SPONTANEOUS DISSECTION OF THE CAROTID AND VERTEBRAL ARTERIES N Engl J Med, Vol.
344, No. 12. March 22, 2001
950518
張維傑
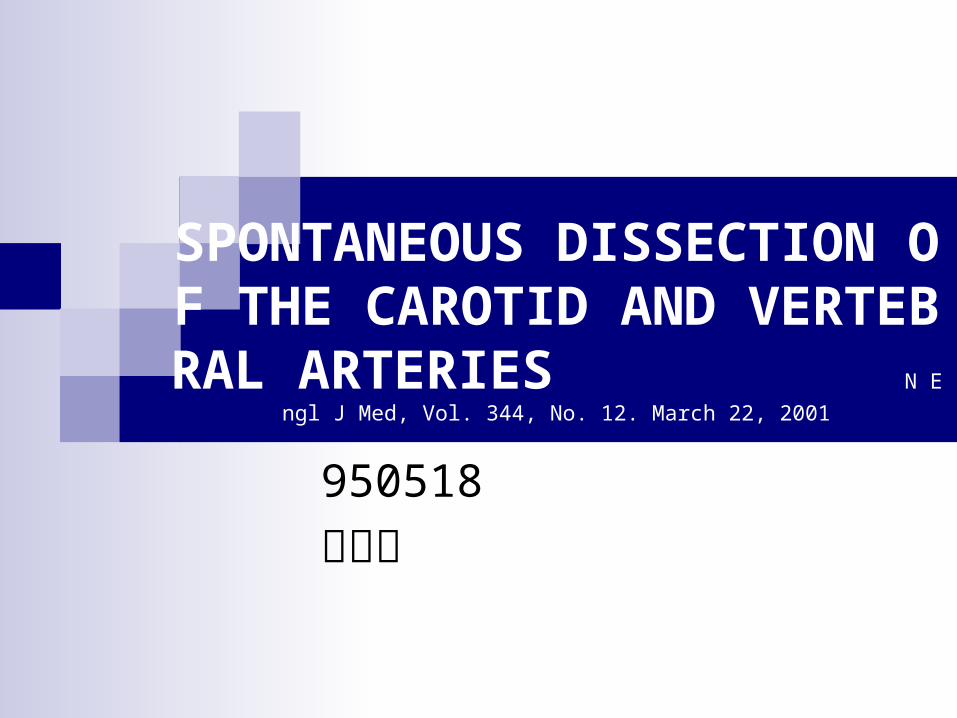
Mr. Jou, 42 yrs Male, sudden onset of blindness and recovery 2 years ago. Headache and tinnitus for one month
Introduction
Till the late 1970s, when Fisher et al. and Mokri et al. described dissections of carotid and vertebral arteries
Blood entered the wall of the artery and split its layers, either stenosis or aneurysmal dilatation
EPIDEMIOLOGIC FEATURES
2.5-3 /100000, 2 % of all ischemic stroke, 10-15% young and middle-aged ischemic stroke patients
all age groups, including children, but there is a distinct peak in the fifth decade of life
Female average about five years younger than men at the time of the dissection.
PATHOLOGICAL FEATURES
Extracranial segments, the greater mobility, contact with bony structures
arise from an intimal tear >> intramural hematoma: subintimal dissection >stenosis; subadventitial dissection >aneurysmal formation

PATHOGENESIS Genetic Factors1. Connective-tissue disorder: (1-5%) Ehl
ers–Danlos syndrome type IV. Marfan’s syndrome, autosomal dominant polycystic kidney disease, and osteogenesis imperfecta type I.
2. The arterial media of the aorta melanocytes, and the aortic valvular cusps derived from neural-crest cells,
3. Fibromuscular dysplasia(15%)
Environmental Factors1. Hyperextension or rotation of the neck:
yoga, painting a ceiling, coughing, vomiting, sneezing, the act of resuscitation
2. Chiropractic manipulation of the neck: 1 in 20,000 spinal manipulations
3. Respiratory tract infection: with a peak incidence in the fall.
4. Vascular disease: tobacco use, hypertension,
5. migraine as a risk factor for dissection.
CLINICAL MANIFESTATIONS Dissection of the Internal Carotid Artery1. Pain on one side of the ipsilateral headache (fronto
temporal, “thunderclap”), face, or neck accompanied by a partial Horner’s syndrome
2. Oculosympathetic palsy: miosis, ptosis, (No facial anhidrosis: ECA sympathetic plexus)
3. Cranial-nerve palsies(12%):the most commonly the hypoglossal nerve, Impairment of taste, ¼ Pulsatile tinnitus
4. Cerebral or retinal ischemic symptoms (50-90%), Permanent blindness as a result of ischemic optic neuropathy or occlusion of the retinal artery: rare
Vertebral-Artery Dissection
1. Pain in the back of the neck (1/2), occipital area headache(2/3)
2. Ischemic symptoms(90%), brain stem, particularly the lateral medulla (Wallenberg’s syndrome),
3. Transient ischemic attacks are less frequent after vertebral-artery dissections than after carotid-artery dissections.
DIAGNOSTIC TESTS
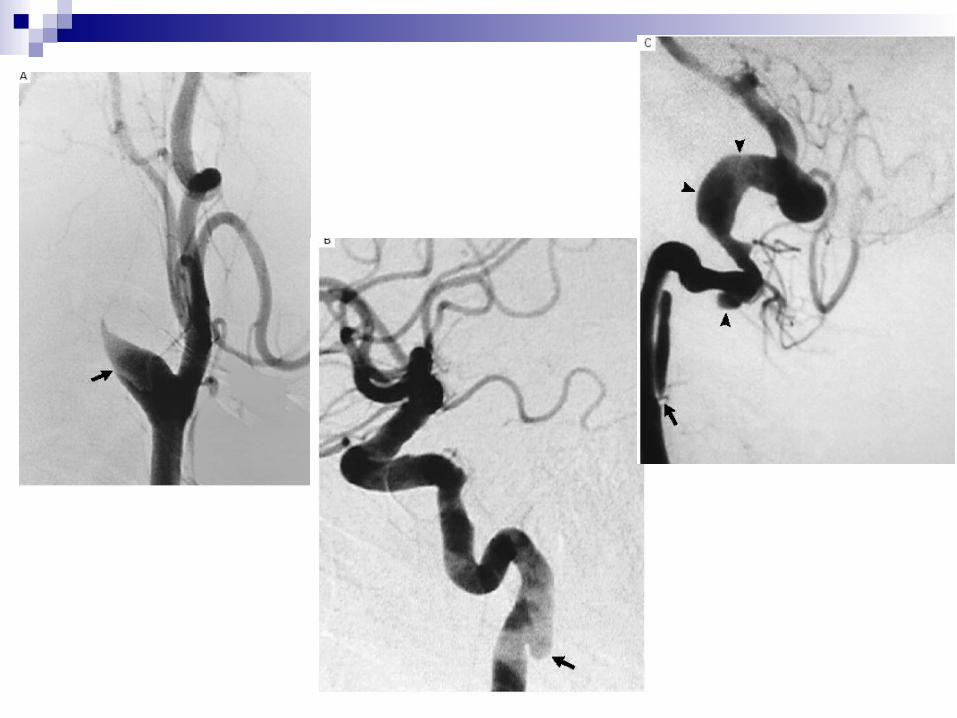
Conventional angiography: gold standard Starts about 2 to 3 cm distal to the carotid bulb,
not past its entry into the petrous portion Flame-like appearance in acute phase Aneurysmal type: most commonly in distal subcr
anial segment Both stenotic and aneurysmal lesions of vertebra
l arteries are most common in distal segment of the artery at the level of the first and second cervical vertebrae
The vertebral artery enters the skull through the foramen magnum: 10 % vertebral-artery dissections extend intracranially.
Magnetic resonance techniques are replacing the gold standard
Ultrasonographic techniques are useful in the initial: an abnormal pattern of flow is identified in more than 90 percent
Helical computed tomographic angiography
PROGNOSIS
The rate of death from dissections of the carotid and vertebral arteries <5%, ¾ recovery well
The radiographic appearance may worsen during the acute phase of dissection, about 90 percent of stenoses eventually resolve, two thirds of occlusions are recanalized, and one third of aneurysms decrease in size within the first two to three months, thromboembolic complications years after the dissection but they never rupture.
2% recurrent dissection in initially unaffected vessels in first month, then decreased rate 1% per year
TREATMENT To prevent thromboembolic complications: intravenous h
eparin >> oral warfarin recommended for all patients Because 90 percent of infarcts due to are thromboemboli
c rather than hemodynamic (i.e., caused by insufficient flow)
Anticoagulation with a target PTINR: 2.0 to 3.0 for 3-6 months, MRA in 3 months, if luminal irregularities medication for another 3 months
Recanalization within the first three months after the dissection symptoms occasionally recur within three to six months after the onset of dissection rarely after six months.
no symptoms of ischemia: antiplatelet therapy alone,
Surgical or endovascular treatment should be reserved for patients who have persistent symptoms of ischemia despite adequate anticoagulation.
Ligation of the carotid or vertebral artery, combined with an in extracranial-to-intracranial bypass.
Balloon angioplasty placement of one or more metallic stents,
The long-term results of carotid stenting are unknown
Recommended