11
RPA NEPHROLOGY CODINGRPA NEPHROLOGY CODING
AND BILLING SEMINARSAND BILLING SEMINARS
20122012
22
Coding and Billing for Coding and Billing for
Nephrology PracticesNephrology Practices
Debra Lawson, CPC, PCSDebra Lawson, CPC, PCSNephrology Billing & Management Services, LLC.Nephrology Billing & Management Services, LLC.
Rogersville, TennesseeRogersville, Tennessee

Breaking NewsBreaking News……......... .........
CRIME RATES RISECRIME RATES RISE
Perpetrators caughtPerpetrators caught
Accomplices namedAccomplices named
Details at 11Details at 11
33
IT CANIT CAN’’T HAPPEN TO ME!T HAPPEN TO ME!
�� Been in practice for years and every time Been in practice for years and every time
they look itthey look it’’s been OKs been OK
�� II’’ll ll ““fly under the radarfly under the radar”” so they wonso they won’’t look at t look at
meme
�� It happened to Dr. Joe, but everyone knows It happened to Dr. Joe, but everyone knows
hehe’’s a crooks a crook
�� II’’m a small fish, they will go after the big m a small fish, they will go after the big
guysguys
44
WHAT MAKES YOU A WHAT MAKES YOU A
TARGET?TARGET?�� Time lapse in getting to the documentationTime lapse in getting to the documentation
�� Lack of documentationLack of documentation
�� Sloppy documentationSloppy documentation
�� Lack of knowledge of the documentation rulesLack of knowledge of the documentation rules
�� Thinking documentation is Thinking documentation is ““just for billingjust for billing”” and and
is not important is not important –– it has nothing to do with it has nothing to do with
medical caremedical care
�� II’’m a specialist m a specialist –– all my services are high levelall my services are high level
55
WHO IS LOOKING?WHO IS LOOKING?
�� The Audit Alphabet SoupThe Audit Alphabet Soup
–– CMSCMS
–– CERTCERT
–– RACRAC
–– OIGOIG
–– MICMIC
–– ZIPZIP
66
Isn’t it amazing…..they can lookat us, but who is looking at them!
WHY WOULD THEY LOOK AT WHY WOULD THEY LOOK AT
ME?ME?
�� Billing for services not renderedBilling for services not rendered
�� Intentional upcoding or downcoding servicesIntentional upcoding or downcoding services
�� Billing one provider under another providerBilling one provider under another provider’’s s
numbernumber
�� Billing Billing ““incident toincident to”” services when the services when the
physician is not in the suitephysician is not in the suite
�� ““MonotoneMonotone”” billingbilling
77
WHO ARE THE TARGETS?WHO ARE THE TARGETS?
�� Large practicesLarge practices
�� Small practicesSmall practices
�� Hospital owned practicesHospital owned practices
�� Teaching practicesTeaching practices
�� Joint venturesJoint ventures
�� YOU!YOU!
88
WHO ARE THE HIRED GUNS?WHO ARE THE HIRED GUNS?
�� RAC RAC –– As of March 27, 2008 CMS reported As of March 27, 2008 CMS reported
that the RAC had that the RAC had ““succeededsucceeded”” in correcting in correcting
more than $1 billion in improper payments more than $1 billion in improper payments
from Medicare from Medicare –– 96% ($992.7 million) in 96% ($992.7 million) in
overpayments and 4% (37.8 million) in overpayments and 4% (37.8 million) in
underpayments returned to providersunderpayments returned to providers–– www.cms.hhs.gov/RAC/Downloads/RAC%20Evaluation%20Report.pdfwww.cms.hhs.gov/RAC/Downloads/RAC%20Evaluation%20Report.pdf
99
WHEN WILL THEY COME FOR WHEN WILL THEY COME FOR
YOU?YOU?
�� The Tax Relief and Health Care Act of 2006 The Tax Relief and Health Care Act of 2006
made the RAC permanent and mandated made the RAC permanent and mandated
that CMS expand the program to all 50 that CMS expand the program to all 50
states by 2010states by 2010
�� Third party auditors hired by CMS will Third party auditors hired by CMS will
conduct the auditsconduct the audits
�� They will keep a percentage of what is They will keep a percentage of what is
collectedcollected
1010
HOW DO THEY IDENTIFY HOW DO THEY IDENTIFY
PROBLEM CLAIMS?PROBLEM CLAIMS?
�� Automated review Automated review –– conducted without conducted without
review of the medical record supporting the review of the medical record supporting the
claimclaim
�� Complex review Complex review –– analyzes actual medical analyzes actual medical
records supporting claims under records supporting claims under
investigationinvestigation
�� Cannot review any claims prior to Oct. 2007Cannot review any claims prior to Oct. 2007
1111
COMPLEX REVIEWSCOMPLEX REVIEWS
�� OnOn--site reviews look at the providersite reviews look at the provider’’s s
records in personrecords in person
�� May request a mail or secure transmission May request a mail or secure transmission
of the records to the RACof the records to the RAC
�� May review 10 records per 45 days for solo May review 10 records per 45 days for solo
practitionerspractitioners
�� If not received within 45 days RAC may If not received within 45 days RAC may
render a overpayment decision without render a overpayment decision without
reviewreview1212
PROVIDERPROVIDER’’S RIGHTSS RIGHTS
�� May request an extension to secure and May request an extension to secure and
forward records to the RACforward records to the RAC
�� RAC must follow Medicare policies, RAC must follow Medicare policies,
regulations, national and local carrier regulations, national and local carrier
determinations and manual instructionsdeterminations and manual instructions
�� Must follow Medicare coverage, coding and Must follow Medicare coverage, coding and
billing policies and may not apply their ownbilling policies and may not apply their own
1313
APPEAL OF A RAC DECISIONAPPEAL OF A RAC DECISION
�� Redetermination Redetermination –– 120 days from denial120 days from denial
�� Reconsideration Reconsideration –– 180 days from 180 days from
redetermination by Qualified Independent redetermination by Qualified Independent
Contractor (QIC)Contractor (QIC)
�� Administrative Law Judge hearing (60 days after Administrative Law Judge hearing (60 days after
QIC)QIC)
�� Medicare Appeals Council (MAC) hearing (60 Medicare Appeals Council (MAC) hearing (60
days after ALJ)days after ALJ)
�� Federal District Court (60 days after MAC)Federal District Court (60 days after MAC)
1414
SUCCESS RATE IN APPEAL?SUCCESS RATE IN APPEAL?
�� Providers have been successful 34% of the Providers have been successful 34% of the
time the claims were challengedtime the claims were challenged
�� This may be low given the number of This may be low given the number of
appeals still pendingappeals still pending
�� Because of the incentive given the RAC to Because of the incentive given the RAC to
find errors, providers should consider an find errors, providers should consider an
appeal if they think the RAC is erroneousappeal if they think the RAC is erroneous
1515
ARE THEY ALWAYS RIGHT?ARE THEY ALWAYS RIGHT?
�� Just because you have gotten information Just because you have gotten information
about a RAC determination, donabout a RAC determination, don’’t always t always
assume it is the correct decisionassume it is the correct decision
�� Recently there was an erroneous decision Recently there was an erroneous decision
by Connolly Consulting Associates (Region by Connolly Consulting Associates (Region
““CC”” RAC) that involved numerous providers RAC) that involved numerous providers
from West Virginia to Texas. This decision from West Virginia to Texas. This decision
was involving hospital admissions during a was involving hospital admissions during a
month the MCP was providedmonth the MCP was provided
1616
HOW DO WE PREPARE FOR HOW DO WE PREPARE FOR
AN AUDIT?AN AUDIT?
�� ““An ounce of prevention is worth a pound of An ounce of prevention is worth a pound of
curecure”” applies to auditing as much as to applies to auditing as much as to
medicinemedicine
�� Look at how things are doneLook at how things are done…….objectively .objectively
not just in how is should be donenot just in how is should be done
�� EducationEducation
�� Corrective action Corrective action –– if you are not going to if you are not going to
take the steptake the step……dondon’’t do the auditt do the audit
1717
DOCUMENTATIONDOCUMENTATION
GUIDELINESGUIDELINES
1818
ICD 9ICD 9
�� What is the patients problem that YOU are What is the patients problem that YOU are
addressing?addressing?
�� Is it a symptom or a diagnosed condition? Is it a symptom or a diagnosed condition?
�� Is it singular or multiple?Is it singular or multiple?
�� Is the clinical picture reflected complete?Is the clinical picture reflected complete?
�� How is it recorded?How is it recorded?
–– In the chartIn the chart
–– On the billOn the bill
1919
CPTCPT
�� What is the physician service What is the physician service YOU YOU
performed?performed?
–– Are the elements of documentation guidelines Are the elements of documentation guidelines
reflected?reflected?
–– Where did you do it? (site of service)Where did you do it? (site of service)
–– How is it categorized? (screening or treatment)How is it categorized? (screening or treatment)
–– How is it recorded?How is it recorded?
�� In the chartIn the chart
�� On the billOn the bill
2020
INTRODUCTIONINTRODUCTION
�� ““The proof is in the detailThe proof is in the detail””
�� The medical record is not only a document The medical record is not only a document
for billing but also a chronological record of for billing but also a chronological record of
the care that is rendered to the patientthe care that is rendered to the patient
�� The medical record protects both the patient The medical record protects both the patient
and the provider in the event of a and the provider in the event of a
malpractice case malpractice case
�� In an audit, the medical record is the only In an audit, the medical record is the only
thing an auditor will reviewthing an auditor will review2121
DOCUMENTATION DOCUMENTATION
GUIDELINES FOR GUIDELINES FOR
EVALUATION AND EVALUATION AND
MANAGEMENT MANAGEMENT
SERVICESSERVICES2222
DOCUMENTATION DOCUMENTATION
E/M SERVICESE/M SERVICES
Descriptors for the levels of E/M services Descriptors for the levels of E/M services recognize seven components:recognize seven components:
�� HistoryHistory
�� ExamExam
�� Medical Decision MakingMedical Decision Making
�� CounselingCounseling
�� Coordination of CareCoordination of Care
�� Nature of Presenting ProblemNature of Presenting Problem
�� TimeTime2323
E/M DOCUMENTATIONE/M DOCUMENTATION HISTORYHISTORY
�� History includes some or all of the History includes some or all of the following elements:following elements:
�� Chief Complaint (CC)Chief Complaint (CC)
�� History of Present Illness (HPI)History of Present Illness (HPI)
�� Review of Systems (ROS)Review of Systems (ROS)
�� Past, Family and/or Social History Past, Family and/or Social History (PFSH)(PFSH)
–– DG: The CC, ROS, and PFSH must DG: The CC, ROS, and PFSH must be listed as separate elements of be listed as separate elements of history, or may be included in the history, or may be included in the description of the recorded history of description of the recorded history of the present illnessthe present illness
2424
E/M DOCUMENTATIONE/M DOCUMENTATION HISTORYHISTORY
–– DG: An earlier ROS and/or PFSH need DG: An earlier ROS and/or PFSH need
not be renot be re--recorded if evidence shows recorded if evidence shows
update. The review and update may be update. The review and update may be
documented by:documented by:
�� Describing any new ROS and/or PFSH Describing any new ROS and/or PFSH
or noting no change in info; and/oror noting no change in info; and/or
�� Noting the date and location of the Noting the date and location of the
earlier ROS and/or PFSHearlier ROS and/or PFSH
2525
E/M DOCUMENTATIONE/M DOCUMENTATION HISTORYHISTORY
–– DGDG: The ROS and/or PFSH may be : The ROS and/or PFSH may be
recorded by staff or on a form completed recorded by staff or on a form completed
by patient. There must be a notation by patient. There must be a notation
supplementing or confirming the info supplementing or confirming the info
recorded by others to document that the recorded by others to document that the
physician reviewed the info physician reviewed the info
–– DGDG: If the physician is unable to obtain : If the physician is unable to obtain
history, history, the recordthe record should describe should describe
condition or circumstance which precludes condition or circumstance which precludes
obtaining history **IMPORTANT**obtaining history **IMPORTANT**2626
DOCUMENTATION DOCUMENTATION
CHIEF COMPLAINTCHIEF COMPLAINT
�� The CC is a concise statement describing The CC is a concise statement describing
the symptom, problem, condition, diagnosis, the symptom, problem, condition, diagnosis,
physician recommended return, or other physician recommended return, or other
factor that is the reason for the encounterfactor that is the reason for the encounter
–– DGDG: The medical record should clearly reflect : The medical record should clearly reflect
the chief complaintthe chief complaint
�� Without a chief complaint there is no element of Without a chief complaint there is no element of
historyhistory
2727
DOCUMENTATION DOCUMENTATION HISTORY OF PRESENT ILLNESSHISTORY OF PRESENT ILLNESS
HPI HPI –– chronological description of development chronological description of development
of patientof patient’’s present illness from first sign to the s present illness from first sign to the
presentpresent�� Location Location –– pain in legpain in leg
�� Quality Quality –– aching, burning, radiatingaching, burning, radiating
�� Severity Severity –– 10 on a scale of 110 on a scale of 1--1010
�� Duration Duration –– started 3 days agostarted 3 days ago
�� Timing Timing –– comes & goescomes & goes
�� Context Context –– lifted large object @ worklifted large object @ work
�� Modifying factors Modifying factors –– better with heatbetter with heat
�� Associated signs and symptoms Associated signs and symptoms –– numbnessnumbness
2828
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
�� Describe the history of the present illness Describe the history of the present illness
fully and in such a way that the nature of the fully and in such a way that the nature of the
presenting problem in clear.presenting problem in clear.
–– The documentation guidelines specify elements The documentation guidelines specify elements
that must be recorded. Higher services require that must be recorded. Higher services require
four or more elements. four or more elements.
–– Medical necessity of an E/M encounter is often Medical necessity of an E/M encounter is often
viewed through the characteristics captured in viewed through the characteristics captured in
specific HPI elements.specific HPI elements.
2929
DOCUMENTATION GUIDELINESDOCUMENTATION GUIDELINESELEMENTS OF HISTORYELEMENTS OF HISTORY
�� A A problem pertinentproblem pertinent ROS relates directly to ROS relates directly to
the problem(s) identified in the HPIthe problem(s) identified in the HPI
–– DGDG: The patient: The patient’’s positive responses and s positive responses and
pertinent negatives for the system related to pertinent negatives for the system related to
the problem should be documentedthe problem should be documented
�� An An extendedextended ROS inquires about system ROS inquires about system
directly related to problem(s) identified in directly related to problem(s) identified in
the HPI and a limited number of additional the HPI and a limited number of additional
systemssystems
3030
DOCUMENTATION GUIDELINESDOCUMENTATION GUIDELINESELEMENTS OF HISTORYELEMENTS OF HISTORY
–– DGDG: The patient: The patient’’s positive responses and s positive responses and
pertinent negatives for two to nine systems pertinent negatives for two to nine systems
must be documentedmust be documented
�� A A completecomplete ROS inquires about the ROS inquires about the
system(s) directly related to problem(s) system(s) directly related to problem(s)
identified in HPI identified in HPI plusplus all additional body all additional body
systemssystems
3131
DOCUMENTATION GUIDELINESDOCUMENTATION GUIDELINESELEMENTS OF HISTORYELEMENTS OF HISTORY
–– DGDG: : At least ten organ systems must be At least ten organ systems must be
reviewed. Those systems with positive or reviewed. Those systems with positive or
pertinent responses must be individually pertinent responses must be individually
documented. For the remaining systems, a documented. For the remaining systems, a
notation indicating notation indicating ““all other systems all other systems
reviewed and are negativereviewed and are negative”” is permissible. is permissible.
In the absence of such a notation, at least In the absence of such a notation, at least
ten systems must be individually ten systems must be individually
documented.documented.
3232
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
�� Record the ROS appropriate for the clinical Record the ROS appropriate for the clinical circumstance of the encounter. Expansive circumstance of the encounter. Expansive ROS is unnecessary for lowerROS is unnecessary for lower--level level services.services.–– When using When using ““negativenegative”” notation, always identify which notation, always identify which
systems are queried and found to be negativesystems are queried and found to be negative
�� DonDon’’t record unnecessary information t record unnecessary information solelysolely to to meet documentation requirements for a highmeet documentation requirements for a high--level level service when the nature of the presenting problem service when the nature of the presenting problem dictates a lowerdictates a lower--level of service to be medically level of service to be medically appropriate appropriate
3333
PAST, FAMILY AND/OR SOCIAL PAST, FAMILY AND/OR SOCIAL
HISTORY (HISTORY (PFSH)PFSH)
The PFSH consists of a review of three The PFSH consists of a review of three areas:areas:
�� Past HistoryPast History
�� Family HistoryFamily History
�� Social HistorySocial History
For sub. Hospital care, established pt For sub. Hospital care, established pt visits, and sub. Nursing facility care, CPT visits, and sub. Nursing facility care, CPT requires only interval history (not requires only interval history (not necessary to record PFSH)necessary to record PFSH)
3434
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
�� DonDon’’t use the terms t use the terms ““unremarkableunremarkable””, , ““nonnon--contributorycontributory”” or or ““irrelevantirrelevant””..
�� Record information about all three realms to Record information about all three realms to document document ““completecomplete”” PFSH for these PFSH for these services:services:–– New patient, new consults, initial hospital, New patient, new consults, initial hospital,
observation, nursing homeobservation, nursing home
�� DonDon’’t record unnecessary information t record unnecessary information solelysolelyto meet requirements for higherto meet requirements for higher--level level service.service.
3535
DOCUMENTATIONDOCUMENTATION
EXAMINATIONEXAMINATION
�� Problem FocusedProblem Focused
�� Expanded Problem FocusedExpanded Problem Focused
�� DetailedDetailed
�� ComprehensiveComprehensive
3636
ORGAN SYSTEMS RECOGNIZEDORGAN SYSTEMS RECOGNIZED
EXAMINATIONEXAMINATION
�� Constitutional (e.g., vital signs, general Constitutional (e.g., vital signs, general
appearance)appearance)
�� EyesEyes
�� Ears, Nose, Mouth, and ThroatEars, Nose, Mouth, and Throat
�� CardiovascularCardiovascular
�� RespiratoryRespiratory
�� Gastrointestinal Gastrointestinal
3737
ORGAN SYSTEMS RECOGNIZEDORGAN SYSTEMS RECOGNIZED
EXAMINATIONEXAMINATION
�� GenitourinaryGenitourinary
�� MusculoskeletalMusculoskeletal
�� SkinSkin
�� NeurologicNeurologic
�� PsychiatricPsychiatric
�� Hematologic/Lymphatic/Immunologic Hematologic/Lymphatic/Immunologic
3838
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING�� Understand the difference in Understand the difference in ““Expanded Problem FocusedExpanded Problem Focused””
and and ““DetailedDetailed”” exams under 1995 guidelinesexams under 1995 guidelines–– The difference is not the number of systems required (2The difference is not the number of systems required (2--7 for both 7 for both
exams)exams)
–– The difference is in the detail in which the examined system is The difference is in the detail in which the examined system is describeddescribed
�� Always examine the system(s) related to the presenting Always examine the system(s) related to the presenting problemproblem–– Use Use ““normalnormal”” or or ““negativenegative”” and and ““WNLWNL”” notations only to describe notations only to describe
unaffected or asymptomatic organ systemsunaffected or asymptomatic organ systems
�� Code the Physical Exam by the clinical circumstances of Code the Physical Exam by the clinical circumstances of the encounter, not to meet highthe encounter, not to meet high--level requirementslevel requirements
3939
DOCUMENTATIONDOCUMENTATION
COMPLEXITY OF MEDICAL DECISION MAKINGCOMPLEXITY OF MEDICAL DECISION MAKING
Medical Decision Making is measured by:Medical Decision Making is measured by:
�� The number of possible diagnoses and/or The number of possible diagnoses and/or the number of management options that the number of management options that must be consideredmust be considered
�� The amount and/or complexity of medical The amount and/or complexity of medical records, diagnostic tests, and/or other records, diagnostic tests, and/or other information that must be obtained, information that must be obtained, reviewed and analyzedreviewed and analyzed
�� The risk of significant complications, The risk of significant complications, morbidity and/or mortalitymorbidity and/or mortality
4040
NUMBER OF DIAGNOSES OR NUMBER OF DIAGNOSES OR
MANAGEMENT OPTIONSMANAGEMENT OPTIONS
–– DG: For each encounter, an DG: For each encounter, an assessment, clinical impression, or assessment, clinical impression, or diagnosis should be documenteddiagnosis should be documented�� For a presenting problem with an established For a presenting problem with an established
diagnosis, the records should indicate diagnosis, the records should indicate whether the problem is: improved, well whether the problem is: improved, well controlled, resolving or resolved or controlled, resolving or resolved or inadequately controlled, worsening, or failing inadequately controlled, worsening, or failing to change as expectedto change as expected
4141
NUMBER OF DIAGNOSES OR NUMBER OF DIAGNOSES OR
MANAGEMENT OPTIONSMANAGEMENT OPTIONS–– For a presenting problem without an established For a presenting problem without an established
diagnosis, the assessment or clinical impression diagnosis, the assessment or clinical impression
may be stated in the form of a differential may be stated in the form of a differential
diagnoses or as diagnoses or as ““possiblepossible””, , ““probableprobable”” or or ““rule rule
outout”” (R/O) diagnoses(R/O) diagnoses
–– DGDG: The initiation of, or changes in treatment : The initiation of, or changes in treatment
should be documented. Treatment includes should be documented. Treatment includes
patient instructions, nursing instructions, therapy patient instructions, nursing instructions, therapy
and medsand meds
((NOTE:NOTE: All changes in meds and refills All changes in meds and refills mustmust be be
documented)documented)
4242
AMOUNT AND/OR COMPLEXITY OF AMOUNT AND/OR COMPLEXITY OF
DATA TO BE REVIEWEDDATA TO BE REVIEWED
�� Test or procedures ordered or scheduled must be Test or procedures ordered or scheduled must be documenteddocumented
�� Review of diagnostic tests should be documentedReview of diagnostic tests should be documented
�� Decision to obtain additional info/records should be Decision to obtain additional info/records should be documenteddocumented
�� Relevant finds from review of records/info should Relevant finds from review of records/info should be documentedbe documented
�� Discussion of findings from tests with performing Discussion of findings from tests with performing physician should be documentedphysician should be documented
�� Direct interpretation of tests previously interpreted Direct interpretation of tests previously interpreted should be documentedshould be documented
4343
RISK OF COMPLICATIONS, MORBIDITY RISK OF COMPLICATIONS, MORBIDITY
AND/OR MORTALITYAND/OR MORTALITY
�� Co morbidities/underlying diseases that Co morbidities/underlying diseases that
increase the complexity of Medical Decision increase the complexity of Medical Decision
Making must be documentedMaking must be documented
�� If procedure is ordered at time of E/M If procedure is ordered at time of E/M
encounter, that test must be documentedencounter, that test must be documented
�� If procedure is done at time of E/M service, If procedure is done at time of E/M service,
that must be documentedthat must be documented
�� The referral for procedure must be The referral for procedure must be
documenteddocumented
4444
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
�� Record relevant impressions, tentative Record relevant impressions, tentative diagnosis, confirmed diagnoses and all diagnosis, confirmed diagnoses and all therapeutic options chosen related to every therapeutic options chosen related to every problem for which E/M is clearly problem for which E/M is clearly documented in the record of the other key documented in the record of the other key componentscomponents–– DonDon’’t count existent old diagnoses unless the t count existent old diagnoses unless the
record clearly demonstrates their presence record clearly demonstrates their presence increased physician work related to the increased physician work related to the encounter encounter
4545
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
�� Summarize old records or other outside Summarize old records or other outside
information reviewed and incorporated into information reviewed and incorporated into
decisiondecision--making.making.
�� Beware of templatesBeware of templates that overthat over--estimate estimate
decisiondecision--making. Understand the logic of making. Understand the logic of
templates and/or computer programs used templates and/or computer programs used
for E/M service coding.for E/M service coding.
4646
DOCUMENTATIONDOCUMENTATION
ENCOUNTER DOMINATED BYENCOUNTER DOMINATED BY
COUNSELING / COORDINATION OF CARECOUNSELING / COORDINATION OF CARE
�� If counseling and/or coordination of care If counseling and/or coordination of care
dominates more than 50% of the dominates more than 50% of the
physician/patient and/or family encounter, physician/patient and/or family encounter,
time is considered the key or controlling time is considered the key or controlling
factor to qualify for a particular level of E/M factor to qualify for a particular level of E/M
servicesservices
4747
DOCUMENTATIONDOCUMENTATIONENCOUNTER DOMINATED BYENCOUNTER DOMINATED BY
COUNSELING / COORDINATION OF CARECOUNSELING / COORDINATION OF CARE
–– DGDG: If the physician elects to report the level : If the physician elects to report the level
of care based on time, the total length of time of of care based on time, the total length of time of
the encounter must be documented along with the encounter must be documented along with
the amount of time spent in counseling and the the amount of time spent in counseling and the
content of the counseling sessioncontent of the counseling session
�� Who was presentWho was present
�� What was discussed What was discussed
�� Conclusions metConclusions met
4848
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
�� Subsequent hospital services Subsequent hospital services –– Pay attention to Pay attention to
medical necessity medical necessity –– strongly consider the strongly consider the ““nature nature
of the presenting problemof the presenting problem””
–– 99231 99231 –– usually the patient is stable, recovering or usually the patient is stable, recovering or
improvingimproving
�� A problem focused interval historyA problem focused interval history
�� A problem focus examination (a limited examination of the A problem focus examination (a limited examination of the
affected body area or organ system)affected body area or organ system)
�� Medical decision making that is straightforward or of low Medical decision making that is straightforward or of low
complexitycomplexity
4949
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
–– 99232 99232 –– usually the patient is responding usually the patient is responding
inadequately to therapy or has developed a inadequately to therapy or has developed a
minor complicationminor complication
�� An expanded problem focused interval historyAn expanded problem focused interval history
�� An expanded problem focused examination (a limited An expanded problem focused examination (a limited examination of the affected body area or organ examination of the affected body area or organ
system and other symptomatic or related organ system and other symptomatic or related organ
system(s)system(s)
�� Medical decision making of moderate complexityMedical decision making of moderate complexity
5050
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
–– 99233 99233 –– usually the patient is unstable or has usually the patient is unstable or has
developed a significant complication or developed a significant complication or
significant new problemsignificant new problem
�� A detailed interval historyA detailed interval history
�� A detailed examination (an extended examination of A detailed examination (an extended examination of the affected body area(s) and other symptomatic or the affected body area(s) and other symptomatic or
related organ system(s)related organ system(s)
�� Medical decision making of high complexityMedical decision making of high complexity
5151

CONSULTATIONCONSULTATION
SERVICESSERVICES
5252
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS
�� Consult codes 99251Consult codes 99251--99255 are no longer 99255 are no longer
recognized for Medicare Part B paymentrecognized for Medicare Part B payment
�� In the inpatient hospital setting the initial In the inpatient hospital setting the initial
evaluation by any physician will be 99221evaluation by any physician will be 99221--
9922399223
�� This change will result in multiple billings This change will result in multiple billings
of the initial hospital codeof the initial hospital code
5353
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS
�� Modifier Modifier ““--AIAI”” will be utilized by the admitting will be utilized by the admitting
or attending physician and is identified as or attending physician and is identified as
““Principal Physician of RecordPrincipal Physician of Record””
�� Each time the patient is admitted to the Each time the patient is admitted to the
hospital and a physician provides an initial hospital and a physician provides an initial
evaluation, this code may be usedevaluation, this code may be used
5454
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS�� Even for an established dialysis patient, where a Even for an established dialysis patient, where a
consultation code would not have been consultation code would not have been
appropriate, 99221appropriate, 99221--99223 can be used99223 can be used
�� If the patient also has dialysis on the day of the If the patient also has dialysis on the day of the
initial evaluation (not necessarily the day of initial evaluation (not necessarily the day of
admission) both the 99221admission) both the 99221--99223 99223 and and
90935/37/45/47 can be used 90935/37/45/47 can be used –– append modifier append modifier
““--2525”” to the 99221to the 99221--
9922399223
5555
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS
�� Providers must pay close attention to the Providers must pay close attention to the
complexity level performed when choosing complexity level performed when choosing
the level of service billedthe level of service billed
�� A crosswalk from the consultation codes A crosswalk from the consultation codes
would be:would be:
–– 9925199251--99253 = 99221 (watch documentation 99253 = 99221 (watch documentation
requirements)requirements)
–– 99254 = 9922299254 = 99222
–– 99255 = 9922399255 = 99223
5656
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS
�� Follow up care in the hospital settings use Follow up care in the hospital settings use
the subsequent visits appropriate for the the subsequent visits appropriate for the
locationlocation
�� 9923199231--99233 are used for inpatient 99233 are used for inpatient
hospital followhospital follow--up careup care
5757
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS�� Reminder Reminder –– when using the higher levels of the initial when using the higher levels of the initial
hospital visit codes (99222hospital visit codes (99222--99223) there must be a 99223) there must be a comprehensive history and physical examcomprehensive history and physical exam�� For the history of present illness there must be at least For the history of present illness there must be at least
four of the elements:four of the elements:�� LocationLocation SeveritySeverity QualityQuality
�� Timing ContextTiming Context Modifying factorsModifying factors
�� Associated signs & symptomsAssociated signs & symptoms
�� Past, family and social history obtained at Past, family and social history obtained at thisthis visitvisit
�� At least a 10 organ system review At least a 10 organ system review
�� At least an 8 organ system physical examAt least an 8 organ system physical exam
5858
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS�� Observation care presents some different issuesObservation care presents some different issues
�� Only the physician who Only the physician who ordered ordered the outpatient the outpatient
observation admission may bill the observation observation admission may bill the observation
admission codes 99218admission codes 99218--9922099220
�� Other physicians providing care in the observation Other physicians providing care in the observation
setting are to bill 99201setting are to bill 99201--99205 new 99205 new
office/outpatient visit code or 99211office/outpatient visit code or 99211--99215 99215
established office/outpatient visit code depending established office/outpatient visit code depending
on the status of the patienton the status of the patient’’s relationship with the s relationship with the
evaluating physicianevaluating physician
5959
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS�� Office/outpatient consultation codes (99241Office/outpatient consultation codes (99241--
99245) are also not recognized for Medicare 99245) are also not recognized for Medicare Part B paymentPart B payment
�� Unlike the hospital codes that allow physicians Unlike the hospital codes that allow physicians to bill the inpatient initial hospital care code to bill the inpatient initial hospital care code each time the patient is admitted to the hospital, each time the patient is admitted to the hospital, in the outpatient setting, the provider must in the outpatient setting, the provider must determine if the patient is new or establisheddetermine if the patient is new or established
�� If the patient has been seen by any member of If the patient has been seen by any member of the group during the past 3 years, the patient is the group during the past 3 years, the patient is establishedestablished
6060
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS
�� This care could have been provided in the This care could have been provided in the
inpatient or the outpatient settinginpatient or the outpatient setting
�� If the patient is new to the practice bill 99201If the patient is new to the practice bill 99201--
99205 as appropriate based on the elements and 99205 as appropriate based on the elements and
nature of the presenting problemnature of the presenting problem
�� If the patient has been seen within three years, If the patient has been seen within three years,
regardless of the diagnosis, the patient is regardless of the diagnosis, the patient is
established and you must use 99211established and you must use 99211--9921599215
6161
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS
�� There is a direct crosswalk to these codes There is a direct crosswalk to these codes
making the billing simpliermaking the billing simplier
–– 99241 = 9920199241 = 99201
–– 99242 = 9920299242 = 99202
–– 99243 = 9920399243 = 99203
–– 99244 = 9920499244 = 99204
–– 99245 = 99205 99245 = 99205 –– remember at this level the remember at this level the
intensity of the visit is high intensity of the visit is high
6262
BILLING FOR BILLING FOR
CONSULTATIONSCONSULTATIONS�� Documentation of all elements are required Documentation of all elements are required
including the chief complaint (reason for the visit)including the chief complaint (reason for the visit)
�� I also suggest that the provider continue to I also suggest that the provider continue to
document who requested the document who requested the ““consultationconsultation”” if this if this
is an initial encounter either new or establishedis an initial encounter either new or established
�� If any portion of the encounter is performed by a If any portion of the encounter is performed by a
NPP, and the billing is done under the physicianNPP, and the billing is done under the physician’’s s
provider number, the physician would have to be provider number, the physician would have to be
physically present in the suite and see the patient physically present in the suite and see the patient
as a as a ““sharedshared”” visitvisit
6363

6464
OIG TARGETSOIG TARGETS
““What the What the inspectorsinspectors are looking forare looking for””
OIG WORK PLANOIG WORK PLAN
�� ““The size and scope of the Medicare system The size and scope of the Medicare system
places it at high risk for payment errorsplaces it at high risk for payment errors””
�� OIG audits help to avoid fraud and protect OIG audits help to avoid fraud and protect
the solvency of the Medicare Trust.the solvency of the Medicare Trust.
�� These reviews have revealed payments for These reviews have revealed payments for
unallowable services, improper coding, and unallowable services, improper coding, and
other types of improper payments. other types of improper payments.
6565

6666
2012 TARGETS2012 TARGETS
�� Place of Service ErrorsPlace of Service Errors
�� Incident to ServicesIncident to Services
�� Impact of Opting out of MedicareImpact of Opting out of Medicare
�� Trends in Coding of ClaimsTrends in Coding of Claims
�� E&M during Global Surgical PeriodsE&M during Global Surgical Periods

6767
2012 TARGETS2012 TARGETS
�� Modifiers During Global Surgical Modifiers During Global Surgical
PeriodsPeriods
�� Potentially Inappropriate PaymentsPotentially Inappropriate Payments
6868
2012 TARGETS2012 TARGETS
�� Place of Service ErrorsPlace of Service Errors
–– OIG will determine whether physicians properly coded OIG will determine whether physicians properly coded
the place of service on claims for services provided in the place of service on claims for services provided in
ambulatory surgical centers and hospital outpatient ambulatory surgical centers and hospital outpatient
departments. departments.
–– Medicare regulations provide for different levels of Medicare regulations provide for different levels of
payments to physicians depending on where the service payments to physicians depending on where the service
is performed. is performed.
–– Medicare makes higher payments for physician office Medicare makes higher payments for physician office
services.services.
6969
2012 TARGETS2012 TARGETS�� Incident to ServicesIncident to Services
––OIG will review physician billing for OIG will review physician billing for ““incidentincident--toto”” services services
to determine whether payment for such services had a to determine whether payment for such services had a
higher error rate than that for nonhigher error rate than that for non--incidentincident--to services. to services.
We will also assess CMSWe will also assess CMS’’s ability to monitor services s ability to monitor services
billed as billed as ““incidentincident--to.to.”” Medicare Part B pays for certain Medicare Part B pays for certain
services billed by physicians that are performed by nonservices billed by physicians that are performed by non--
physicians incident to a physician office visit. A 2009 physicians incident to a physician office visit. A 2009
OIG review found that when Medicare allowed OIG review found that when Medicare allowed
physiciansphysicians’’ billings for more than 24 hours of services in billings for more than 24 hours of services in
a day, half of the services were not performeda day, half of the services were not performed
by a physician. by a physician.
2012 TARGETS2012 TARGETS
�� Incident to ServicesIncident to Services–– We also found that unqualified nonWe also found that unqualified non--physicians physicians
performed 21 percent of the services that physicians did performed 21 percent of the services that physicians did
not perform personally. Incidentnot perform personally. Incident--to services represent a to services represent a program vulnerability in that they do not appear in program vulnerability in that they do not appear in
claims data and can be identified only by reviewing the claims data and can be identified only by reviewing the medical record. They may also be vulnerable to medical record. They may also be vulnerable to
overutilization and expose Medicare beneficiaries to overutilization and expose Medicare beneficiaries to
care that does not meet professional standards of care that does not meet professional standards of quality. quality.
7070
2012 TARGETS2012 TARGETS
�� Impact of Opting Out of MedicareImpact of Opting Out of Medicare–– OIG will review the extent to which physicians are opting OIG will review the extent to which physicians are opting
out of Medicare and determine whether physicians who out of Medicare and determine whether physicians who
have opted out of Medicare are submitting claims to have opted out of Medicare are submitting claims to Medicare. We will also examine whether specific areas Medicare. We will also examine whether specific areas
of the country have seen higher numbers of physicians of the country have seen higher numbers of physicians opting out and its potential impact on beneficiaries. opting out and its potential impact on beneficiaries.
Physicians are permitted to enter into private contracts Physicians are permitted to enter into private contracts
with Medicare beneficiaries. (Social Security Act, with Medicare beneficiaries. (Social Security Act, §§1802(b).) As a result of entering into private contracts, 1802(b).) As a result of entering into private contracts,
physicians must commit that they will not submit a claim physicians must commit that they will not submit a claim to Medicare for any Medicare beneficiary. to Medicare for any Medicare beneficiary.
7171
2012 TARGETS2012 TARGETS�� Trends in Coding of Claims Trends in Coding of Claims
–– OIG will review evaluation and management (E/M) OIG will review evaluation and management (E/M) claims to identify trends in the coding of E/M services claims to identify trends in the coding of E/M services
from 2000from 2000--2009. We will also identify providers that 2009. We will also identify providers that exhibited questionable billing for E/M services in 2009. exhibited questionable billing for E/M services in 2009.
Medicare paid $32 billion for E/M services in 2009, Medicare paid $32 billion for E/M services in 2009, representing 19 percent of all Medicare Part B representing 19 percent of all Medicare Part B
payments. Providers are responsible for ensuring that payments. Providers are responsible for ensuring that
the codes they submit accurately reflect the services the codes they submit accurately reflect the services they provide. E/M codes represent the type, setting, and they provide. E/M codes represent the type, setting, and
complexity of services provided and the patient status, complexity of services provided and the patient status, such as new or established. such as new or established.
(CMS(CMS’’s s Medicare Claims Processing Manual, Pub. No. Medicare Claims Processing Manual, Pub. No.
100100--04, ch. 12, 04, ch. 12, §§ 30.6.1.)30.6.1.)7272
2012 TARGETS2012 TARGETS�� Evaluation and Management Services Evaluation and Management Services
Provided During Global Surgery PeriodsProvided During Global Surgery Periods–– OIG will review industry practices related to the number OIG will review industry practices related to the number
of E/M services provided by physicians and reimbursed of E/M services provided by physicians and reimbursed as part of the global surgery fee to determine whether as part of the global surgery fee to determine whether
the practices have changed since the global surgery fee the practices have changed since the global surgery fee
concept was developed in 1992. Under the global concept was developed in 1992. Under the global surgery fee concept, physicians bill a single fee for all of surgery fee concept, physicians bill a single fee for all of
their services that are usually associated with a surgical their services that are usually associated with a surgical procedure and related E/M services provided during the procedure and related E/M services provided during the
global surgery period.global surgery period.
Medicare Claims Processing Manual, Pub. 100Medicare Claims Processing Manual, Pub. 100--04, ch. 12, 04, ch. 12, §§ 40.40.
7373
2012 TARGETS2012 TARGETS�� Use of Modifiers During the Global Use of Modifiers During the Global
Surgery Period Surgery Period –– OIG will review the appropriateness of the use of certain OIG will review the appropriateness of the use of certain
claims modifier codes during the global surgery period claims modifier codes during the global surgery period and determine whether Medicare payments for claims and determine whether Medicare payments for claims
with modifiers used during the global surgery period with modifiers used during the global surgery period
were in accordance with Medicare requirements. Prior were in accordance with Medicare requirements. Prior OIG work has shown that improper use of modifiers OIG work has shown that improper use of modifiers
during the global surgery period resulted in during the global surgery period resulted in inappropriate payments. The global surgery payment inappropriate payments. The global surgery payment
includes a surgical service and related preoperative and includes a surgical service and related preoperative and
postoperative E/M services provided during the global postoperative E/M services provided during the global surgery period. surgery period.
Medicare Claims Processing Manual, Pub. 100Medicare Claims Processing Manual, Pub. 100--04, ch. 12, 04, ch. 12, §§ 40.1. 40.1. 7474
2012 TARGETS2012 TARGETS
�� Potentially Inappropriate PaymentsPotentially Inappropriate Payments–– OIG will assess the extent to which CMS made potentially OIG will assess the extent to which CMS made potentially
inappropriate payments for E/M services and the inappropriate payments for E/M services and the
consistency of E/M medical review determinations. We will consistency of E/M medical review determinations. We will
also review multiple E/M services for the same providers also review multiple E/M services for the same providers
and beneficiaries to identify electronic health records and beneficiaries to identify electronic health records
(EHR) documentation practices associated with potentially (EHR) documentation practices associated with potentially
improper payments. Medicare contractors have noted an improper payments. Medicare contractors have noted an
increased frequency of medical records with identical increased frequency of medical records with identical
documentation across services. Medicare requires documentation across services. Medicare requires
providers to select the code for the service based upon the providers to select the code for the service based upon the
content of the service and have documentation to support content of the service and have documentation to support
the level of service reported. the level of service reported.
7575
7676
END STAGE RENAL DISEASEEND STAGE RENAL DISEASE
PHYSICIAN COMPENSATIONPHYSICIAN COMPENSATION
BILLING FOR THE MONTHLY BILLING FOR THE MONTHLY CAPITATION PAYMENTCAPITATION PAYMENT
MCPMCP

REGULATIONSREGULATIONS
�� Conditions of coverage?? orConditions of coverage?? or
�� MCP??MCP??
�� Are there conflicting regulations?Are there conflicting regulations?
�� Which should be followed?Which should be followed?
7777
7878
MEDICARE AND ESRDMEDICARE AND ESRD
““A match made in CongressA match made in Congress””
7979
ESRD DEFINEDESRD DEFINED
�� Medicare regulations define ESRD as Medicare regulations define ESRD as ““that that
stage of kidney impairment that appears stage of kidney impairment that appears
irreversible and permanent and requires a irreversible and permanent and requires a
regular course of dialysis treatment or kidney regular course of dialysis treatment or kidney
transplantation to survivetransplantation to survive””..
�� 1972, Congress changed the Social Security 1972, Congress changed the Social Security
Act to instruct CMS to pay the cost of treating Act to instruct CMS to pay the cost of treating
ESRD via Medicare eligibilityESRD via Medicare eligibility
8080
MEDICARE ENTITLEMENT DATE MEDICARE ENTITLEMENT DATE --
ESRDESRD
�� Entitlement begins after completion of three Entitlement begins after completion of three
month waiting period for inmonth waiting period for in--center patientscenter patients
�� Waiting period waived for home dialysisWaiting period waived for home dialysis
�� Waiting period also waived for transplantsWaiting period also waived for transplants
8181
MEDICARE SECONDARY PAYERMEDICARE SECONDARY PAYER
(MSP)(MSP)
�� Beneficiary is workingBeneficiary is working
�� Beneficiary is disabledBeneficiary is disabled
�� Completion of coordination periodCompletion of coordination period–– 30 months as Medicare Secondary 30 months as Medicare Secondary
–– Primary coverage must be an employer group Primary coverage must be an employer group planplan
8282
MONTHLY CAPITATION PAYMENTMONTHLY CAPITATION PAYMENT
�� CMS method to reimburse Nephrologists CMS method to reimburse Nephrologists
for all outpatient care of patients with for all outpatient care of patients with
ESRDESRD
�� MCP is comprehensive, per patient, per MCP is comprehensive, per patient, per
month payment for month payment for allall outpatient renaloutpatient renal--
related carerelated care
8383
MONTHLY CAPITATION PAYMENTMONTHLY CAPITATION PAYMENT
Not included in MCP:Not included in MCP:
�� NonNon--renal related evaluation and renal related evaluation and
managementmanagement
�� Hospital inpatient servicesHospital inpatient services
�� All nonAll non--renal proceduresrenal procedures
�� Evaluation for transplant or LRD evaluationEvaluation for transplant or LRD evaluation
�� Training of patients to perform home Training of patients to perform home
dialysisdialysis
8484
MONTHLY CAPITATION PAYMENTMONTHLY CAPITATION PAYMENT
Included in the MCPIncluded in the MCP
�� All renalAll renal--related related outpatientoutpatient services rendered services rendered
to the dialysis patientto the dialysis patient
�� Interpretation of ancillary testing (nerve Interpretation of ancillary testing (nerve
conduction studies, bone density, doppler conduction studies, bone density, doppler
studies)studies)
�� Services rendered to the dialysis patient while Services rendered to the dialysis patient while
on dialysison dialysis
�� Physicals required by the dialysis facility for the Physicals required by the dialysis facility for the
renal patientrenal patient
MONTHLY CAPITATION MONTHLY CAPITATION
PAYMENTPAYMENT
Included in the MCPIncluded in the MCP
�� Certification of the need for items & Certification of the need for items &
services such as DME & home health careservices such as DME & home health care
�� Care plan oversight services described by Care plan oversight services described by
CPT code 99375 CPT code 99375
8585
8686
MONTHLY CAPITATION PAYMENTMONTHLY CAPITATION PAYMENTIncluded in the MCPIncluded in the MCP
�� Periodic visits to the patient during dialysis to Periodic visits to the patient during dialysis to
determine if the dialysis is working well both determine if the dialysis is working well both
physiologically & psychologically. During this physiologically & psychologically. During this
encounter the physician will determine if any encounter the physician will determine if any
elements of the plan need to be revised to elements of the plan need to be revised to
optimize the patientoptimize the patient’’s treatment and/or care. s treatment and/or care.
�� Coordination & direction of the multiCoordination & direction of the multi--
disciplinary team involved in the patientdisciplinary team involved in the patient’’ss
care.care.
8787
OUTPATIENT SETTINGSOUTPATIENT SETTINGS
�� The MCP covers all The MCP covers all outpatientoutpatient services services
related to the patientrelated to the patient’’s renal conditions renal condition
�� Services may be rendered in the inServices may be rendered in the in--center center
dialysis unit, patientdialysis unit, patient’’s home, practitioners home, practitioner’’s s
office, outpatient hospital, observation care, office, outpatient hospital, observation care,
emergency room and outpatient surgeryemergency room and outpatient surgery
–– Inpatient services cannot count as MCP Inpatient services cannot count as MCP
encountersencounters
8888
PRACTITIONER DEFINITIONSPRACTITIONER DEFINITIONS
�� MCP physician is the MCP physician is the physician physician who performs who performs
the the ““majormajor”” (care plan) visit during the month. (care plan) visit during the month.
This physician is the billing physicianThis physician is the billing physician
�� NonNon--physician practitioner physician practitioner –– NP/PA who is NP/PA who is
employed by the same entity as the physicianemployed by the same entity as the physician
–– Must be able under statute to furnish services that Must be able under statute to furnish services that
would be physician serviceswould be physician services
�� NonNon--MCP physician MCP physician –– must have a relationship must have a relationship
with the MCP physician such as partnerwith the MCP physician such as partner
8989
USE OF NONUSE OF NON--PHYSICIAN PHYSICIAN
PRACTITIONERSPRACTITIONERS�� MCPMCP physician (billing physician) must provide physician (billing physician) must provide
the visit with the complete assessment of the the visit with the complete assessment of the
patient, establish the plan of care, and submit patient, establish the plan of care, and submit
the bill for the monthly servicethe bill for the monthly service –– Must see the Must see the
patient at least once a monthpatient at least once a month
–– NonNon--physicians can provide some of the visits to physicians can provide some of the visits to
equal total # submittedequal total # submitted
–– Non MCP physician can provide some of the visitsNon MCP physician can provide some of the visits
–– NonNon--physician must have a relationship with the physician must have a relationship with the
physician (employee) physician (employee)
9090
PARTIAL MONTH RULEPARTIAL MONTH RULE
�� 9096790967--90970 ESRD related services for dialysis 90970 ESRD related services for dialysis less than a full month of service less than a full month of service
�� Use limited to:Use limited to:–– Transient patientsTransient patients
–– Home dialysis patientsHome dialysis patients–– Patients who have a permanent change in their MCP Patients who have a permanent change in their MCP
physician during the monthphysician during the month–– Partial month with one or more facePartial month with one or more face--toto--face visits face visits
without the complete (care plan) visit but only in patients without the complete (care plan) visit but only in patients withwith�� Dialysis stopped due to death. Dialysis stopped due to death. �� Dialysis patient transplantedDialysis patient transplanted�� Dialysis patient hospitalized during the monthDialysis patient hospitalized during the month

9191
PARTIAL MONTH RULEPARTIAL MONTH RULE
(cont.)(cont.)
�� Partial month rule Partial month rule does notdoes not apply to apply to
patients who start dialysis during the monthpatients who start dialysis during the month
�� Without a complete (care plan) visit, these Without a complete (care plan) visit, these
patients cannot be billed for this first month patients cannot be billed for this first month
on dialysison dialysis
�� Cannot bill 90967Cannot bill 90967--9097090970
9292
TRANSIENT PATIENTSTRANSIENT PATIENTS
�� Only one physician can bill for the management of Only one physician can bill for the management of
a patient per montha patient per month
�� Bill 90970 for the number of days the patient is Bill 90970 for the number of days the patient is
under the transient physicianunder the transient physician’’s cares care
�� If the transient patient is in the transient dialysis If the transient patient is in the transient dialysis
unit for a full month, then the same rules apply as unit for a full month, then the same rules apply as
with any other inwith any other in--center patient. Transient MD center patient. Transient MD
becomes MCP physicianbecomes MCP physician
9393
PATIENTS WITH LESS THAN A PATIENTS WITH LESS THAN A
FULL MONTH MCPFULL MONTH MCP�� Bill as if the patient had a full month of Bill as if the patient had a full month of
dialysis with the appropriate CPT code for dialysis with the appropriate CPT code for
the number of encounters if:the number of encounters if:
–– Dies during the monthDies during the month
–– Transplants during the month Transplants during the month
–– Transfers during the monthTransfers during the month
–– HospitalizedHospitalized
Patient must have Patient must have complete (care plan) visitcomplete (care plan) visit to to
bill using the appropriate CPT codebill using the appropriate CPT code
9494
HOSPITAL OBSERVATION HOSPITAL OBSERVATION
STATUSSTATUS
�� ESRDESRD--related visits furnished in hospital related visits furnished in hospital
observation status count as an MCP observation status count as an MCP
encounter encounter
�� Visit will count towards the total number of Visit will count towards the total number of
encounters submitted (CPT code)encounters submitted (CPT code)
�� Describe (document) in the medical record Describe (document) in the medical record
the type of ESRDthe type of ESRD--related service rendered related service rendered
in observation statusin observation status
9595
HOSPITALIZATION & THE MCPHOSPITALIZATION & THE MCP
ININ--CENTER PATIENTSCENTER PATIENTS
�� ESRD patients, other than home dialysis patients, ESRD patients, other than home dialysis patients,
hospitalized during the month will be billed for the hospitalized during the month will be billed for the
number of facenumber of face--toto--face encounters that occurred face encounters that occurred
when the patient was when the patient was notnot in the hospitalin the hospital
�� Since the MCP is no longer Since the MCP is no longer ““timetime”” dependent, but dependent, but
based on encounters facebased on encounters face--toto--face, the face, the
practitioners no longer practitioners no longer ““carve outcarve out”” hospital days.hospital days.
�� Bill inpatient care Bill inpatient care andand the CPT code for the the CPT code for the
number of outpatient facenumber of outpatient face--toto--face encountersface encounters
9696
HOME DIALYSISHOME DIALYSIS
�� Payment based on 2Payment based on 2--3 visit payment level 3 visit payment level
approximately $221.66approximately $221.66
�� Monthly visit is the Monthly visit is the REQUIREDREQUIRED in 2011 in 2011 –– bill using bill using
full month code 90966 for 20+ years old)full month code 90966 for 20+ years old)
�� If patient has less than full month at homeIf patient has less than full month at home–– bill bill
using by day code 90970 for 20+ years old)using by day code 90970 for 20+ years old)
�� Home patients are billed similarly to how MCP was Home patients are billed similarly to how MCP was
billed historicallybilled historically
9797
HOME DIALYSIS HOME DIALYSIS (cont)(cont)
�� If the home patient receives inIf the home patient receives in--center center
dialysis during the month, the provider dialysis during the month, the provider
would still bill the management fee for the would still bill the management fee for the
month under the home dialysis provisionmonth under the home dialysis provision
�� The physician cannot bill the inThe physician cannot bill the in--center CPT center CPT
code code oror CPT 90935CPT 90935--90937 for the 90937 for the
encounters inencounters in--centercenter
9898
HOSPITALIZATION & THE MCPHOSPITALIZATION & THE MCP
HOME DIALYSISHOME DIALYSIS
�� Home patients continue to be billed in a Home patients continue to be billed in a
full month or partial month format similar full month or partial month format similar
to prior codes to prior codes
�� If the patient is home for the 1If the patient is home for the 1stst --1010thth
hospitalized from the 11hospitalized from the 11thth--2020thth, then back , then back
home from the 21home from the 21stst--3030thth, you would bill for , you would bill for
the 90970 (adult) for the 1the 90970 (adult) for the 1--10 (10 days), 10 (10 days),
inpatient codes for 11inpatient codes for 11--20, then 90970 for 20, then 90970 for
the 21the 21--30 (10 days)30 (10 days)
9999
MODALITY CHANGESMODALITY CHANGES
�� If a patient switches modalities during the If a patient switches modalities during the
month, bill the entire month using the month, bill the entire month using the
appropriate appropriate HOMEHOME dialysis code 90963dialysis code 90963--
9096690966
�� If partial month care bill using 90967If partial month care bill using 90967--9097090970
100100
DOCUMENTATION DOCUMENTATION
REQUIREMENTSREQUIREMENTS
�� CMS stopped short of dictating CMS stopped short of dictating documentation requirements however were documentation requirements however were very specific on what was necessaryvery specific on what was necessary
�� With requirements now for verification of With requirements now for verification of physicianphysician’’s face to face visits, s face to face visits, documentation of encounters will be documentation of encounters will be necessarynecessary
�� RPA documentation tool has been revised RPA documentation tool has been revised to meet CMS recommendationsto meet CMS recommendations
101101
DOCUMENTATION REQUIREMENTS DOCUMENTATION REQUIREMENTS
(cont)(cont)
�� Document what is clinically relevant iDocument what is clinically relevant includingncluding
but but not limitednot limited to:to:
–– patient's current status and complaints, patient's current status and complaints,
–– a clinically appropriate physical examination, a clinically appropriate physical examination, assessment of the patient's treatment for ESRD that assessment of the patient's treatment for ESRD that
includes assessment of the adequacy of the dialysis includes assessment of the adequacy of the dialysis treatment, the status of the patient's vascular treatment, the status of the patient's vascular
access, assessment and treatment of the other access, assessment and treatment of the other
conditions associated with ESRD, such as anemia, conditions associated with ESRD, such as anemia, electrolyte management, and bone density, as well electrolyte management, and bone density, as well
as changes to the patient's managementas changes to the patient's management
102102
ADDITIONAL DOCUMENTATION ADDITIONAL DOCUMENTATION
NEEDED FOR PEDIATRIC NEEDED FOR PEDIATRIC
PATIENTSPATIENTS
�� In addition to the requirements for adult In addition to the requirements for adult patients, pediatric nephrologists also need to:patients, pediatric nephrologists also need to:
–– Monitor the patient for adequacy of nutritionMonitor the patient for adequacy of nutrition
–– Assess for growth and developmentAssess for growth and development
–– Counsel parentsCounsel parents
Documentation must show these elements Documentation must show these elements
In addition to the adult documentation In addition to the adult documentation requirementsrequirements
103103
CHANGES IN DOCUMENTATION CHANGES IN DOCUMENTATION
REQUIREMENTS (cont)REQUIREMENTS (cont)
�� Documentation of the complete (care plan)Documentation of the complete (care plan)visit is requiredvisit is required
�� Documentation that the physician Documentation that the physician performed a service for the patient is performed a service for the patient is required for the other encountersrequired for the other encounters
�� Signing a dialysis flow sheet or any other Signing a dialysis flow sheet or any other form if not enoughform if not enough……the physician must the physician must document they are performing a service at document they are performing a service at each encountereach encounter
104104
MCP CONCLUSIONSMCP CONCLUSIONS
�� Documentation will be key in managing new Documentation will be key in managing new
MCP changesMCP changes
�� Administrative challenges will create additional Administrative challenges will create additional
requirements for excellent record keepingrequirements for excellent record keeping
�� Complete visit, including disease appropriate Complete visit, including disease appropriate
physical exam is necessary to bill the inphysical exam is necessary to bill the in--center center
CPT codeCPT code
105105
NEPHROLOGYNEPHROLOGY
SPECIFICSPECIFIC
CPT CPT
CODINGCODING
106106
INPATIENT DIALYSIS CODESINPATIENT DIALYSIS CODES
�� 9093590935 -- Single physician evaluation of Single physician evaluation of
hemodialysishemodialysis
�� 9093790937 -- Multiple physician evaluation of Multiple physician evaluation of
hemodialysishemodialysis
�� 9094590945 -- Single physician evaluation of Single physician evaluation of
continuous forms of dialysiscontinuous forms of dialysis
�� 9094790947 -- Multiple physician evaluation of Multiple physician evaluation of
continuous forms of dialysiscontinuous forms of dialysisIncludes E&M services rendered on the same dayIncludes E&M services rendered on the same day
107107
INPATIENT DIALYSIS CODESINPATIENT DIALYSIS CODES
To bill physician must meet the following:To bill physician must meet the following:
�� Be present Be present duringduring the dialysis treatmentthe dialysis treatment
�� Documentation must reflect presence during Documentation must reflect presence during
the treatmentthe treatment
�� The need for repeated visit should be noted The need for repeated visit should be noted
in the patientin the patient’’s chart. The note should s chart. The note should
include the problem or anticipated problem include the problem or anticipated problem
which required the physicianwhich required the physician’’s repeat s repeat
evaluationevaluation
108108
INPATIENT DIALYSIS CODESINPATIENT DIALYSIS CODES
Four E/M services that can be billed on the Four E/M services that can be billed on the same day as dialysis services rendered same day as dialysis services rendered in the inpatient settingin the inpatient setting
�� Hospital admissionHospital admission�� Hospital dischargeHospital discharge�� Inpatient consultation (for commercial Inpatient consultation (for commercial
payers only)payers only)�� Critical CareCritical Care
–– Most carriers require the use of a Most carriers require the use of a ““--2525”” modifier modifier on the E/M code on the same day as a on the E/M code on the same day as a procedure procedure

109109
HOSPICEHOSPICE
SERVICESSERVICES
110110
WHAT IS HOSPICE?WHAT IS HOSPICE?�� Hospice is a program of care and support for Hospice is a program of care and support for
people who are terminally illpeople who are terminally ill
�� To get Hospice benefits from Medicare the patient To get Hospice benefits from Medicare the patient
must meet must meet all all of the following conditionsof the following conditions: : –– Be eligible for Medicare Part A (Hospital Insurance). Be eligible for Medicare Part A (Hospital Insurance).
–– The patientThe patient’’s doctor and the hospice medical director certify that the s doctor and the hospice medical director certify that the patient is terminally ill and has 6 months or less to live if thpatient is terminally ill and has 6 months or less to live if their illness eir illness runs its normal course. runs its normal course.
–– The patient must sign a statement choosing hospice care instead The patient must sign a statement choosing hospice care instead of of other Medicareother Medicare--covered benefits to treat the terminal illness. covered benefits to treat the terminal illness. *Medicare will still pay for covered benefits for any health pro*Medicare will still pay for covered benefits for any health problems blems that arenthat aren’’t related to the terminal illness. t related to the terminal illness.
–– Care comes from a MedicareCare comes from a Medicare--approved hospice program. approved hospice program.
WHO DO YOU BILL FOR WHO DO YOU BILL FOR
SERVICES?SERVICES?
�� Hospice pays for all care related to the Hospice pays for all care related to the
hospice conditionhospice condition
�� The patient must use standard Medicare to The patient must use standard Medicare to
cover any health care not related to the cover any health care not related to the
terminal conditionterminal condition
�� ““GVGV”” modifier is used to bill Medicare by the modifier is used to bill Medicare by the
attending physician not employed by a attending physician not employed by a
hospice for the evaluation and treatment of hospice for the evaluation and treatment of
a terminal conditiona terminal condition111111
WHO DO YOU BILL FOR WHO DO YOU BILL FOR
SERVICES?SERVICES?
�� Any physician providing services to the Any physician providing services to the
hospice patient for the terminal condition hospice patient for the terminal condition
other than the attending must have a other than the attending must have a
contract with the hospice and bill to the contract with the hospice and bill to the
hospicehospice
�� ““GWGW”” modifier is used to report all physician modifier is used to report all physician
services to services to MedicareMedicare that are unrelated to a that are unrelated to a
patientpatient’’s terminal conditions terminal condition
112112
113113
HOME DIALYSIS HOME DIALYSIS
TRAININGTRAINING
114114
HOME TRAINING DIALYSIS HOME TRAINING DIALYSIS
MANAGEMENTMANAGEMENT
�� 9098990989 -- Dialysis training, patient, including Dialysis training, patient, including helper where applicable, any mode, helper where applicable, any mode, complete coursecomplete course
�� 9099390993 -- Dialysis training, patient, including Dialysis training, patient, including helper where applicable, any mode, course helper where applicable, any mode, course not completed, per training session (billed not completed, per training session (billed by units completed)by units completed)
�� Physician Physician mustmust have direct participation in have direct participation in the training to bill the training to bill
115115
HOME TRAINING DIALYSIS HOME TRAINING DIALYSIS
MANAGEMENTMANAGEMENT
�� Example of billing for trainingExample of billing for training
–– Patient on hemodialysis March 1Patient on hemodialysis March 1--15, 201115, 2011�� Seen with comprehensive visit 2 timesSeen with comprehensive visit 2 times
–– Patient began home PD training March 16 Patient began home PD training March 16
continued through March 21, 2011. continued through March 21, 2011. �� Physician participated directly in training Physician participated directly in training –– 90989, PD training 90989, PD training
complete, March 16,17,19,20,21, 2011complete, March 16,17,19,20,21, 2011
–– Patient at home for the full month (90963Patient at home for the full month (90963--
90966)90966)
116116
HOME TRAINING DIALYSIS HOME TRAINING DIALYSIS
MANAGEMENTMANAGEMENT
�� A completed course is reimbursed with a A completed course is reimbursed with a
maximum $500 allowablemaximum $500 allowable
�� A completed course should be reported with A completed course should be reported with
90989 with a quantity of 90989 with a quantity of ““oneone””
�� For a training course not completed bill For a training course not completed bill
90993 for the number of sessions completed 90993 for the number of sessions completed
and reimbursed at a $20 per session and reimbursed at a $20 per session
allowableallowable
117117
BILLING FOR BILLING FOR
ERYTHROPOIETIC STIMULATINGERYTHROPOIETIC STIMULATING
AGENTSAGENTS
CAUTION!CAUTION!
�� POLICIES CHANGE QUICKLY!!POLICIES CHANGE QUICKLY!!
�� Please review your own carriers LCD on a Please review your own carriers LCD on a
monthly basis.monthly basis.
�� Knowledge in this arena is vital. Knowledge in this arena is vital.
�� An ounce of preventionAn ounce of prevention………………..
118118
119119
�� Pretreatment HCT Pretreatment HCT
Level of less than 30Level of less than 30
�� Creatinine of 3.0 or Creatinine of 3.0 or
greater greater OROR
�� Documented renal Documented renal
insufficiency (stage insufficiency (stage
33--5)5)
�� PatientPatient’’s current s current
weight in kilogramsweight in kilograms
�� Date of lab (within 7 Date of lab (within 7
days days -- this may vary this may vary
by location)by location)Please understand this is an example Please understand this is an example
& not intended to be taken as & not intended to be taken as
policy!policy!
INITIAL PROCRITINITIAL PROCRIT®® (Epoetin Alfa) & (Epoetin Alfa) &
ARANESPARANESP®® (Darbepoetin Alfa)(Darbepoetin Alfa)
ADMINISTRATION ADMINISTRATION EXAMPLEEXAMPLE GUIDELINESGUIDELINES
120120
FOLLOWFOLLOW--UP PROCRITUP PROCRIT®® (Epoetin Alfa) (Epoetin Alfa)
ARANESPARANESP®® (Darbepoetin Alfa)(Darbepoetin Alfa)
ADMINISTRATION ADMINISTRATION EXAMPLE EXAMPLE GUIDELINESGUIDELINES
�� Current HCT level to max of 30 or multiply of Current HCT level to max of 30 or multiply of
Hgb x 3 (watch the LCD, this level varies by Hgb x 3 (watch the LCD, this level varies by
state)state)
�� Date of Laboratory Data (within the last 30 Date of Laboratory Data (within the last 30
days)days)
�� ICDICD--9 code appropriate for state9 code appropriate for state
121121
BILLING FOR ADMINISTRATION OF BILLING FOR ADMINISTRATION OF
PROCRIT AND ARANESPPROCRIT AND ARANESP
�� Drug and administration is covered Drug and administration is covered ““incident incident
toto”” physician service physician service
�� If the purpose of the visit is for an injection, If the purpose of the visit is for an injection,
use 96372 for the subcutaneous use 96372 for the subcutaneous
administration of either Procrit or Aranespadministration of either Procrit or Aranesp
�� 99211 is only used when another service, 99211 is only used when another service,
not protocol for the injection, is providednot protocol for the injection, is provided
122122
BILLING FOR ADMINISTRATION OF BILLING FOR ADMINISTRATION OF
PROCRIT AND ARANESPPROCRIT AND ARANESP
�� When the drug is administered When the drug is administered ““incident toincident to”” a a
physicianphysician’’s visit, bill the appropriate level of s visit, bill the appropriate level of
E&M for the physician visit with a E&M for the physician visit with a ““--2525””
modifier (CCI edit effective 10/1/05), the modifier (CCI edit effective 10/1/05), the
administration fee 96372 and the drug. administration fee 96372 and the drug.
�� REMEMBERREMEMBER: The provider must be : The provider must be
physically present in the suite when the physically present in the suite when the
injection is given to bill for the administration injection is given to bill for the administration
or the drugor the drug
123123
““INCIDENT TOINCIDENT TO”” AND AND
““SHAREDSHARED”” SERVICE SERVICE
BILLINGBILLING
““GETTING THE MOST FROM GETTING THE MOST FROM
THE WORK PHYSICIAN THE WORK PHYSICIAN
EXTENDERS PERFORMEXTENDERS PERFORM””
BILLING OPTIONS FOR NPPsBILLING OPTIONS FOR NPPs
�� NPPs own provider number receiving 85% NPPs own provider number receiving 85%
of the MPFS (Medicare Physicianof the MPFS (Medicare Physician’’s Fee s Fee
Schedule) amountSchedule) amount
�� ““IncidentIncident--toto”” the physician receiving 100% of the physician receiving 100% of
the MPFSthe MPFS
�� Split/Shared service rendering 100% of Split/Shared service rendering 100% of
MPFSMPFS
124124
125125
WHAT IS WHAT IS ““INCIDENT TOINCIDENT TO””
�� Incident to services are:Incident to services are:
–– Services performed by nonServices performed by non--physician practitionersphysician practitioners
–– Services paid as physicianServices paid as physician’’s servicess services
�� ““Furnished as a Furnished as a partpart of the physicianof the physician’’s personal, s personal,
professional service in the course of diagnosis or professional service in the course of diagnosis or
treatment of an injury or illnesstreatment of an injury or illness””
–– Medicare Benefits Policy Manual, Chapter 15, Section Medicare Benefits Policy Manual, Chapter 15, Section
60.160.1
126126
REQUIREMENTS FOR REQUIREMENTS FOR ““INCIDENT INCIDENT
TO BILLINGTO BILLING””
�� Services must be of the type that would be Services must be of the type that would be
covered by Medicare if rendered by a covered by Medicare if rendered by a
physicianphysician
�� Services must be of the type that an NP or Services must be of the type that an NP or
PA can perform under state statute as PA can perform under state statute as
defined in scope of practicedefined in scope of practice
�� Services must be performed under direct Services must be performed under direct
supervision by the physiciansupervision by the physician
127127
REQUIREMENTS FOR REQUIREMENTS FOR ““INCIDENT INCIDENT
TO BILLINGTO BILLING””
�� Cost of the Cost of the ““Incident toIncident to”” services must be services must be
incurred by the entity that bills for the incurred by the entity that bills for the
serviceservice
�� Medicare does not cover services that are Medicare does not cover services that are
not medically necessary or are not of the not medically necessary or are not of the
type of service that would normally be type of service that would normally be
performed in the physicianperformed in the physician’’s offices office
128128
REQUIREMENTS FOR REQUIREMENTS FOR ““INCIDENT INCIDENT
TO BILLINGTO BILLING””
�� NP or PA must be an employee of the NP or PA must be an employee of the
physician or groupphysician or group
�� Applies only to office servicesApplies only to office services
�� Physician must be physically present in the Physician must be physically present in the
office suite to qualify, even if the physician office suite to qualify, even if the physician
does not personally see the patientdoes not personally see the patient
129129
REQUIREMENTS FOR REQUIREMENTS FOR ““INCIDENT INCIDENT
TO BILLINGTO BILLING””
�� ““The availability of a physician by telephone The availability of a physician by telephone and the presence of the physician and the presence of the physician somewhere in the institution does not somewhere in the institution does not constitute direct supervisionconstitute direct supervision””–– Medicare Benefit Policy Manual, Chapter 15, Medicare Benefit Policy Manual, Chapter 15,
Section 60.1.BSection 60.1.B
If the nonIf the non--physician practitioner outpatient service physician practitioner outpatient service does not meet all the qualifications of does not meet all the qualifications of ““incident incident toto”” bill under the NP or PA at 85%bill under the NP or PA at 85%
REQUIREMENTS FOR REQUIREMENTS FOR
““INCIDENT TO BILLINGINCIDENT TO BILLING””
�� RememberRemember…….. Incident.. Incident--to cannot be for new to cannot be for new
patient visitspatient visits
�� ““Incident toIncident to”” must be an integral part of the must be an integral part of the
physicianphysician’’s established plan of care for the s established plan of care for the
patientpatient
�� Does not apply cover new problems Does not apply cover new problems
130130
131131
SHARED SERVICE BILLINGSHARED SERVICE BILLING
�� Services provided by both the physician and the Services provided by both the physician and the
extender in the hospital settingextender in the hospital setting
�� Each provider must document the faceEach provider must document the face--toto--face face
services renderedservices rendered
�� If NP or PA does dictation for services, If NP or PA does dictation for services,
documentation must show that both providers saw documentation must show that both providers saw
the patient and the patient and ““sharedshared”” in the patientin the patient’’s cares care
�� Statement of Statement of ““Sally Jones, NP for Dr. Sam SmithSally Jones, NP for Dr. Sam Smith””
is not adequate to show physicianis not adequate to show physician’’s involvements involvement
SHARED SERVICE BILLINGSHARED SERVICE BILLING
�� Cannot report shared service in the skilled Cannot report shared service in the skilled
nursing facility (SNF) or nursing facility (NF) nursing facility (SNF) or nursing facility (NF)
settingsetting
�� Each provider (physician & NPP) must Each provider (physician & NPP) must
personally perform a substantive portion of personally perform a substantive portion of
the E/M visitthe E/M visit……faceface--toto--faceface……with the same with the same
patient on the same daypatient on the same day
�� The physician & the NPP must be a member The physician & the NPP must be a member
of the same practiceof the same practice132132
SHARED SERVICE BILLING SHARED SERVICE BILLING
EXAMPLESEXAMPLES
�� NPP sees the hospital inpatient early in the NPP sees the hospital inpatient early in the
day and the physician follows with a later day and the physician follows with a later
faceface--toto--face encounter. This service may be face encounter. This service may be
reported by either the physician or the NPPreported by either the physician or the NPP
133133
DOCUMENTATION OF DOCUMENTATION OF
SPLIT/SHARED BILLINGSPLIT/SHARED BILLING
�� Each physician/NPP should personally Each physician/NPP should personally
document in the medical record his/her document in the medical record his/her
portion of the E/M split/shared visitportion of the E/M split/shared visit
�� The physicianThe physician’’s documentation must show s documentation must show
faceface--toto--face componentface component……suggest examsuggest exam
�� Documentation must support the combined Documentation must support the combined
service level reported on the claimservice level reported on the claim
�� Staff may document ROS & PFSH but the Staff may document ROS & PFSH but the
physician & NPP must show reviewphysician & NPP must show review134134
EXAMPLES OF UNACCEPTABLE EXAMPLES OF UNACCEPTABLE
DOCUMENTATIONDOCUMENTATION
�� Agree with aboveAgree with above
�� Rounded, reviewed, agreeRounded, reviewed, agree
�� Discussed with NPP agreeDiscussed with NPP agree
�� Seen & agreeSeen & agree
�� Patient seen and evaluatedPatient seen and evaluated
�� Legible CountersignatureLegible Countersignature
135135
EXAMPLES OF ACCEPTABLE EXAMPLES OF ACCEPTABLE
DOCUMENTATIONDOCUMENTATION
�� I performed a history & PE of the patient and I performed a history & PE of the patient and
discussed his management with the NPP. I discussed his management with the NPP. I
reviewed the NPP note & I agree with the reviewed the NPP note & I agree with the
documented findings and plan of care.documented findings and plan of care.
�� I saw and evaluated the patient. I reviewed I saw and evaluated the patient. I reviewed
the NPPthe NPP’’s note and agree except that s note and agree except that
picture is more consistent with acute tubular picture is more consistent with acute tubular
necrosis. Will begin XYZ therapy.necrosis. Will begin XYZ therapy.
136136
EXAMPLES OF ACCEPTABLE EXAMPLES OF ACCEPTABLE
DOCUMENTATIONDOCUMENTATION
�� I saw and evaluated the patient. Agree with I saw and evaluated the patient. Agree with
the NPPthe NPP’’s note but lower extremity edema is s note but lower extremity edema is
increased. Will increase lasix and monitor increased. Will increase lasix and monitor
closelyclosely
137137
138138
EXTENDERS AND THE MCPEXTENDERS AND THE MCP
�� Can provide some of the visits to equate to the Can provide some of the visits to equate to the
total billedtotal billed
�� Watch any state regulations that may applyWatch any state regulations that may apply
�� If extender providers the If extender providers the ““Care PlanCare Plan”” visit, then the visit, then the
MCP must be billed under the extenderMCP must be billed under the extender’’s provider s provider
number at 85% of physiciannumber at 85% of physician’’s fees fee
�� For 100% reimbursement, physician must see the For 100% reimbursement, physician must see the
patient for the major patient for the major ““Care PlanCare Plan”” visitvisit
139139
BILLING PHYSICIANS AS BILLING PHYSICIANS AS
““INCIDENT TOINCIDENT TO””
�� DO NOT bill an uncredentialed physician DO NOT bill an uncredentialed physician
““incident toincident to”” another physiciananother physician
�� CMS policy prohibits use of CMS policy prohibits use of ““incident toincident to””
billing from one physician to anotherbilling from one physician to another
140140
CODING FOR CODING FOR
OBSERVATION CAREOBSERVATION CARE
23 Hour short stay23 Hour short stay
Observation StatusObservation Status
141141
OBSERVATION STATUS CAREOBSERVATION STATUS CARE
�� ““23 hour23 hour”” short stay short stay –– can extend depending can extend depending
on hospitalon hospital’’s interpretation s interpretation
�� Outpatient hospital servicesOutpatient hospital services
�� Bill using outpatient hospital place of service Bill using outpatient hospital place of service
““2222””
�� RenalRenal--related services are part of the MCPrelated services are part of the MCP
�� Outpatient consult codes will be subject to Outpatient consult codes will be subject to
practice expense adjustment practice expense adjustment –– 25% of 25% of
reimbursementreimbursement
142142
OBSERVATION STATUS CAREOBSERVATION STATUS CARE
�� For services that cross over more than one For services that cross over more than one
calendar daycalendar day
�� Billed by supervising or admitting MDBilled by supervising or admitting MD
–– 9921899218--99220 for observation admission day99220 for observation admission day
–– 99217 for observation discharge day services99217 for observation discharge day services
�� Obs encounters by other physicians bill Obs encounters by other physicians bill
9924199241--99245 or 9922499245 or 99224--99226 as 99226 as
appropriateappropriate
143143
OBSERVATION STATUS CAREOBSERVATION STATUS CARE
�� When observation care is within same When observation care is within same
calendar day calendar day –– but exceeds 8 hoursbut exceeds 8 hours
�� Bill 99234Bill 99234--99236 only99236 only
�� Do not bill discharge care Do not bill discharge care –– 9921799217
�� Other services such as Emergency room Other services such as Emergency room
services are part of the observation status services are part of the observation status
codecode
144144
OBSERVATION STATUS CAREOBSERVATION STATUS CARE
�� For observation care of less than 8 hours, For observation care of less than 8 hours,
bill only the appropriate observation admit bill only the appropriate observation admit
code 99218code 99218--9922099220
�� Do not bill a discharge codeDo not bill a discharge code
SUBSEQUENT OBSERVATION SUBSEQUENT OBSERVATION
CARECARE
�� 9922499224--99226 are used to bill subsequent 99226 are used to bill subsequent
observation care by any physicianobservation care by any physician
�� Document changes in the history, physical Document changes in the history, physical
condition and response to management condition and response to management
since the last assessment by the physiciansince the last assessment by the physician
145145
146146
CODING FOR CRITICAL CODING FOR CRITICAL
CARECARE
147147
9929199291
�� Critical care, evaluation and management of Critical care, evaluation and management of
the critically ill or critically injured patient; the critically ill or critically injured patient;
first 30first 30--74 minutes74 minutes
148148
9929299292
�� Critical care, evaluation and management Critical care, evaluation and management
of the critically ill or critically injured patient; of the critically ill or critically injured patient;
each additional 30 minutes each additional 30 minutes
149149
CPT DEFINITIONCPT DEFINITION
CRITICAL ILLNESS OR INJURYCRITICAL ILLNESS OR INJURY
�� ““A critical illness or injury acutely impairs A critical illness or injury acutely impairs
one or more vital organ system(s) such one or more vital organ system(s) such
that there is a high probability of imminent that there is a high probability of imminent
or life threatening deterioration in the or life threatening deterioration in the
patientpatient’’s condition.s condition.””
150150
CPT DEFINITIONCPT DEFINITION
CRITICAL CARE SERVICESCRITICAL CARE SERVICES
�� ““Critical care is the Critical care is the direct deliverydirect delivery by a by a
physician(s) of medical care for a critically ill physician(s) of medical care for a critically ill
or injured patient.or injured patient.””
�� ““Involves decision making of high Involves decision making of high
complexity to assess, manipulate, and complexity to assess, manipulate, and
support system function(s), to treat single or support system function(s), to treat single or
multiple vital organ system failure and/or to multiple vital organ system failure and/or to
prevent further life threatening deterioration prevent further life threatening deterioration
of the patientof the patient’’s condition.s condition.””
151151
CPT DEFINITIONCPT DEFINITION
CRITICAL CARE SERVICESCRITICAL CARE SERVICES
Examples of Vital Organ System FailureExamples of Vital Organ System Failure
�� Central nervous system failureCentral nervous system failure
�� ShockShock
�� Circulatory failureCirculatory failure
�� Renal failureRenal failure
�� Hepatic failureHepatic failure
�� Respiratory failureRespiratory failure
�� Metabolic failureMetabolic failure
152152
WHERE IS CRITICAL CARE WHERE IS CRITICAL CARE
PROVIDEDPROVIDED
�� Critical care is usually, but not always, given Critical care is usually, but not always, given
in a critical care area, such as the coronary in a critical care area, such as the coronary
care unit, intensive care unit, pediatric care unit, intensive care unit, pediatric
intensive care unit, respiratory care unit, or intensive care unit, respiratory care unit, or
the emergency care facility.the emergency care facility.
153153
TREATMENT CRITERIONTREATMENT CRITERION
�� Critical care services require direct Critical care services require direct personal personal
management by the physician. They are life management by the physician. They are life
and organ supporting interventions that and organ supporting interventions that
require frequent, personal assessment and require frequent, personal assessment and
manipulation by the physician.manipulation by the physician.
�� Failure to provide these interventions on an Failure to provide these interventions on an
urgent basis would result in life threatening urgent basis would result in life threatening
deterioration in the patientdeterioration in the patient’’s condition.s condition.
154154
““FULL ATTENTIONFULL ATTENTION””
REQUIREMENTREQUIREMENT�� ““Critical care is used to report the total Critical care is used to report the total
duration of time spent by a physician duration of time spent by a physician
providing critical care services to a critically providing critical care services to a critically
ill or injured patient, even if the time spent ill or injured patient, even if the time spent
by the physician on that date is not by the physician on that date is not
continuous. For the time spent, the continuous. For the time spent, the
physician must devote his or her physician must devote his or her fullfull
attention to the patientattention to the patient…”…”
155155
WHERE IS THE CARE PROVIDEDWHERE IS THE CARE PROVIDED
�� Time spent with the individual patient Time spent with the individual patient mustmust be be
recorded in the patientrecorded in the patient’’s record.s record.
�� Time spent can be reported if spent is at the Time spent can be reported if spent is at the
bedside or on the unit or floor, i.e.. Coordinating bedside or on the unit or floor, i.e.. Coordinating
care, but care, but cannotcannot be in caring for another patient. be in caring for another patient.
�� Can include time spent with family, etc. when the Can include time spent with family, etc. when the
patient cannot make decisions for self.patient cannot make decisions for self.
156156
DOCUMENTIONDOCUMENTION
FOR MEDICAL REVIEWFOR MEDICAL REVIEW
�� Must indicate full attention providedMust indicate full attention provided
�� Since time based, must contain documentation of Since time based, must contain documentation of
total time involved total time involved
�� Time involved with family to gain pertinent history Time involved with family to gain pertinent history
or make decisions must be documentedor make decisions must be documented
�� Telephone calls to family members to be Telephone calls to family members to be
considered must meet same criteria as faceconsidered must meet same criteria as face--toto--
faceface
157157
SERVICES SERVICES NOTNOT INCLUDED IN INCLUDED IN
CRITICAL CARE TIMECRITICAL CARE TIME
�� Time spent providing services not bundled into critical care timTime spent providing services not bundled into critical care time e
such as dialysis or access placement are not includedsuch as dialysis or access placement are not included
�� Services rendered earlier in the day prior to the patientServices rendered earlier in the day prior to the patient’’s need s need
for critical care. This service can be reported separately, butfor critical care. This service can be reported separately, but
documentation needs to be sent with the claim and a modifier documentation needs to be sent with the claim and a modifier
((--25) needs to be appended to this service. 25) needs to be appended to this service. CR 5792 CR 5792
�� Time spent updating patientTime spent updating patient’’s family about status not meeting s family about status not meeting
previous criteria regardless of how lengthyprevious criteria regardless of how lengthy
158158
CRITICAL CARE & DIALYSISCRITICAL CARE & DIALYSIS
�� Dialysis (90935, 90937, 90945, 90947) is Dialysis (90935, 90937, 90945, 90947) is
not included in Critical Care timenot included in Critical Care time
�� Make sure a separate note is made for Make sure a separate note is made for
dialysis and all the criteria for billing dialysis and all the criteria for billing
dialysis are metdialysis are met……physical presence physical presence
during the treatmentduring the treatment
�� Append a Append a ““--2525”” modifier to the Critical modifier to the Critical
Care codeCare code
159159
CRITICAL CARE TIDBITSCRITICAL CARE TIDBITS
�� 99291 is used to report first hour (3099291 is used to report first hour (30--74 minutes) 74 minutes) of critical careof critical care
�� 99292 is used to report each additional 30 99292 is used to report each additional 30 minutesminutes
�� 99292 is used to report final 1599292 is used to report final 15--30 minutes of 30 minutes of critical carecritical care
�� Critical care of less than 30 minutes is reported Critical care of less than 30 minutes is reported using appropriate E/M code using appropriate E/M code
�� Only one physician may bill for a given hour of Only one physician may bill for a given hour of critical care even if more than one physician is critical care even if more than one physician is providing careproviding care
160160
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
�� Critical CareCritical Care
–– Does the documentation demonstrate all of the Does the documentation demonstrate all of the
following?following?
�� Direct personal management.Direct personal management.
�� Frequent personal assessment and manipulation (not Frequent personal assessment and manipulation (not just the general oncejust the general once--aa--day visit).day visit).
�� HighHigh--complexity decisioncomplexity decision--making to assess, making to assess, manipulate and support vital system function(s) to manipulate and support vital system function(s) to
treat single or multiple organ system failure or to treat single or multiple organ system failure or to
prevent further deterioration.prevent further deterioration.
161161
TIPS FOR PREVENTING CODING TIPS FOR PREVENTING CODING
ERRORS WITH E/M CODINGERRORS WITH E/M CODING
�� Critical Care Critical Care –– cont.cont.�� Interventions of a nature that failure to initiate these Interventions of a nature that failure to initiate these
interventions on an urgent basis would likely result in sudden interventions on an urgent basis would likely result in sudden clinically significant or lifeclinically significant or life--threatening deterioration in the threatening deterioration in the patientpatient’’s condition.s condition.
–– What about the time spent providing critical care?What about the time spent providing critical care?
�� Is specifically recorded?Is specifically recorded?
�� Is it reasonable considering the documented work provided?Is it reasonable considering the documented work provided?
�� Does it exclude time spent performing procedures separately Does it exclude time spent performing procedures separately billable?billable?
�� If it includes time spent with family, was the family members If it includes time spent with family, was the family members operating as a surrogate decisionoperating as a surrogate decision--maker because the patient maker because the patient was unable to make decisions?was unable to make decisions?
CKD EDUCATION CKD EDUCATION
BENEFITSBENEFITS
IMPLEMENTATION IMPLEMENTATION
JANUARY 1, 2010JANUARY 1, 2010
162162
CKD EDUCATION BENEFITCKD EDUCATION BENEFIT
�� Limited to beneficiaries with Stage IV CKDLimited to beneficiaries with Stage IV CKD
�� Defined as six, 60 minute sessionsDefined as six, 60 minute sessions
�� Allows for individual or group sessionsAllows for individual or group sessions
–– G0420 G0420 –– for individualsfor individuals
–– G0421G0421–– for group sessionsfor group sessions
�� The RVUs for G0420 was multiplied by 4 and The RVUs for G0420 was multiplied by 4 and
G0421 was multiplied by 2G0421 was multiplied by 2
�� G0420 would pay approximately $108.18G0420 would pay approximately $108.18
�� G0421 would pay approximately $25.60G0421 would pay approximately $25.60
163163
CKD EDUCATION BENEFITCKD EDUCATION BENEFIT
�� ““Incident toIncident to”” does not apply does not apply –– education must education must
be rendered by a physician, physician be rendered by a physician, physician
assistant, nurse practitioner or clinical nurse assistant, nurse practitioner or clinical nurse
specialistspecialist
�� Dialysis facilities expressly are excluded from Dialysis facilities expressly are excluded from
providing this serviceproviding this service
164164
EDUCATION TALKING POINTSEDUCATION TALKING POINTS
�� Basic information regarding CKD, how the Basic information regarding CKD, how the
kidneys work, what happens when the kidney kidneys work, what happens when the kidney
fail and the permanence of the diseasefail and the permanence of the disease
�� Survival rates with and without renal Survival rates with and without renal
replacement therapy and survival rates if the replacement therapy and survival rates if the
patient refused treatment for the CKDpatient refused treatment for the CKD
�� The need for kidney transplantationThe need for kidney transplantation
165165
EDUCATION TALKING POINTSEDUCATION TALKING POINTS
•• Unbiased information about RRT options Unbiased information about RRT options
including advantages and disadvantages for including advantages and disadvantages for
all modalitiesall modalities
•• Adequate information regarding why some Adequate information regarding why some
RRT options were not viable for a patientRRT options were not viable for a patient
•• How different RRT options affected the How different RRT options affected the
patientpatient’’s cos co--morbid conditionsmorbid conditions
•• Effects of RRT choices on lifestyle such as Effects of RRT choices on lifestyle such as
treatment flexibility & session lengthtreatment flexibility & session length
166166
EDUCATION TALKING POINTSEDUCATION TALKING POINTS
�� Whether a patient will need assistance based on Whether a patient will need assistance based on
RRT modality choice and training requirements for RRT modality choice and training requirements for
helpershelpers
�� The right to refuse treatmentThe right to refuse treatment
�� Effects of the disease and the subsequent Effects of the disease and the subsequent
treatment on the patienttreatment on the patient’’s physical appearances physical appearance
�� Patient recognition of the symptoms that would Patient recognition of the symptoms that would
empower the patient with the knowledge to seek empower the patient with the knowledge to seek
helphelp
167167
EDUCATION TALKING POINTSEDUCATION TALKING POINTS
�� Disease and treatment complications related to Disease and treatment complications related to
renal replacement therapy such as renal replacement therapy such as
hypertension, catheter migration, temporary/ hypertension, catheter migration, temporary/
permanent loss of dialysis access and risk of permanent loss of dialysis access and risk of
infection at the access siteinfection at the access site
�� How to control and manage consequences of How to control and manage consequences of
complications and symptoms (for example: complications and symptoms (for example:
treatment for itchy skin or insomnia)treatment for itchy skin or insomnia)
168168
EDUCATION TALKING POINTSEDUCATION TALKING POINTS
�� The ability to travel and organize holidays The ability to travel and organize holidays
depending on RRT choicedepending on RRT choice
�� Maintenance of social relationships, activities and Maintenance of social relationships, activities and
commitmentscommitments
�� How the disease and RRT may affect the patientHow the disease and RRT may affect the patient’’s s
ability to continue workingability to continue working
�� Available support servicesAvailable support services
�� Medication management Medication management
169169
POSTPOST-- EDUCATION EDUCATION
ASSESSMENTASSESSMENT
�� Requires beneficiaries to be assessed at the Requires beneficiaries to be assessed at the
conclusion of the sessionsconclusion of the sessions
�� Providers must develop outcome assessments Providers must develop outcome assessments
tailored to beneficiariestailored to beneficiaries
�� At this point CMS is seeking comment on the At this point CMS is seeking comment on the
factors to include in the outcomes assessmentfactors to include in the outcomes assessment
170170
DOCUMENTATIONDOCUMENTATION
�� Although the regulations did not address Although the regulations did not address
specific documentation requirements, it will specific documentation requirements, it will
be necessary to documentation the elements be necessary to documentation the elements
covered in each sessioncovered in each session
�� Maintain the documentation in the patientMaintain the documentation in the patient’’s s
chartchart
�� RPA has developed a documentation tool to RPA has developed a documentation tool to
assist our physicians in this taskassist our physicians in this task
171171
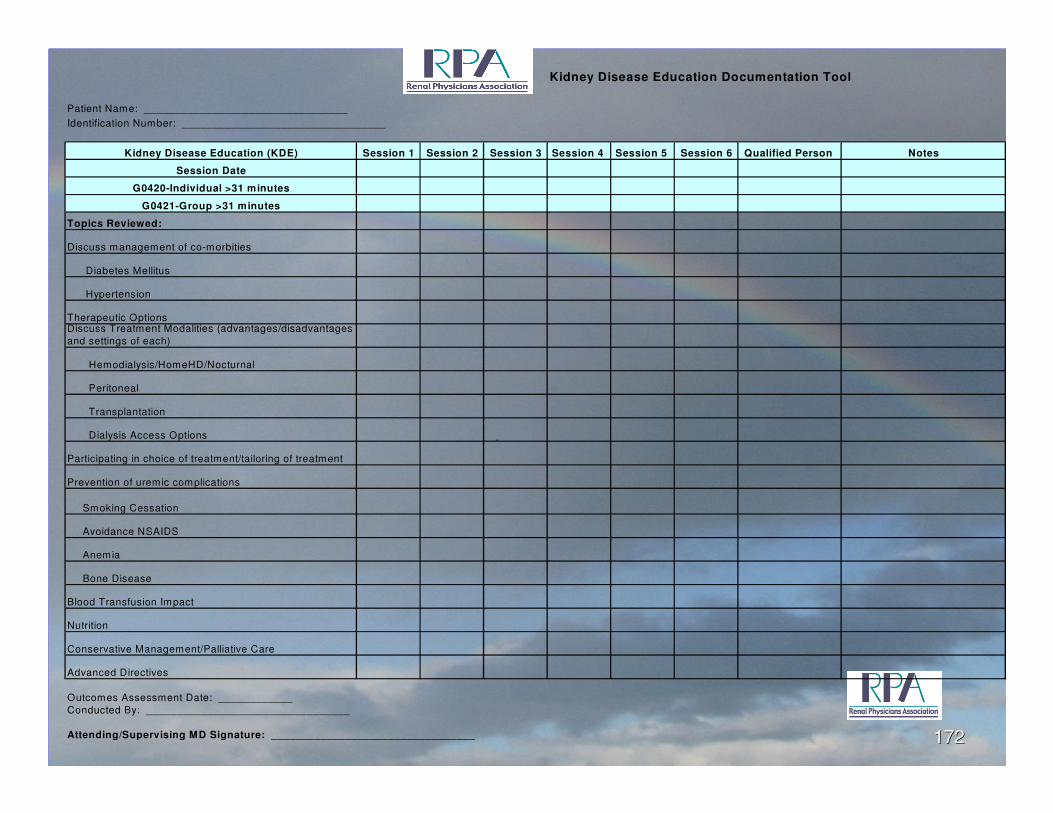
Kidney Disease Education Documentation Tool
Patient Name: _________________________________
Identification Number: _________________________________
Kidney Disease Education (KDE) Session 1 Session 2 Session 3 Session 4 Session 5 Session 6 Qualified Person Notes
Session Date
G0420-Individual >31 minutes
G0421-Group >31 minutes
Topics Reviewed:
Discuss management of co-morbities
Diabetes Mellitus
Hypertension
Therapeutic OptionsDiscuss Treatment Modalities (advantages/disadvantages
and settings of each)
Hemodialysis/HomeHD/Nocturnal
Peritoneal
Transplantation
Dialysis Access Options
Participating in choice of treatment/tailoring of treatment
Prevention of uremic complications
Smoking Cessation
Avoidance NSAIDS
Anemia
Bone Disease
Blood Transfusion Impact
Nutrition
Conservative Management/Palliative Care
Advanced Directives
Outcomes Assessment Date: ____________
Conducted By: _________________________________
Attending/Supervising MD Signature: _________________________________
172172
MEDICARE PREVENTIVE MEDICARE PREVENTIVE
SERVICESSERVICES
Section 4103 of the Affordable Section 4103 of the Affordable
Care Act of 2010Care Act of 2010
Annual Wellness VisitAnnual Wellness Visit
173173
WELCOME TO MEDICARE WELCOME TO MEDICARE
PHYSICALPHYSICAL
�� G0402 G0402 –– Initial preventive physical exam Initial preventive physical exam
(IPPE)(IPPE)
–– Within first 12 months of having Part B MedicareWithin first 12 months of having Part B Medicare
–– No deductible applies but coinsurance appliesNo deductible applies but coinsurance applies
–– Can bill separate E&M service with modifier Can bill separate E&M service with modifier ““--2525””
–– EKG no longer is required (deductible & EKG no longer is required (deductible &
coinsurance do apply if performed)coinsurance do apply if performed)
174174
WELCOME TO MEDICARE WELCOME TO MEDICARE
PHYSICAL (IPPE)PHYSICAL (IPPE)
�� Review of medical & social history with Review of medical & social history with
emphasis on disease detectionemphasis on disease detection
�� Review of risk for depressionReview of risk for depression
�� Review of functional ability & level of safetyReview of functional ability & level of safety
�� PE including height, weight, BP, visual screenPE including height, weight, BP, visual screen
�� Referral, education & counseling as needed Referral, education & counseling as needed
including written plan for appropriate including written plan for appropriate
screening and other preventive services screening and other preventive services
175175
ANNUAL WELLNESS VISIT ANNUAL WELLNESS VISIT
(AWV)(AWV)
�� G0438 G0438 -- beneficiary is no longer within 12 beneficiary is no longer within 12
months after effective date of first Medicare months after effective date of first Medicare
Part B coverage period and did not receive Part B coverage period and did not receive
the IPPE benefit during the 1the IPPE benefit during the 1stst 12 months12 months
�� Once in a lifetime benefitOnce in a lifetime benefit
�� G0439 G0439 –– subsequent AWV annually subsequent AWV annually
thereafterthereafter
176176
ANNUAL WELLNESS VISIT ANNUAL WELLNESS VISIT
(AWV) ELEMENTS(AWV) ELEMENTS�� Establishment of medical/family historyEstablishment of medical/family history
�� Measurement of height, weight, body mass index (or waist Measurement of height, weight, body mass index (or waist
circumference, if appropriate), blood pressure, and other circumference, if appropriate), blood pressure, and other measurements as deem appropriatemeasurements as deem appropriate
�� List of current providers and suppliers used regularly for List of current providers and suppliers used regularly for
beneficiarybeneficiary
�� Detection of any cognitive impairmentsDetection of any cognitive impairments
�� Review of risk for depression using screening testsReview of risk for depression using screening tests
�� Review of functional ability & level of safety based on Review of functional ability & level of safety based on
observation and screening questions or questionnairesobservation and screening questions or questionnaires
177177
ANNUAL WELLNESS VISIT ANNUAL WELLNESS VISIT
(AWV) ELEMENTS(AWV) ELEMENTS�� Establishment of written screening schedule such as a Establishment of written screening schedule such as a
check list for the next 5 to 10 years, include immunizations check list for the next 5 to 10 years, include immunizations
and health screening as age appropriateand health screening as age appropriate
�� Personalized health advice and referrals as appropriate for Personalized health advice and referrals as appropriate for
health education and preventive counseling services or health education and preventive counseling services or
programs to reduce risk and promote selfprograms to reduce risk and promote self--management management and wellness including weight loss, smoking cessation, fall and wellness including weight loss, smoking cessation, fall
prevention & nutritionprevention & nutrition
�� Voluntary advance care planningVoluntary advance care planning
�� Any other elements as deemed appropriate through the Any other elements as deemed appropriate through the National Carrier Determination process (NDC)National Carrier Determination process (NDC)
178178
ANNUAL WELLNESS VISIT ANNUAL WELLNESS VISIT
(AWV)(AWV)
�� May be performed by MD, DO, or qualified May be performed by MD, DO, or qualified
NPP, health educator, registered dietitian, NPP, health educator, registered dietitian,
nutrition professional or other licensed nutrition professional or other licensed
practitioner or a team of such professionalspractitioner or a team of such professionals
�� As a result of the Affordable Care Act, the As a result of the Affordable Care Act, the
deductible and coinsurance for the AWV is deductible and coinsurance for the AWV is
waivedwaived
179179
SUBSEQUENT AWV SUBSEQUENT AWV
ELEMENTSELEMENTS�� Update the individualUpdate the individual’’s medical/family historys medical/family history
�� Measure the patients weight, BP and other routine Measure the patients weight, BP and other routine
measurementsmeasurements
�� Update list of patientUpdate list of patient’’s current providers and supplierss current providers and suppliers
�� Detection of any cognitive impairments that the patient may Detection of any cognitive impairments that the patient may havehave
�� Update the individualUpdate the individual’’s written screening schedule s written screening schedule
developed at the first AWV providing PPPS (personal developed at the first AWV providing PPPS (personal preventive plan services)preventive plan services)
�� Update the list of risk factors and conditionsUpdate the list of risk factors and conditions
180180
SUBSEQUENT AWV SUBSEQUENT AWV
ELEMENTSELEMENTS�� Furnish appropriate personalized health advice to the Furnish appropriate personalized health advice to the
individual and referrals as necessary to health education or individual and referrals as necessary to health education or
preventive counseling or programspreventive counseling or programs
�� Voluntary advance care planning upon agreement with the Voluntary advance care planning upon agreement with the
patientpatient
�� Other elements that may be added through the National Other elements that may be added through the National Carrier Determination process (NCD)Carrier Determination process (NCD)
�� Deductible and coinsurance are waived for the Deductible and coinsurance are waived for the
subsequent AWV as well as the initialsubsequent AWV as well as the initial
181181
PAYMENT FOR AWVPAYMENT FOR AWV
�� Payment for G0438 AWV is approximately Payment for G0438 AWV is approximately
$155.19$155.19
�� Payment for G0439 subsequent AWV is Payment for G0439 subsequent AWV is
approximately $103.88.approximately $103.88.
182182
183183
ICDICD--99--CM CODINGCM CODING
WHY YOU DID WHAT YOU DIDWHY YOU DID WHAT YOU DID
ICDICD--9 Coding9 Coding
�� Detail is very important today in billing the Detail is very important today in billing the
diagnosis our patients havediagnosis our patients have
�� But as we approach October, 2013 detail But as we approach October, 2013 detail
becomes far more importantbecomes far more important
�� Diseases that are associated with Kidney Diseases that are associated with Kidney
disease are sometimes more challenging disease are sometimes more challenging
than CKD or ESRDthan CKD or ESRD
�� LetLet’’s take a different approach at ICDs take a different approach at ICD--99
184184
DIABETES INSIPIDUSDIABETES INSIPIDUS
�� Diabetes insipidus (DI) is an uncommon Diabetes insipidus (DI) is an uncommon
condition that occurs when the kidneys are condition that occurs when the kidneys are
unable to conserve water as they perform unable to conserve water as they perform
their function of filtering blood. The their function of filtering blood. The
amount of water conserved is controlled by amount of water conserved is controlled by
antidiuretic hormone (ADH), also called antidiuretic hormone (ADH), also called
vasopressin. (ICDvasopressin. (ICD--9 253.5)9 253.5)
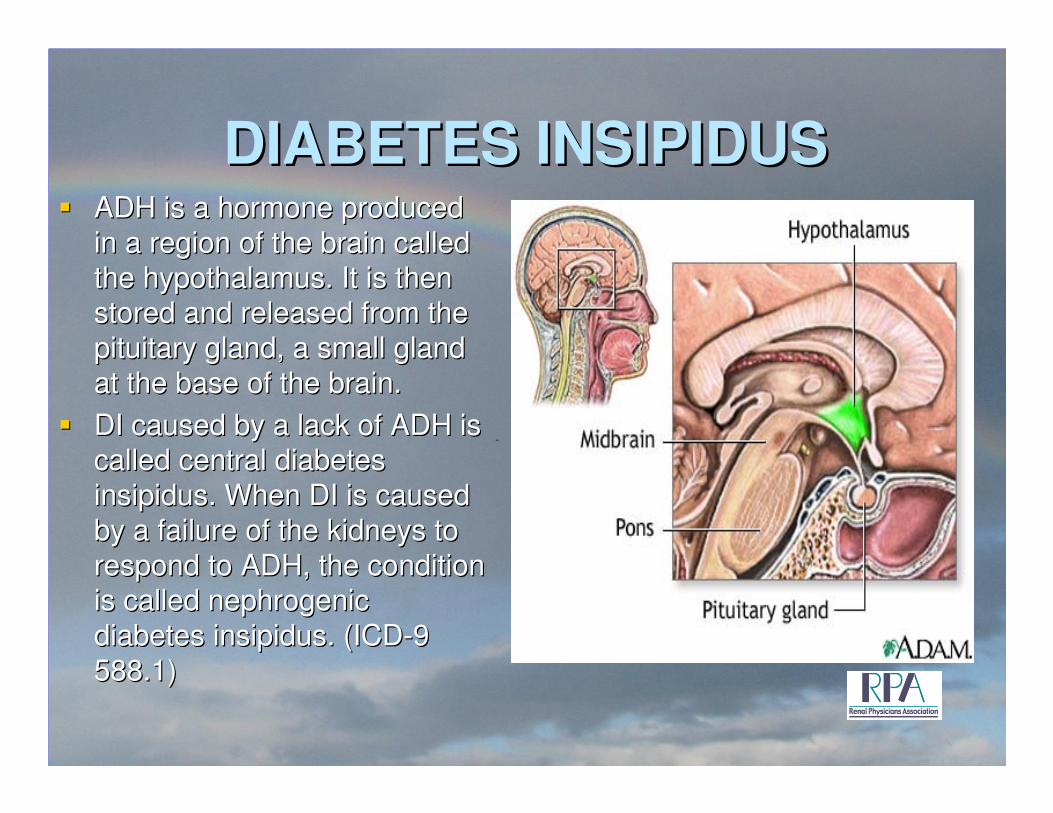
DIABETES INSIPIDUSDIABETES INSIPIDUS�� ADH is a hormone produced ADH is a hormone produced
in a region of the brain called in a region of the brain called
the hypothalamus. It is then the hypothalamus. It is then stored and released from the stored and released from the
pituitary gland, a small gland pituitary gland, a small gland
at the base of the brain.at the base of the brain.
�� DI caused by a lack of ADH is DI caused by a lack of ADH is called central diabetes called central diabetes
insipidus. When DI is caused insipidus. When DI is caused
by a failure of the kidneys to by a failure of the kidneys to
respond to ADH, the condition respond to ADH, the condition is called nephrogenic is called nephrogenic
diabetes insipidus. (ICDdiabetes insipidus. (ICD--9 9
588.1)588.1)
DIABETES INSIPIDUSDIABETES INSIPIDUS�� Nephrogenic DI involves a Nephrogenic DI involves a
defect in the parts of the defect in the parts of the
kidneys that reabsorb water kidneys that reabsorb water back into the bloodstream. It back into the bloodstream. It
occurs less often than central occurs less often than central
DI. Nephrogenic DI may DI. Nephrogenic DI may
occur as an inherited occur as an inherited
disorder in which male disorder in which male children receive the children receive the
abnormal gene that causes abnormal gene that causes
the disease from their the disease from their
mothers.mothers.
�� Nephrogenic DI may also be Nephrogenic DI may also be
caused by:caused by:
�� Certain drugs such as Certain drugs such as
lithiumlithium
�� High levels of calcium in the High levels of calcium in the
body (hypercalcemia) body (hypercalcemia)
(275.42)(275.42)
�� Kidney disease (such as Kidney disease (such as
polycystic kidney disease)polycystic kidney disease)
�� SymptomsSymptoms
–– Excessive thirst (783.5)Excessive thirst (783.5)�� May be intense or uncontrollableMay be intense or uncontrollable
�� May involve a craving for ice May involve a craving for ice
waterwater
–– Excessive urine volume Excessive urine volume (788.42)(788.42)
SIADHSIADH�� SSyndrome of yndrome of IInappropriate nappropriate AAntintiddiuretic iuretic HHormone ormone
secretion or SIADH secretion or SIADH
�� The body normally maintains very tight control over its The body normally maintains very tight control over its total amount of water and its concentration of sodiumtotal amount of water and its concentration of sodium
�� Certain disease states can upset the delicate balance of Certain disease states can upset the delicate balance of water and salt in the bodywater and salt in the body
�� If there is too much ADH in the body, or if the kidneys If there is too much ADH in the body, or if the kidneys overreact to the ADH they receive, the body retains overreact to the ADH they receive, the body retains excess water and the serum sodium concentration excess water and the serum sodium concentration becomes diluted and falls to abnormal levelsbecomes diluted and falls to abnormal levels
�� Treatment includes water restriction and salt Treatment includes water restriction and salt administration and diagnosis of the underlying cause of administration and diagnosis of the underlying cause of the SIADH, usually a neoplasm (ICDthe SIADH, usually a neoplasm (ICD--9 Code 253.6)9 Code 253.6)
HYPERTENSIONHYPERTENSION
�� Hypertension Table found under the main Hypertension Table found under the main
term term ““hypertensionhypertension”” in the index, contains a in the index, contains a
complete listing of all conditions due to or complete listing of all conditions due to or
associated with hypertension and classifies associated with hypertension and classifies
them according to malignant, benign, and them according to malignant, benign, and
unspecified.unspecified.
189189
HYPERTENSIONHYPERTENSION
�� Hypertension, essential, or NOSHypertension, essential, or NOS
–– Assign hypertension to category code 401 with Assign hypertension to category code 401 with
the appropriate fourth digit to indicate malignant the appropriate fourth digit to indicate malignant
(0), benign (1), or unspecified (9). Do not use (0), benign (1), or unspecified (9). Do not use
either .0 malignant or .1 benign unless the either .0 malignant or .1 benign unless the
medical record documentation supports such a medical record documentation supports such a
designationdesignation
190190
HYPERTENSIONHYPERTENSION
�� Hypertension with heart diseaseHypertension with heart disease
–– Heart conditions (425.8, 429.0Heart conditions (425.8, 429.0--429.3) are 429.3) are
assigned to a code from category 402 when a assigned to a code from category 402 when a
causal relationship is stated (due to causal relationship is stated (due to
hypertension) or implied (hypertensive). Use hypertension) or implied (hypertensive). Use
an additional code from category 428 to identify an additional code from category 428 to identify
the type of heart failure in those patients with the type of heart failure in those patients with
heart failure. More than one code from heart failure. More than one code from
category 428 may be assigned if the patient has category 428 may be assigned if the patient has
systolic or diastolic failure and CHFsystolic or diastolic failure and CHF
191191
HYPERTENSIONHYPERTENSION
�� Hypertension with heart disease (cont.)Hypertension with heart disease (cont.)
–– The same heart conditions with hypertension The same heart conditions with hypertension
without a stated causal relationship are coded without a stated causal relationship are coded
separately. Sequence according to the separately. Sequence according to the
circumstances of the encountercircumstances of the encounter
192192
HYPERTENSIONHYPERTENSION
�� Hypertensive chronic kidney diseaseHypertensive chronic kidney disease
–– Assign codes from category 403 when Assign codes from category 403 when
conditions classified in categories 585conditions classified in categories 585--587 587
are present. Unlike hypertensive heart are present. Unlike hypertensive heart
disease, there is a presumed cause and effect disease, there is a presumed cause and effect
relationship between hypertension and CKDrelationship between hypertension and CKD
–– Fourth digit is type of hypertensionFourth digit is type of hypertension
–– Fifth digit Fifth digit ““00”” is stage 1is stage 1--44
–– Fifth digit Fifth digit ““11”” is stage 5is stage 5--66
193193
HYPERTENSIONHYPERTENSION
�� Hypertensive chronic kidney diseaseHypertensive chronic kidney disease
–– If the physician states that the hypertension and If the physician states that the hypertension and
CKD are unrelated code the conditions CKD are unrelated code the conditions
separately sequencing according to the separately sequencing according to the
encounterencounter
194194
HYPERTENSIONHYPERTENSION
�� Hypertension secondary Hypertension secondary –– two codes are two codes are
required; one to identify the underlying required; one to identify the underlying
etiology and one from category 405 to etiology and one from category 405 to
identify the hypertension. Sequencing of the identify the hypertension. Sequencing of the
codes is determined by the reason for the codes is determined by the reason for the
encounter.encounter.
�� Elevated blood pressure reading without a Elevated blood pressure reading without a
diagnosis of hypertension is coded 796.2diagnosis of hypertension is coded 796.2
195195
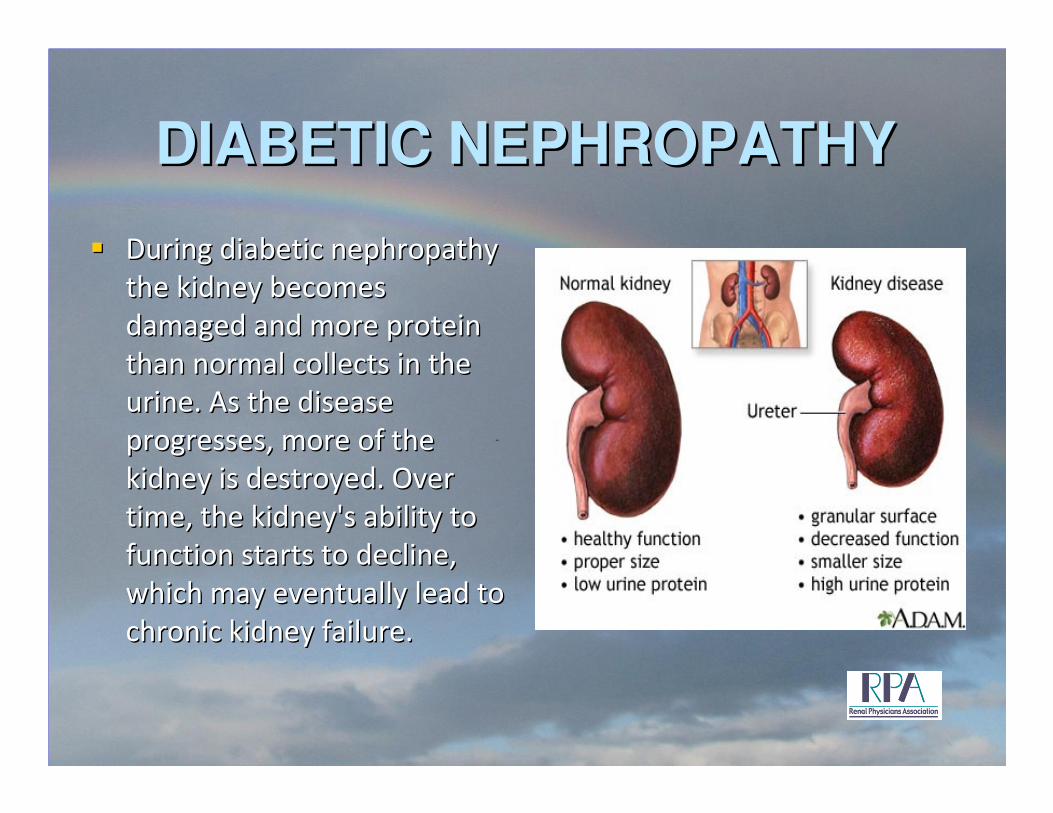
DIABETIC NEPHROPATHYDIABETIC NEPHROPATHY
�� During diabetic nephropathy During diabetic nephropathy
the kidney becomes the kidney becomes
damaged and more protein damaged and more protein
than normal collects in the than normal collects in the
urine. As the disease urine. As the disease
progresses, more of the progresses, more of the
kidney is destroyed. Over kidney is destroyed. Over
time, the kidney's ability to time, the kidney's ability to
function starts to decline, function starts to decline,
which may eventually lead to which may eventually lead to
chronic kidney failure.chronic kidney failure.
DIABETES MELLITUSDIABETES MELLITUS
�� 250 is the main category for diabetes250 is the main category for diabetes
�� The fourth digit is the manifestation of the The fourth digit is the manifestation of the
diabetes such as 250.4X is diabetes with diabetes such as 250.4X is diabetes with
renal manifestationsrenal manifestations
�� The fifth digit defines the type of diabetesThe fifth digit defines the type of diabetes
–– ““00”” is type II or unspecified not stated as is type II or unspecified not stated as
uncontrolleduncontrolled
–– ““11”” is type I not stated uncontrolledis type I not stated uncontrolled
–– ““22”” is type II uncontrolledis type II uncontrolled
–– ““33”” is type I uncontrolledis type I uncontrolled197197
DIABETES MELLITUSDIABETES MELLITUS
�� The age of the patient is not the sole The age of the patient is not the sole
determining factor of the type of diabetesdetermining factor of the type of diabetes
�� All type I diabetics must use insulin All type I diabetics must use insulin
�� However the use of insulin does not mean However the use of insulin does not mean
the patient is type Ithe patient is type I
�� Add the code V58.67 for long term insulin Add the code V58.67 for long term insulin
useuse
198198
DIABETES MELLITUSDIABETES MELLITUS
�� Assign and sequence manifestation and Assign and sequence manifestation and
association conditions with the 250.XX code association conditions with the 250.XX code
before associated codes before associated codes
�� For example: 250.40 is diabetes II with For example: 250.40 is diabetes II with
renal manifestations, if the patient has renal manifestations, if the patient has
diabetic nephropathy add 583.81 diabetic nephropathy add 583.81
(nephropathy) add the stage of CKD (ie. (nephropathy) add the stage of CKD (ie.
585.3) then add V58.67 if there is long term 585.3) then add V58.67 if there is long term
insulin useinsulin use
199199
SECONDARY DIABETES SECONDARY DIABETES
MELLITUSMELLITUS
�� Used to report diabetes when the disease Used to report diabetes when the disease
process is process is ““due todue to”” some other situation some other situation
such as drug induced or chemical inducedsuch as drug induced or chemical induced
�� Code the situation that caused the Code the situation that caused the
diabetesdiabetes
�� 249.XX is the series of codes249.XX is the series of codes
�� Do not use for sequencing diabetes when Do not use for sequencing diabetes when
the primary reason for the encounter was the primary reason for the encounter was
another problem another problem 200200
SECONDARY DIABETES SECONDARY DIABETES
MELLITUSMELLITUS
�� 249.4X 249.4X –– Secondary diabetes mellitus with Secondary diabetes mellitus with
renal manifestationsrenal manifestations
�� Fifth digit Fifth digit ““00”” not stated as uncontrolled or not stated as uncontrolled or
unspecified or unspecified or ““11”” uncontrolleduncontrolled
�� Use additional code to identify manifestationUse additional code to identify manifestation
–– CKD (585.1CKD (585.1--585.9)585.9)
–– Diabetic nephropathy (583.81)Diabetic nephropathy (583.81)
–– Intercapillary glomerulosclerosis (581.81)Intercapillary glomerulosclerosis (581.81)
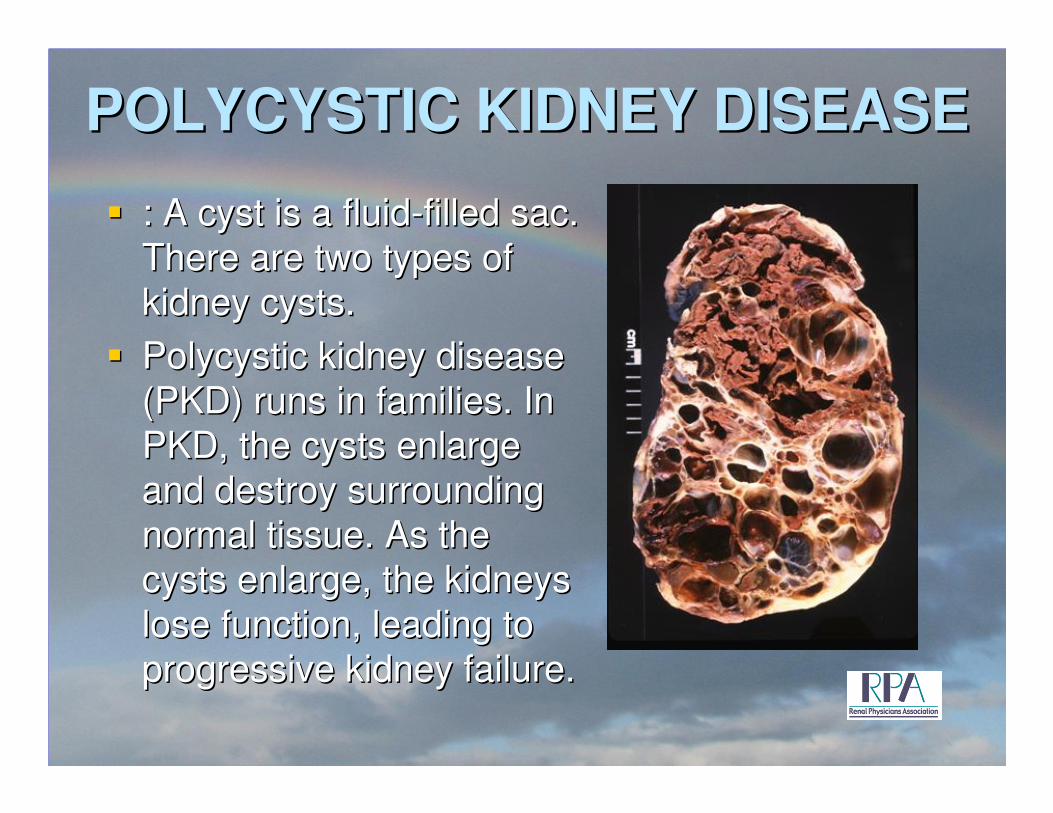
POLYCYSTIC KIDNEY DISEASEPOLYCYSTIC KIDNEY DISEASE
�� : A cyst is a fluid: A cyst is a fluid--filled sac. filled sac.
There are two types of There are two types of
kidney cysts.kidney cysts.
�� Polycystic kidney disease Polycystic kidney disease
(PKD) runs in families. In (PKD) runs in families. In
PKD, the cysts enlarge PKD, the cysts enlarge
and destroy surrounding and destroy surrounding
normal tissue. As the normal tissue. As the
cysts enlarge, the kidneys cysts enlarge, the kidneys
lose function, leading to lose function, leading to
progressive kidney failure.progressive kidney failure.
POLYCYSTIC KIDNEY DISEASEPOLYCYSTIC KIDNEY DISEASE
•• PKD can cause kidneys PKD can cause kidneys to fail requiring dialysis to fail requiring dialysis or transplantor transplant
•• PKD can cause blood PKD can cause blood in the urinein the urine
•• PKD can cause cysts to PKD can cause cysts to develop on other develop on other organsorgans
•• Symptoms of PKDSymptoms of PKD–– Pain in the back and Pain in the back and
lower sidelower side
–– HeadacheHeadache
–– Urinary tract infectionsUrinary tract infections
•• Diagnosis is made with Diagnosis is made with imaging and patient imaging and patient historyhistory
•• Treatments are Treatments are medication and RRT medication and RRT (renal replacement (renal replacement therapy)therapy)
ICD-9 Code 753.12 – Polycystic unspec
753.13 PKD, autosomal dominant
753.14 PKD, autosomal recessive (rare
disease causing cysts on the kidney &
liver causing renal and kidney failure
in children and adolescents
ACQUIRED CYSTIC KIDNEY ACQUIRED CYSTIC KIDNEY
DISEASEDISEASE
�� Acquired cystic kidney disease (ACKD) Acquired cystic kidney disease (ACKD)
happens when people are on dialysishappens when people are on dialysis
�� Unlike PKD, patients with ACKD do not Unlike PKD, patients with ACKD do not
develop cysts on other organsdevelop cysts on other organs
�� The kidneys are normal sizeThe kidneys are normal size
�� ACKD usually is symptom freeACKD usually is symptom free
�� ACKD is harmless and does not need ACKD is harmless and does not need
treatmenttreatmentICD-9 Code 593.2
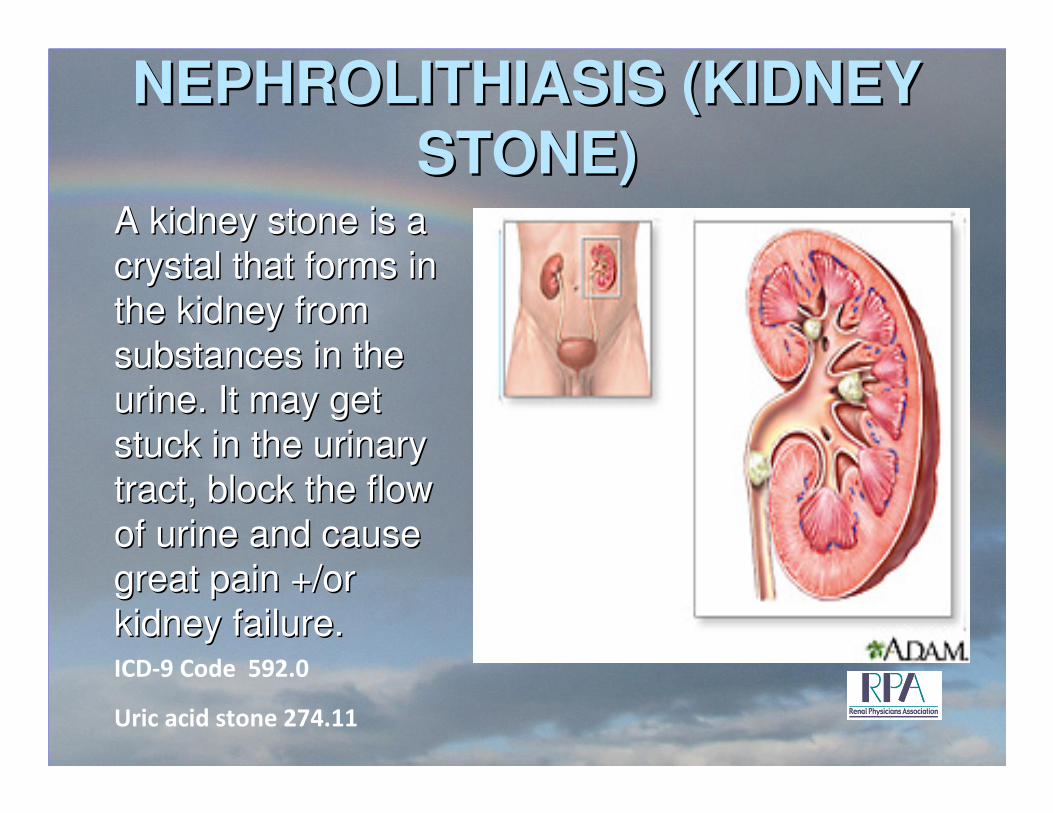
NEPHROLITHIASIS (KIDNEY NEPHROLITHIASIS (KIDNEY
STONE)STONE)A kidney stone is a A kidney stone is a
crystal that forms in crystal that forms in
the kidney from the kidney from
substances in the substances in the
urine. It may get urine. It may get
stuck in the urinary stuck in the urinary
tract, block the flow tract, block the flow
of urine and cause of urine and cause
great pain +/or great pain +/or
kidney failure. kidney failure. ICD-9 Code 592.0
Uric acid stone 274.11
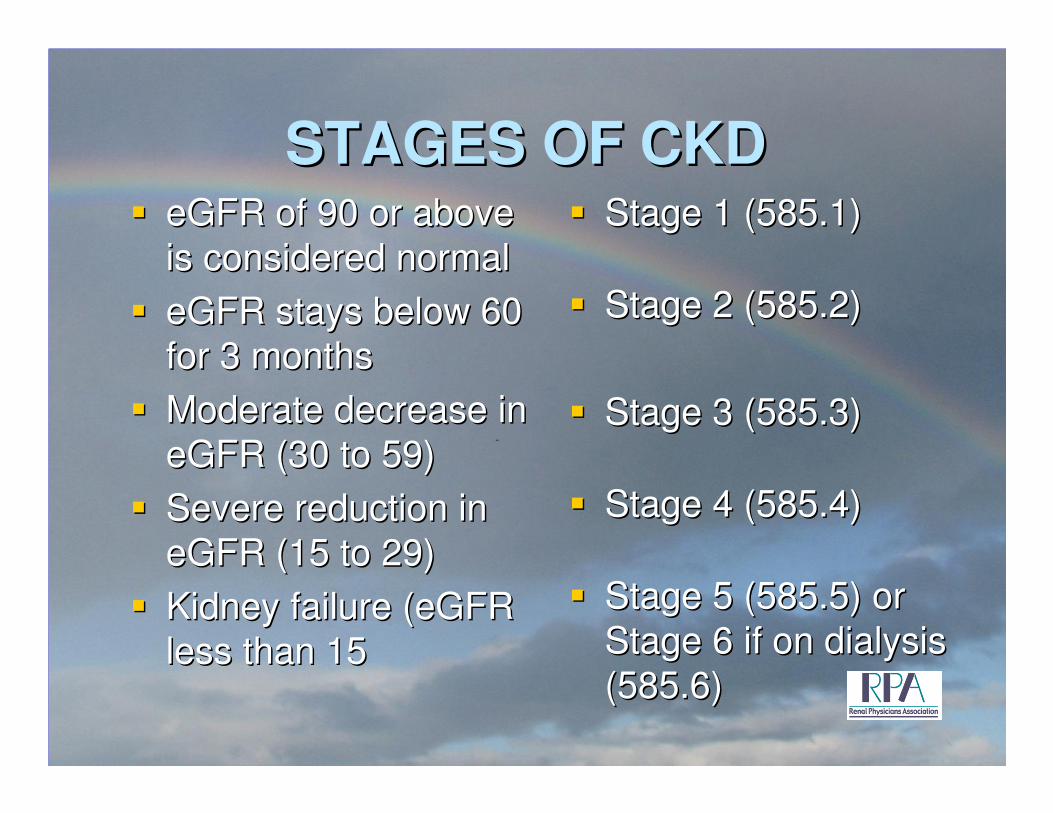
STAGES OF CKDSTAGES OF CKD�� eGFR of 90 or above eGFR of 90 or above
is considered normalis considered normal
�� eGFR stays below 60 eGFR stays below 60
for 3 monthsfor 3 months
�� Moderate decrease in Moderate decrease in
eGFR (30 to 59)eGFR (30 to 59)
�� Severe reduction in Severe reduction in
eGFR (15 to 29)eGFR (15 to 29)
�� Kidney failure (eGFR Kidney failure (eGFR
less than 15less than 15
�� Stage 1 (585.1)Stage 1 (585.1)
�� Stage 2 (585.2)Stage 2 (585.2)
�� Stage 3 (585.3)Stage 3 (585.3)
�� Stage 4 (585.4)Stage 4 (585.4)
�� Stage 5 (585.5) or Stage 5 (585.5) or
Stage 6 if on dialysis Stage 6 if on dialysis
(585.6)(585.6)
ACUTE KIDNEY FAILUREACUTE KIDNEY FAILURE
�� Acute (sudden) kidney Acute (sudden) kidney
failure is the sudden failure is the sudden
loss of the ability of the loss of the ability of the
kidneys to remove kidneys to remove
waste and concentrate waste and concentrate
urine +/or excrete urine +/or excrete
electrolytes.electrolytes.
�� Physician may list as Physician may list as
AKI (acute kidney AKI (acute kidney
injury)injury)
�� May have AKF in the May have AKF in the
setting of CKDsetting of CKD
�� Code the AKF primary Code the AKF primary
with the underlying with the underlying
stage of CKD stage of CKD
secondarysecondary
ICD-9 Code 584.9
Acute on Chronic 584.9 followed by the
stage of CKD prior to the exacerbation
585.X
ACUTE TUBULAR NECROSISACUTE TUBULAR NECROSIS
•• Acute tubular necrosis (ATN) Acute tubular necrosis (ATN) is damaging and loss of is damaging and loss of tubular cells usually caused tubular cells usually caused by lack of oxygen and/or by lack of oxygen and/or chemical insult to the kidney chemical insult to the kidney tissues (ischemia of the tissues (ischemia of the kidneys). It may also occur if kidneys). It may also occur if the kidney cells are damaged the kidney cells are damaged by a poison or harmful by a poison or harmful substance.substance.
•• Diabetes can make more Diabetes can make more susceptiblesusceptible
•• Common in hospitalized Common in hospitalized patientspatients–– Blood transfusionsBlood transfusions–– Injury or trauma that damages Injury or trauma that damages
musclemuscle–– Hypotension > 30 minsHypotension > 30 mins
–– Major surgeryMajor surgery–– Septic ShockSeptic Shock
–– ContrastContrast–– Medication ToxicityMedication Toxicity
�� ATN is often recoverable but ATN is often recoverable but may need short term dialysis may need short term dialysis to support the body while the to support the body while the kidney recovers.kidney recovers.
ICD-9 Code 584.5
ACUTE KIDNEY FAILUREACUTE KIDNEY FAILURE
•• Acute Kidney Failure with lesion of renal Acute Kidney Failure with lesion of renal cortical necrosis (ICDcortical necrosis (ICD--9 584.6)9 584.6)
•• Acute Kidney Failure with lesion of renal Acute Kidney Failure with lesion of renal Medullary (papillary) necrosis Medullary (papillary) necrosis (most often (most often diabetic or associated with NSAID use) diabetic or associated with NSAID use) (ICD(ICD--9 9 584.7)584.7)
•• Acute Kidney Failure with other specified Acute Kidney Failure with other specified pathological lesion in kidney (ICDpathological lesion in kidney (ICD--9 584.8)9 584.8)
•• These lesions may require a biopsy to prove These lesions may require a biopsy to prove presence of which type lesionpresence of which type lesion
RENAL BIOPSYRENAL BIOPSY
•• In renal biopsy, a small In renal biopsy, a small sample of kidney tissue is sample of kidney tissue is removed with a needle. The removed with a needle. The test is used to evaluate a test is used to evaluate a malfunctioning transplanted malfunctioning transplanted kidney. It is also used to kidney. It is also used to evaluate an unexplained evaluate an unexplained decrease in kidney function, decrease in kidney function, persistent blood in the urine persistent blood in the urine (ICD(ICD--9 599.70), or protein in 9 599.70), or protein in the urine (ICDthe urine (ICD--9 791.0).9 791.0).
•• Many glomerular diseases Many glomerular diseases will need a kidney biopsy for will need a kidney biopsy for definitive diagnosisdefinitive diagnosis
CPT Code 50200
ANALGESIC NEPHROPATHYANALGESIC NEPHROPATHY
•• Caused by use of pain Caused by use of pain killers such as aspirin, killers such as aspirin, ibuprofen, and naproxen ibuprofen, and naproxen sodium as well as sodium as well as prescription NSAIDsprescription NSAIDs
•• Use can be a single Use can be a single dose or more long termdose or more long term
•• Can cause acute or Can cause acute or chronic kidney diseasechronic kidney disease
•• Most frequent in women Most frequent in women over 30over 30
•• Statistics show that 4 out Statistics show that 4 out of every 100,000 people of every 100,000 people will develop Analgesic will develop Analgesic NephropathyNephropathy
•• Blood test should be Blood test should be done frequently to done frequently to monitor kidney monitor kidney involvementinvolvement
•• A less nephrotoxic A less nephrotoxic substance should be substance should be used when possible to used when possible to avoid damageavoid damage
ICD-9 Code 583.89
IgA NEPHROPATHYIgA NEPHROPATHY
•• IgA is a protein called an IgA is a protein called an antibody that helps the antibody that helps the body fight infections. IgA body fight infections. IgA nephropathy (Berger's nephropathy (Berger's disease) occurs when too disease) occurs when too much of this protein is much of this protein is deposited in the kidneys. deposited in the kidneys. IgA builds up inside the IgA builds up inside the small blood vessels of the small blood vessels of the kidney. Structures in the kidney. Structures in the kidney called glomeruli kidney called glomeruli become inflamed and become inflamed and damaged.damaged.
•• Risk factors include:Risk factors include:–– A personal or family history A personal or family history
of IgA nephropathy or of IgA nephropathy or Henoch Schonlein purpura, Henoch Schonlein purpura, a form of vasculitis that a form of vasculitis that affects many parts of the affects many parts of the bodybody
–– Caucasian or Asian Caucasian or Asian ethnicityethnicity
–– IgA nephropathy most IgA nephropathy most often affects males in their often affects males in their teens to late 30steens to late 30s
•• Symptoms include:Symptoms include:–– Blood in the urineBlood in the urine–– Repeated blood or dark Repeated blood or dark
urineurine–– Swelling of hands and feetSwelling of hands and feet
ICD-9 Code 583.9
LUPUS NEPHRITISLUPUS NEPHRITIS
•• An inflammation of the An inflammation of the kidney caused by kidney caused by systemic lupus systemic lupus erythematosus (SLE) erythematosus (SLE) (ICD(ICD--9 Code 710.0) 9 Code 710.0)
•• Lupus can affect the Lupus can affect the connective tissues of connective tissues of multisystemmultisystem
•• Fever, muscle & joint Fever, muscle & joint pain, rash of a butterfly pain, rash of a butterfly patternpattern
•• Additionally code as a Additionally code as a secondary code for the secondary code for the manifestation of the manifestation of the diseasedisease–– Endocarditis (424.91)Endocarditis (424.91)
–– Nephritis (583.81)Nephritis (583.81)•• Chronic (582.81)Chronic (582.81)
–– Nephrotic Syndrome Nephrotic Syndrome (581.81)(581.81)
Coding Note: Watch use of 583.81
This code is a secondary code and cannot
be used as a primary code
FOCAL SEGMENTAL FOCAL SEGMENTAL
GLOMERULOSCLEROSISGLOMERULOSCLEROSIS
•• Focal Segmental GS is Focal Segmental GS is scar tissue that forms in scar tissue that forms in the glomerulithe glomeruli
•• Focal means that some of Focal means that some of the glomeruli become the glomeruli become damaged while others damaged while others remain normalremain normal
•• Segmental means that Segmental means that only part of the individual only part of the individual glomeruli becomes glomeruli becomes damageddamaged
•• FSGS affect children and FSGS affect children and adults but most frequently adults but most frequently AfricanAfrican--AmericansAmericans
•• Known causes are:Known causes are:–– Heroin useHeroin use–– HIVHIV–– Inherited genetic problemsInherited genetic problems–– ObesityObesity–– Reflux Nephropathy (a Reflux Nephropathy (a
condition in which urine condition in which urine flows backward from the flows backward from the bladder to the kidney)bladder to the kidney)
–– Sickle Cell DiseaseSickle Cell Disease
�� Most are unknown etiologyMost are unknown etiologyICD-9 Code 582.1; with
Nephrotic syndrome 581.1
GOODPASTUREGOODPASTURE‘‘S SYNDROMES SYNDROME
•• Is a rare disease that Is a rare disease that targets the lungs and targets the lungs and kidneyskidneys
•• Is an autoimmune Is an autoimmune syndrome there the syndrome there the bodies own defense bodies own defense system attacks itselfsystem attacks itself
•• Symptoms includeSymptoms include–– Blood in urine (599.70)Blood in urine (599.70)
–– Protein in urine (791.0)Protein in urine (791.0)–– Fatigue and tiredness Fatigue and tiredness
(780.79)(780.79)
–– Hemoptysis (786.30)Hemoptysis (786.30)
•• GoodpastureGoodpasture’’s may be s may be diagnosis using blood diagnosis using blood tests, but biopsy of the tests, but biopsy of the lung or kidney may be lung or kidney may be necessarynecessary
•• Treatment may be Treatment may be immunosuppressive immunosuppressive therapy or therapy or plasmapheresisplasmapheresis
•• Patients may need Patients may need dialysis or kidney dialysis or kidney transplantationtransplantation
ICD-9 Code 446.21

SECONDARY SECONDARY
HYPERPARATHYROIDISMHYPERPARATHYROIDISM
�� Kidney failure is a Kidney failure is a
common cause of common cause of
secondary secondary
hyperparathyroidism. hyperparathyroidism.
Kidney failure can Kidney failure can
interfere with the interfere with the
body's ability to body's ability to
remove phosphate.remove phosphate.
�� Too much phosphate Too much phosphate
can cause a change in can cause a change in
calcium levels in the calcium levels in the
body. The calcium body. The calcium
needs to be corrected needs to be corrected
in these patients as in these patients as
well.well.
ICD-9 Code for Secondary hyperparathyroidism ofRenal origin 588.81
Secondary hyperparathyroidism of non-renal origin252.02
ICD-9 Hypocalcemia 275.41
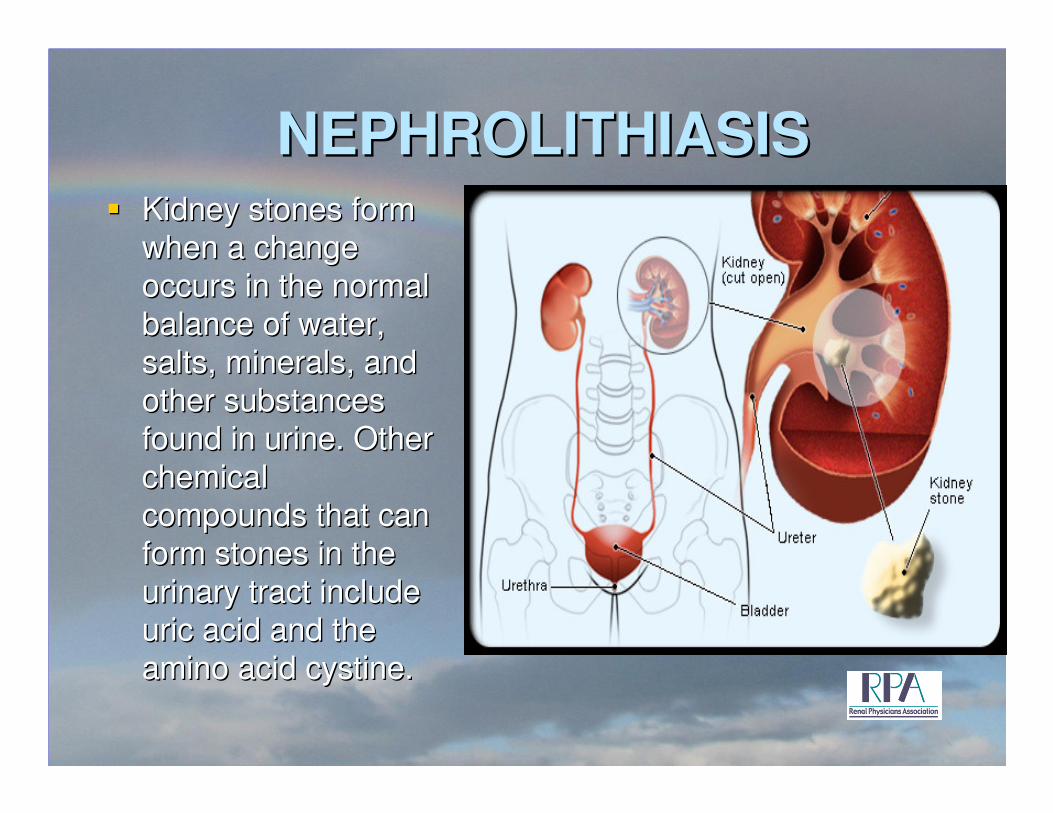
NEPHROLITHIASISNEPHROLITHIASIS�� Kidney stones form Kidney stones form
when a change when a change
occurs in the normal occurs in the normal
balance of water, balance of water, salts, minerals, and salts, minerals, and
other substances other substances found in urine. Other found in urine. Other
chemical chemical compounds that can compounds that can
form stones in the form stones in the
urinary tract include urinary tract include uric acid and the uric acid and the
amino acid cystine.amino acid cystine.
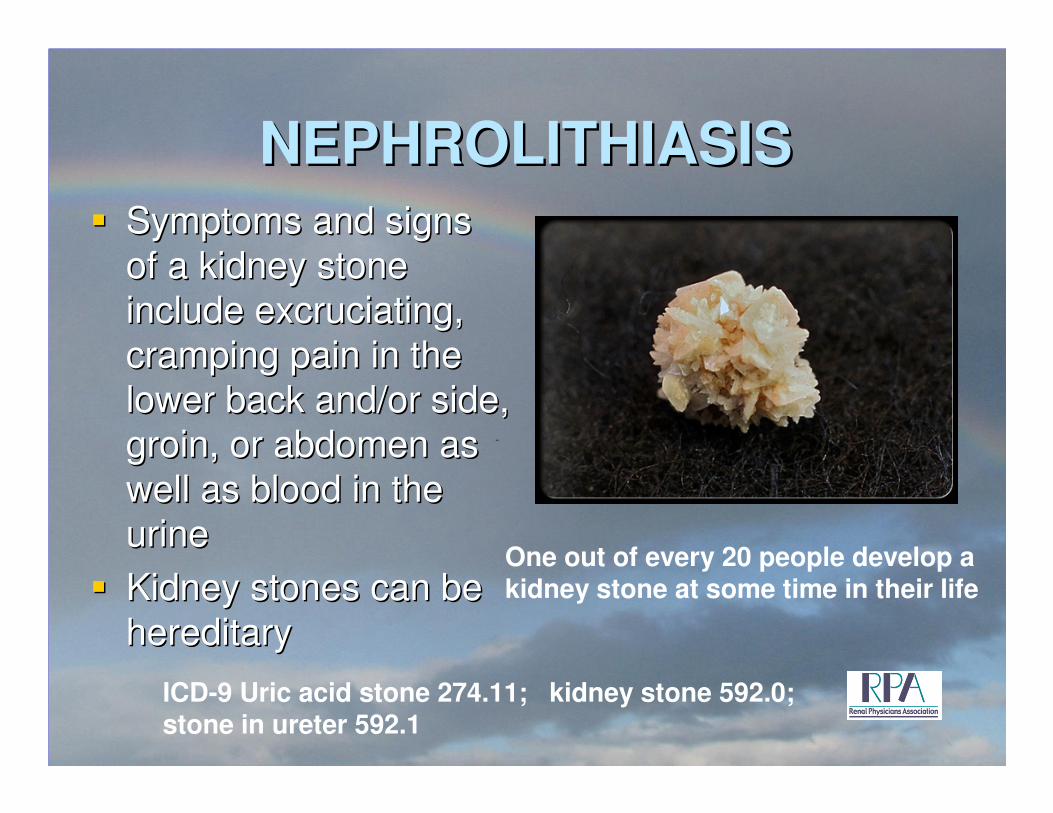
NEPHROLITHIASISNEPHROLITHIASIS�� Symptoms and signs Symptoms and signs
of a kidney stone of a kidney stone
include excruciating, include excruciating,
cramping pain in the cramping pain in the
lower back and/or side, lower back and/or side,
groin, or abdomen as groin, or abdomen as
well as blood in the well as blood in the
urineurine
�� Kidney stones can be Kidney stones can be
hereditaryhereditary
One out of every 20 people develop a kidney stone at some time in their life
ICD-9 Uric acid stone 274.11; kidney stone 592.0; stone in ureter 592.1
INTRODUCTION TOINTRODUCTION TO
ICDICD--10CM10CM
PROPOSED EFFECTIVE DATE PROPOSED EFFECTIVE DATE
OCTOBER 1, 2013OCTOBER 1, 2013
219219
ICDICD--1010--CM/PCSCM/PCS
�� Enacted in the Health Insurance Portability Enacted in the Health Insurance Portability
and Accountability Act (HIPAA) of 1996and Accountability Act (HIPAA) of 1996
�� All covered entities must implement the new All covered entities must implement the new
code sets for dates of service or date of code sets for dates of service or date of
discharge for inpatients that occur on or discharge for inpatients that occur on or
after October 1, 2013after October 1, 2013
�� Health and Human Services has no plans to Health and Human Services has no plans to
extend the implementation dateextend the implementation date
220220
ICDICD--1010--CM/PCSCM/PCS
�� Consists of two parts:Consists of two parts:
–– ICDICD--1010--CM CM –– The diagnosis classification The diagnosis classification
system developed for the CDC and all other US system developed for the CDC and all other US
treatment settingstreatment settings
–– ICDICD--1010--PCS PCS –– procedure classification system procedure classification system
developed by CMS for use in the US for developed by CMS for use in the US for
inpatient hospital settings ONLY. ICDinpatient hospital settings ONLY. ICD--10 uses 10 uses
7 alpha/numeric digits where ICD7 alpha/numeric digits where ICD--9 uses 39 uses 3--5 5
numeric digitsnumeric digits
221221
ICDICD--1010--CM/PCSCM/PCS
�� Incorporates much greater specificity and Incorporates much greater specificity and
clinical information which allows forclinical information which allows for
–– Improved ability to measure health care Improved ability to measure health care
servicesservices
–– Increased sensitivity when refining groupings Increased sensitivity when refining groupings
and reimbursement methodologiesand reimbursement methodologies
–– Enhanced ability to conduct public health Enhanced ability to conduct public health
surveillancesurveillance
–– Decrease need to including supporting Decrease need to including supporting
documentation with claimsdocumentation with claims222222
ICDICD--1010--CM/PCSCM/PCS
�� Includes updated medical terminology and Includes updated medical terminology and
classification of diseaseclassification of disease
�� Provides codes to allow comparison of Provides codes to allow comparison of
mortality and morbidity datamortality and morbidity data
�� Provides better data forProvides better data for
–– Measuring care furnished to patientsMeasuring care furnished to patients
–– Designing payment systemsDesigning payment systems
–– Making clinical decisionsMaking clinical decisions
223223
ICDICD--1010--CM/PCSCM/PCS
–– Processing claimsProcessing claims
–– Tracking public health Tracking public health
–– Identifying fraud and abuseIdentifying fraud and abuse
–– Conducting researchConducting research
224224
STRUCTURAL DIFFERENCES STRUCTURAL DIFFERENCES
BETWEEN THE TWO CODING BETWEEN THE TWO CODING
SYSTEMSSYSTEMS
�� ICDICD--99--CM Diagnosis CodesCM Diagnosis Codes
–– 33--5 digits5 digits
–– First digit is alpha (E or V) or numericFirst digit is alpha (E or V) or numeric
–– Digits 2Digits 2--5 are numeric5 are numeric
–– ExamplesExamples
�� 496 496 –– Chronic airway obstruction NECChronic airway obstruction NEC
�� 511.9 511.9 –– Unspecified pleural effusionUnspecified pleural effusion
�� V42.0 V42.0 –– Renal transplantRenal transplant225225
STRUCTURAL DIFFERENCES STRUCTURAL DIFFERENCES
BETWEEN THE TWO CODING BETWEEN THE TWO CODING
SYSTEMSSYSTEMS
�� ICDICD--1010--CM Diagnosis CodesCM Diagnosis Codes
–– 33--7 digits7 digits
–– Digit 1 is alphaDigit 1 is alpha
–– Digit 2 and 3 are numericDigit 2 and 3 are numeric
–– Digits 4Digits 4--7 are alpha or numeric (alpha digits are 7 are alpha or numeric (alpha digits are
not case sensitivenot case sensitive
226226
STRUCTURAL DIFFERENCES STRUCTURAL DIFFERENCES
BETWEEN THE TWO CODING BETWEEN THE TWO CODING
SYSTEMSSYSTEMS
–– ExamplesExamples
�� N18.6 N18.6 –– End stage renal diseaseEnd stage renal disease
�� S52.131a S52.131a -- Displaced fracture of neck of right radius, Displaced fracture of neck of right radius, initial encounter for closed fractureinitial encounter for closed fracture
�� N28.9 N28.9 –– Acute Renal FailureAcute Renal Failure
�� N18.1N18.1--5 5 –– Stages of CKDStages of CKD
�� I12.0 I12.0 –– ESRD due to HypertensionESRD due to Hypertension
227227
WHAT GENERATES THE WHAT GENERATES THE
RESISTANCE?RESISTANCE?
�� Perceptions regarding impact on practice Perceptions regarding impact on practice
managementmanagement–– General office staff lack sufficient expertiseGeneral office staff lack sufficient expertise
–– May require certified coders and current coders May require certified coders and current coders
may need to recertify, incurring costly training may need to recertify, incurring costly training
and exam feesand exam fees
�� Costly investment in new infrastructureCostly investment in new infrastructure–– New information technology tools requiredNew information technology tools required
–– New billing and collection systems requiredNew billing and collection systems required
–– Limited resources for staff trainingLimited resources for staff training
228228
WHAT GENERATES THE WHAT GENERATES THE
RESISTANCE?RESISTANCE?
�� Impact on reimbursementImpact on reimbursement
–– Decreased shortDecreased short--term coding accuracy and term coding accuracy and
productivityproductivity
�� Physician practice changesPhysician practice changes
–– Greater medical record documentation to Greater medical record documentation to
support more detailed codessupport more detailed codes
229229
GET PHYSICIAN BUYGET PHYSICIAN BUY--ININ
�� Provide evidence that simplifies the processProvide evidence that simplifies the process
�� Work with organized medicine to deliver the Work with organized medicine to deliver the
messagemessage
�� Partner with key professionals that can help Partner with key professionals that can help
facilitate trainingfacilitate training
�� Leverage existing relationships between Leverage existing relationships between
health information management health information management
professionals and physiciansprofessionals and physicians
230230
KNOCK IT DOWN TO SIZE!KNOCK IT DOWN TO SIZE!
�� Although the coding book is huge, we will Although the coding book is huge, we will
only use a small segment of the informationonly use a small segment of the information
�� Work with your physicians to develop Work with your physicians to develop
crosswalks between ICDcrosswalks between ICD--9 and ICD9 and ICD--10 10
codes they frequently usecodes they frequently use
�� Begin discussions now to reduce anxiety but Begin discussions now to reduce anxiety but
train later train later –– needs to be done needs to be done ““just in timejust in time””
�� Training should have both a general and Training should have both a general and
practice specific focuspractice specific focus231231
IMPLEMENTATION PLANNINGIMPLEMENTATION PLANNING
�� Start to organize your implementation effortStart to organize your implementation effort
�� Establish who will be the lead person in your Establish who will be the lead person in your
organization to oversee the implementation organization to oversee the implementation
efforteffort
�� Look at all areas that will be impacted by the Look at all areas that will be impacted by the
change change –– Practice Management SystemPractice Management System
–– Electronic Medical RecordsElectronic Medical Records
–– SuperbillsSuperbills
–– Clinical areasClinical areas232232
IMPLEMENTATION PLANNINGIMPLEMENTATION PLANNING
�� Schedule regular meetings to keep Schedule regular meetings to keep
everyone in the organization informed of the everyone in the organization informed of the
progressprogress
�� Develop a budget Develop a budget –– Look at what the costs Look at what the costs
will bewill be–– What resources will be required for What resources will be required for
implementationimplementation
–– Practice management system Practice management system –– disc spacedisc space
–– Software costsSoftware costs
–– Training Training 233233
IMPLEMENTATION PLANNINGIMPLEMENTATION PLANNING
�� Develop a reasonable timeline that can be Develop a reasonable timeline that can be
accomplished accomplished –– frustration will only end in frustration will only end in
failure and more frustrationfailure and more frustration
�� Keep the physicians involved Keep the physicians involved –– assess the assess the
physicianphysician’’s acceptance to changes acceptance to change
�� Documentation changes will need to be Documentation changes will need to be
made to accommodate more specificity in made to accommodate more specificity in
codingcoding
234234
IMPLEMENTATION PLANNINGIMPLEMENTATION PLANNING
�� Contact your system vendors earlyContact your system vendors early–– Will they be ready to accommodate ICDWill they be ready to accommodate ICD--10 on 10 on
schedule?schedule?
–– What costs will be involved with the transition?What costs will be involved with the transition?
–– Will they be ready to accept the 5010 electronic Will they be ready to accept the 5010 electronic
transaction standard required by HIPAA by transaction standard required by HIPAA by
January 1, 2012?January 1, 2012?
–– What are their plans for implementation?What are their plans for implementation?
–– When will they have software ready for testing?When will they have software ready for testing?
–– Is your current hardware adequate?Is your current hardware adequate?
235235
IMPLEMENTATION PLANNINGIMPLEMENTATION PLANNING
�� Develop your training planDevelop your training plan
–– Who needs training Who needs training –– physicians, coders, billing physicians, coders, billing
staff, administrative staff, clinical staffstaff, administrative staff, clinical staff
–– How much training will each classification of How much training will each classification of
personnel needpersonnel need
–– Establish your training schedule Establish your training schedule –– be realistic be realistic
�� Determine if temporary staff or overtime will Determine if temporary staff or overtime will
be needed during the training processbe needed during the training process
�� What materials will be neededWhat materials will be needed236236
IMPLEMENTATION PLANNINGIMPLEMENTATION PLANNING
�� Analyze your business processesAnalyze your business processes–– Identify all systems that utilize or are tied to Identify all systems that utilize or are tied to
ICDICD--99
–– Review existing policies related to ICDReview existing policies related to ICD--99
–– Do you have any payer contracts that are tied to Do you have any payer contracts that are tied to
ICDICD--99
–– If so modify those contracts before the payers If so modify those contracts before the payers
get wiseget wise
–– Carefully review any new contracts that are Carefully review any new contracts that are
received during implementation processreceived during implementation process
237237
IMPLEMENTATION PLANNINGIMPLEMENTATION PLANNING
�� Work with vendors to ensure that testing is Work with vendors to ensure that testing is
done before implementation datesdone before implementation dates
–– Volunteer to be a Volunteer to be a ““betabeta”” site for testingsite for testing
–– Integrate software into your systemsIntegrate software into your systems
–– Make internal customizationsMake internal customizations
–– Test systems with your clearinghouses, payers, Test systems with your clearinghouses, payers,
electronic systems electronic systems
–– Ensure vendors will maintain and update codes Ensure vendors will maintain and update codes
during the transition periodduring the transition period
238238
GEMsGEMs
�� GEMs are a crosswalk developed by CMS GEMs are a crosswalk developed by CMS
and CDC for use by all providers, payers, and CDC for use by all providers, payers,
and data users. The mappings are free of and data users. The mappings are free of
charge and can be found in the public charge and can be found in the public
domaindomain
�� http://http://www.cms.hhs.gov/MLNProducts/downwww.cms.hhs.gov/MLNProducts/down
loads/ICDloads/ICD--10_GEM_factsheet.pdf10_GEM_factsheet.pdf
�� http://www.cms.hhs.gov/MLNProducts/downhttp://www.cms.hhs.gov/MLNProducts/down
loads/ICDloads/ICD--10Mappingfctsht.pdf10Mappingfctsht.pdf239239
240240
ICDICD--1010--CM CODINGCM CODING
WHAT YOUR NEW CODING WORLD WILL WHAT YOUR NEW CODING WORLD WILL LOOK LIKELOOK LIKE
HYPERPARATHYROIDISMHYPERPARATHYROIDISM
�� E21.3 E21.3 –– Unspecified HyperparathyroidismUnspecified Hyperparathyroidism
�� E21.0 E21.0 –– Primary hyperparathyroidismPrimary hyperparathyroidism
�� N25.81 N25.81 –– Secondary hyperparathyroidism Secondary hyperparathyroidism
(renal)(renal)
�� E21.2 E21.2 –– Secondary hyperparathyroidism Secondary hyperparathyroidism
(non(non--renal)renal)
�� E21.2 E21.2 –– Hyperparathyroidism specified, Not Hyperparathyroidism specified, Not
elsewhere classifiedelsewhere classified
�� E21.2 E21.2 –– Tertiary hyperparathyroidismTertiary hyperparathyroidism241241
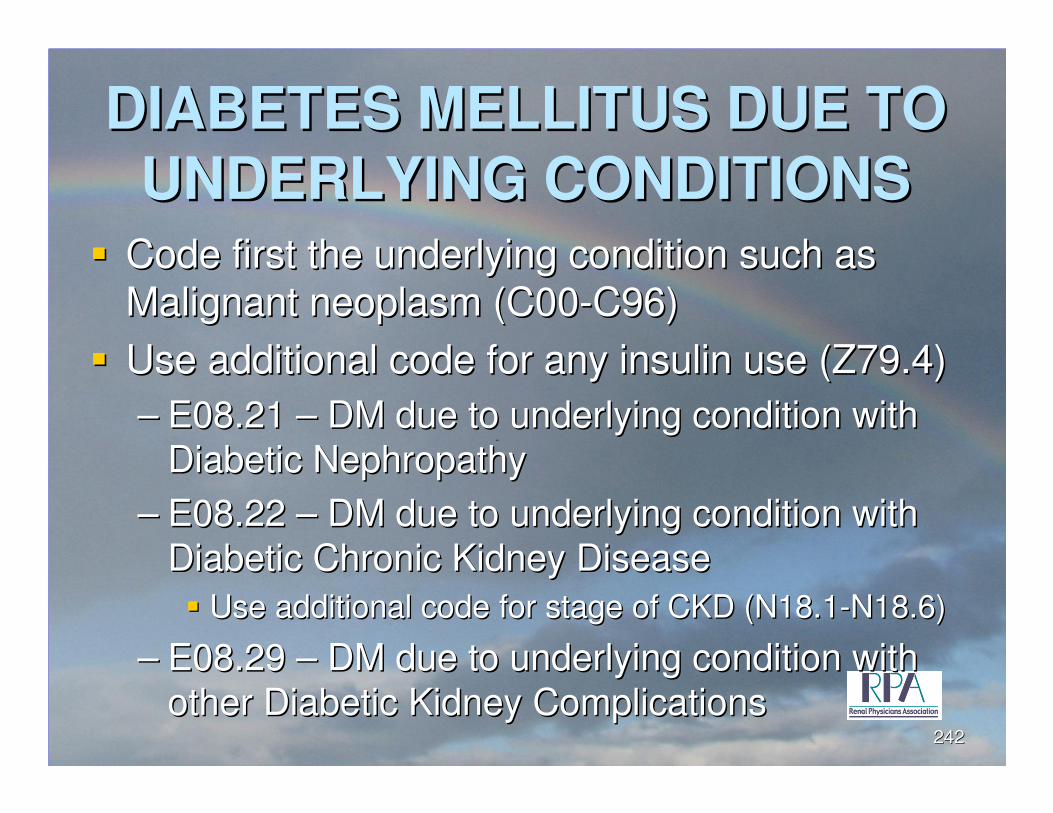
DIABETES MELLITUS DUE TO DIABETES MELLITUS DUE TO
UNDERLYING CONDITIONSUNDERLYING CONDITIONS�� Code first the underlying condition such as Code first the underlying condition such as
Malignant neoplasm (C00Malignant neoplasm (C00--C96)C96)
�� Use additional code for any insulin use (Z79.4)Use additional code for any insulin use (Z79.4)
–– E08.21 E08.21 –– DM due to underlying condition with DM due to underlying condition with
Diabetic NephropathyDiabetic Nephropathy
–– E08.22 E08.22 –– DM due to underlying condition with DM due to underlying condition with
Diabetic Chronic Kidney DiseaseDiabetic Chronic Kidney Disease
�� Use additional code for stage of CKD (N18.1Use additional code for stage of CKD (N18.1--N18.6)N18.6)
–– E08.29 E08.29 –– DM due to underlying condition with DM due to underlying condition with
other Diabetic Kidney Complicationsother Diabetic Kidney Complications242242
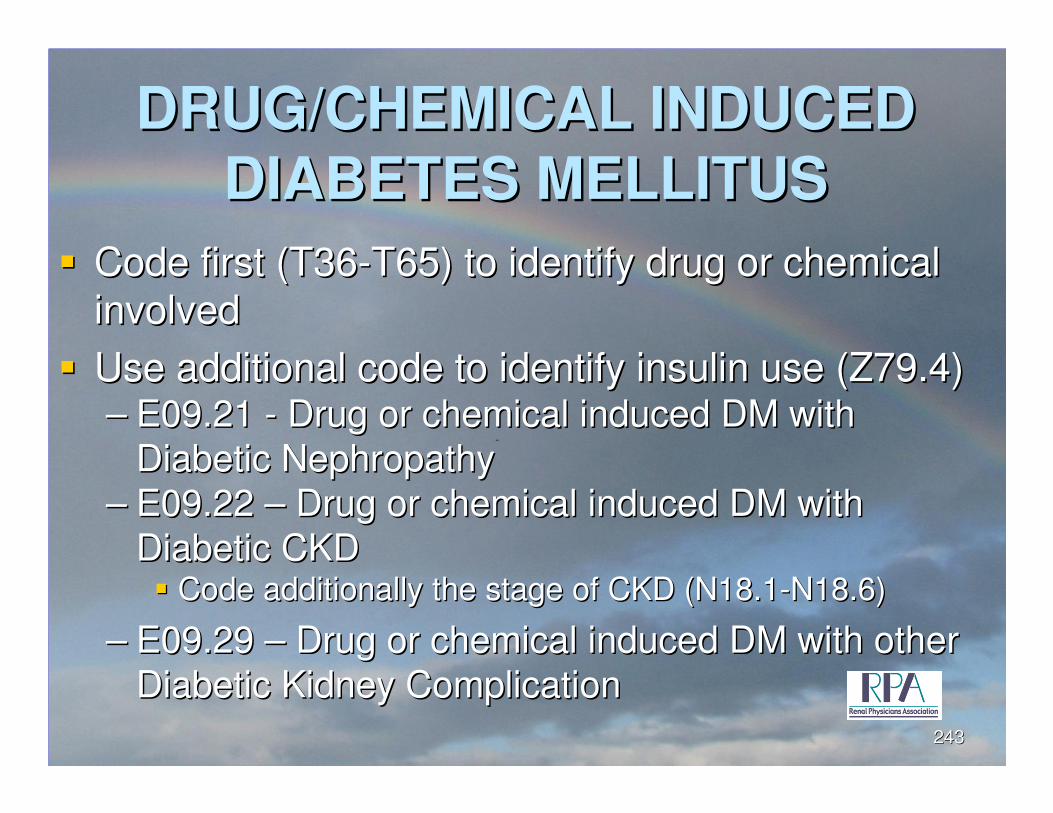
DRUG/CHEMICAL INDUCED DRUG/CHEMICAL INDUCED
DIABETES MELLITUSDIABETES MELLITUS
�� Code first (T36Code first (T36--T65) to identify drug or chemical T65) to identify drug or chemical
involvedinvolved
�� Use additional code to identify insulin use (Z79.4)Use additional code to identify insulin use (Z79.4)–– E09.21 E09.21 -- Drug or chemical induced DM with Drug or chemical induced DM with
Diabetic NephropathyDiabetic Nephropathy
–– E09.22 E09.22 –– Drug or chemical induced DM with Drug or chemical induced DM with
Diabetic CKDDiabetic CKD�� Code additionally the stage of CKD (N18.1Code additionally the stage of CKD (N18.1--N18.6)N18.6)
–– E09.29 E09.29 –– Drug or chemical induced DM with other Drug or chemical induced DM with other
Diabetic Kidney ComplicationDiabetic Kidney Complication
243243
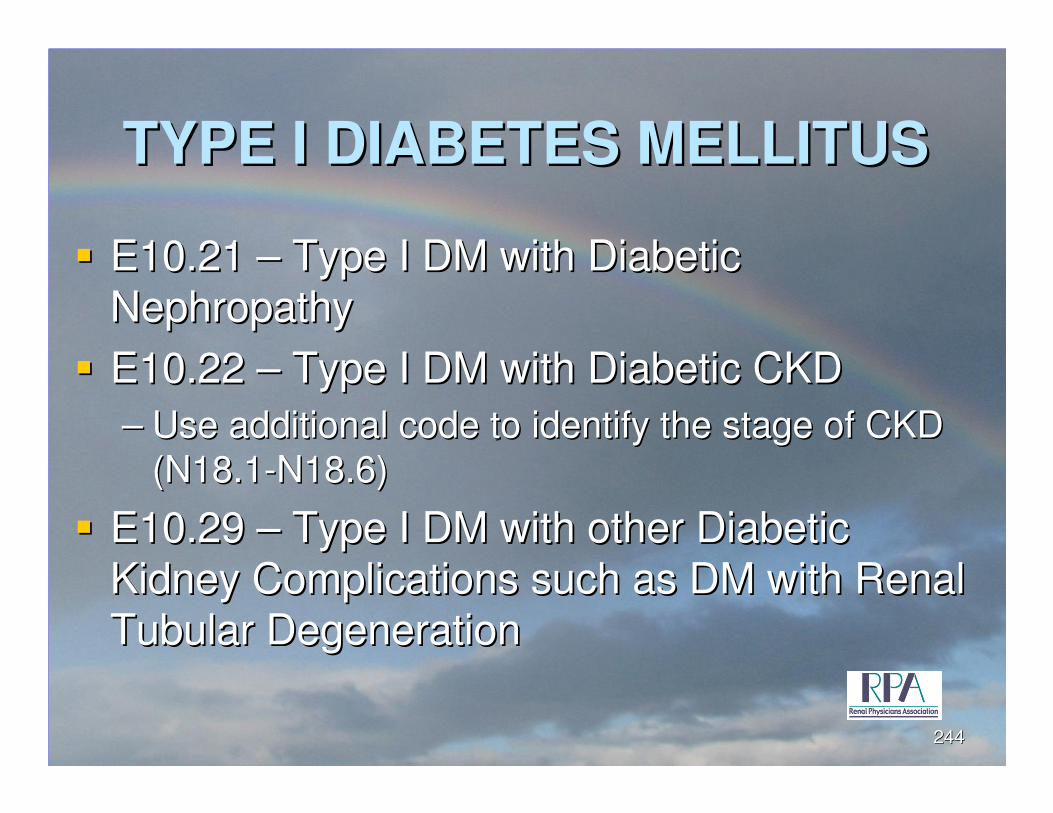
TYPE I DIABETES MELLITUSTYPE I DIABETES MELLITUS
�� E10.21 E10.21 –– Type I DM with Diabetic Type I DM with Diabetic
NephropathyNephropathy
�� E10.22 E10.22 –– Type I DM with Diabetic CKDType I DM with Diabetic CKD
–– Use additional code to identify the stage of CKD Use additional code to identify the stage of CKD
(N18.1(N18.1--N18.6)N18.6)
�� E10.29 E10.29 –– Type I DM with other Diabetic Type I DM with other Diabetic
Kidney Complications such as DM with Renal Kidney Complications such as DM with Renal
Tubular DegenerationTubular Degeneration
244244
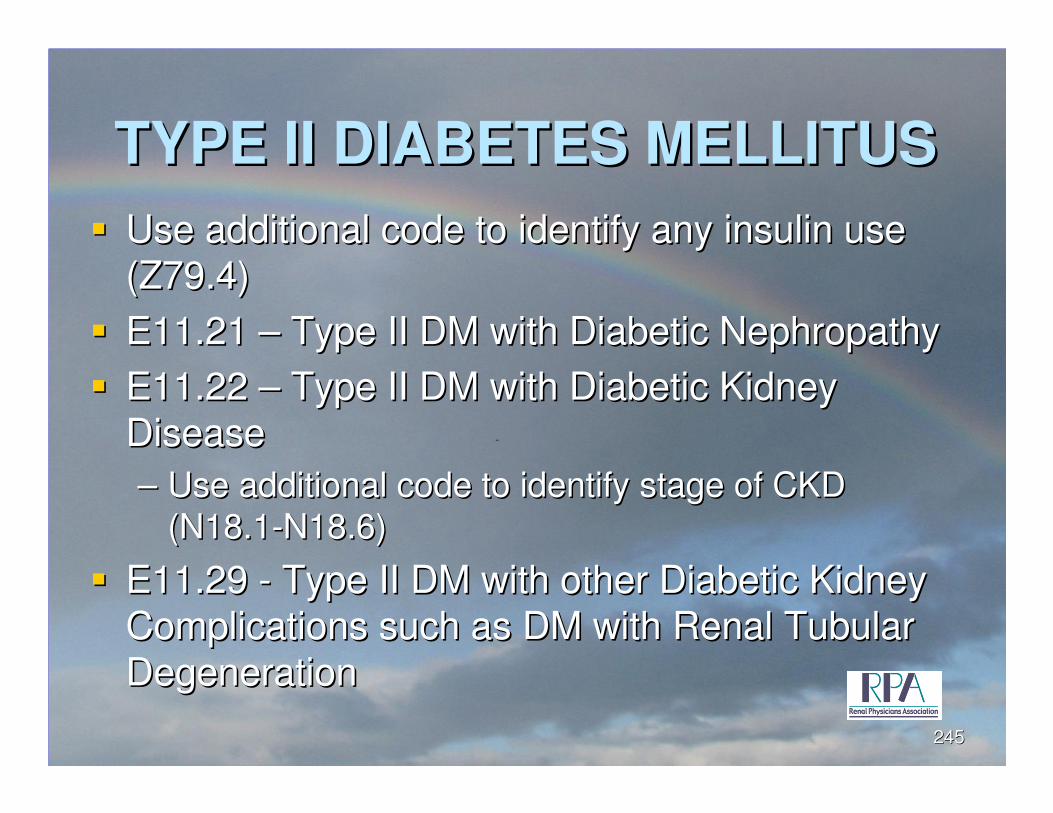
TYPE II DIABETES MELLITUSTYPE II DIABETES MELLITUS
�� Use additional code to identify any insulin use Use additional code to identify any insulin use
(Z79.4)(Z79.4)
�� E11.21 E11.21 –– Type II DM with Diabetic Nephropathy Type II DM with Diabetic Nephropathy
�� E11.22 E11.22 –– Type II DM with Diabetic Kidney Type II DM with Diabetic Kidney
DiseaseDisease
–– Use additional code to identify stage of CKD Use additional code to identify stage of CKD
(N18.1(N18.1--N18.6)N18.6)
�� E11.29 E11.29 -- Type II DM with other Diabetic Kidney Type II DM with other Diabetic Kidney
Complications such as DM with Renal Tubular Complications such as DM with Renal Tubular
DegenerationDegeneration
245245
ESSENTIAL PRIMARY ESSENTIAL PRIMARY
HYPERTENSIONHYPERTENSION
�� I10 I10 –– Includes high blood pressureIncludes high blood pressure
Malignant HypertensionMalignant Hypertension
Benign HypertensionBenign Hypertension
246246
HYPERTENSION CHRONIC HYPERTENSION CHRONIC
KIDNEY DISEASEKIDNEY DISEASE
�� I12.0 I12.0 –– Hypertensive chronic kidney disease Hypertensive chronic kidney disease
Stage 5 CKD or End Stage Renal DiseaseStage 5 CKD or End Stage Renal Disease
–– Use additional code to identify stage of CKD Use additional code to identify stage of CKD
(N18.5 or N18.6)(N18.5 or N18.6)
�� I12.1 I12.1 –– Hypertensive chronic kidney disease Hypertensive chronic kidney disease
Stage 1Stage 1--4 or unspecified CKD 4 or unspecified CKD
–– Use additional code to identify stage of CKD Use additional code to identify stage of CKD
(N18.1 (N18.1 -- N18.4)N18.4)
247247
SECONDARY HYPERTENSIONSECONDARY HYPERTENSION
�� Code also underlying primary conditionCode also underlying primary condition
�� I15.0 I15.0 –– Renovascular HypertensionRenovascular Hypertension
�� I15.9 I15.9 –– Secondary Hypertension, Secondary Hypertension,
unspecifiedunspecified
248248
CHRONIC KIDNEY DISEASECHRONIC KIDNEY DISEASE
�� Code first any associated:Code first any associated:
–– Diabetic chronic kidney disease (E08.22, E09.22, Diabetic chronic kidney disease (E08.22, E09.22,
E10.22, E11.22, E13.22)E10.22, E11.22, E13.22)
–– Hypertensive chronic kidney disease (I12.X, Hypertensive chronic kidney disease (I12.X,
I13.X)I13.X)
�� Use additional code to identify kidney Use additional code to identify kidney
transplant status, if applicable (Z94.0)transplant status, if applicable (Z94.0)
249249
CHRONIC KIDNEY DISEASECHRONIC KIDNEY DISEASE
�� N18.1 N18.1 –– Chronic kidney disease, Stage 1Chronic kidney disease, Stage 1
�� N18.2 N18.2 –– Chronic kidney disease, Stage 2Chronic kidney disease, Stage 2
�� N18.3 N18.3 –– Chronic kidney disease, Stage 3Chronic kidney disease, Stage 3
�� N18.4 N18.4 –– Chronic kidney disease, Stage 4Chronic kidney disease, Stage 4
�� N18.5 N18.5 –– Chronic kidney disease, Stage 5Chronic kidney disease, Stage 5
�� N18.6 N18.6 –– End Stage Renal Disease requiring End Stage Renal Disease requiring
dialysisdialysis
–– Use additional code to identify dialysis status Use additional code to identify dialysis status
(Z99.2)(Z99.2)250250
ACUTE KIDNEY FAILUREACUTE KIDNEY FAILURE
�� Code also associated underlying conditionCode also associated underlying condition
�� N17.0 N17.0 –– AKF with tubular necrosisAKF with tubular necrosis
�� N17.1 N17.1 –– AKF with acute cortical necrosisAKF with acute cortical necrosis
�� N17.2 N17.2 –– AKF with medullary necrosisAKF with medullary necrosis
�� N17.8 N17.8 –– Other acute kidney failureOther acute kidney failure
�� N17.9 N17.9 –– Acute kidney failure, unspecifiedAcute kidney failure, unspecified
251251
KIDNEY TRANSPLANTKIDNEY TRANSPLANT�� Z94.0 Z94.0 –– Kidney transplant statusKidney transplant status
�� Do not code with complications of transplantDo not code with complications of transplant
–– T86.10 T86.10 –– Unspecified complication of kidney Unspecified complication of kidney
transplanttransplant
–– T86.11 T86.11 –– Kidney transplant rejectionKidney transplant rejection
–– T86.12 T86.12 –– Kidney transplant failureKidney transplant failure
–– T86.13 T86.13 –– Kidney transplant infectionKidney transplant infection
�� Use additional code to specify infectionUse additional code to specify infection
–– T86.19 T86.19 –– Other complication of kidney Other complication of kidney
transplanttransplant
252252
253253
Final ThoughtsFinal Thoughts
The Driving Force The Driving Force --
$$$ $$$
Been thereBeen there--done done
that! that!
Prove it!Prove it!
254254
CONTACT INFORMATIONCONTACT INFORMATION
�� Debra Lawson, CPC, PCSDebra Lawson, CPC, PCS–– [email protected]@NBandMS.com
�� Renal Physicians AssociationRenal Physicians Association–– 11--800800--RPARPA--75257525
–– www.renalmd.orgwww.renalmd.org�� American College of Medical Coding SpecialistsAmerican College of Medical Coding Specialists
–– 11--800800--946946--94029402–– www.acmcs.orgwww.acmcs.org. .
�� American Academy of Professional CodersAmerican Academy of Professional Coders–– 11--800800--626626--CODECODE
–– www.www.aapc.comaapc.com
Recommended

















