276 AMERICAN JOURNAL OF OPHTHALMOLOGY August, 1986
planation tonometry was R.E.: 29 mm Hg andL.E.: 31 mm Hg. Gonioscopy disclosed an openanterior chamber angle without abnormality.Biomicroscopic findings were normal. Goldmann perimetry visual field testing showed aninferior nasal step in the left eye and a normalvisual field in the right eye. Ophthalmoscopydisclosed a cup-disk ratio of 0.6 without rimencroachment in the right eye and 0.7 withsuperior temporal rim encroachment in the lefteye. My impression was early chronic openangle glaucoma, for which I prescribed a monocular therapeutic trial of timolol 0.5%, onedrop twice daily in the left eye.
Two weeks later, intraocular pressure by applanation tonometry was 18 mm Hg in eacheye; four months later, it was R.E.: 19 mm Hgand L.E.: 21 mm Hg. When timolol was discontinued for two weeks, the intraocular pressurewas R.E.: 28 mm Hg and L.E.: 30 mm Hg atabout the same time.
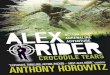
Subsequent monocular therapeutic trials oftimolol 0.5% once a day in either eye for various intervals decreased intraocular pressure inthe untreated eye almost as much as in thetreated eye (Figure). The average decrease inresponse to timolol 0.5% once or twice a daywas 13.2 mm Hg in the treated eye and 11.4 mm
30 ~ClJ:EE'-' 20DO
10
.6
~\ .; ~ -0 ..- ~.
Hg in the untreated eye, an average differenceof only 1.8 mm Hg between the two eyes.According to the principle of monocular therapy, therefore, timolol once or twice a day apparently does not substantially decrease intraocular pressure in the treated eye compared tothe untreated eye. However, instillation oftimolol once or twice a day in one eye of thispatient did result in a substantial decrease inintraocular pressure in both eyes compared tobaseline measurements.
Since I encountered this seemingly unusualphenomenon, I have discovered Seven morepatients in whom monocular treatment withtimolol 0.5% decreased intraocular pressure inthe untreated fellow eye as much as in thetreated eye.
References
1. Kolker, A. E., and Hetherington, J., [r.: BeckerShaffer's Diagnosis and Therapy of the Glaucomas.St. Louis, C. V. Mosby, 1983, pp. 247 -249.
2. Leydhecker, W., Krieglstein, G., and Kollani,E.: Observer variation in applanation tonometry andestimation of the cup disc ratio. In Krieglstein, G.,and Leydhecker, W. (eds.): Glaucoma Update. Berlin, Springer-Verlag, 1979, p. 101.
3. Smith, J., and Wandel, T.: Rationale for theone-eye therapeutic trial. Ann. Ophthalmol. 18:8,1986.
4. Zimmerman, T. J., and Kaufman, H. E.:Timolol. A l3-adrenergic blocking agent for the treatment of glaucoma. Arch. Ophthalmol. 95:601, 1977.
5. Zimmerman, T. J., Kass, M. A., Yablonski,M. E., and Becker, B.: Timolol maleate. Efficacy andsafety. Arch. Ophthalmol. 97:656, 1979.
o 4 12 20 28 36 44 52
Time (weeks)Figure (Shin). Plot of intraocular pressures during
mocular therapy with timolol 0.5% once or twice aday for various intervals. The intraocular pressureswere measured by Goldmann applanation tonometryat about the same time of day throughout a 52-weekperiod. Circles indicate right eyes and triangles indicate left eyes. Solid figures indicate monocular treatment and open figures indicate discontinuation oftreatment.
Sequential Retinal Tears Attributedto Intraocular Gas
Richard F. Dreyer, M.D.Department of Ophthalmology, University of Iowa.Inquiries to Richard F. Dreyer, M.D., Oregon Lions Sight& Hearing Institute, Portland, OR 97210.
New retinal breaks in an eye with a rhegmatogenous retinal detachment occur with a frequency of 7% to 10% and are an importantcause of failed detachment surgery.I" I recentlytreated a patient in whom the injection ofintraocular gas after uneventful retinal reat-

Vol. 102, No. 2 Letters to The Journal 277
tachment surgery seemed to cause three newretinal breaks and a bullous retinal detachment.
A 70-year-old man was referred with a rhegmatogenous retinal detachment involving thesuperior retina in his right eye. Fifteen monthsearlier he had undergone extracapsular cataractsurgery with a posterior chamber lens implantfollowed by YAG laser capsulotomy severalmonths later. Examination of the right anteriorsegment showed the intraocular lens to be ingood position with a small central opening inthe posterior capsule. A superior retinal detachment was present with three flap tears andone atrophic hole associated with lattice degeneration. The view of the inferior retina wasclear and there were no tears or subretinal fluidinferiorly (Fig. 1). An uneventful retinal reattachment procedure was performed with a silicone exoplant and partial drainage of subretinal fluid.
On the first postoperative day, residual subretinal fluid persisted with elevated retinalfolds over the exoplant. Because the folds communicated with the superotemporal flap tearand no appreciable settling of the retina hadoccurred, 0.25 ml of 100% sulfur hexafluoridewas injected via the inferotemporal pars plana,3 mm posterior to the corneoscleral limbuswhile the patient was under topical anesthesia.
Fig. 1 (Dreyer). Superior rhegmatogenous retinaldetachment in right eye. Two of the three flap tears(arrows) and the atrophic hole (arrowhead) are associated with visible lattice degeneration.
prominentinsertion
vitreousbase
Fig. 2 (Dreyer). The superior retina has reattached,but three new tiny flap tears (arrows) have resultedin an inferior detachment. There is a prominentinsertion of the posterior vitreous base.
There were no complications with this procedure, including no incarceration of vitreous atthe injection site.
The next morning, there was marked flattening of the superior retina. The inferior retinaremained completely attached. On the nextmorning, the superior retina was completelyattached. However, there was an inferior bullous retinal detachment with three, small,aphakic flap tears not associated with latticedegeneration (Fig. 2). The silicone exoplantwas extended circumferentially to cover thesethree tears and no drainage of subretinal fluidwas performed. The retina reattached and theremainder of the postoperative course was unremarkable.
In this case, several features suggest that theinjection of intraocular gas caused the newbreaks. First, the new breaks were differentfrom the existing breaks in that the originalbreaks occurred in areas of lattice degenerationand were of moderate size. The new breakswere tiny, aphakic tears occurring just posterior to the vitreous base. Second, the appearanceof these breaks occurred 180 degrees away fromthe position of the air bubble superiorly where

278 AMERICAN JOURNAL OF OPHTHALMOLOGY August, 1986
one might predict the greatest traction on thevitreous base might occur. Third, the newbreaks appeared the second day after the injection of intraocular gas whereas Goldberg andBoyer' indicated that spontaneous sequentialretinal breaks occurred over a period of threedays to 22 months. The early appearance of th.enew breaks in this patient suggested that thenappearance was temporally related to the injection of intraocular gas. Fourth, it is more usualfor new retinal tears to be located near an initialretinal break, whereas the tears in my patientwere located far away.'
The presumed mechanism for formation ofnew retinal breaks in this patient was the presence of an intraocular gas bubble that shiftedsuperiorly when the patient was sitting, placing traction on the inferior vitreous base creat-ing three additional tiny flap tears. .
This case suggests that the postoperativeinjection of intraocular gas may cause newretinal breaks. The vitreoretinal surgeon employing this technique to speed resorpt.ion ofsubretinal fluid should be aware of this andexamine the peripheral retina of patients treated with injection of intraocular gas for newvitreous base tears.
References
1. Goldberg, R. E., and Boyer, D. S.: Sequentialretinal breaks following a spontaneous initial retinalbreak. Ophthalmology 88:10. 1980.
2. Rachal, W. F., and Burton, T. c.. Changingconcepts of failures after retinal detachment surgery.Arch. Ophthalmol. 97:480, 1979.
3. Robertson, D. M., and Norton, E. W. D.: Causeof failure in prophylactic treatment of retinal breaks.Mod. Probl. Ophthalmol. 12:74, 1974.
Effect of Intravenous Fluorescein onFluorescent Treponemal AntibodyTesting
Bradley F. Jost, M.D.,R. Joseph Olk, M.D.,Mark H. Spurrier, M.D.,and Lisa F. Rosenberg, M. D.Department of Op~t~almology, Washington University School of Medicine.
Inquiries to R. Joseph Olk, M.D., East Pavilion, Suite17413,4949 Barnes Hospital Plaza, St. Louis, MO 63110.
Before the discovery of penicillin, syphiliswas considered to be an important cause ofocular disease. Despite our ability to treatsyphilis, there has been an increase in its incidence in recent years and an anticipated corresponding increase in cases of late ocular syphilis and neurosyphilis.' Recent reports haveemphasized the importance of considering thediagnosis of syphilis in cases of necrotizinpretinitis, acute chorioretinitis, retinal vasculitis, and pseudoretinitis pigmentosa.v" Manyophthalmologists include fluorescein angiography in the clinical evaluation of patients withthese conditions.
Patients with suspected syphilis should betested with the VDRL test to assess currentsyphilitic activity as well as o~e of themal antigen tests, which are highly specific .andsensitive for confirming current or previousinfection with Treponema pallidum. The fluorescent treponemal antibody-absorption (FTAABS) test is the most commonly used treponemal antigen test." This test uses rabbitantihuman globulin labeled with fluore~cein
isothiocyanate. Fluorescence of T. pallidumcells reacted with patient serum is graded fromnegative to 4+. Because of the use ofcence in grading test results, some cliniciansbelieve that false-positive FTA-ABS test resultsmay occur if serum ~s obtained sho.rt~y afterintravenous fluorescein has been administered.
In an effort to clarify this issue, four healthyvolunteers underwent serial FTA-ABS testingafter intravenous fluorescein administration.Before fluorescein injection, baseline VDRL,FTA-ABS, and microhemagglutination T. pallidum tests were performed, and negative resultswere obtained for all subjects. After intravenous injection of 5 ml of 10% fluorescein sodium, serum for FTA-ABS testing was collectedone hour, three hours, six hours, and 24 hourslater. The Zeus Scientific Inc. FTA-ABS TestSystem was used to evaluate the ser~. Negativeresults were obtained for all test subjects for alltime periods.
These findings suggest that intravenous fluorescein does not produce false-positive resultswith the method of FTA-ABS testing currentlyused in our laboratory when applied to the seraof healthy individuals. If any doubt exists regarding FTA-ABS testing by ot~er lab~ratorymethods, we suggest concomitant microhemagglutination T. pallidum testing which relies
Recommended