2018.05.04.
1
Organization of Motor Functions 1. The Spinal Cord
Prof. Szabolcs Kéri
Prof. Gyula Sáry
Learning objectives 106-111.
Why is it important to study the motor system?

2018.05.04.
2
Motor symptoms: the most important first-glance diagnostic features in
STROKE
85% 15%
- 15 million people/year worldwide suffer a stroke- 6 million die, 5 million permanently disabled
Transient ischemic attack (TIA): symptoms resolved within 24 hours
Myoelectronic control for robotic hand-assisted training in stroke
Lu Z et al. Front Neurol 2017;8:107.
2018.05.04.
3
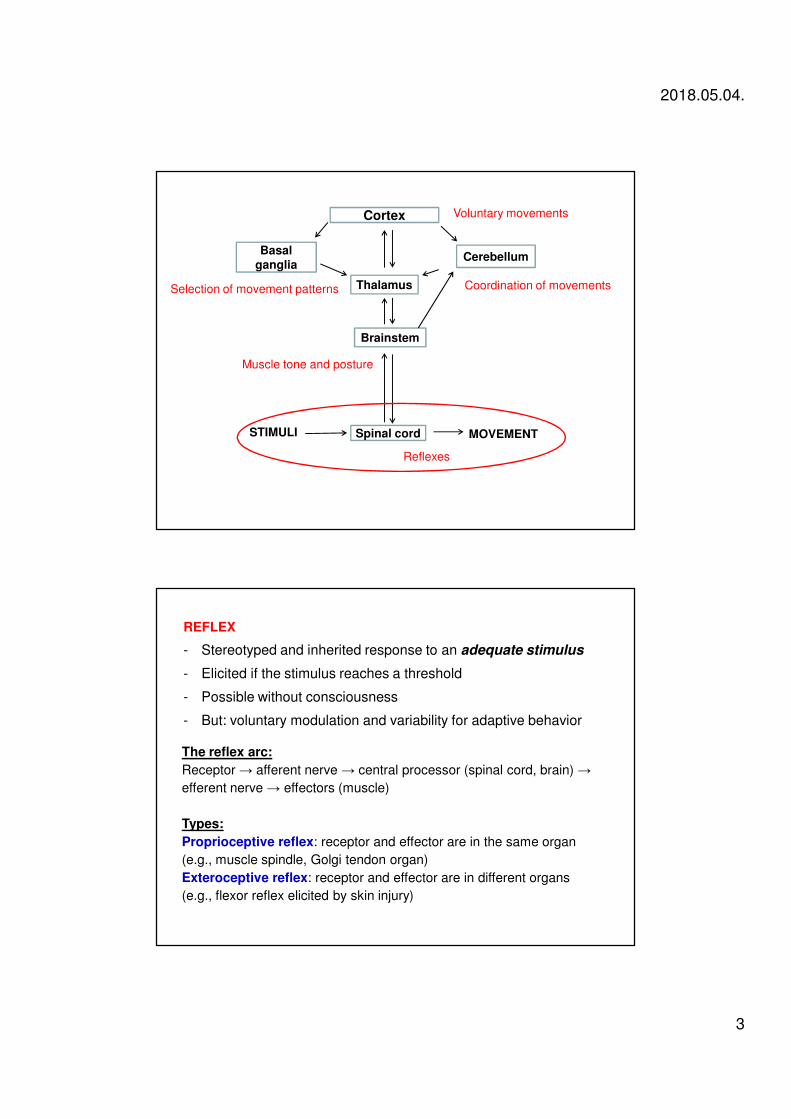
Cortex
Basalganglia
Cerebellum
Thalamus
Brainstem
Spinal cord MOVEMENTSTIMULI
Reflexes
Muscle tone and posture
Voluntary movements
Coordination of movementsSelection of movement patterns
REFLEX
- Stereotyped and inherited response to an adequate stimulus
- Elicited if the stimulus reaches a threshold
- Possible without consciousness
- But: voluntary modulation and variability for adaptive behavior
The reflex arc:
Receptor → afferent nerve → central processor (spinal cord, brain) →
efferent nerve → effectors (muscle)
Types:
Proprioceptive reflex: receptor and effector are in the same organ
(e.g., muscle spindle, Golgi tendon organ)
Exteroceptive reflex: receptor and effector are in different organs
(e.g., flexor reflex elicited by skin injury)
2018.05.04.
4
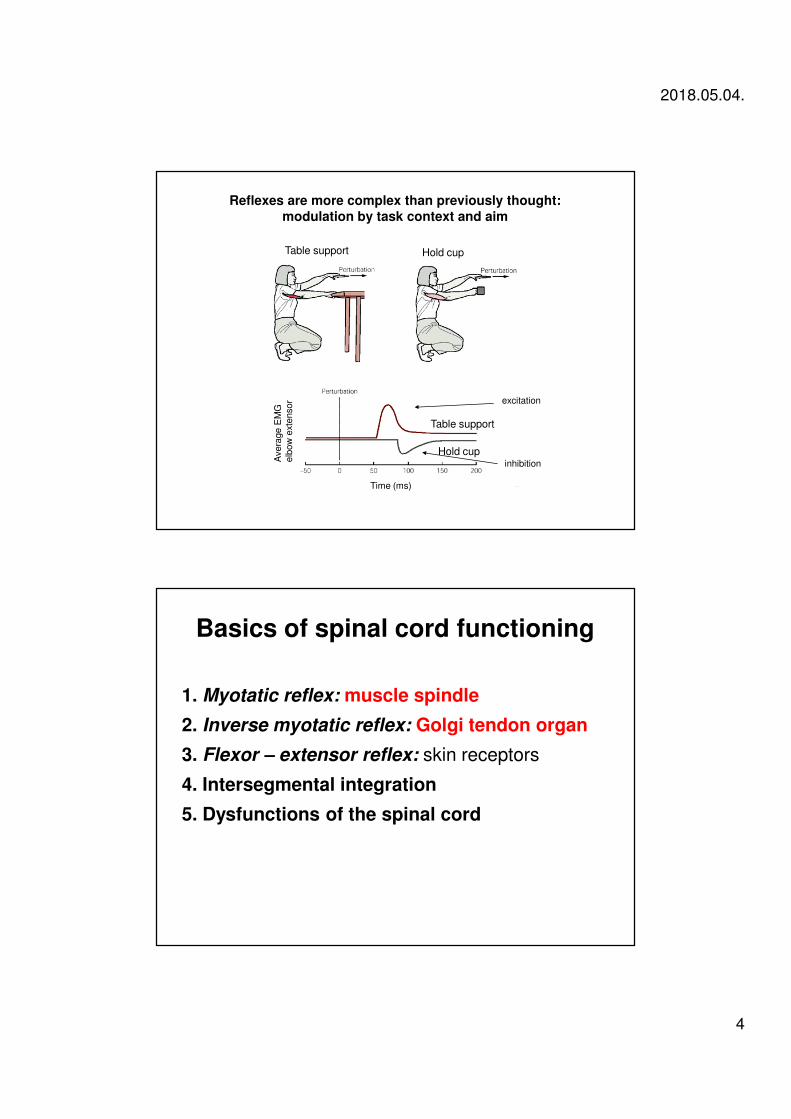
Table support Hold cup
Table support
Hold cup
Avera
ge E
MG
elb
ow
exte
nsor
Hold cup
Time (ms)
Reflexes are more complex than previously thought:modulation by task context and aim
excitation
inhibition
Basics of spinal cord functioning
1. Myotatic reflex: muscle spindle
2. Inverse myotatic reflex: Golgi tendon organ
3. Flexor – extensor reflex: skin receptors
4. Intersegmental integration
5. Dysfunctions of the spinal cord
2018.05.04.
5
I. Reflexes of the spinal cord
Essential basics
• Skeleton as a framework for movement
– flexion, extension, adduction, abduction
• Muscle function and body movement
– isotonic and isometric contraction, agonists and antagonists
• Nervous system components
– α motor neurons as the final common path
• α and γ motoneurons, extra and intrafusal fibres, motor unit
– feedback system for continuous control
2018.05.04.
6
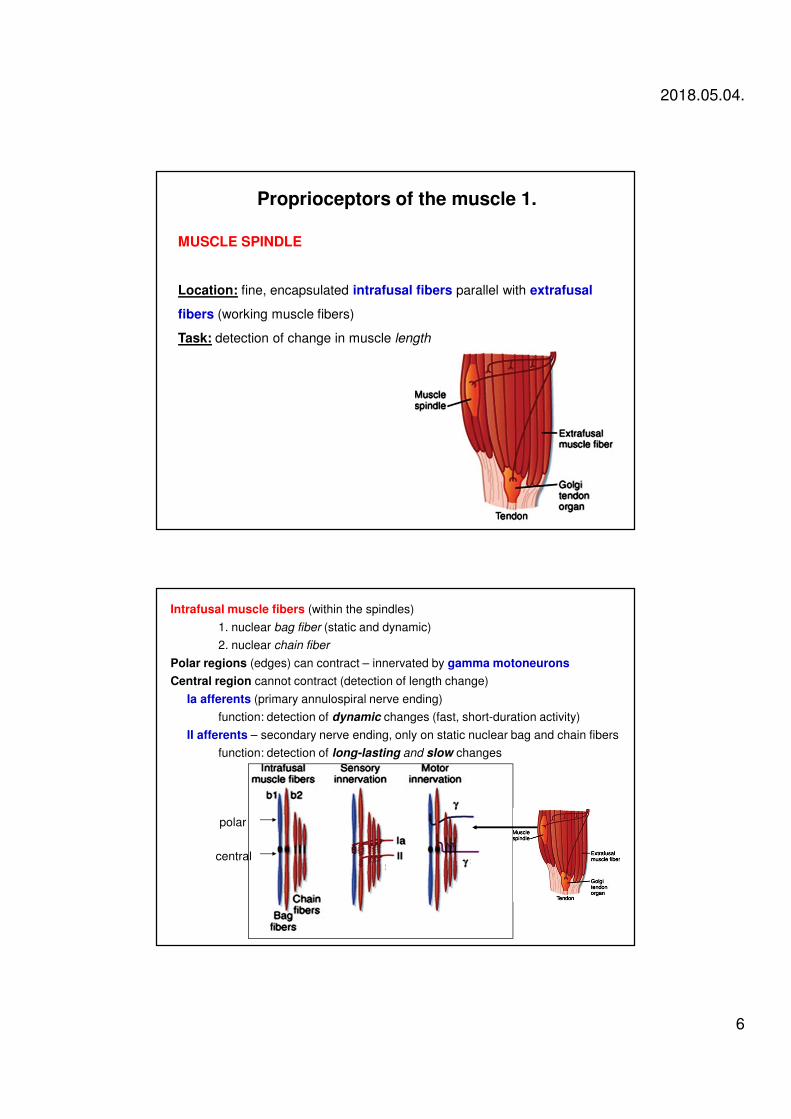
Proprioceptors of the muscle 1.
MUSCLE SPINDLE
Location: fine, encapsulated intrafusal fibers parallel with extrafusal
fibers (working muscle fibers)
Task: detection of change in muscle length
Intrafusal muscle fibers (within the spindles)
1. nuclear bag fiber (static and dynamic)
2. nuclear chain fiber
Polar regions (edges) can contract – innervated by gamma motoneurons
Central region cannot contract (detection of length change)
Ia afferents (primary annulospiral nerve ending)
function: detection of dynamic changes (fast, short-duration activity)
II afferents – secondary nerve ending, only on static nuclear bag and chain fibers
function: detection of long-lasting and slow changes
central
polar
2018.05.04.
7
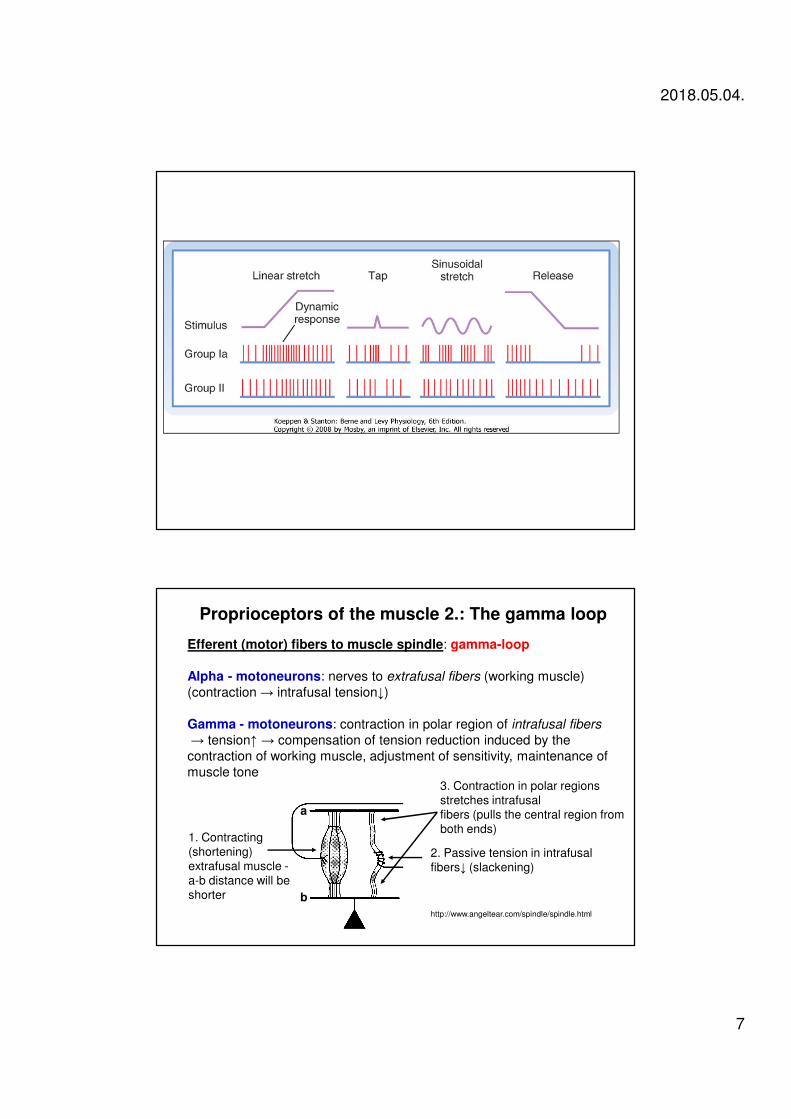
Efferent (motor) fibers to muscle spindle: gamma-loop
Alpha - motoneurons: nerves to extrafusal fibers (working muscle)
(contraction → intrafusal tension↓)
Gamma - motoneurons: contraction in polar region of intrafusal fibers
→ tension↑ → compensation of tension reduction induced by the
contraction of working muscle, adjustment of sensitivity, maintenance of
muscle tone
1. Contracting
(shortening)
extrafusal muscle -
a-b distance will be
shorter
2. Passive tension in intrafusal
fibers↓ (slackening)
3. Contraction in polar regions
stretches intrafusal
fibers (pulls the central region from
both ends)
Proprioceptors of the muscle 2.: The gamma loop
http://www.angeltear.com/spindle/spindle.html
a
b
2018.05.04.
8
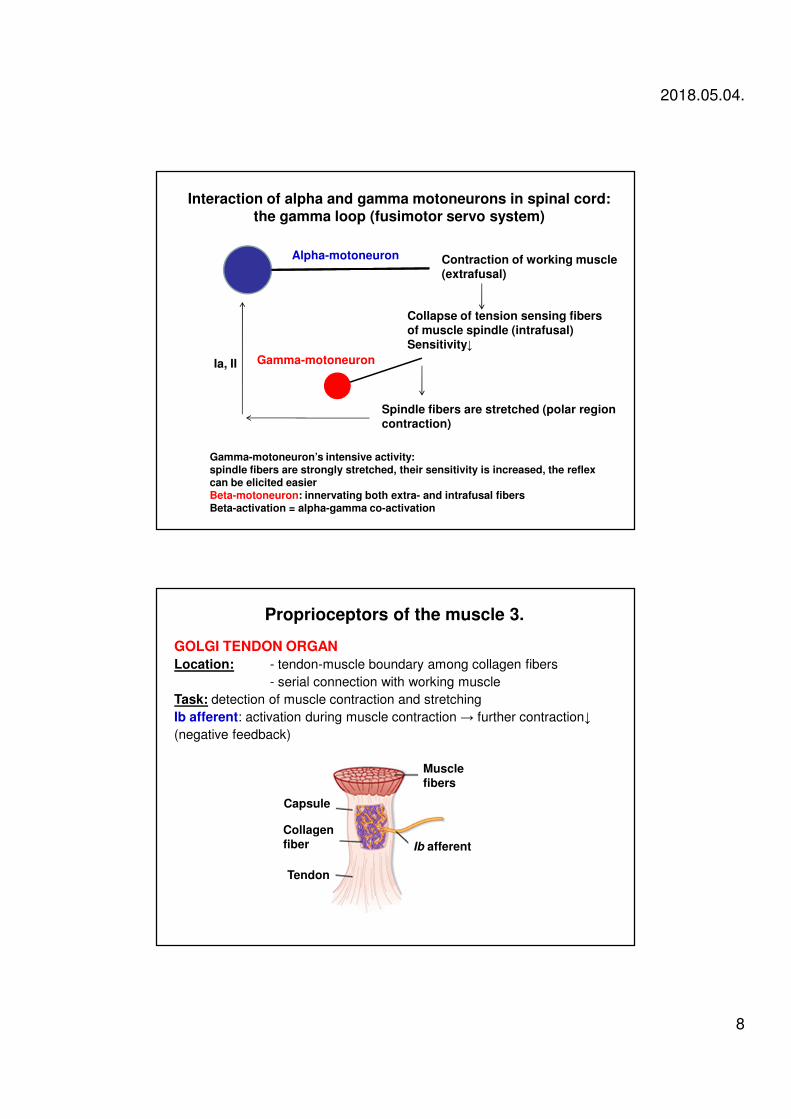
Alpha-motoneuron Contraction of working muscle(extrafusal)
Collapse of tension sensing fibersof muscle spindle (intrafusal)Sensitivity↓
Gamma-motoneuron
Spindle fibers are stretched (polar regioncontraction)
Gamma-motoneuron’s intensive activity:spindle fibers are strongly stretched, their sensitivity is increased, the reflexcan be elicited easierBeta-motoneuron: innervating both extra- and intrafusal fibersBeta-activation = alpha-gamma co-activation
Ia, II
Interaction of alpha and gamma motoneurons in spinal cord:the gamma loop (fusimotor servo system)
GOLGI TENDON ORGAN
Location: - tendon-muscle boundary among collagen fibers
- serial connection with working muscle
Task: detection of muscle contraction and stretching
Ib afferent: activation during muscle contraction → further contraction↓
(negative feedback)
Proprioceptors of the muscle 3.
Musclefibers
Ib afferent
Capsule
Collagenfiber
Tendon
2018.05.04.
9
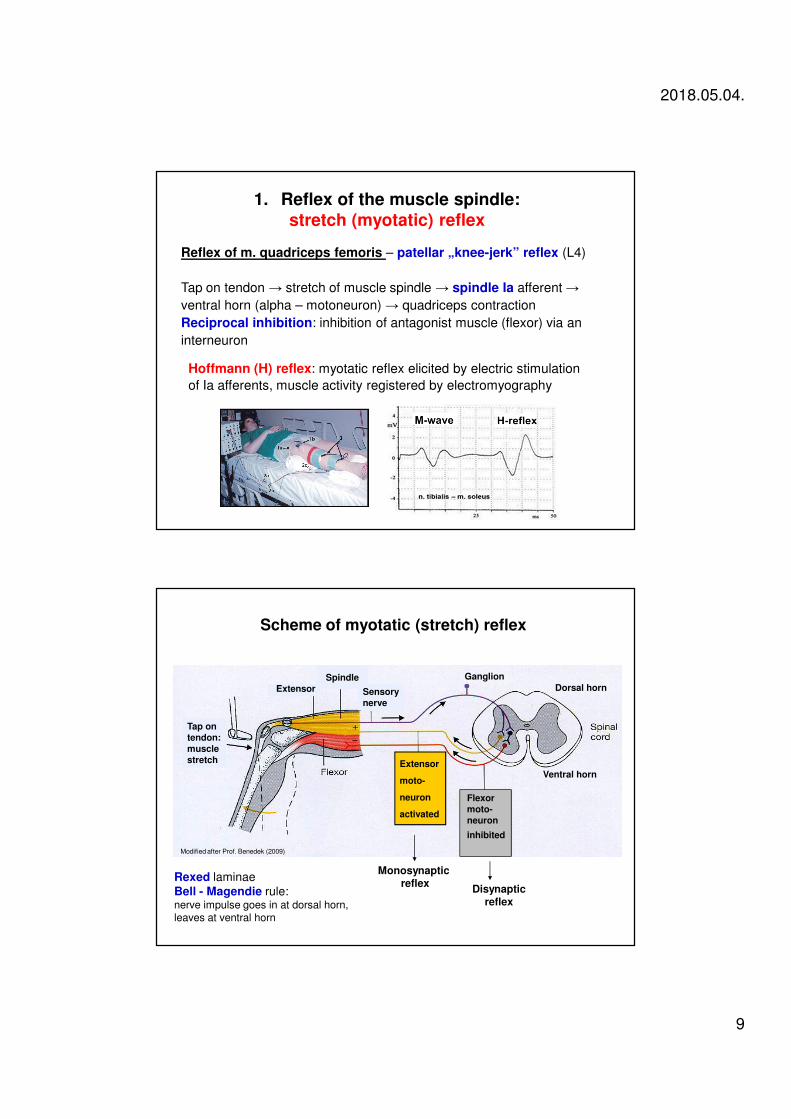
1. Reflex of the muscle spindle:stretch (myotatic) reflex
Reflex of m. quadriceps femoris – patellar „knee-jerk” reflex (L4)
Tap on tendon → stretch of muscle spindle → spindle Ia afferent →
ventral horn (alpha – motoneuron) → quadriceps contraction
Reciprocal inhibition: inhibition of antagonist muscle (flexor) via an
interneuron
Hoffmann (H) reflex: myotatic reflex elicited by electric stimulation
of Ia afferents, muscle activity registered by electromyography
Tap on tendon:musclestretch
ExtensorSpindle
Scheme of myotatic (stretch) reflex
Sensorynerve
Extensor
moto-
neuron
activated
Flexor moto-neuron
inhibited
Monosynaptic reflex
Disynapticreflex
Ganglion
Dorsal horn
Ventral horn
Rexed laminae
Bell - Magendie rule:nerve impulse goes in at dorsal horn, leaves at ventral horn
Modified after Prof. Benedek (2009)
2018.05.04.
10
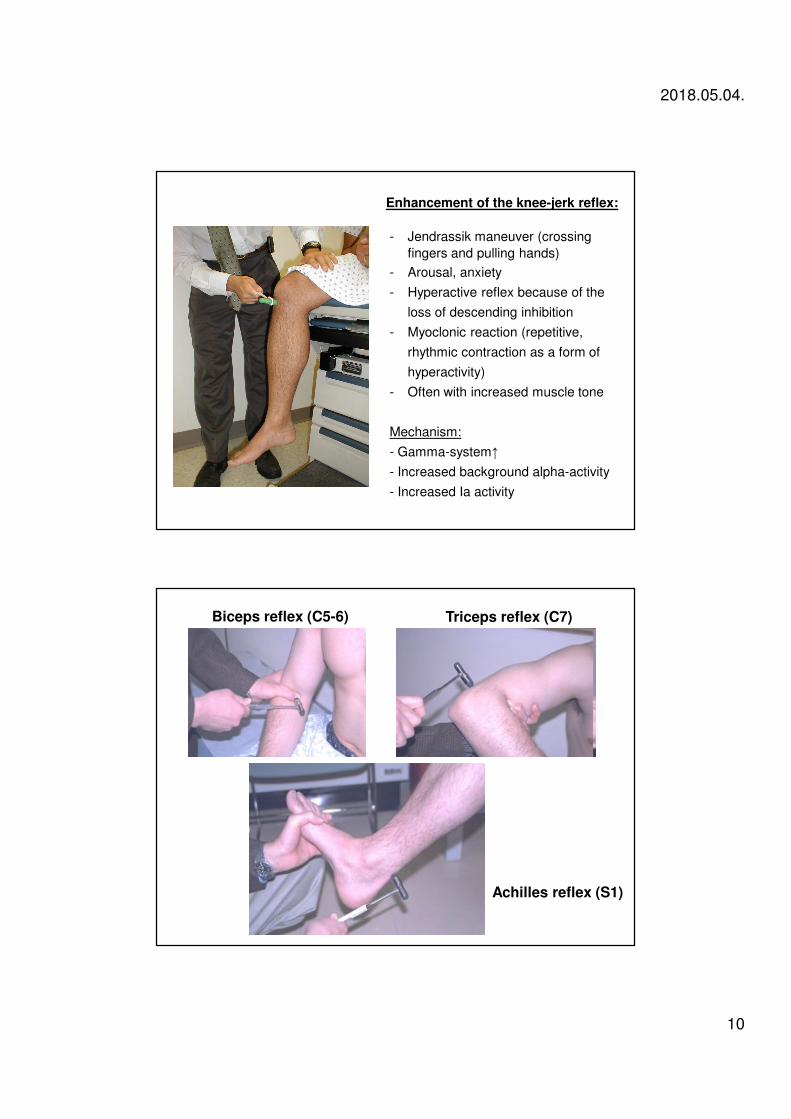
Enhancement of the knee-jerk reflex:
- Jendrassik maneuver (crossing
fingers and pulling hands)
- Arousal, anxiety
- Hyperactive reflex because of the
loss of descending inhibition
- Myoclonic reaction (repetitive,
rhythmic contraction as a form of
hyperactivity)
- Often with increased muscle tone
Mechanism:
- Gamma-system↑
- Increased background alpha-activity
- Increased Ia activity
Achilles reflex (S1)
Biceps reflex (C5-6) Triceps reflex (C7)
2018.05.04.
11
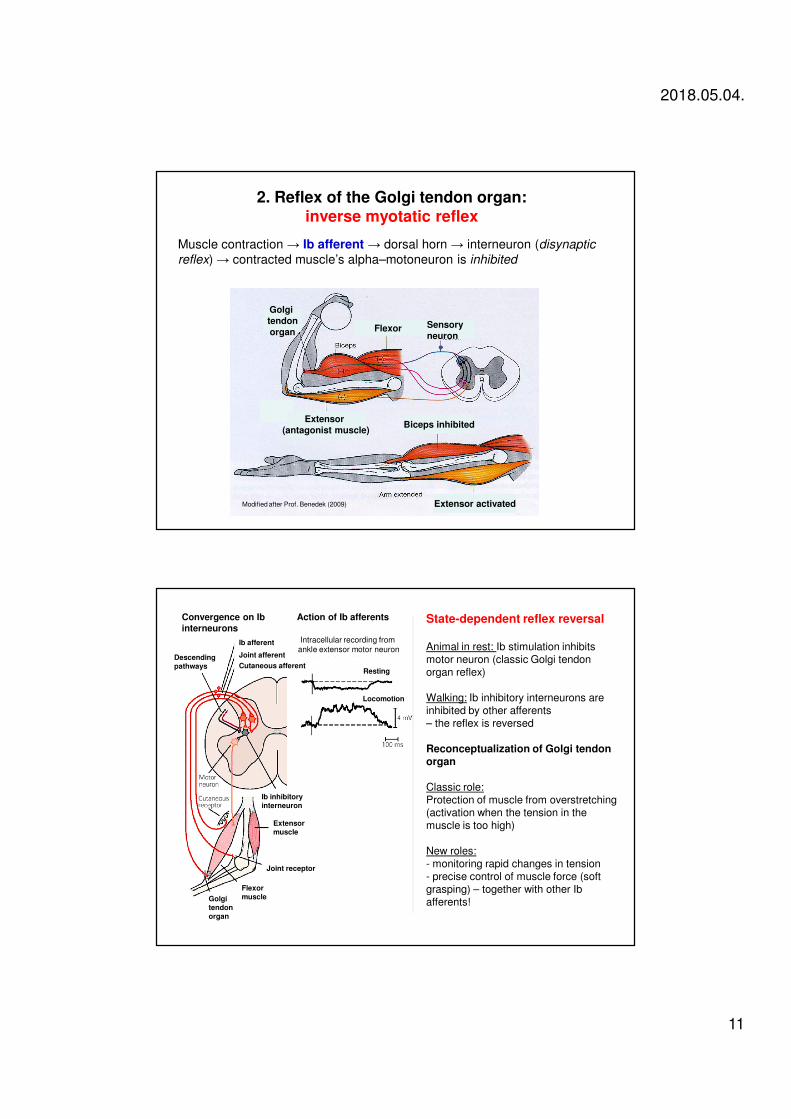
2. Reflex of the Golgi tendon organ: inverse myotatic reflex
Muscle contraction → Ib afferent → dorsal horn → interneuron (disynaptic
reflex) → contracted muscle’s alpha–motoneuron is inhibited
Sensory neuron
Extensor (antagonist muscle)
Flexor
Golgi tendonorgan
Biceps inhibited
Extensor activatedModified after Prof. Benedek (2009)
Convergence on Ib interneurons
Action of Ib afferents
Intracellular recording from
ankle extensor motor neuronIb afferent
Joint afferent
Cutaneous afferentDescendingpathways
Ib inhibitoryinterneuron
Resting
Locomotion
Joint receptor
Flexor muscleGolgi
tendonorgan
Extensor muscle
State-dependent reflex reversal
Animal in rest: Ib stimulation inhibitsmotor neuron (classic Golgi tendonorgan reflex)
Walking: Ib inhibitory interneurons areinhibited by other afferents – the reflex is reversed
Reconceptualization of Golgi tendonorgan
Classic role:Protection of muscle from overstretching(activation when the tension in themuscle is too high)
New roles:- monitoring rapid changes in tension- precise control of muscle force (softgrasping) – together with other Ib afferents!
2018.05.04.
12
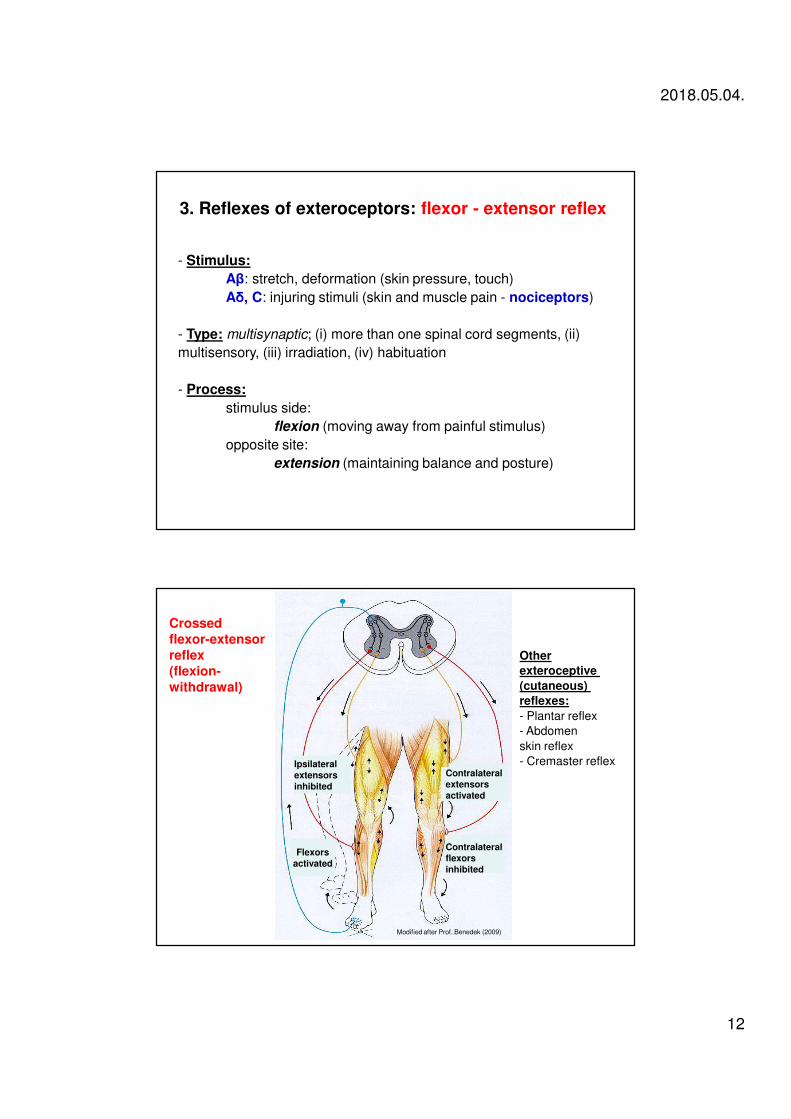
3. Reflexes of exteroceptors: flexor - extensor reflex
- Stimulus:
Aβ: stretch, deformation (skin pressure, touch)
Aδ, C: injuring stimuli (skin and muscle pain - nociceptors)
- Type: multisynaptic; (i) more than one spinal cord segments, (ii)
multisensory, (iii) irradiation, (iv) habituation
- Process:
stimulus side:
flexion (moving away from painful stimulus)
opposite site:
extension (maintaining balance and posture)
Crossed flexor-extensor reflex(flexion-withdrawal)
Other
exteroceptive
(cutaneous)
reflexes:
- Plantar reflex
- Abdomen
skin reflex
- Cremaster reflexIpsilateralextensorsinhibited
Flexorsactivated
Contralateralflexorsinhibited
Contralateralextensorsactivated
Modified after Prof. Benedek (2009)
2018.05.04.
13
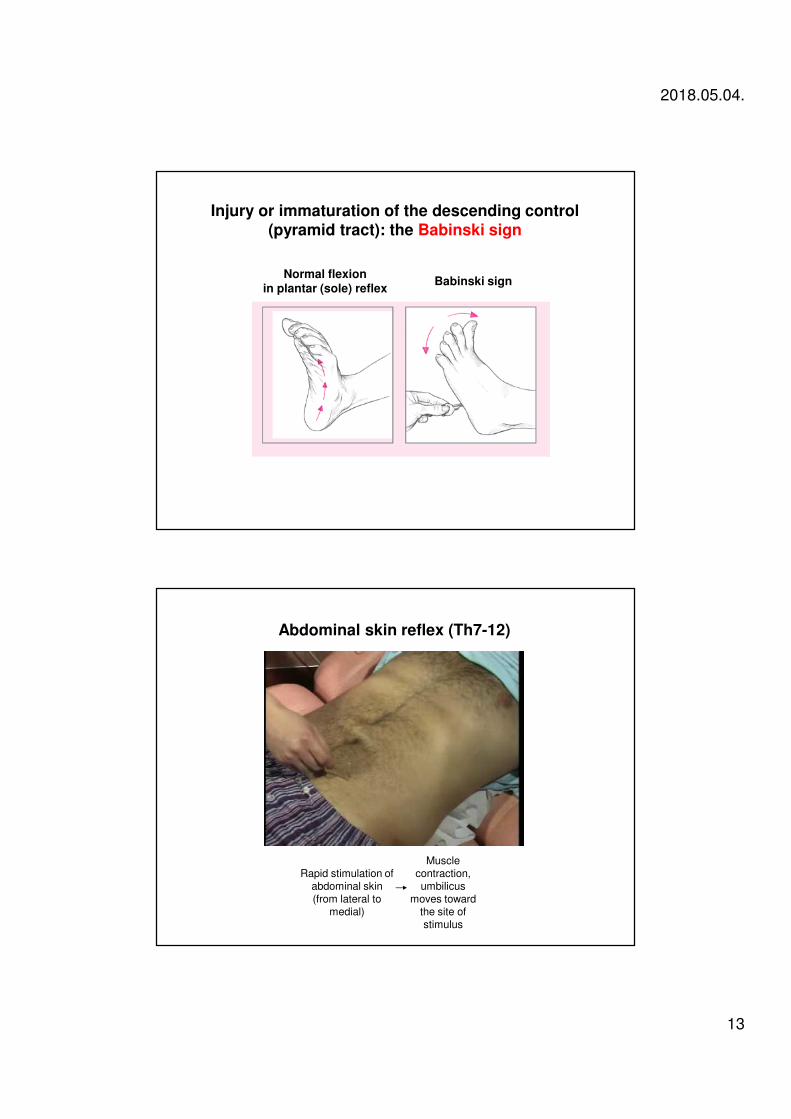
Normal flexion in plantar (sole) reflex
Babinski sign
Injury or immaturation of the descending control(pyramid tract): the Babinski sign
Rapid stimulation of abdominal skin (from lateral to
medial)
Muscle contraction,umbilicus
moves toward the site of stimulus
Abdominal skin reflex (Th7-12)
2018.05.04.
14
II. Intersegmental integration in the spinal cord
Multisegmental and integrative functions of the spinal cord
Interneurons and motoneurons - complex interactions
Functions of the interneurons:
1. Receiving afferent pathway information (e.g., reflex arc, Ia inhibitory
interneurons)
2. Receiving descending controls pathways (e.g., pyramid tract)
3. Intrinsic cyclic activity
- Central Pattern Generation population of cells
- LDP [locomotor drive potential] - activation and
coordination of flexor/extensor muscles and limbs (e.g.,
walking)
4. Renshaw-cell: inhibitory interneuron of motoneurons (transmitter:
GABA or glycine)
2018.05.04.
15
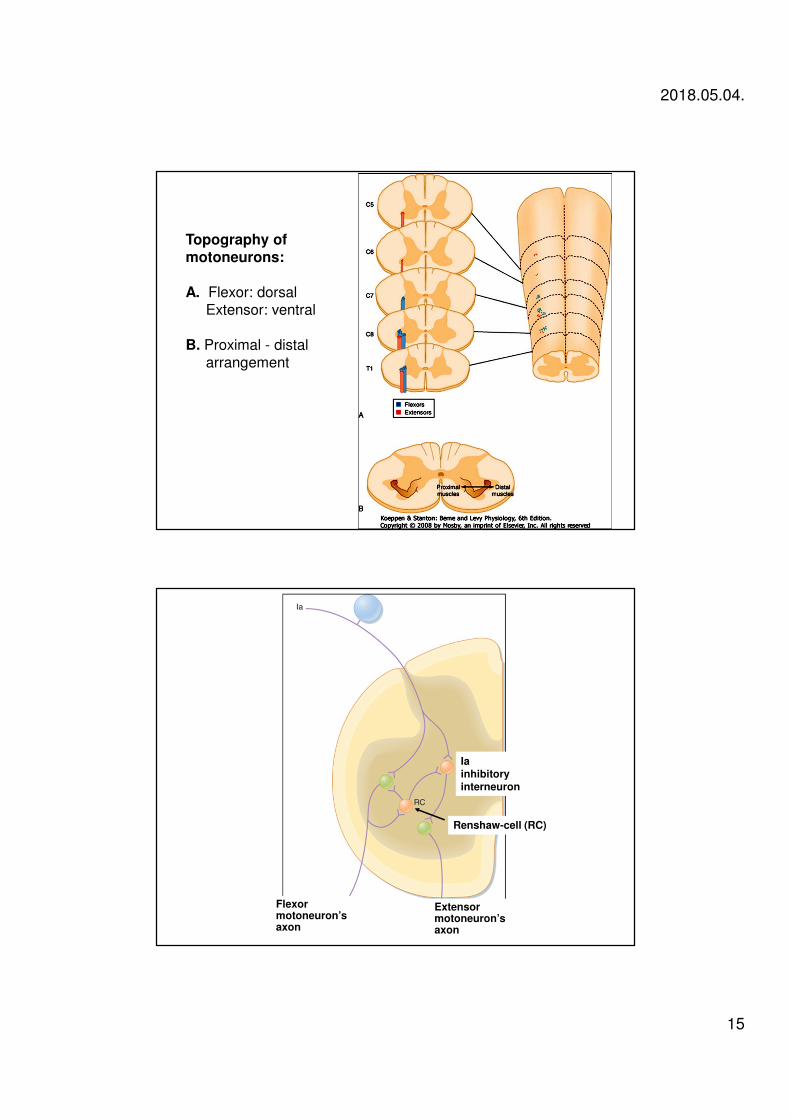
Topography of motoneurons:
A. Flexor: dorsalExtensor: ventral
B. Proximal - distalarrangement
Flexormotoneuron’saxon
Extensormotoneuron’saxon
Iainhibitoryinterneuron
Renshaw-cell (RC)
2018.05.04.
16
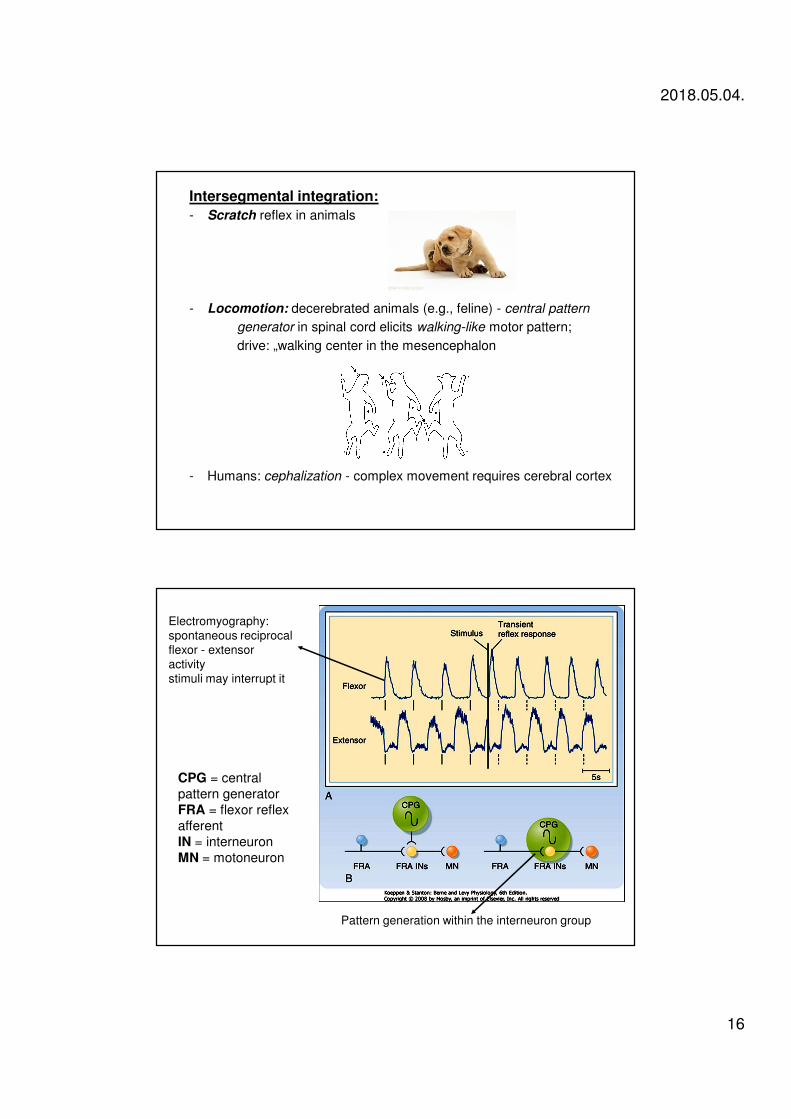
Intersegmental integration:
- Scratch reflex in animals
- Locomotion: decerebrated animals (e.g., feline) - central pattern
generator in spinal cord elicits walking-like motor pattern;
drive: „walking center in the mesencephalon
- Humans: cephalization - complex movement requires cerebral cortex
CPG = central
pattern generator
FRA = flexor reflex
afferent
IN = interneuron
MN = motoneuron
Electromyography:
spontaneous reciprocal
flexor - extensor
activity
stimuli may interrupt it
Pattern generation within the interneuron group
2018.05.04.
17
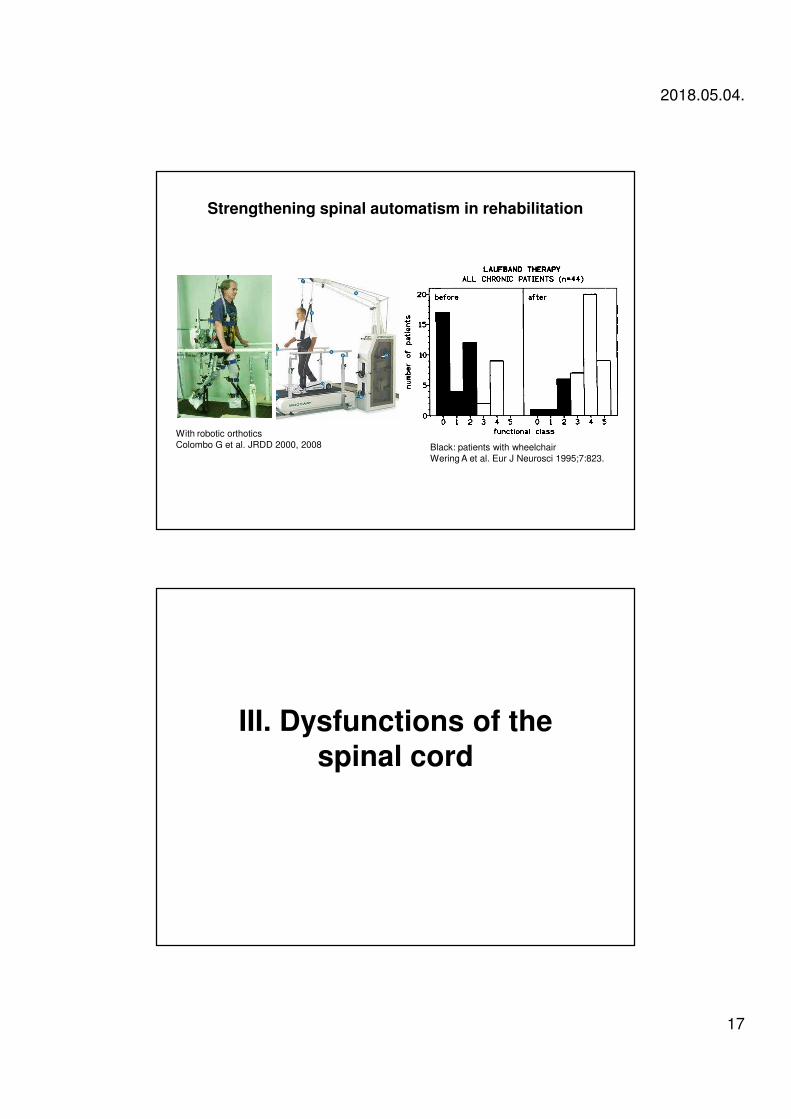
Strengthening spinal automatism in rehabilitation
Black: patients with wheelchair
Wering A et al. Eur J Neurosci 1995;7:823.
With robotic orthotics
Colombo G et al. JRDD 2000, 2008
III. Dysfunctions of the spinal cord
2018.05.04.
18
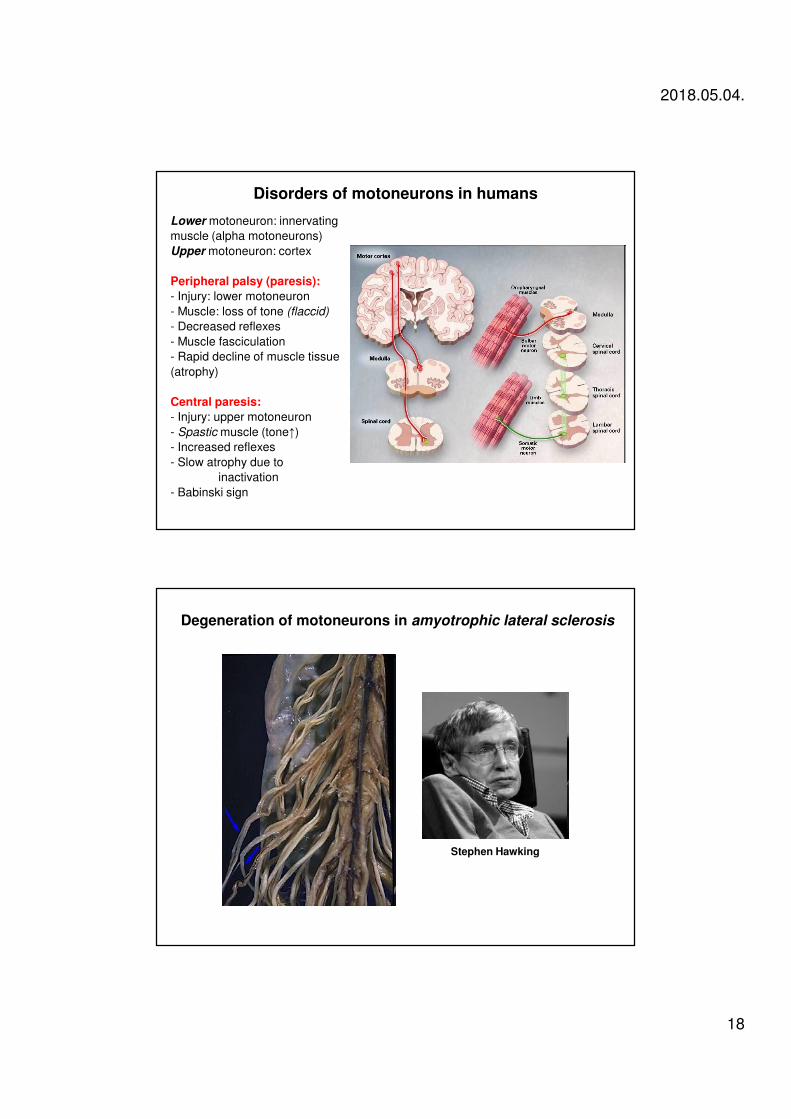
Disorders of motoneurons in humans
Lower motoneuron: innervating
muscle (alpha motoneurons)
Upper motoneuron: cortex
Peripheral palsy (paresis):
- Injury: lower motoneuron
- Muscle: loss of tone (flaccid)
- Decreased reflexes
- Muscle fasciculation
- Rapid decline of muscle tissue
(atrophy)
Central paresis:
- Injury: upper motoneuron
- Spastic muscle (tone↑)
- Increased reflexes
- Slow atrophy due to
inactivation
- Babinski sign
Stephen Hawking
Degeneration of motoneurons in amyotrophic lateral sclerosis
2018.05.04.
19
Consequences of spinal cord injury in humans 1.
Partial or total injury induced by: trauma, tumor, infection, hypoxia,
discus hernia
Severe injury: spinal shock with motor, sensory, and vegetative
symptoms
Phases:
1. Loss of all reflexes below the level of transsection (~ 24 hours) –
(disconnection of descending facilitation)
2. Polysynaptic reflexes regenerate (~ 72 hours)
3. Tendon reflexes return + hyperreflexia (~ 1 week - 1 year) –
- growth of moto- and interneuron’s projections
- genesis of new synapses
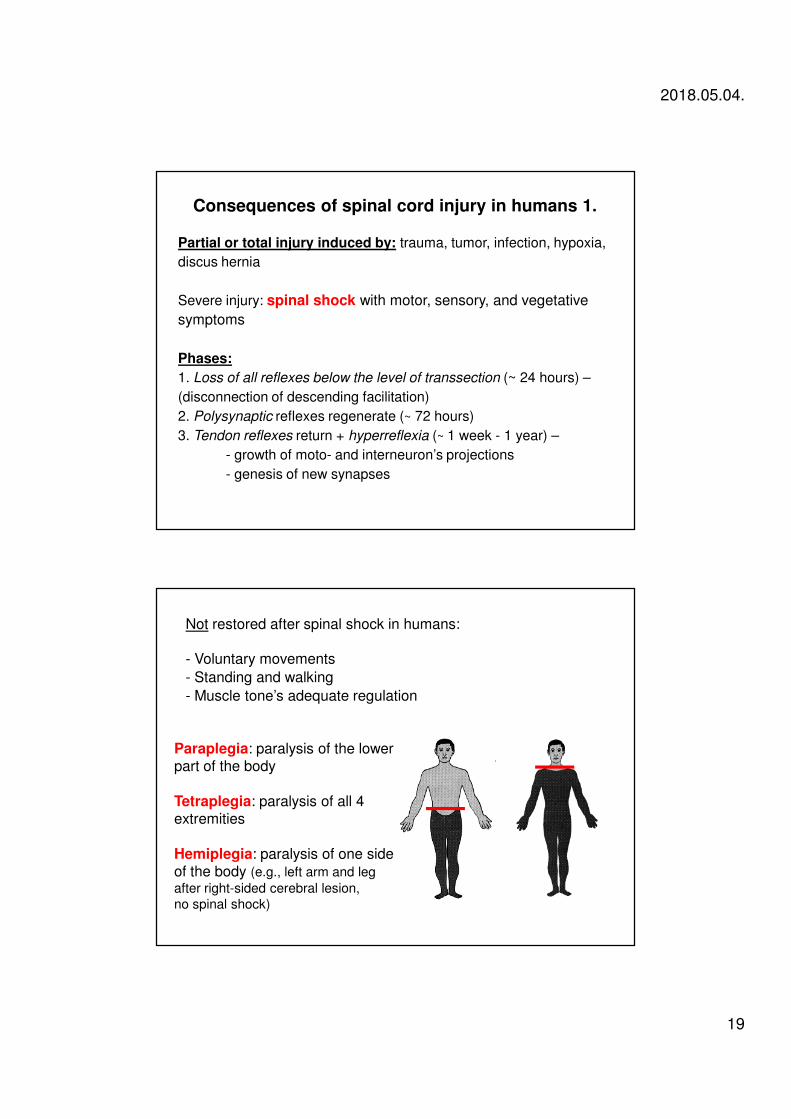
Not restored after spinal shock in humans:
- Voluntary movements
- Standing and walking
- Muscle tone’s adequate regulation
Paraplegia: paralysis of the lowerpart of the body
Tetraplegia: paralysis of all 4extremities
Hemiplegia: paralysis of one sideof the body (e.g., left arm and leg
after right-sided cerebral lesion,
no spinal shock)
2018.05.04.
20
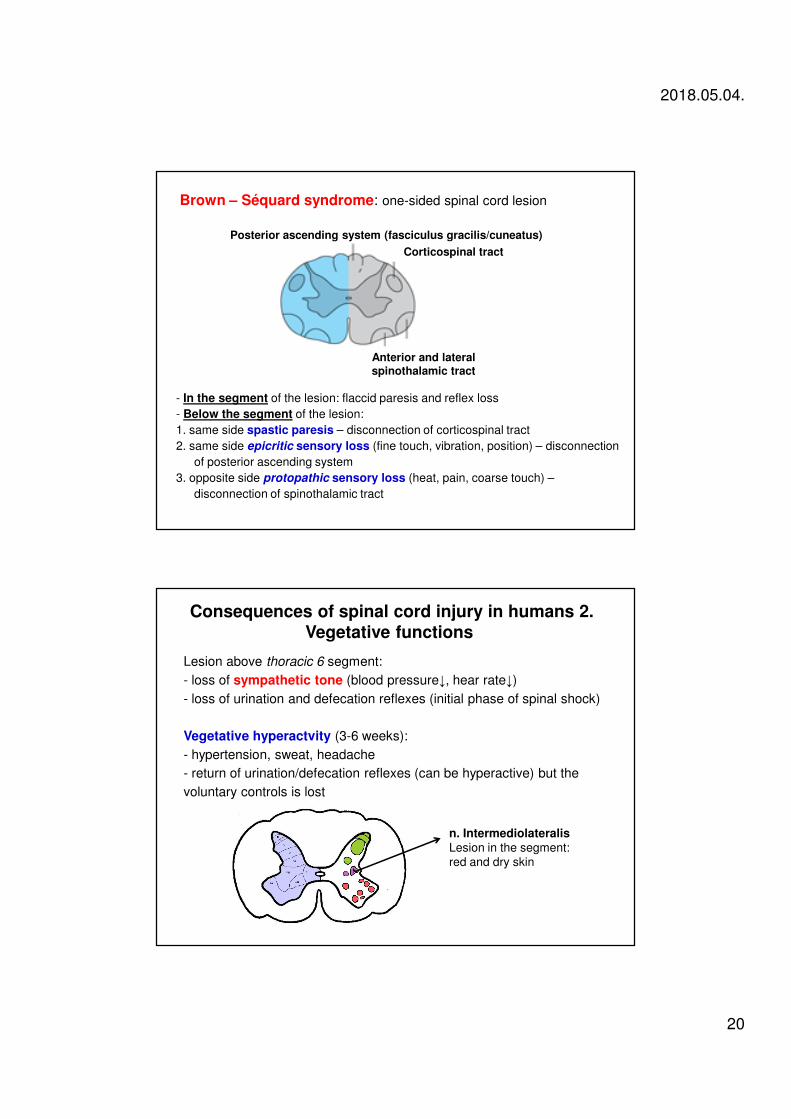
Brown – Séquard syndrome: one-sided spinal cord lesion
Posterior ascending system (fasciculus gracilis/cuneatus)
Corticospinal tract
Anterior and lateral spinothalamic tract
- In the segment of the lesion: flaccid paresis and reflex loss
- Below the segment of the lesion:
1. same side spastic paresis – disconnection of corticospinal tract
2. same side epicritic sensory loss (fine touch, vibration, position) – disconnection
of posterior ascending system
3. opposite side protopathic sensory loss (heat, pain, coarse touch) –
disconnection of spinothalamic tract
Lesion above thoracic 6 segment:
- loss of sympathetic tone (blood pressure↓, hear rate↓)
- loss of urination and defecation reflexes (initial phase of spinal shock)
Vegetative hyperactvity (3-6 weeks):
- hypertension, sweat, headache
- return of urination/defecation reflexes (can be hyperactive) but the
voluntary controls is lost
n. IntermediolateralisLesion in the segment:
red and dry skin
Consequences of spinal cord injury in humans 2.Vegetative functions
2018.05.04.
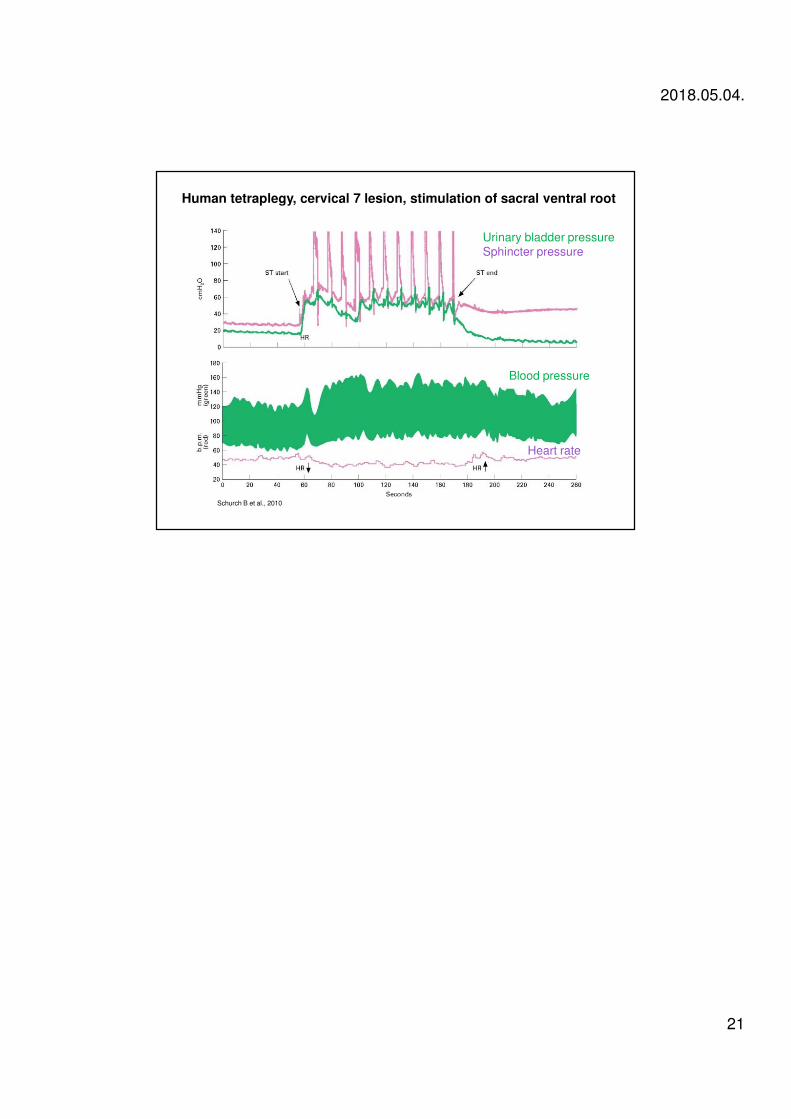
21
Human tetraplegy, cervical 7 lesion, stimulation of sacral ventral root
Urinary bladder pressure
Sphincter pressure
Blood pressure
Heart rate
Schurch B et al., 2010
Recommended