient had a CRR or not at 6
months
Malvar et al, NDT, 2015

What Can You Do With these Models
An Example For CKD
From the CKD model we can generate a table to estimate how a patient will do
based on data collected after 12 months of treatment
Clinical settings Time to
future Outcome
Predicted to Develop CKD CI (%)
90% prot ; SCr =0.7 2 years 2% 4.2
90% prot ; SCr =0.7 6 years 9% 13.4
0% prot ; SCr =0.7 2 year 9% 13.5
0% prot ; SCr =0.7 6 years 31% 43.17
90% prot ; SCr =2 2 years 12% 18.5
90% prot ; SCr =2 6 years 31% 55.19
Potential application : In clinic you could match a patient to the closest clinical setting and estimate, after a given length of follow up, their chances of developing CKD

What are we trying to achieve ? Preservation of renal function and life, quality of life
and fertility
Requires:
• Rational targeted therapy related to pathophysiology which induces
remission and prevents flares
• Minimize treatment- related toxicities
• Improve the quality of life and survival
Predictors of good response/poor responseWhich are the best combinations of medications?
Get rid of steroids
Improve adherence
Get rid of steroids
Improve adherence
Facilitate good pregnancies

Lupus nephritis : Induction TherapyMMF 2-3 gm a day for 6 months
(preferred to CYC in african Americans
and Hispanics)
Plus
GC IV pulse x 3 days then prednisone
0.5 -1 mg/kg per day tapered after a few
weeks to lowest effective dose
(1 mg /kg/ day if cerscents seen)
Not ImprovedImproved
CYC (low or high)+
pulse GC then daily GC
MMF 1-2 gm /day
OR
AZA 2mg/kg/day + /-
low-dose daily GC
Not ImprovedImproved
Rituximab
Or
Calcineurin
inhibitors +GC
Maintenance
MMF 1-2 gm /day
OR
AZA 2 mg/kg/day
+/- low dose GC
6 mos
CYC
Plus
GC IV pulse x 3 days then prednisone
0.5 -1 mg/kg per day tapered after a few weeks
to lowest effective dose
(1 mg /kg/ day if cerscents seen)
Low-Dose CYC
500mg IV every 2 weeks x6
followed by maintenance
with oral MMF or
AZA(regimen for whites
with european background)
High-Dose CYC
500-1000mg/
BSA IV every
months x6
Improved
MMF 1-2 gm /day
OR
AZA 2mg/kg/day + /-
low-dose daily GC
MMF 2-3 gm /daily
for 6 months
+ pulse GC then
daily GC
Not Improved
OR
Not ImprovedImproved
Rituximab
Or Calcineurin inhibitors
+GC
MaintenanceMMF 1-2 gm /day OR AZA 2
mg/kg/day +/- low dose

The International MMF vs IV
Cyclophosphamide Study (Appel et al 2009)
370 patients with lupus nephritis randomized to MMF vs IV CTX .
Mean dose of prednisone 26 mg/d.
Primary endpoint: decrease in urine protein/ creatinine ratio and stable or improving serum creatinine.
Secondary endpoint: complete renal remission, disease activity, safety.

The Most Interesting Result
only 8-9% in either group were in complete
remission at 24 weeks!
Appel et al J Am Soc Nephrol 2009

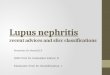
Remission Rates by Renal Criteria
No significant differences between groups in
complete remission or by individual criteria
Slide courtesy of G. Appel

The Lesson from Primary Membranous Nephropathy
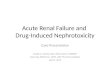
There is a lag between disappearance of the causative antibody
and resolution of proteinuria .
When antibody levels reach zero, there is still 2-3 g/day of
proteinuria .
This is compatible with residual structural deficits in the
absence of immunologic activity .
Beck and Salant, Kidney Int 2010

Lag Between Disappearance of Antibody and Resolution of
Proteinuria (Primary Membranous Nephropathy)
Beck and Salant , Kidney Int 2010

Lag Between Disappearance of Antibody &
Improvement In Proteinuria: Rituximab
Beck et al J Am Soc Nephrol 2011
Anti
PLA2R
Proteinuria

Probably the same Phenomenon in
Lupus Membranous
XWhatever
it is in lupus
membranous

The Toronto Cohort: It Takes a Long
Time for Proteinuria to Improve
Touma J Rheum 2014

Insert the j rheum editorial here
Bargman and Avila Casado J Rheum 2014
Moroni et al Semin Arthritis Rheum 2012
Pure membranous lupus

The Lag Time To Resolution Of Proteinuria
we shouldn’t be continuing intensive immunosuppression
or escalating immunosuppression for ongoing proteinuria
or hematuria
Be wise, wait and see

Lupus Nephritis: When to Change Treatment
(KDIGO)
2 important points about waiting, buried in the rationale:

CAN WE TREAT WITHOUT
STEROIDS ?

The Importance of Corticosteroids
the steroid brings the
disease under control the
fastest .

Prednisone
Patients need urgent prednisone the most in order to turn off the
inflammation.
1 mg/kg X at least 6 weeks, with a s-l-o-w taper.
IV pulse steroid is indicated for organ-threatening emergencies
(rapidly progressive renal failure, cerebritis, pulmonary
hemorrhage)

The Importance of Corticosteroids
this isn’t asthma.
for severe lupus nephritis, the current standard of therapy is
prednisone 1 mg/kg body weight X 6 weeks minimum.
slow taper (to zero or to some lower dose) over 12 months or
longer
some patients may never get off steroids.
nephrologists are more focused on the “second agent” than the
corticosteroid

KDIGO Guidelines For Treatment of
Lupus Nephritis
Kidney Int Suppl 2012; 2: 143-153

Treatment of Diffuse Proliferative Lupus Nephritis with
Prednisone and Combined Prednisone and
Cyclophosphamide
50 patients with diffuse proliferative lupus nephritis .
randomized to prednisone alone or with daily oral
cyclophosphamide
Donadio et al, N England J Med 1978
prednisone
prednisone + CTX

Treatment of Diffuse Proliferative Lupus Nephritis with
Prednisone and Combined Prednisone and
Cyclophosphamide
Results
Both groups had same degree of improvement over first 6 months
Prednisone-only group had more renal relapses.
The addition of a second agent did not improve the initial
response rate.
Patients with advanced disease ended up on dialysis with either
therapy.
Donadio et al, N England J Med 1978

Donadio et al: What it Teaches Us Three
Decades Later
it’s the corticosteroid that works the fastest.
But don’t be lulled into leaving them just on corticosteroids:
corticosteroids alone is associated with more relapses and
worse renal outcome.
use a second agent, but you don’t have to do this right away.
patients with a lot of established renal damage don’t do well,
no matter what to give more

CAN WE TREAT WITHOUT
STEROIDS ?

Imperial College London lupus Centre
Rituxilup Protocol
Single centre cohort study, the rituxilup regimen;
NO ORAL STEROIDS
From 1 January 2006 until 1 November 2010, all patients at imperial college healthcare NHTS trust lupus centre with biopsy-proven active ISN/RPS class III, IV or class V LN if not already on steroids and do not have RPGN/cerebral lupus.
2 doses of rituximab (1g) and methly prednisolone(500 mg) on days 1 and 15
Maintenance treatment of mycophenolate mofetil (500 mg BD-titrated up to level(1.4- 2.4 mg/L).

Time to Remission and Relapse
Condon MB et al Ann Rheum Dis.2013; 1280- 1285

Summary of 5 years Rituxilup Cohort Data
Rituxilup regimen leads to remission, preservation of renal function & minimal oral steroid use in significant proportion of patients.
Relapses were only in patients with class IV or V disease, majority responded to retreatment, again with no oral steroids.
Flares were not uncommon but did not predict poor outcomes.
Poor outcomes were predicted by baseline creatinine <120µmol/or a failure to achieve PR at 6 months.
The minimal use of oral steroids in the majority would be expected to have long term benefits in terms of CVS risk and reduced side effects.
The Rituxilup trial (NCT01773616) will address efficacy & safety in an international multicentre RCT .


Randomized controlled trials of rituximab in SLENo. and
ethnicity
Study duration
and comparator
Inclusion Main results Adverse events
EXPLORE
R (phase
III)
257 (42% Asians,
Hispanics or
Africans)
52 weeks RTX
(1 g × 2) versus PBO
in addition to steroid
and background
therapies
≥ 1 BILAG A
(except severe
or organ-
threatening
disease) or ≥ 2
BILAG B score
Major clinical
response at week
52 (RTX vs.
PBO: 12% vs.
16%); partial
clinical response
(RTX vs. PBO:
17% vs. 13%)
(differences NS)
AEs, SAEs and
infusion reactions
similar between
RTX and PBO
LUNAR
(phase III)
144 (69% Asians,
Hispanics or
Africans)
RTX (1 g × 2) versus
PBO in addition to
high-dose steroid and
MMF (3 g/day)
Biopsy-
confirmed
active class
III/IV lupus
nephritis with
urine P/Cr ratio
> 1.0
Complete renal
response at week
52 (RTX vs.
PBO: 26% vs.
31%); partial
renal response
(RTX vs. PBO:
31% vs. 15%)
(differences NS)
AEs, SAEs, rates
of infusion reaction
and infection
similar between
RTX and PBO;
neutropenia,
leukopenia and
hypotension more
common with RTX
AE, adverse events; BILAG, British Isles Lupus Assessment Group; MMF, mycophenolate mofetil; NS, not
significant; PBO, placebo;; P/Cr, protein to creatinine ratio; RTX, rituximab; SAE, serious adverse events;
SLE, systemic lupus erythematosus.

The Second Agent
Too much attention is focussed on this.
MMF may be better than azathioprine, but if the patient is
intolerant of MMF, then azathioprine or daily oral
cyclphosphamide may be reasonable second choices.
If the patient is likely to become pregnant, or can’t afford MMF,
azathioprine is a good second choice.
Some save IV cyclophosphamide for patients they don’t trust to
take tablets at home.
Some don’t give IV cyclophosphamide to patients with
decreased GFR because it is too unpredictable.

Low Dose versus High Dose Cyclophosphamide
• high dose (monthly pulses X 6)
then quarterly pulses X 2
versus
low dose (500 mg q2weeks X
6) followed by azathioprine
• same renal outcome
• twice as many infections in the
high-dose group
• did AZA do all the work in the
low-dose group?
Houssiau et al Arthr Rheum 2002
(AZA)

Multi drug induction regimens may help
CORTISTEROIDS Tacrolimus MMF
Cortisteroids IV cyclophosphamic

Important considerations
Lifetime maximum of 36 g cyclophosphamide in patients with systemic lupus.
The dose of cyclophosphamide should be decreased by 20%(CrCl 25–50 ml/min) or 30% (10–25 ml/min).
CNIs with low-dose cortico-steroids be used for maintenance therapy in patients who are intolerant of MMF and azathioprine.
After complete remission is achieved, maintenance therapy be continued for at least 1 year before consideration is given to tapering the immunosuppression

If complete remission has not been achieved after 12
months of maintenance therapy, consider performing a
repeat kidney biopsy before determining if a change in
therapy is indicated.
While maintenance therapy is being tapered, if kidney
function deteriorates and/or proteinuria worsens,
treatment be increased to the previous level of
immunosuppression that controlled the LN.

Systemic Lupus &Thrombotic
Microangiopathy
The antiphospholipid anti-body syndrome (APS)
involving the kidney in systemic lupus patients, with
or without LN,be treated by anticoagulation; target
INR 2–3.
Patients with systemic lupus and thrombotic
thrombocytopenic purpura (TTP) receive plasma
exchange as for patients with TTP without systemic
lupus.

LN patients with proteinuria >0.5 gm per 24 hours should have blockade of the renin–angiotensin system, which drives intraglomerular pressure.
Rationale: Reduces proteinuria by 30%, and
Significantly delays doubling of serum creatinine.
Delays progression to end-stage renal disease.
Control of hypertension, with a target of <130/80 mm Hg
Statin therapy be introduced in patients with low-density lipoprotein cholesterol >100 mg/dl

Antimalarial Drugs
The probability of a patient with lupus receiving an
antimalarial is decreased (odds ratio 0.51) if their primary
lupus doctor is a nephrologist instead of a rheumatologist.
Randomized, controlled trials and other studies have shown
that use of antimalarials is associated with:
Decreased frequency of lupus flares, including renal flares
Diminished damage accrual
Safe in pregnancy
Decreased thrombosis risk

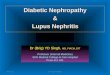
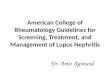
Antimalarial Use Associates with Protection
from Atherosclerosis in Lupus Patients
Study of carotid intima-medial
thickness in long-term lupus
patients
The absence of plaque was
associated with
More prednisone use (!)
Hydroxychoroquine
No
plaque
plaque P value
% using
prednisone93% 85% .09
Avg daily
dose12 mg 7 mg .002
% using
antimalarial82% 63% .003
Roman et al N Engl J Med 2003

Anti-Malarials
What you need to remember about
antimalarials:
• it’s all good
– reduced flares, including renal
flares
– damage index, including vascular
disease
– reduced thrombosis
– may also apply to lupus
membranous
chloroquine
no chloroquine
Okpechi et al Nephrol Dial Transplant 2012
Outcome of Membranous Lupus

For further information…
Nature Reviews Nephrology 2011

How Do the Guidelines Define Resistance?
ACR: give it 6 months
If patient on CTX, change to MMF (or vice versa) and re-pulse
with corticosteroids.
Can consider rituximab (no consensus reached).
Not enthusiastic about calcineurin inhibitors.
EULAR: same as above

Resistant Lupus Nephritis
For increasing creatinine and/or proteinuria, a repeat renal
biopsy may help to distinguish from superimposed scarring
(ungraded).
If still active disease, consider an alternative agent (ungraded).
Consider use of IVIG, rituximab or calcineurin inhibitors (2D).

Lack of Remission is Associated with
Poor Renal Outcome
Reich Kidney Int 2011

One of the major causes for “nonresponse” is not addressed:
non-adherence to therapy:
Think of this if serology is not improving and hemoglobin is not
increasing.
Think of this if patient doesn’t look cushingoid .
Think of this if patient can’t immediately tell you how many prednisone
tablets they take every day

What to Do About Non-Adherence
Diagnosis
Pill counts .
Calls to the pharmacy .
Quizzing the patient (but they
will lie).
Drug levels (MMF,
calcineurin inhibitors).
*Minimize the number of
pills*
Changing behaviour: I wish
I knew

What to Do About Non-Adherence
Patients don’t know that lupus is a potentially fatal disease
(unless you tell them).
If you prescribe prednisone and they develop acne, they may
just stop it .
Compared to cancer
Patients undergoing chemo know that their hair will fall out,
mucositis, etc. But it is life-saving therapy.
How many patients know this about lupus?

What to Do About Non-Adherence
Minimize the Number of Pills
22 year old, previously well, severe lupus nephritis.
The most important medicine they should be adherent to is prednisone +/- a second agent.
BUT they are also prescribed
proton pump inhibitor
co-trimoxazole for PJP prophylaxis
calcium and vitamin D
bisphosphonate
statin for increased lipids
ACE-inhibitor or ARB for “proteinuria”
approximately 24 tablets/day
Is it any surprise that they stop taking all their medicines?

Parenteral Therapy May Help
Examples: intravenous
methylprednisolone, cyclophosphamide,
rituximab + pulse steroid.
at least you know if the patient got the
drug (or didn’t show up)

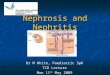
Mansoura Experience

This figure showed that renal survival of all lupus patients is 95% after 1 year, 86% after 5 years, 71% after 10 years and 60% after 15
years.

This curve demonstrated that There’s no difference in renal survival between male and female lupus nephritis patients (P value = 0.9)

Renal survival in relation to different histopathological classes of lupus nephritis

Renal survival of proliferative and non-proliferative lupus nephritis

Renal survival relative to different types of induction therapy among proliferative lupus nephritis patients

Renal survival in relation to the level of serum creatinine at the 1st
presentation

Renal survival in relation to the level of proteinuria at the 1st
presentation

Summary/ Suggestions
Apply end points after at least 12 months of treatment.
Evaluate by clinical response criteria that reflect long term,
preservation of kidney function
Add histologic response to clinical response criteria
Abandon the current complete and partial renal response paradigm may lead
to losing potentially useful drugs because criteria too restrictive
Verify histologic remission by repeat biopsy at 12 months (or a surrogate
marker of histology when available)
Assess damage accumulation- does a therapy reduce damage?

Conclusions: Four Important Points
About Lupus Nephritis
It takes much longer for resolution of proteinuria or hematuria than is
appreciated (and it may never resolve).
Corticosteroids (high dose and for a long time) and a second agent
remain the cornerstones of therapy till now.
Don’t forget to use antimalarial drugs.
The main cause of “resistant” lupus is that the patient isn’t taking
their medicine, and this is much more common than you think.

.