The Urinary System
Anatomy and
Physiology
2014

Structure
KidneysUretersUrinary bladderurethra

Function
Maintains homeostasisControls blood and water
volumeMaintains blood pressureRegulates electrolyte levels

Eliminates protein wastes, excess salts and toxic materials from blood
Balances acid/base (PH)Secretes renin and
erythropoietin



Kidney Structure
2 reddish brown, bean-shaped organs
Located in small of the back at lower edge of ribs on either side of spine
“Retroperitoneal”


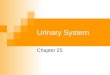
How the kidneys Regulate BP
ADH
RENIN
ALDOSTERONE

3 Parts
CortexMedullaPelvis

BecomeHealthyNow.com Home

Nephron
Functional units of the kidney
Cells that form urineOver 1 million nephrons in
each kidney

Glomerular Filtration
Tubular Reabsorption
Tubular Secretion

WORD WALL
1. Oliguria
2. Anuria
3. Dysuria
4. Polyuria
5. hematuria

Urine
Body excretes 1000-2000 ml of urine/day
Is normally sterileColor varies with hydration

Characteristics of Normal Urine
CLARITY
ODOR
SPECIFIC GRAVITY

THINK….
A STRONG, OFFENSIVE ODOR FROM FRESHLY VOIDED URINE IS SUGGESTIVE OF……..
Urinary Tract Infection

Composition of Normal Urine
WaterProtein wastes products
(urea, uric acid & creatinine)Excessive minerals from diet
(Na+,K+, Ca,sulfates & phosphates

ToxinsHormonesBile compoundsPigments from food/drugs

WORD WALL
FrequencyUrgency NocturiaEnuresisretention

Effects of Aging on the Urinary System
Ability to filter blood, reabsorb electrolytes & secrete wastes decreases
Less ability to return to normal after changes in blood volume

Decrease in number & size of nephrons
Decrease in GFRSmaller capacity of bladderWeaker bladder muscles

Incontinence
Not a normal consequence of age
Common due to many reasonsSee Chpter 23 for more
information on incontinence

Critical Thinking ChallengeCOMPARE & CONTRAST STRESS vs.
FUNCTIONAL
COMPARE & CONTRAST URGE vs. OVERFLOW

Nursing Assessmentof
The Urinary
System

HEALTH HISTORY
Chief complaintHistory of Present IllnessPast Medical HistoryFamily HistoryReview of Systems

Diagnostic & Laboratory Tests
Urinary System

URINE TESTS UA ( urinalysis )
C & S ( Culture & Sensitivity )
Creatinine Clearance (24 hr)

BLOOD TESTS
BUN ( blood urea nitrogen )
Serum Creatinine
Serum Electrolytes

Radiographic Studies
KUB ( flat plate ) IVP Arteriogram Renal Scan US

Invasive Procedures
1. Renal Biopsy
2. Cystoscopy

What are
Urodynamic Studies ??

What are common Therapeutic measures
Related to
“Catheterization”

Catheter Types
Foley
Ureteral
Suprapubic
Nephrostomy

Common Tubes and Catheters
Ureteral Catheter
Nephrostomy Tube
Urinary Stent

Pre-Op Care Urologic Surgery
Evaluate fluid status
Bowel cleansing
Enterostomal Therapist/Nurse
Counseling/Teaching

Post-Op Care Urologic Surgery
Report to MD U/O < 30 ml/hr
Pain Management
Mon. lung sounds
Assess for Paralytic ileus

Urinary Tract
Inflammation and Infections

Cystitis
Inflammation of the urinary bladder
Bacteria enters from the urethra, lymph nodes, infected kidneys
Women more suseptible

Causes
E-coliCandida AlbicansCoitusDiabetes mellitusSee Box 40-2 Risk Factors
for UTI’s

Signs & Symptoms
Dysuria, hematuriaFrequency, urgencyLow grade feverPelvic or abd. discomfortBladder spasms

Med. Dx & Tx
C&S and UA obtained Increase fluids 3-4 L / dayAntibiotics
(Cipro,Bactrim,SeptraAnalgesics(Pyridium)See Pt. Teaching pg. 898

Gerontologic Considerations
Watch for signs of mental confusion
Fever may be maskedSepsis develops quickly

Pyelonephritis
Bacterial infection of renal pelvis and kidney
Most common form of kidney disease
Often the result of reflux

Signs & Symptoms
Flank painChills, fever,N & VDysuria, fatiqueBladder irritation

Med & Nursing Considerations
Bedrest Increase fluids (8 8oz. Glasses
water/day) IV Monitor I + OProtein & Na+ restrictionsMon. for circulatory overload

Pharmacological TX
Antibiotics (Bactrim) or Cipro
AntipyreticsAnalgesics AntispasmoticsAntihypertensives

Glomerulonephritis
Autoimmune diseaseGlomerulus becomes
inflammedSymptoms dev. 1-3 wks after
respiratory infection cau by group A- hemolytic strep

Signs & Symptoms
Tea colored urineDecrease in u/oPeriobital edemaHTNHypervolemia

Medical Dx
Clinical PresentationUA ProteinuriaBUN, CrStrep. Antibody TestsRenal Biopsy or Ultrasound

Medical Treatment
Diuretics
Antihypertensives
Antibiotics

Nursing Considerations
Bedrest several weeksStrict I & O, daily weightsRestrict Fluids if orderedLow Na, low protein dietPrognosis is good

UA w/ RBC’s, Albumin, casts
protein

Treatment
Low Na, protein dietBedrestVS, BP…Strict I & ORestrict fluids

Condition may lead to pulmonary edema, increased BP,anemia,cerebral hemorrage, CHF and ultimately uremia or ESRD

In the absence of dialysis or kidney transplant, prognosis is poor.

Polycystic Kidney Disease
Congenital, familial, also may be acquired
Fluid-filled cystsAbdominal, low back or
flank pain and headache

Diagnosis
X-ray or sonogramBUN & CreatinineGoal of management is…..

Renal Failure
A.K.A. Uremia
May be Acute or Chronic

Renal Failure
Kidneys no longer meet everyday demands
Kidneys unable to filter waste products from blood
BUN & Creatinine levels elevate

Causes of Renal Failure
GlomerulonephritisIDDMAny condition which
decreases blood supply to kidneys

InjuryRecurrent UTIDrug overdosePoisoningNephrotoxic Drugs

Acute Renal Failure
CAUSED BY:
1. Prerenal Failure
2. Intrarenal Failure
3. Postrenal Failure

Acute Renal Failure
4 PHASES1.Onset2.Oliguria3.Diuresis4.Recovery

Medical & Drug Management
AntihypertensivesDiureticsCardiotonicsDialysis if needed

Diet & Fluids
Diet based on consideration of serum electrolytes and BUN. Adequate carbs to prevent breakdown of fat & protein.
Fluids calculated by adding 400-600ml to previous days output.

Nursing Considerations
Freq. BUN, Creatinine, Na & K levels
Usually Low Na, K and protein diet
Mon. I & O

Chronic Renal Failure“ESRD”
IrreversibleChronic abnormalities in
internal environment of kidney
Dialysis or kidney transplant necessary for survival

Signs & Symptoms• Azotemia • Hyperkalemia• Hypocalcemia• Metabolic acidosis• Hypernatremia and
hypervolemia• Insulin Resistance

Medical Treatment
IV Glucose and Insulin Calcium, Vitamin D and phosphates Fluid restriction & diuretics Beta blockers, calcium channel blockers
and ACE inhibitors Iron, folic acid and synthetic
erythropoietin High carb/low protein diet

Urinary Tract Obstructions
RENAL CALCULI

Urolithiasis
Calculus or stone formed in the urinary tract
Etiology is unknownCan occur in renal pelvis,
ureters, bladder or urethra

Contributing Factors
Infection & or DehydrationUrinary stasis ImmobilityRecurrent UTI’sDiet low in calcium

Signs & Symptoms
Size & location of stone affects degree of pain
Spasm = “colic”HematuriaN & V

Medical Treatment
OpioidsNSAIDSAntispasmodics IV FluidsAntibiotics

Surgical Management
Lithotripsy (ESWL)UrethroscopyNephrolithotomySee Post-Op Care Goals pg.
906

Nursing Considerations
Strain all urine & pain reliefSend gravel or stones to labMonitor of s/s infectionGive antispasmodics Encourage fluids ; IVManage Pain

Hydronephrosis
Distention of kidneyCan cause permanent damageMaintain accurate I & OStrain all urineSend all stones for analysis

Dialysis• Mechanical• Imitates the function of the
nephron• May be chronic or acute• Removes body wastes through
semipermeable membrane

Dialysis
PeritonealHemodialysis

HemodialysisBlood circulates through a
machine outside the bodySemipermeable membrane is
within machine“Artificial kidney”Performed 3x/wk for approx.
4 hrs


AV Shunts, fistula or cannula
All allow access to the arterial system
All must be assessed for patency by:
“Feel the thrill” & “listen for the bruit”

http://classes.kumc.edu/cahe/respcared/cybercas/dialysis/franvasc.html




Peritoneal Dialysis
Uses the peritoneal lining of the abd. Cavity as semipermeable membrane
Diffusion & osmosis occur through membrane
Performed 4x/day 7 days/wk


3 Phases of Peritoneal Dialysis
Inflow Dwell Drain All 3 phases comprise one exchange

CAPD
• Used in the home• Freedom from machines• Steady bld chemistry levels• Process is shorter• Less expensive


CCPD
Also called: Automated peritoneal dialysis
Requires a cycler Free from exchanges during
day Must take cycler if traveling


Nursing Considerations
Weigh before & after VS Observe for edema, resp.
distress Check bleeding at access
site

Acc. I & O, ? Fluid restriction High calorie Low protein, Na & K diet Strict asepsis Skin care ( s/s infection)

Kidney Transplant
Kidney Donation

Live donor or cadaverTissue and blood-typed Amendment to Social
Security ActWhy is counseling advised
for both donor and recipient?

Before surgery…
BP medications Immunosuppressant drugs Possible transfusion Dialyzed before transplantation Explore patient understanding Record VS Address questions

Surgery & Complications
See fig. 40-16 pg. 924ATN, rejection, renal artery
stenosis, hematomas, abscesses and leakage of ureteral or vascular anastomoses

Organ Rejection
Hyperacute Acute Chronic s/s fever, ^ BP, pain at site of new
kidney Immunosuppressant drugs

Why are they called:
Immunosuppressants????
What is the patient predisposed to???

Routine Nursing CareMonitor urine outputMonitor fluid intakeVSNote weight changesTC & DBControl pain

Bladder CA
Most common site of urinary system CA
Men bet. 50-70 yrsMost bladder tumors are
malignant

Risk Factors
Cigarette smokingLung cancerCaffeine intakeDyes found in industrial
compounds

Medical Treatment
Cytoscopic resectionFulgurationLaser photocoagulationSegmental resectionRadical cystectomy

Types of urinary Diversion
Ileal conduit (most common)Colon conduit,
ureterosigmoidostomy Cutaneous ureterostomy Internal ileal reservoir, aka:
“Kock pouch” or “continent ileostomy”

Nursing Interventions• VS• I & O• Patency of tubes • BS, stoma appearance• Special skin care• Signs of infection
Recommended