Medical and Surgical Nursing Review
The Respiratory System
Nurse Licensure Examination Review


Outline Of Review Concepts:Review of the relevant respiratory
anatomyReview of the relevant respiratory
physiologyThe respiratory assessmentCommon laboratory examinations

Outline Of Review Concepts:Review of the common respiratory
problems and the nursing managementReview of common respiratory diseases
Upper respiratory conditions Lower respiratory conditions

Respiratory Anatomy & Physiology
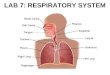
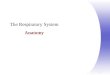
The respiratory system consists of two main parts - the upper and the lower tracts

Respiratory Anatomy & Physiology
The UPPER respiratory system consists of:
1. nose2. mouth3. pharynx4. larynx

Respiratory Anatomy & Physiology
The LOWER respiratory system consists of:
1. Trachea2. Bronchus3. Bronchioles4. Respiratory unit

Upper Respiratory Tract

The NoseThis is the first part of the upper
respiratory system that contains nasal bones and cartilages
There are numerous hairs called vibrissae
There are numerous superficial blood vessels in the nasal mucosa

The NoseThe functions of the nose are:1. To filter the air2. To humidify the air3. To aid in phonation4. Olfaction

The PharynxThe pharynx is a musculo -
membranous tube that is composed of three parts
1. Nasopharynx2. Oropharynx3. Laryngopharynx

The PharynxThe pharynx functions :1. As passageway for both air and foods
(in the oropharynx)2. To protect the lower airway

The LarynxAlso called the voice boxMade of cartilage and membranes and
connects the pharynx to the trachea

The LarynxFunctions of the larynx:1. Vocalization2. Keeps the patency of the upper
airway3. Protects the lower airway

The Paranasal sinusesThese are four paired bony cavities that
are lined with nasal mucosa and ciliated pseudostratified columnar epithelium
Named after their location - frontal, ethmoidal, sphenoidal and maxillary

The Paranasal sinusesThe function of the sinuses:
Resonating chambers in speech

The Lower Respiratory System
The lower respiratory system consists of1. Trachea2. Main bronchus3. Bronchial tree4. Lungs- 3R/ 2LThe trachea to the terminal bronchioles
is called the conducting airwayThe respiratory bronchioles to the
alveoli is called the respiratory acinus

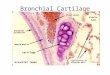
The TracheaA cartilaginous tube measures 10-12
centimetersComposed of about 20 C-shaped
cartilages, incomplete posteriorly

The TracheaThe function of the trachea is to conduct
air towards the lungsThe mucosa is lined up with mucus and
cilia to trap particles and carry them towards the upper airway

The BronchusThe right and left primary bronchi begin
at the carinaThe function is for air passage

The Primary Bronchus RIGHT BRONCHUS
Wider Shorter More Vertical
LEFT BRONCHUS
Narrower Longer More horizontal

The BronchiolesThe primary bronchus further divides
into secondary, then tertiary then into bronchioles
The terminal bronchiole is the last part of the conducting airway

The Respiratory AcinusThe respiratory acinus is the chief
respiratory unit It consists of 1. Respiratory bronchiole2. Alveolar duct3. alveolar sac

The Respiratory AcinusThe respiratory acinus is the chief
respiratory unitThe function of the respiratory acinus is
gas exchange through the respiratory membrane

The Respiratory AcinusThe respiratory membrane is composed
of two epithelial cells1.The type 1 pneumocyte - most
abundant, thin and flat. This is where gas exchange occurs
2. The type 2 pneumocyte - secretes the lung surfactant

The Respiratory AcinusA type III pneomocyte is just the
macrophage that ingests foreign material and acts as an important defense mechanism

Accessory Structures
The PLEURAEpithelial serous membrane lining the
lung parenchymaComposed of two parts- the visceral
and parietal pleuraeThe space in between is the pleural
space containing a minute amount of fluid for lubrication

Accessory Structures
The Thoracic cavityThe chest wall composed of the
sternum and the rib cageThe cavity is separated by the
diaphragm, the most important respiratory muscle

Accessory Structures
The MediastinumThe space between the lungs, which
includes the heart and pericardium, the aorta and the vena cavae.

GENERAL FUNCTIONS OF THE Respiratory System
Gas exchange through ventilation, external respiration and cellular respiration
Oxygen and carbon dioxide transport

The Assessment
HISTORYReason for seeking carePresent illnessPrevious illnessFamily historySocial history

The Assessment
PHYSICAL EXAMINATIONSkin- cyanosis, pallorNail clubbingCough and sputum production Inspect - palpate - percuss - auscultate
the thorax

The Assessment
LABORATORY EXAMINATION1. ABG analysis2. Sputum analysis3. Direct visualization - bronchoscopy4. Indirect visualization - CXR, CT and
MRI5. Pulmonary function test

ABG AnalysisThis test helps to evaluate gas
exchange in the lungs by measuring the gas pressures and pH of an arterial sample

ABG AnalysisPre-test: choose site carefully, perform
the Allen’s test, secure equipments- syringe, needle, container with ice
Intra-test: Obtain a 5 mL specimen from the artery (brachial, femoral and radial)
Post-test: Apply firm pressure for 5 minutes, label specimen correctly, place in the container with ice

ABG Analysis
ABG normal valuesPaO2 80-100 mmHgPaCO2 35-45 mmHgpH 7.35- 7.45HCO3 22- 26 mEq/LO2 Sat 95-99%

Sputum AnalysisThis test analyzes the sample of sputum
to diagnose respiratory diseases, identify organism, and identify abnormal cells

Sputum Analysis Pre-test: Encourage to increase fluid intake Intra-test: rinse mouth with WATER only,
instruct the patient to take 3 deep breaths and force a deep cough, steam nebulization, collect early morning sputum
Post-test: provide oral hygiene, label specimen correctly

Pulse OximetryNon-invasive method of continuously
monitoring the oxygen saturation of hemoglobin
A sensor or probe is attached to the earlobe, forehead, fingertip or the bridge of the nose

BronchoscopyA direct inspection of the trachea and
bronchi through a flexible fiber-optic or a rigid bronchoscope
Done to determine location of pathologic lesions, to remove foreign objects, to collect tissue specimen and remove secretions/aspirated materials

Bronchoscopy Pre-test: Consent, NPO x 6h, teaching Intra-test: position supine or sitting upright in
a chair, administer sedative, gag reflex will be abolished, remove dentures
Post-test: NPO until gag reflex returns, position SEMI-fowler’s with head turned to sides, hoarseness is temporary, CXR after the procedure, keep tracheostomy set and suction x 24 hours

ThoracentesisPleural fluid aspiration for obtaining a
specimen of pleural fluid for analysis, relief of lung compression and biopsy specimen collection

Thoracentesis Pre-test: Consent Intra-test: position the patient sitting with arms
on a table or side-lying fowler’s, instruct not to cough, breathe deeply or move
Post-test: position unaffected side to allow lung expansion of the affected side, CXR obtained, maintain pressure dressing and monitor respiratory status

Pulmonary Function TestsVolume and capacity tests aid diagnosis
in patient with suspected pulmonary dysfunction
Evaluates ventilatory functionDetermines whether obstructive or
restrictive diseaseCan be utilized as screening test

Pulmonary Function Test
Lung VolumesTidal volume Inspiratory reserve volumeExpiratory reeve volumeResidual volume

Pulmonary Function Test
Lung capacities Inspiratory capacityVital capacityFunctional residual capacityTotal lung capacity

Pulmonary Function Test Pre-test: Teaching, no smoking for 3 days,
only light meal 4 hours before the test Intra-test: position sitting, bronchodilator,
nose-clip and mouthpiece, fatigue and dyspnea during the test
Post-test: adequate rest periods, loosen tight clothing

Common Respiratory Problemsand the common interventions

Dyspnea
Breathing difficultyAssociated with many
conditions- CHF, MG, GBS, Muscular dystrophy, obstruction, etc…

Dyspnea
General nursing interventions: 1. Fowler’s position to promote
maximum lung expansion and promote comfort. An alternative position is the ORTHOPNEIC position
2. O2 usually via nasal cannula 3. Provide comfort and distractions

Cough and sputum production
Cough is a protective reflexSputum production has many stimuliThick, yellow, green or rust-colored
bacterial pneumoniaProfuse, Pink, frothy pulmonary
edemaScant, pink-tinged, mucoid Lung
tumor

Cough and sputum production
General nursing Intervention1. Provide adequate hydration2. Administer aerosolized solutions3. advise smoking cessation4. oral hygiene

CyanosisBluish discoloration of the skinA LATE indicator of hypoxiaAppears when the unoxygenated
hemoglobin is more than 5 grams/dLCentral cyanosis observe color on the
undersurface of tongue and lipsPeripheral cyanosis observe the nail
beds, earlobes

Cyanosis Interventions:
Check for airway patency Oxygen therapy Positioning Suctioning Chest physiotherapy Check for gas poisoning Measures to increased hemoglobin

HemoptysisExpectoration of blood from the
respiratory tractCommon causes: Pulmo infection, Lung
CA, Bronchiectasis, Pulmo emboliBleeding from stomach acidic pH,
coffee ground material

Hemoptysis
Interventions:Keep patent airwayDetermine the causeSuction and oxygen therapyAdminister Fibrin stabilizers like
aminocaproic acid and tranexamic acid

EpistaxisBleeding from the nose caused by rupture
of tiny, distended vessels in the mucus membrane
Most common site- anterior septumCauses
1. trauma2. infection3. Hypertension4. blood dyscrasias , nasal tumor, cardio
diseases

EpistaxisNursing Interventions1. Position patient: Upright, leaning
forward, tilted prevents swallowing and aspiration
2. Apply direct pressure. Pinch nose against the middle septum x 5-10 minutes
3. If unrelieved, administer topical vasoconstrictors, silver nitrate, gel foams
4. Assist in electrocautery and nasal packing for posterior bleeding

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections1. Rhinitis- allergic, non-allergic and
infectious2. Sinusitis- acute and chronic3. Pharyngitis- acute and chronic

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections
1. Rhinitis- Assessment findingsRhinorrheaNasal congestionNasal itchinessSneezingHeadache

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections
2. sinusitis- Assessment findingsFacial painTenderness over the paranasal sinusesPurulent nasal dischargesEar pain, headache, dental painDecreased sense of smell

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections
3. Pharyngitis- Assessment findings Fiery-red pharyngeal membrane White-purple flecked exudates Enlarged and tender cervical lymph nodes Fever malaise ,sore throat Difficulty swallowing Cough may be absent

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections- Laboratory tests
1. CBC2. Culture

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections: Nursing Interventions
1. Maintain Patent Airway Increase fluid intake to loosen secretions Utilize room vaporizers or steam inhalation Administer medications to relieve nasal
congestion

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections: Nursing Interventions
2. Promote comfortAdminister prescribed analgesicsAdminister topical analgesicsWarm gargles for the relief of sore
throatProvide oral hygiene

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections: Nursing Interventions
3. Promote communication Instruct patient to refrain from speaking
as much as possibleProvide writing materials

CONDITIONS OF THE UPPER AIRWAY
Upper airway infections: Nursing Interventions
4. Administer prescribed antibioticsMonitor for possible complications like
meningitis, otitis media, abscess formation
5. Assist in surgical intervention

CONDITIONS OF THE UPPER AIRWAY
Upper airway infection: Tonsillitis Infection and inflammation of the tonsilsMost common organism- Group A- beta
hemolytic streptococcus (GABS)

CONDITIONS OF THE UPPER AIRWAY
Upper airway infection: TonsillitisASSESSMENT FINDINGSSore throat and mouth breathingFeverDifficulty swallowingEnlarged, reddish tonsilsFoul-smelling breath

CONDITIONS OF THE UPPER AIRWAY
Upper airway infection: TonsillitisLaboratory test1. CBC2. throat culture

CONDITIONS OF THE UPPER AIRWAY
Upper airway infection: TonsillitisMEDICAL management1. Antibiotics- penicillin2. Tonsillectomy for chronic cases and
abscess formation

CONDITIONS OF THE UPPER AIRWAY
Upper airway infection: TonsillitisNURSING INTERVENTION for
tonsillectomy1. Pre-operative careConsentRoutine pre-op surgical care

CONDITIONS OF THE UPPER AIRWAY
Upper airway infection: TonsillitisNURSING INTERVENTION for
tonsillectomy2. POST-operative carePosition: Most comfortable is PRONE,
with head turned to sideMaintain oral airway, until gag reflex
returns

CONDITIONS OF THE UPPER AIRWAY
Upper airway infection: TonsillitisNURSING INTERVENTION for
tonsillectomy2. POST-operative careApply ICE collar to the neck to reduce
edemaAdvise patient to refrain from talking and
coughing Ice chips are given when there is no
bleeding and gag reflex returns

CONDITIONS OF THE UPPER AIRWAY
Upper airway infection: TonsillitisNURSING INTERVENTION for
tonsillectomy2. POST-operative careNotify physician ifa. Patient swallows frequentlyb. vomiting of large amount of bright red or
dark bloodc. PR increased, restless and Temp is
increased

Laryngeal Cancer A malignant tumor of the larynx More frequent in men 50-70 years oldRISK FACTORS
1. Smoking2. Alcohol3. Exposure to chemicals4. Straining of voice5. chronic laryngitis6. Deficiency of Riboflavin7. family history

Laryngeal CancerGrowth can be anywhere in the larynx1. Supraglottic- above the vocal cords2. glottic- vocal cord area3. infraglottic- below the vocal cords
Most tumors are found in the glottic area

Laryngeal CancerASSESSMENT FINDINGSHoarseness of more than TWO weeks
durationCough and sore throat Burning and pain in the throat especially
after consuming HOT liquids and citrus foods
Neck lumpDysphagia, dyspnea, foul breath, CLAD

Laryngeal CancerLABORATORY FINDINGS1. Indirect laryngoscopy2. direct laryngoscopy3. Biopsy4. CT and MRI
Most commonly- squamos carcinoma

Laryngeal CancerMEDICAL MANAGEMENTRadiation therapyChemotherapySurgery
Partial laryngectomy Supraglottic laryngectomy Hemilaryngectomy Total laryngectomy

Laryngeal CancerNURSING MANAGEMENT: PRE-operative1. Provide the patient pre-operative
teachingsClarify misconceptionsTell that the natural voice will be lostTeach communication alternativesCollaborate with other team members

Laryngeal CancerNURSING MANAGEMENT2. reduce patient ANXIETYProvide opportunities for patient and family
members to ask questionsReferrals to previous patients with
laryngeal cancers and cancer groups

Laryngeal CancerNURSING MANAGEMENT: POST-op3. Maintain PATENT AirwayPosition patient: Semi or High Fowler’sSuction secretionsEncourage to deep breath, turn and cough

Laryngeal CancerNURSING MANAGEMENT: POST-op4. Administer care of the laryngectomy
tubeSuction as neededCleanse the stoma with salineAdminister humidified oxygenLaryngectomy tube is usually removed
within 3-6 weeks after surgery

Laryngeal CancerNURSING MANAGEMENT: POST-op5. Promote alternative communication
methodsCall bell or hand bellMagic SlateHand signalsCollaborate with speech therapist

Laryngeal CancerNURSING MANAGEMENT: POST-op6. Promote adequate NutritionNPO after operationNo foods or drinks per orem for 10 days IVF, TPN are alternative nutrition routesStart oral feedings with thick liquids, avoid
sweet foods

Laryngeal CancerNURSING MANAGEMENT: POST-op7. Promote positive body image and self-
esteemEncourage verbalization of feelingsAllow independence in self-care

Laryngeal CancerNURSING MANAGEMENT: POST-op8. Monitor for COMPLICATIONSRespiratory Distress
Suction Coughing and deep breathing Humidified oxygen Alert the surgeon

Laryngeal CancerNURSING MANAGEMENT: POST-op8. Monitor for ComplicationsHemorrhage
Monitor for bleeding Monitor vital signs Apply direct pressure over the bleeding artery Summon assistance and alert the surgeon

Laryngeal CancerNURSING MANAGEMENT: POST-op8. Monitor for COMPLICATIONSWound infection and breakdownMonitor for increased temperature,
purulent drainage and increased redness/tenderness
Administer antibioticsClean and change dressing OD

Laryngeal CancerNURSING MANAGEMENT: HOME CAREHumidification system at home is neededAVOID swimmingCover the stoma with hands or plastic bib
over the openingAdvise beauty salons to avoid hair sprays,
powders and loose hair near the openingOral hygiene frequently

Acute Respiratory Failure
Sudden and life-threatening deterioration of the gas-exchange function of the lungs
Occurs when the lungs no longer meet the body’s metabolic needs

Acute Respiratory Failure Defined clinically as:1. PaO2 of less than 50 mmHg2. PaCO2 of greater than 5o mmHg3. Arterial pH of less than 7.35

Acute Respiratory Failure
CAUSES CNS depression- head trauma, sedatives CVS diseases- MI, CHF, pulmonary emboli Airway irritants- smoke, fumes Endocrine and metabolic disorders-
myxedema, metabolic alkalosis Thoracic abnormalities- chest trauma,
pneumothorax

Acute Respiratory Failure
PATHOPHYSIOLOGYDecreased Respiratory DriveBrain injury, sedatives, metabolic
disorders impair the normal response of the brain to normal respiratory stimulation

Acute Respiratory Failure
PATHOPHYSIOLOGYDysfunction of the chest wallDystrophy, MS disorders, peripheral
nerve disorders disrupt the impulse transmission from the nerve to the diaphragm abnormal ventilation

Acute Respiratory Failure
PATHOPHYSIOLOGYDysfunction of the Lung ParenchymaPleural effusion, hemothorax,
pneumothorax, obstruction interfere ventilation prevent lung expansion

Acute Respiratory Failure ASSESSMENT FINDINGS Restlessness dyspnea Cyanosis Altered respiration Altered mentation Tachycardia Cardiac arrhythmias Respiratory arrest

Acute Respiratory Failure DIAGNOSTIC FINDINGSPulmonary function test- pH below 7.35CXR- pulmonary infiltratesECG- arrhythmias

Acute Respiratory Failure MEDICAL TREATMENT IntubationMechanical ventilationAntibioticsSteroidsBronchodilators

Acute Respiratory Failure NURSING INTERVENTIONS1. Maintain patent airway 2. Administer O2 to maintain Pa02 at
more than 50 mmHg3. Suction airways as required4. Monitor serum electrolyte levels5. Administer care of patient on
mechanical ventilation

COPDThese are group of disorders
associated with recurrent or persistent obstruction of air passage and airflow, usually irreversible.

COPDThe most common cause of COPD is
cigarette smoking. Asthma, Chronic bronchitis, Emphysema and Bronchiectasis are the common disorders.

COPD
The general pathophysiology: In COPD there is airflow limitation
that is both progressive and associated with abnormal inflammatory response of the lungs to stimuli, usually smoke, particles and dust

ASTHMAThe acute episode of airway
obstruction is characterized by airway hyperactivity to various stimuli that results in recurrent wheezing brought about by edema and bronchospasm

Asthma Pathophysiology Immunologic/allergic reaction results in
histamine release, which produces three main airway responses
a. Edema of mucous membranesb. Spasm of the smooth muscle of
bronchi and bronchiolesc. Accumulation of tenacious secretions

Asthma Assessment Findings Assessment findings1. Family history of allergies2. Client history of eczema

Asthma Assessment Findings Assessment findings 3. Pulmonary signs and symptoms-
Respiratory distress: slow onset of shortness of breath, expiratory wheeze, prolonged expiratory phase, air trapping (barrel chest if chronic), use of accessory muscles, irritability (from hypoxia), diaphoresis, cough, anxiety, weak pulse, diaphoresis and change in sensorium if severe attack

Asthma Assessment Findings Assessment findings 4. Use of accessory muscles of
respiration, inspiratory retractions, prolonged I:E ratio
5. Cardiovascular symptoms: tachycardia, ECG changes, hypertension, decreased cardiac contractility, pulsus paradoxus
6. CNS manifestations: anxiety, restlessness, fear and disorientation

EmphysemaThere is progressive and
irreversible alveolocapillary destruction with abnormal alveolar enlargement causing alveolar wall destruction. The result is INCREASED lung compliance, DECREASED oxygen diffusion and INCREASED airway resistance!

Emphysema
These changes cause a state of carbon dioxide retention, hypoxia, and respiratory acidosis.

Emphysema Cigarette smoking
Heredity, Bronchial asthmaAging process
Disequilibrium between
ELASTASE & ANTIELASTASE (alpha-1-antitrypsin)
Destruction of distal airways and alveoliOverdistention of ALVEOLI
Hyper-inflated and pale lungs
Air traping, decreased gas exchange and Retention of CO2
Hypoxia Respiratory acidosis

Emphysema Assessment
1. Anorexia, fatigue, weight loss2. Feeling of breathlessness,
cough, sputum production, flaring of the nostrils, use of accessory muscles of respiration, increased rate and depth of breathing, dyspnea

Emphysema Assessment3. Decreased respiratory excursion,
resonance to hyper-resonance, decreased breath sounds with prolonged expiration, normal or decreased fremitus
4. Diagnostic tests: pCO2 elevated or normal; PO2 normal or slightly decreased

Chronic bronchitisChronic inflammation of the bronchial
air passageway characterized by the presence of cough and sputum production for at least 3 months in each 2 consecutive years.
Excessive production of mucus in the bronchi with accompanying persistent cough.

Chronic Bronchitis pathophysiology
Characteristic changes include hypertrophy/ hyperplasia of the mucus-secreting glands in the bronchi, decreased ciliary activity, chronic inflammation, and narrowing of the small airways.

Chronic Bronchitis Assessment
I. Productive (copious) cough, dyspnea on exertion, use of accessory muscles of respiration, scattered rales and rhonchi
2. Feeling of epigastric fullness, cyanosis, distended neck veins, ankle edema
3. Diagnostic tests: increased pCO2 decreased PO2

Bronchiectasis
Permanent abnormal dilation of the bronchi with destruction of muscular and elastic structure of the bronchial wall

Bronchiectasis
Caused by bacterial infection; recurrent lower respiratory tract infections; congenital defects (altered bronchial structures); lung tumors

Bronchiectasis1. Chronic cough with production of
mucopurulent sputum, hemoptysis, exertional dyspnea, wheezing
2. Anorexia, fatigue, weight loss3. Diagnostic tests
a. Bronchoscopy reveals sources and sites of secretions
b. Possible elevation of WBC

COPD Management
Independent and Collaborative Management
1. Rest-To reduce oxygen demands of tissues
2. Increase fluid intake-To liquefy mucus secretions
3. Good oral care-To remove sputum and prevent infection

COPD ManagementIndependent and Collaborative Management 4. Diet: High caloric diet provides source of energy High protein diet helps maintain integrity of
alveolar walls Moderate fats Low carbohydrate diet limits carbon
dioxide production (natural end product). The client has difficulty exhaling carbon dioxide.

COPD Management
Independent and Collaborative Management
5. O2 therapy 1 to 3 lpm (2 lpm is safest)
Do not give high concentration of oxygen. The drive for breathing may be depressed.

COPD Management
Independent and Collaborative Management
6. Avoid cigarette smoking, alcohol, and environmental pollutants-These inhibit mucociliary function.
7. CPT –percussion, vibration, postural drainage

COPD Management Independent and Collaborative
Management8. Bronchial hygiene measuresSteam inhalationAerosol inhalationMedimist inhalation

COPD Management Pharmacotherapy 1. Expectorants (guaiafenessin)/ mucolytic
(mucomyst/mucosolvan) 2. Antitussives Dextrometorphan Codeine Observe for drowsiness Avoid activities that involve mental alertness,
e.g driving, operating electrical machines Cause decrease peristalsis thereby constipation

COPD ManagementPharmacotherapy3. BronchodilatorsAminophylline (Theophylline)Ventolin (Salbutamol)Bricanyl (Terbutaline)Alupent (Metaproterenol)
Observe for tachycardia

COPD ManagementPharmacotherapy4. AntihistamineBenadryl (Diphenhydramine)Observe for drowsiness5. SteroidsAnti-inflammatory effect6. Antimicrobials

Flail Chest
Complication of chest trauma occurring when 3 or more adjacent ribs are fractured at two or more sites, resulting in free-floating rib segments.

Flail ChestChest wall is no longer able
to provide the bony structure necessary to maintain adequate ventilation; consequently
the flail portion and underlying tissue move paradoxically (in opposition) to the rest of the chest cage and lungs.

Flail ChestThe flail portion is sucked in on
inspiration and bulges out on expiration.
Result is hypoxia, hypercarbia, and increased retained secretions.
Caused by trauma (sternal rib fracture with possible costochondral separations).

Flail Chest PATHOPHYSIOLOGY During inspiration, as the chest expands,
the detached part of the rib segment (flail segment) moves in a “paradoxical” manner
The chest is pulled INWARD during inspiration, reducing the amount of air that can be drawn into the lungs
The chest bulges OUTWARD during expiration because the intrathoracic pressure exceeds atmospheric pressure. The patient has impaired exhalation

Flail Chest
This paradoxical action will lead to:Increased dead spaceReduced alveolar ventilationDecreased lung complianceHypoxemia and respiratory
acidosisHypotension, inadequate tissue
perfusion can also follow

Flail ChestAssessment findings 1. Severe dyspnea; rapid, shallow, grunty
breathing; paradoxical chest motion. The chest will move INWARDS on inhalation and OUTWARDS on exhalation.
2. Cyanosis, possible neck vein distension, tachycardia, hypotension
3. Diagnostic tests a. PO2 decreased b. pCO2 elevated c. pH decreased

Flail ChestNursing interventions 1. Maintain an open airway: suction
secretions, blood from nose, throat, mouth, and via endotracheal tube; note changes in amount, color, and characteristics.
2. Monitor mechanical ventilation 3. Encourage turning, coughing, and deep
breathing. 4. Monitor for signs of shock:
HYPOTENSION, TACHYCARDIA

Flail Chest
Medical management: SUPPORTIVE
1. Internal stabilization with a volume-cycled ventilator
2. Drug therapy (narcotics, sedatives)

PneumothoraxPartial or complete collapse
of the lung due to an accumulation of air or fluid in the pleural space

Pneumothorax
Typesa. Spontaneous pneumothorax: the
most common type of closed pneumothorax; air accumulates within the pleural space without an obvious cause. Rupture of a small bleb on the visceral pleura most frequently produces this type of pneumothorax.

Pneumothorax
Typesb. Open pneumothorax: air enters the
pleural space through an opening in the chest wall; usually caused by stabbing or gunshot wound.

PneumothoraxTypesc. Tension pneumothorax: air enters
the pleural space with each inspiration but cannot escape; causes increased intrathoracic pressure and shifting of the mediastinal contents to the unaffected side (mediastinal shift).

PneumothoraxAssessment findings 1. Sudden sharp pain in the chest,
dyspnea, diminished or absent breath sounds on affected side, tracheal shift to the opposite side (tension pneumothorax accompanied by mediastinal shift)
2. Weak, rapid pulse; anxiety; diaphoresis

PneumothoraxAssessment findings 3. Diagnostic tests
a. Chest x-ray reveals area and degree of pneumothorax
b. pCO2 elevated c. pH decreased

PneumothoraxNursing interventions
1. Provide nursing care for the client with an endotracheal tube: suction secretions, vomitus, blood from nose, mouth, throat, or via endotracheal tube; monitor mechanical ventilation.

Pneumothorax
Nursing interventions
2. Restore/promote adequate respiratory function.
a. Assist with thoracentesis and provide appropriate nursing care.
b. Assist with insertion of a chest tube to water- seal drainage and provide appropriate nursing care.
c. Continuously evaluate respiratory patterns and report any changes.

Pneumothorax
Nursing interventions
3. Provide relief/control of pain.a. Administer
narcotics/analgesics/sedatives as ordered and monitor effects.
b. Position client in high-Fowler’s position.

AtelectasisCollapse of part or all of a lung due
to bronchial obstructionMay be caused by
intrabronchial obstruction tumors, bronchospasm foreign bodies extrabronchial compression (tumors,
enlarged lymph nodes); or endobronchial disease (bronchogenic
carcinoma, inflammatory structures)

AtelectasisAssessment findings 1. Signs and symptoms may be absent
depending upon degree of collapse and rapidity with which bronchial obstruction occurs
2. Dyspnea, decreased breath sounds on affected side, decreased respiratory excursion, dullness to flatness upon percussion over affected area

Atelectasis
Assessment findings3. Cyanosis, tachycardia,
tachypnea, elevated temperature, weakness, pain over affected area

Atelectasis
Assessment findings
4. Diagnostic testsa. Bronchoscopy: may or may not
reveal an obstructionb. Chest x-ray shows diminished size
of affected lung and lack of radiance over atelectatic area
c. pO2 decreased

Pleural Effusion
Defined broadly as a collection of fluid in the pleural space
A symptom, not a disease; may be produced by numerous conditions

Pleural Effusion
General ClassificationTransudative effusion:
accumulation of protein-poor, cell-poor fluid
Exudative effusion: accumulation of protein rich fluid

Pleural Effusion
Assessment findings1. Dyspnea, dullness over affected
area upon percussion, absent or decreased breath sounds over affected area, pleural pain, dry cough, pleural friction rub
2. Pallor, fatigue, fever, and night sweats (with empyema)

Pleural EffusionAssessment findings3. Diagnostic tests a. Chest x-ray positive if greater than
250 cc pleural fluid b. Pleural biopsy may reveal
bronchogenic carcinoma c. Thoracentesis may contain blood if
cause is cancer, pulmonary infarction, or tuberculosis; positive for specific organism in empyema.

Pleural Effusion
Nursing interventions: In general: 1. Assist with repeated thoracentesis. 2. Administer narcotics/sedatives as
ordered to decrease pain. 3. Assist with instillation of medication
into pleural space (reposition client every 15 minutes to distribute the drug within the pleurae).
4. Place client in high-Fowler’s position to promote ventilation.

Pleural EffusionMedical management1. Identification and treatment of the
Underlying cause2. Thoracentesis3. Drug therapy
a. Antibiotics: either systemic or inserted directly into pleural space
b. Fibrinolytic enzymes: trypsin, streptokinase-. streptodornase to decrease thickness of pus and dissolve fibrin clots
4. Closed chest drainage5. Surgery: open drainage

PneumoniaAn inflammation of the alveolar spaces
of the lung, resulting in consolidation of lung tissue as the alveoli fill with exudates
The various types of pneumonias are classified according to the offending organism.
Pneumonia can also be classified as COMMUNITY Acquired Pneumonia (CAP) and Hospital acquired pneumonia (HAP)

Pneumonia
PATHOPHYSIOLOGIC FINDINGS ARE: HYPERTROPHY OF MUCOUS
MEMBRANE Increased sputum productionWheezingDyspneaCoughRalesRonchi

Pneumonia
PATHOPHYSIOLOGIC FINDINGS ARE: INCREASED CAPILLARY
PERMEABILITY Increased Fluid Exudation Consolidation-tissue that solidifies as a
result of collapsed alveoli Hypoxemia

Pneumonia
PATHOPHYSIOLOGIC FINDINGS ARE:
INFLAMMATION OF THE PLEURAChest painPleural effusionDullnessDecreased Breath sounds Increased tactile fremitus

Pneumonia
PATHOPHYSIOLOGIC FINDINGS ARE:
HYPOVENTILATIONDecreased Chest expansionRespiratory acidosis
Depressed PROTECTIVE MECHANISM Increased WBC (leukocytosis) Increased RR and Fever

PneumoniaAssessment findings Cough with greenish to rust-colored
sputum production rapid, shallow respirations with an
expiratory grunt nasal flaring; intercostal rib retraction; use
of accessory muscles of respiration rales or crackles (early) progressing to
coarse (later). Tactile fremitus is INCREASED!

Pneumonia
Assessment findingsFever, chills, chest pain,
weakness, generalized malaiseTachycardia, cyanosis, profuse
perspiration, abdominal distension
Rapid shallow breathing

Pneumonia
Diagnostic testsa. Chest x-ray shows consolidation
over affected areasb. WBC increasedc. pO2 decreasedd. Sputum specimen- culture
reveal particular causative organism

Pneumonia1. Facilitate adequate ventilation. a. Administer oxygen as needed and assess
its effectiveness. b. Place client in Fowler’s position. c. Turn and reposition frequently clients who
are immobilized/obtunded. d. Administer analgesics as ordered to relieve
pain associated with breathing e. Auscultate breath sounds every 2—4 hours. f. Monitor ABGs.

PneumoniaGENERAL Nursing interventions
2. Facilitate removal of secretionsgeneral hydrationdeep breathing and coughingSuctioningExpectorantsaerosol treatments via nebulizer,
humidification of inhaled airchest physical therapy

Pneumonia
GENERAL Nursing interventions
3. Observe color, characteristics of sputum and report any changes; encourage client to perform good oral hygiene after expectoration.

Pneumonia
GENERAL Nursing interventions
4. Provide adequate rest and relief/control of pain.
a. Provide bed rest with limited physical activity.
b. Limit visits and minimize conversations. c. Plan for uninterrupted rest periods. d. Institute nursing care in blocks to ensure
periods of rest. e. Maintain pleasant and restful environment

Pneumonia
GENERAL Nursing interventions5. Administer antibiotics as ordered.
Monitor effects and possible toxicity.6. Prevent transmission (respiratory
isolation may be required for clients with staphylococcal pneumonia).
7. Control fever and chills: monitor temperature and administer antipyretics as ordered, maintain increased
fluid intake, provide frequent clothing and linen changes.

Pneumonia
GENERAL Nursing interventions8. Provide client teaching and discharge
planning concerning prevention of recurrence. a. Medication regimen/antibiotic therapy b. Need for adequate rest, c. Need to continue deep breathing and coughing

Pneumonia
GENERAL Nursing interventions8. Provide client teaching and discharge
planning concerning prevention of recurrence. d. Availability of vaccines e. Techniques that prevent transmission (use of
tissues when coughing, adequate disposal of secretions)
f. Avoidance of persons with known respiratory infections
g. Need to report signs and symptoms of respiratory infection

Lung Cancer
Primary pulmonary tumors arise from the bronchial epithelium and are therefore referred to as bronchogenic carcinomas.
FACTORS: Possibly caused by inhaled carcinogens (primarily cigarette smoke but also asbestos, nickel, iron oxides, air silicone pollution; preexisting pulmonary disorders PTB, COPD)

Lung Cancer Assessment findingsPersistent cough (may be productive
or blood tinged)chest paindyspneaunilateral wheezing, friction rub,
possible unilateral paralysis of the diaphragm
Fatigue, anorexia, nausea, vomiting, pallor

Lung CancerDiagnostic tests. a. Chest x-ray may show presence of tumor or
evidence of metastasis to surrounding structures
b. Sputum for cytology reveals malignant cells
c. Bronchoscopy: biopsy reveals malignancy d. Thoracentesis: pleural fluid contains
malignant cells e. Biopsy of lymph nodes may reveal
metastasis

Lung Cancer
1. Provide support and guidance to client as needed.
2. Provide relief/control of pain.
3. Administer medications as ordered and monitor effects/side effects.
4. Control nausea: administer medications as ordered, provide good oral hygiene, provide small and more frequent feedings.

Lung Cancer
5. Provide nursing care for a client with a thoracotomy.
6. Provide client teaching and discharge planning concerning a. Disease process, diagnostic and
therapeutic interventions b. Side effects of radiation and
chemotherapy c. Realistic information about prognosis

Lung Cancer
Medical management1. Radiation therapy2. Chemotherapy: usually includes
cyclophosphamide, methotrexate, vincristine, doxorubicin, and procarbazine; concurrently in some combination
3. Surgery: when entire tumor can be removed

Lung CancerQuick Notes on Bronchogenic Cancer
Predisposing factors Cigarette smoking Asbestosis Emphysema Smoke from burnt woodTypes Squamous cell Ca- with good prognosis Adenocarcinoma- with good prognosis Oat cell Ca- with good prognosis Undifferentiated Ca- with poor prognosis

Lung Cancer
Quick Notes on Bronchogenic Cancer
Nursing Interventions Patent airway O2 / Aerosol therapy Deep breathing exercises Relief of pain Protection from infection Adequate nutrition Chest tube management

Lung CancerQuick Notes on Bronchogenic CancerSurgery Pneumonectomy=Removal of a lung (either left or
right) Lobectomy=Removal of a lobe. Segmentectomy=Removal of a segment. Wedge resection=Removal of the entire tumor
regardless of the segment. Decortication=Stripping off of fibrinous membrane
enclosing the lung Thoracoplasty=Removal of rib/s. Usually done after
pneumonectomy, to reduce the size of the empty thorax thereby prevent mediastinal shift.

Pulmonary Embolism
This refers to the obstruction of the pulmonary artery or one of its branches by a blood clot (thrombus) that originates somewhere in the venous system or in the right side of the heart.
Most commonly, pulmonary embolism is due to a clot or thrombus from the deep veins of the lower legs.

Pulmonary Embolism
CausesFat embolism. Air embolismMultiple traumaPVD’s Abdominal surgery ImmobilityHypercoagulability

Pulmonary Embolism
PATHOPHYSIOLOGYThe thrombus that travels from any
part of the venous system obstructs either completely or partially. Then the lungs will have inadequate blood supply, with resultant increase in dead space in the lungs
Gas exchange will be impaired or absent in the involved area

Pulmonary Embolism
PATHOPHYSIOLOGYThe regional pulmonary vasculature
will constrict causing increased resistance, increased pulmonary arterial pressure and then increase workload of the right side of the heart.

Pulmonary Embolism
PATHOPHYSIOLOGYWhen the work of the right side of
the heart exceeds its capacity, right ventricular failure will result, leading to a decrease in cardiac output followed by decreased systemic perfusion and eventually, SHOCK

Pulmonary EmbolismAssessment Restlessness (cardinal initial sign) Dyspnea Stabbing chest pain Cyanosis Tachycardia Dilated pupils Apprehension/ fear Diaphoresis Dysrhythmias Hypoxia

Pulmonary Embolism
Diagnostic Tests:Ventilation-perfusion scanPulmonary arteriographyCXRECGABG

Pulmonary Embolism
Nursing InterventionsOxygen therapy STATEarly ambulation postopMonitor obese patientDo not massage legsRelieve pain- analgesicsHOB elevatedHeparin (2 weeks) then Coumadin (3-6
months)

Pulmonary Embolism
Patient Teaching for prevention of Pulmonary Embolism
Active leg exercises to avoid venous stasis
Early ambulationUse of elastic compression stockingsAvoidance of leg-crossing and sitting
for prolonged periodsDrink fluids

Surgical Aspect of Respiratory CareThoracic Surgerya. Exploratory thoracotomy: anterior or
posterolateral incision through the fourth, fifth, sixth, or seventh intercostal spaces to expose and examine the pleura and lung

Surgical Aspect of Respiratory CareThoracic Surgeryb. Lobectomy: removal of one lobe of a
lung; treatment for bronchiectasis, bronchogenic carcinoma, emphysematous blebs, lung abscesses

Surgical Aspect of Respiratory CareThoracic Surgeryc. Pneumonectomy: removal of an
entire lung; most commonly done as treatment for bronchogenic carcinoma

Surgical Aspect of Respiratory CareThoracic Surgeryd. Segmental resection: removal of one
or more segments of lung; most often done as treatment for bronchiectasis

Surgical Aspect of Respiratory CareThoracic Surgerye. Wedge resection: removal of lesions
that occupy only part of a segment of lung tissue; for excision of small nodules or to obtain a biopsy

Surgical Aspect of Respiratory CareNursing interventions: PREOPERATIVE1. Provide routine pre-op care.2. Perform a complete physical
assessment of the lungs to obtain baseline data.
3. Explain expected post-op measures: care of incision site, oxygen, suctioning, chest tubes (except if pneumonectomy performed)

Surgical Aspect of Respiratory Care
Nursing interventions: PREOPERATIVE4. Teach client adequate splinting of
incision with hands or pillow for turning, coughing, and deep breathing.
5. Demonstrate ROM exercises for affected side.
6. Provide chest physical therapy to help remove secretions.

Surgical Aspect of Respiratory Care
Nursing interventions: POSTOPERATIVE 1. Provide routine post-op care. 2. Promote adequate ventilation. a. Perform complete physical assessment of
lungs and compare with pre-op findings. b. Auscultate lung fields every 1—2 hours. c. Encourage turning, coughing, and deep
breathing every 1—2 hours after pain relief obtained.

Surgical Aspect of Respiratory Care
Nursing interventions: POSTOPERATIVE 2. Promote adequate ventilation. d. Perform tracheobronchial suctioning if
needed. e. Assess for proper maintenance of chest
drainage system (except after pneumonectomy).
f. Monitor ABGs and report significant changes.
g. Place client in semi-Fowler’s position

Surgical Aspect of Respiratory Care
Nursing interventions: POSTOPERATIVE
If pneumonectomy is performed, follow surgeon’s orders about positioning, often on back or OPERATIVE SIDE
If Lobectomy, patient is usually positioned on the UNOPERATIVE SIDE

Surgical Aspect of Respiratory Care
Nursing interventions: POSTOPERATIVE
3. Provide pain relief.a. Administer narcotics/analgesics
prior to turning, coughing, and deep breathing.
b. Assist with splinting while turning, coughing, deep breathing.

Surgical Aspect of Respiratory CareNursing interventions:
POSTOPERATIVE
4. Provide client teaching and discharge planning concerning
a. Need to continue with coughing/deep breathing for 6—8 weeks post-op and to continue ROM exercises
b. Importance of adequate rest with gradual increases in activity levels

Surgical Aspect of Respiratory Care
Nursing interventions: POSTOPERATIVE4. Provide client teaching and discharge
planning concerning c. High-protein diet with inclusion of
adequate fluids d. Chest physical therapy e. Good oral hygiene f. Need to avoid persons with known upper
respiratory infection g. Adverse signs and symptoms h. Avoidance of crowds and poorly ventilated
areas.
Recommended






![Respiratory system roadmap.pptx [Repaired] - Loginanatomical-sciences.health.wits.ac.za/roadmaps/Respiratory system... · DIVISION OF THE RESPIRATORY SYSTEM CONDUCTING PORTION Nasal](https://img.pdfslide.net/doc/110x75/5a78c3d87f8b9ae6228c9db0/respiratory-system-repaired-loginanatomical-scienceshealthwitsaczaroadmapsrespiratory.jpg)