Embed Size (px)
Citation preview
Definition
Epidemiology
Types of diarrhea
Causes
Acute Diarrhea
According to WHO
- passage of 3 or more loose or liquid stools per day, or more frequently than is normal for the individual.
• Diarrheal diseases continue to be a major cause of morbidity and mortality in children in developing nations.
• In the year 2000, diarrheal diseases claimed an estimated 1.4 to 2.5 million lives; they are among the leading causes of death in children in developing countries
• In developed nations , they are an important cause of hospital admission although mortality rates may be lower.
• About 9% of all hospitalizations of children younger than 5 years were reported to be a result of diarrhea.
• A greater number of stools of decreased form from the normal lasting for less than 14 days
• 2 types:- Acute watery diarrhoea and dysenteryAcute diarrhoea
• Illness persists for more than 14 days. Persistent diarrhoea
• Duration of symptoms is longer than 1 monthChronic diarrhoea
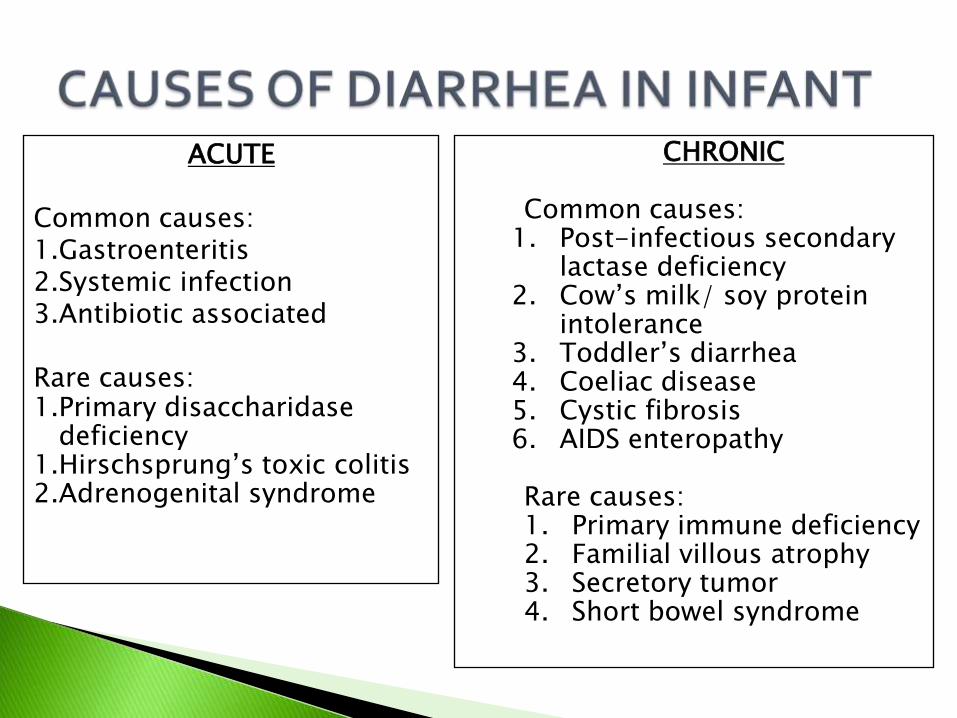
ACUTE
Common causes:1.Gastroenteritis2.Systemic infection3.Antibiotic associated
Rare causes:1.Primary disaccharidase
deficiency1.Hirschsprung’s toxic colitis2.Adrenogenital syndrome
CHRONIC
Common causes:1. Post-infectious secondary
lactase deficiency2. Cow’s milk/ soy protein
intolerance3. Toddler’s diarrhea4. Coeliac disease5. Cystic fibrosis6. AIDS enteropathy
Rare causes:1. Primary immune deficiency2. Familial villous atrophy3. Secretory tumor4. Short bowel syndrome
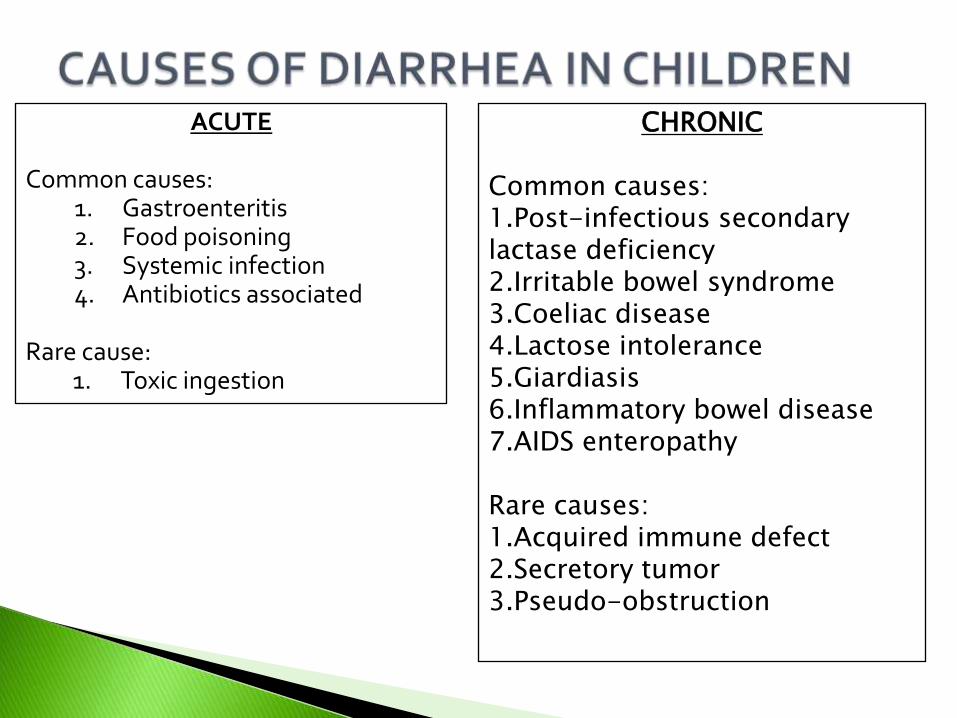
ACUTE
Common causes:1. Gastroenteritis2. Food poisoning3. Systemic infection4. Antibiotics associated
Rare cause:1. Toxic ingestion
CHRONIC
Common causes:1.Post-infectious secondary lactase deficiency2.Irritable bowel syndrome3.Coeliac disease4.Lactose intolerance5.Giardiasis6.Inflammatory bowel disease7.AIDS enteropathy
Rare causes:1.Acquired immune defect2.Secretory tumor3.Pseudo-obstruction

ACUTE DIARRHEA
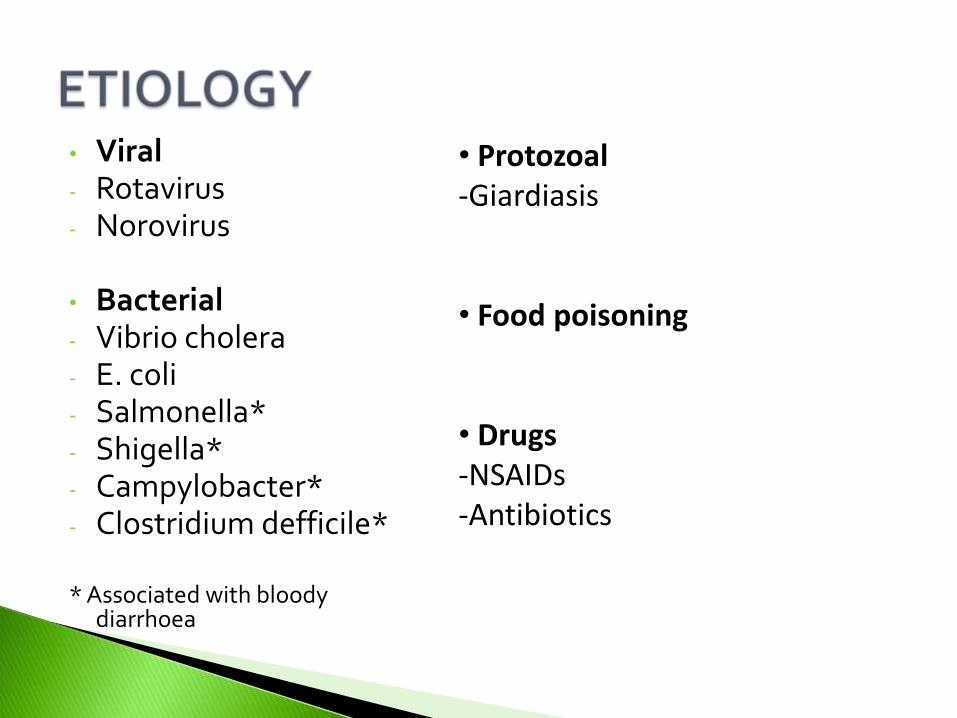
• Viral- Rotavirus- Norovirus
• Bacterial- Vibrio cholera- E. coli- Salmonella*- Shigella*- Campylobacter*- Clostridium defficile*
* Associated with bloody diarrhoea
• Protozoal-Giardiasis
• Food poisoning
• Drugs-NSAIDs-Antibiotics
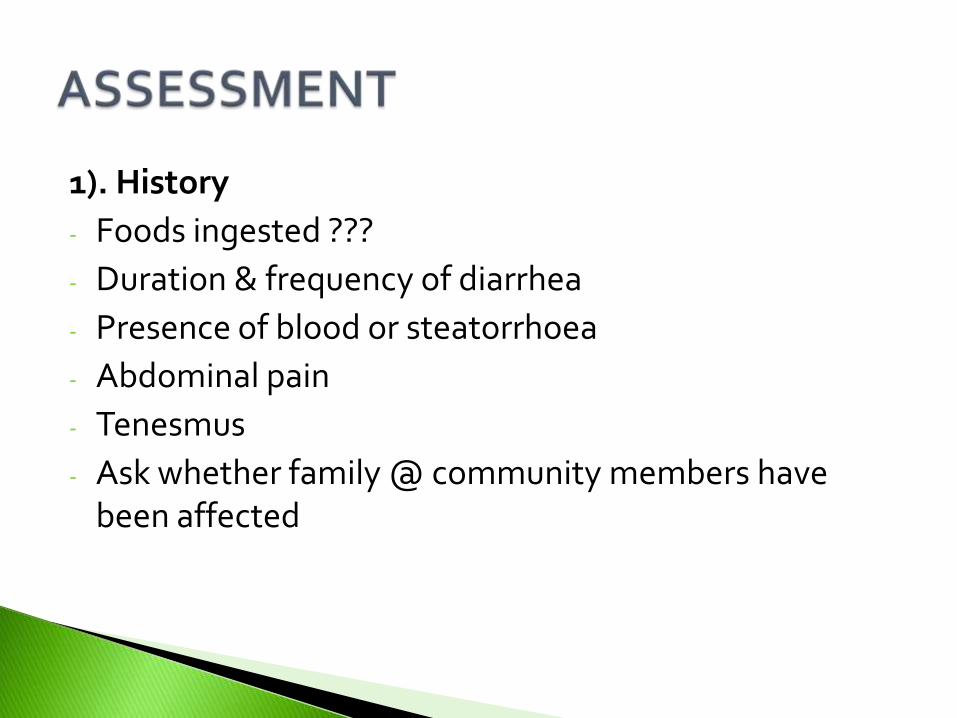
1). History
- Foods ingested ???
- Duration & frequency of diarrhea
- Presence of blood or steatorrhoea
- Abdominal pain
- Tenesmus
- Ask whether family @ community members have been affected
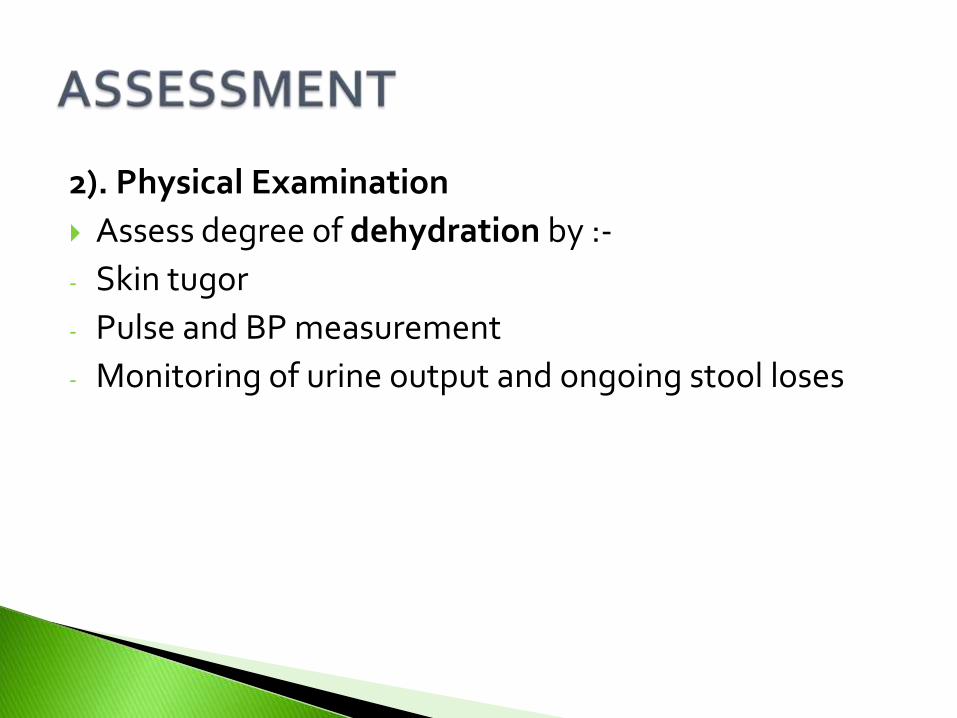
2). Physical Examination
Assess degree of dehydration by :-
- Skin tugor
- Pulse and BP measurement
- Monitoring of urine output and ongoing stool loses
3). Investigation
- FBC
- Serum electrolyte
- Blood and urine culture
- Stool inspection for blood and examination for ova, cysts and parasites
- Chest X-ray
Asses based on :-1.General condition2. Sunken eyes3. Offer the child drink4. Skin turgor
Classification: -1. Mild dehydration (<5%)2. Moderate dehydration (5-10%)3. Severe dehydration (>10%)
• First, assess the state of dehydration & then choose the treatment plan A, B or C
PLAN A (mild diarrhea)
1. Give extra fluid
- Breastfeed frequently
- Give ORS and cooled boiled water
- Plus food-based fluid (not exclusively breastfed)
*10ml/kg of ORS after each loose stool
2. Continue Feeding
- Feed as usual on demand
- Avoid food high in simple sugar as osmotic load may worsen the diarrhea
3. When to Return (to clinic/hospital)
- Not able to drink
- Becomes sicker
- Develops fever
- Has blood in stool
PLAN B (moderate diarrhea)
Give recommended amount of ORS 4- hourly* Approximat amount of ORSs required = weight (in kg) x 75
After 4 hours
- Reassess the child
- Select appropriate treatment
- Begin feeding the child
Explain the 3 rules of PLAN A
PLAN C (severe diarrhea)
• Start IV or IO fluid immediately. Give 100ml/kg Ringers Lactate @ normal saline devided as :-
- 1st give 20ml/kg as fast as possible. Repeat boluses until perfusion has improved
- Give the remaining fluid 5 hrs (age < 1 year)
or 2 ½ hrs (age >1 year)
• Reassess the child after every bolus
• Reassess the child every 1-2 hour during rehydration
• Give ORS as soon as the child can drink.
• Classify the degree of dehyration
• Choose appropriate treatment
Maintenance Fluid Therapy
Volume of fluid required
< 6 months age : 150 ml/kg/day
6 to 1 year : 120 ml/kg/day
>1 year : 1st 10 kg = 100 ml/kg
10- 20 kg = + 50 ml/kg for the subsequent kg
> 20 kg = + 20 ml/kg for the subsequent kg
Antimicrobial Treatment
• Indicators:-
- Toxic looking
- Severe dehydration
- Blood in stool
• Types of Antibiotics:-
- Ampicilin
- Trimethoprim (TMP)
- Sulfamethoxazole

Chief Complaint:
“Sally has a fever and is vomiting.”
History of Present Illness
A 4-year-old female is brought to the emergency dept. by her parents.
She started complaining of abdominal pain 3 hrs ago and then had an onset of vomiting episodes x 4.
No blood noted in the emesis or bile appearance.
Temperature taken at home one half hour ago, temperature was 38.2 C.
Mother has also commented on Sally’s increased level of thirst over the
past week, and has attributed Sally’s new onset of night time bedwetting to her increased consumption of fluids.
Vomiting is a coordinated, sequential series of events that leads to forceful oral emptying of gastric contents.
–Duration, frequency, bilious material, abdominal pain, diarrhea, hematemesis, hematochezia, melena, headache, fever, dysuria, weight loss, urine output
–Sick contacts, cough, rhinorrhea, neck stiffness
Family history: Genetic disease
–Vital signs, weight, mucous membranes, nasal discharge, breath sounds, rashes
–Abdominal pain/distension, hepatosplenomegaly, abdominal masses, Murphy/obturator/psoas sign
–Skin turgor, capillary refill
–Neuro exam including funduscopy for papilledema
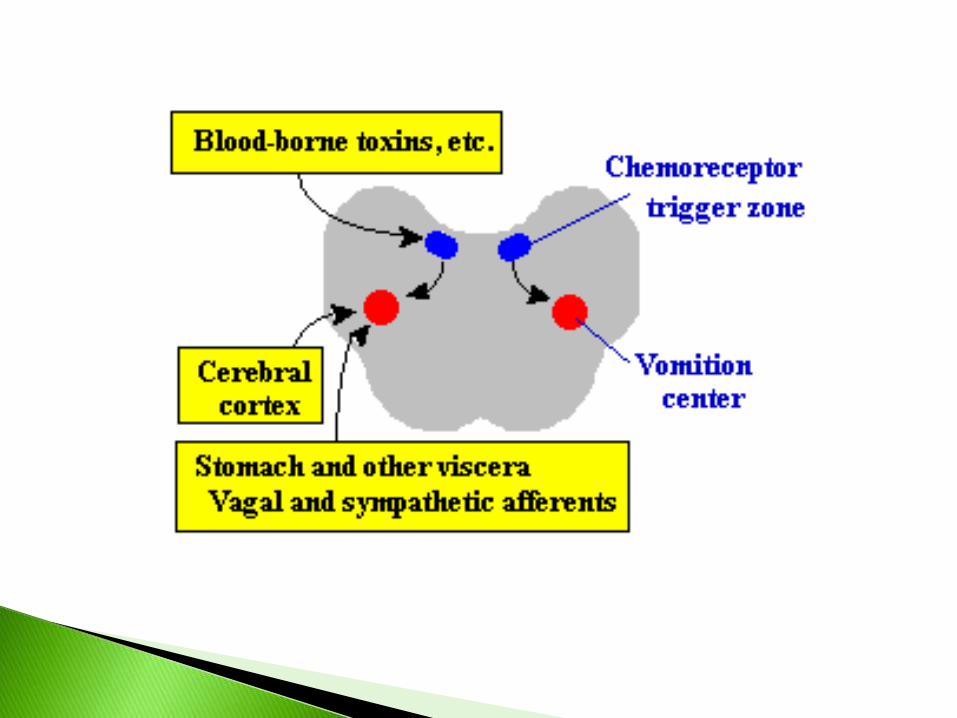
Bilateral vomition centers in the reticular formation of the medulla integrate signals triggers vomition.The vomition centers receive afferent signals from four major sources:
The chemoreceptor trigger zone -bilateral set of centers in the brainstem lying under the floor of the fourth ventricle. The chemoreceptor trigger zones function as emetic chemoreceptors for the vomition centers - chemical abnormalities in the body (e.g. emetic drugs, uremia, hypoxia and diabetic ketoacidosis) are sensed by these centers, which then send excitatory signs to the vomition centers.
Visceral afferents from the gastrointestinal tract (vagus or sympathetic nerves)
Visceral afferents from outside the gastrointestinal tract - this includes signals from bile ducts, peritoneum, heart and a variety of other organs.
Afferents from extramedullary centers in the brain - certain psychic stimuli (odors, fear), vestibular disturbances (motion sickness) and cerebral trauma
1. Nausea - unpleasant psychic experience.
2. Retching phase - abdominal muscles undergo a few rounds of coordinated contractions together with the diaphragm and the muscles used in respiratory inspiration.
3. Expulsive phase - intense pressure is formed in the stomach brought by enormous shifts in both the diaphragm and the abdomen. The vigorous contractions of these muscles last much longer than a normal period of muscular contraction. The pressure is then suddenly released when the upper esophageal sphincter relaxes resulting in the expulsion of gastric contents.
VOMITING
Manifested by nausea, pallor and diaphoresis, followed by forceful gagging and retching.
REGURGITATION
Effortless and not preceded by nausea.
But , the unpleasant sensations of gastric contents in mouth during regurgitation, may trigger gagging and true vomiting.
Gastric secretions are highly acidic. Recent food Malodorous. Blood “coffee ground vomiting"(as the iron in the blood is
oxidized) Bile Fecal vomiting-consequence of intestinal obstruction or a
gastrocolic fistula non-productive emesis or dry heaves-vomiting reflex
continues for an extended period with no appreciable vomitus
Bright red-bleeding from the oesophagus
Dark red vomit with liver-like clots- profuse bleeding in the stomach (e.g.; perforated ulcer)
Coffee ground-like vomit-less severe bleeding in the stomach-gastric acid has had time to change the composition of the blood
Yellow vomit-bile indicates that the pyloric valve is open and bile is flowing into the stomach from the duodenum.
FBC
U & E
Creatinine
Stool serology
Abdominal X-Ray
Surgical opinion if obstruction
Exclude systemic disease
Aspiration of vomit
Under normal circumstances the gag reflex and coughing will prevent this from occurring. The individual may choke and asphyxiate or suffer an aspiration pneumonia.
Dehydration and electrolyte imbalance
Tears in GIT
1. If these tears are limited to the inner lining of esophagus, they are called Mallory-Weiss tears-Passing of bright red or dark blood in the vomitus.
2. Tears through the entire wall of the esophagus resulting in perforation and the escape of stomach contents outside the gut- “Boerhaave’s syndrome
3. Painful bruises or tears in the abdominal wall muscles.
Dentistry
Recurrent vomiting may lead to destruction of the tooth enamel due to the acidity of the vomit and also can degrade tissue of the gum.
If prolonged, weight loss or malnutrition may occur.
Stabilize patient and fluid resuscitation as initial therapy with electrolyte correction
Surgical consultation if obstruction suspected Oral rehydration with small amounts of liquids if tolerated Treat infections if indicated
Remove toxins and allergens Surgical interventions for volvulus, Hirschprung, intracranial
masses, pyloric stenosis, other anatomic causes Correct metabolic derangements
Lifelong gluten-free diet for celiac disease
Rare use of antiemetics/promotility agents for chemotherapy, motion sickness, postsurgery, gastroesophageal reflux disease

Acute and recurrent
ABDOMINAL PAINDEFINITION
Abdomen – the part of body
lying between the thorax and
pelvis, containing the abdominal
cavity & viscera
Pain – feeling of distress,
suffering, caused by
stimulation of specialized
nerve endings.
Visceral pain
•nerves within gut detect
injury,affecting soft organ
n&body tissue
•‘’discomfort’’ and poorly
localized
Somatic pain
•overlying body
structures are injured
•Described as MSK
pain
•Pain is sharp, intense,
discrete & localized
Referred pain
•Painful sensation in a body
region distant from true
source of pain
•Caused by activation of
spinal cord somatic sensory
cell bodies by intense
signaling from visceral
afferent nerves located at
the same level.
CATEGORIES
Can signal presence of dangerous intra-abdominal process
-Eg: appendicitis, bowel obstruction
Or originate from extraintestinal sources
-Eg: lower lobe pneumonia or urinary tract stone
history
onset- sudden or gradual, episodes, association w meals, history of injuryNature – sharp vs dull, colicky or constant, burningLocation – epigastric, periumbilical,generalized, R or L lower quardrant, change in location over timeFever – presence suggests appendicitis or other infection Extraintestinal symptoms – cough, dyspnea, dysuria, urinary frequency, flank painCourse of symptoms – worsening or improving, changes in nature or location of pain
General – growth & nutrition, general appearance,
hydrational status, degree of discomfort, body position
Abdominal – tenderness, distention, bowel sounds, rigidity,
guarding, mass
Genitalia – testicular torsion, hernia, PID, ectopic pregnancy
Surrounding structures – breath sounds, rales(crepitation),
wheezing, flank tenderness, tenderness of abd. wall
structures, ribs, costochondral joints
Rectal examination – perianal lesions, stricture, tenderness,
fecal impaction, blood
LABORATORY
CBC, C-Reactive protein, ESR – evidence of infection/
inflammation
AST, ALT, GGT, Bilirubin – biliary or liver dss
Amylase, lipase - pancreatitis
Urinalysis – UTI, bleeding d/t stone, trauma or obstruction
Pregnancy test (older females) – ectopic pregnancy
RADIOLOGY
Plain flat & upright abdominal films – bowel obstruction,
appendiceal fecalith, free intraperitoneal, kidney stones
CT scans – rule out abscess, appendicitis, Crohn dss,
pancreatitis, gallstones, kidney stones
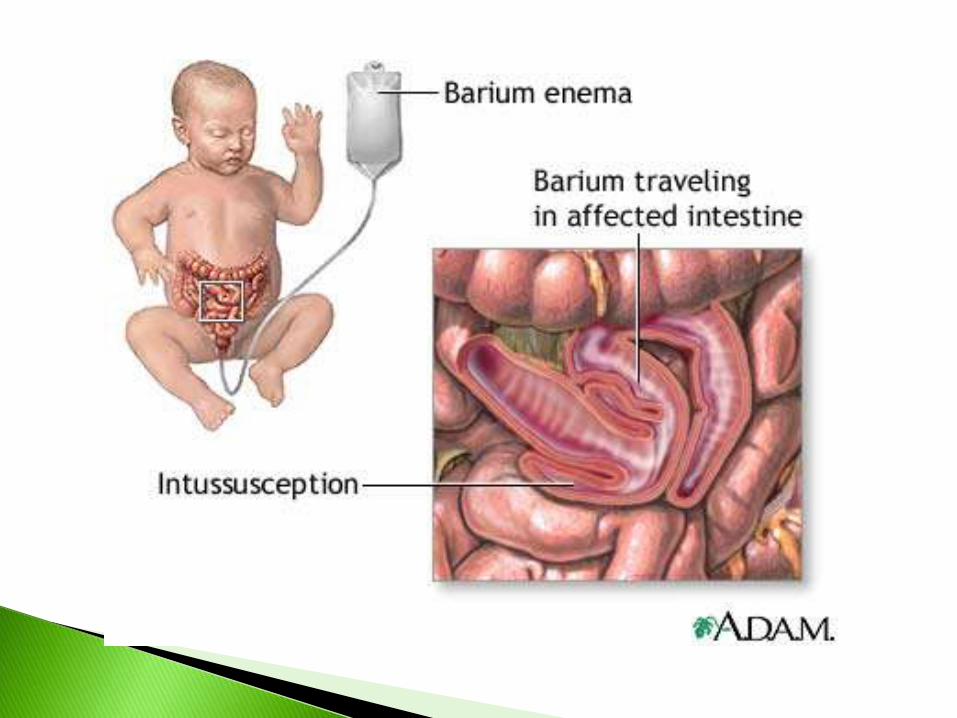
Barium enema - Intussusception, malrotation
Ultrasound – gallstones, appendicitis, intussusception,
pancreatitis, kidney stones.
ENDOSCOPY
Upper endoscopy – suspected PU/ esophagitis
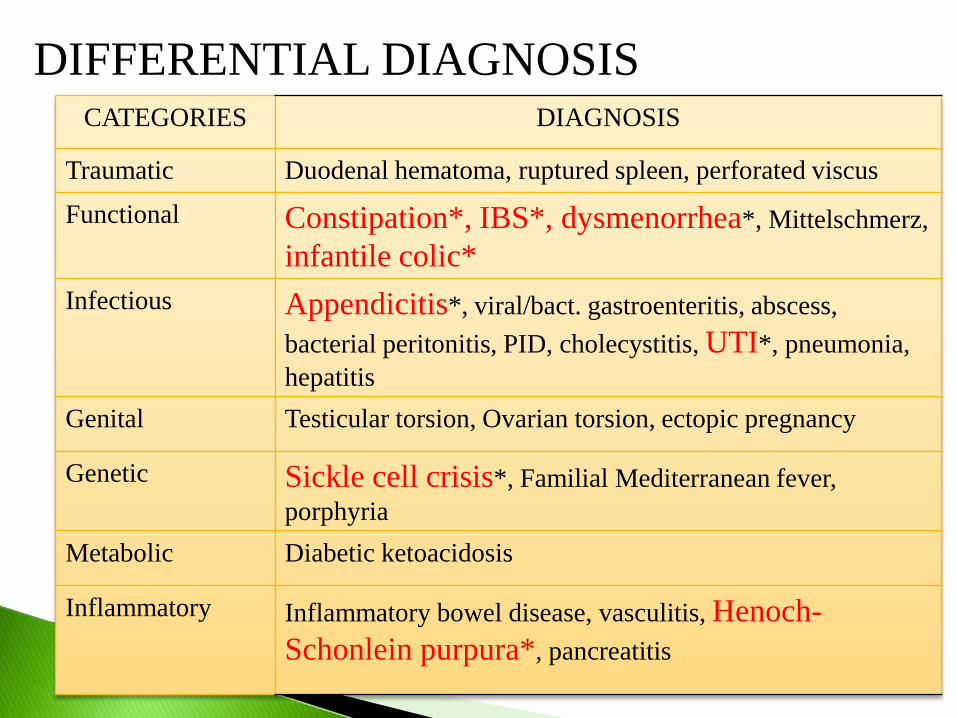
DIFFERENTIAL DIAGNOSISCATEGORIES DIAGNOSIS
Traumatic Duodenal hematoma, ruptured spleen, perforated viscus
Functional Constipation*, IBS*, dysmenorrhea*, Mittelschmerz,
infantile colic*
Infectious Appendicitis*, viral/bact. gastroenteritis, abscess,
bacterial peritonitis, PID, cholecystitis, UTI*, pneumonia,
hepatitis
Genital Testicular torsion, Ovarian torsion, ectopic pregnancy
Genetic Sickle cell crisis*, Familial Mediterranean fever,
porphyria
Metabolic Diabetic ketoacidosis
Inflammatory Inflammatory bowel disease, vasculitis, Henoch-
Schonlein purpura*, pancreatitis
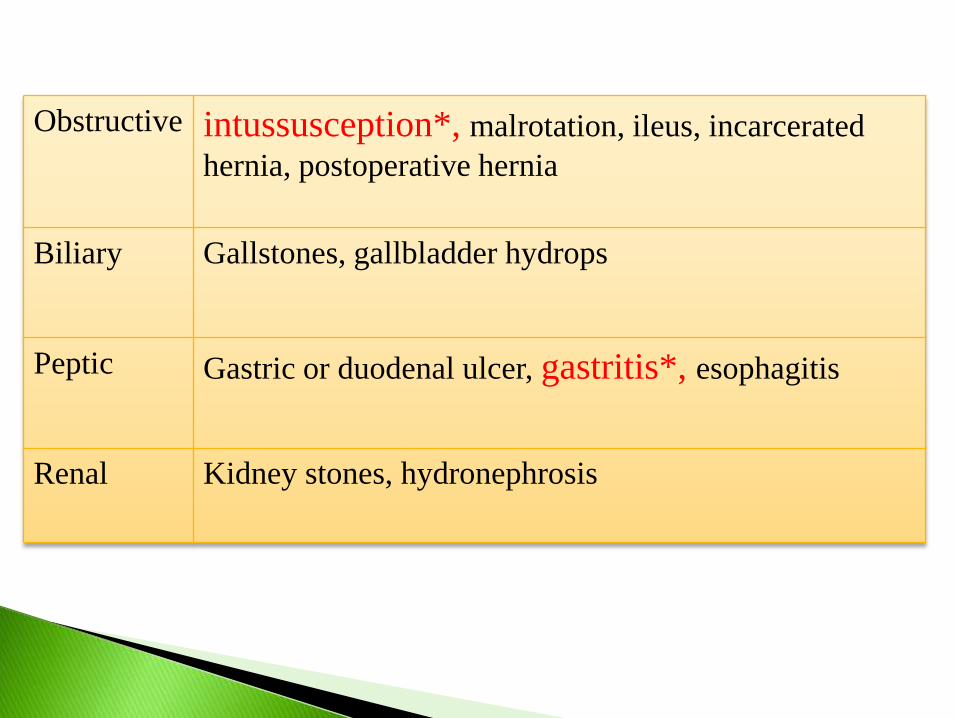
Obstructive intussusception*, malrotation, ileus, incarcerated
hernia, postoperative hernia
Biliary Gallstones, gallbladder hydrops
Peptic Gastric or duodenal ulcer, gastritis*, esophagitis
Renal Kidney stones, hydronephrosis
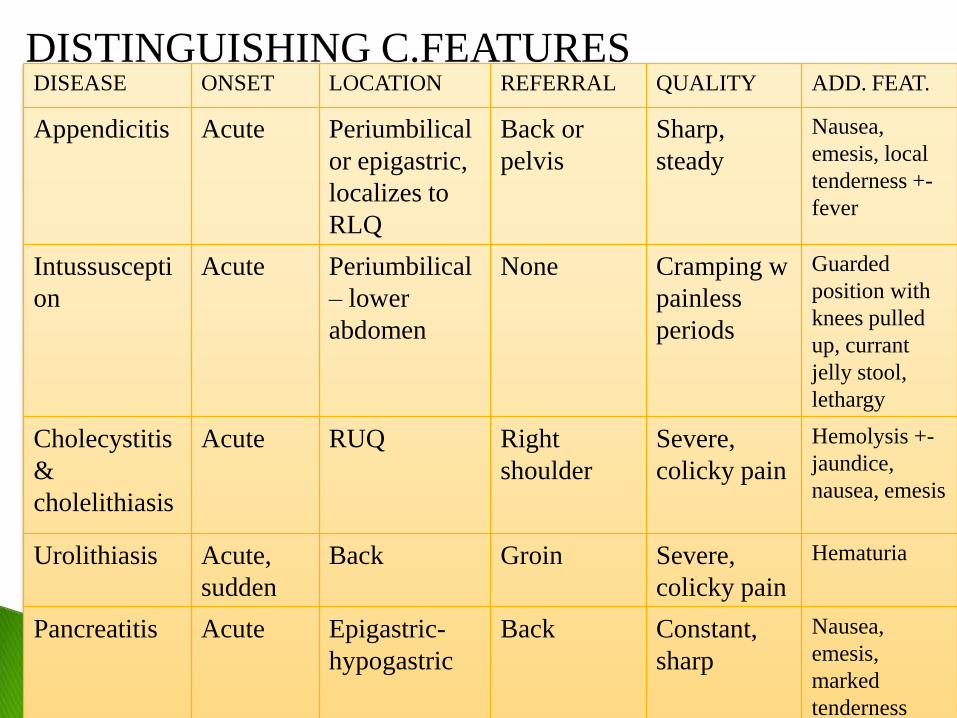
DISTINGUISHING C.FEATURESDISEASE ONSET LOCATION REFERRAL QUALITY ADD. FEAT.
Appendicitis Acute Periumbilical
or epigastric,
localizes to
RLQ
Back or
pelvis
Sharp,
steady
Nausea,
emesis, local
tenderness +-
fever
Intussuscepti
on
Acute Periumbilical
– lower
abdomen
None Cramping w
painless
periods
Guarded
position with
knees pulled
up, currant
jelly stool,
lethargy
Cholecystitis
&
cholelithiasis
Acute RUQ Right
shoulder
Severe,
colicky pain
Hemolysis +-
jaundice,
nausea, emesis
Urolithiasis Acute,
sudden
Back Groin Severe,
colicky pain
Hematuria
Pancreatitis Acute Epigastric-
hypogastric
Back Constant,
sharp
Nausea,
emesis,
marked
tenderness
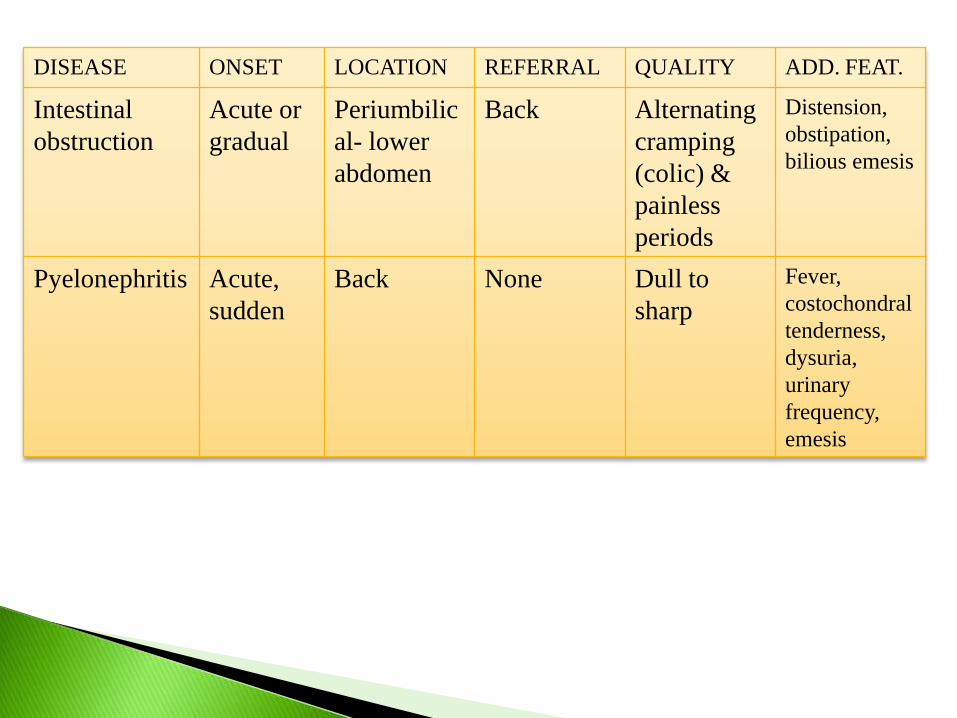
DISEASE ONSET LOCATION REFERRAL QUALITY ADD. FEAT.
Intestinal
obstruction
Acute or
gradual
Periumbilic
al- lower
abdomen
Back Alternating
cramping
(colic) &
painless
periods
Distension,
obstipation,
bilious emesis
Pyelonephritis Acute,
sudden
Back None Dull to
sharp
Fever,
costochondral
tenderness,
dysuria,
urinary
frequency,
emesis
A P P E N D I C I T I S
Clinical Features
Lower abdominal pain- right iliac fossa,Nausea and
vomiting,loss of appetite,Diarrhoea,Dysuria
Physical Findings
quiet ,dehydrated.Tenderness on palpation or
percussion ,discomfort, Guarding signifies
peritonitis,
Rectal examination is only required if other
diagnosis are suspected e.g. ovarian or adnexal
pathology.
APPENDICITIS
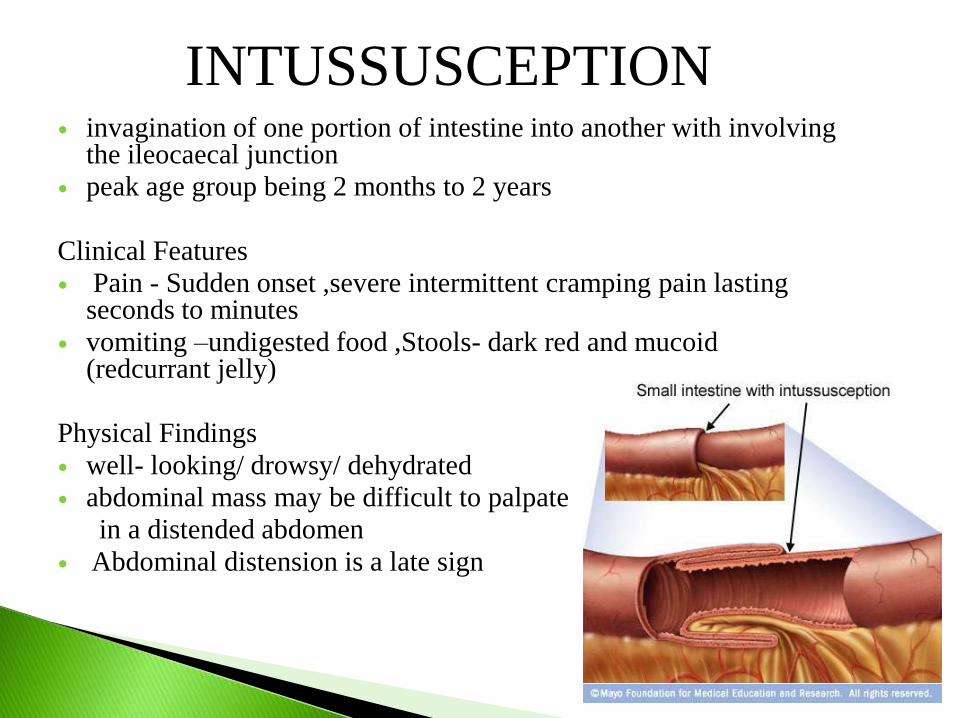
invagination of one portion of intestine into another with involving the ileocaecal junction
peak age group being 2 months to 2 years
Clinical Features
Pain - Sudden onset ,severe intermittent cramping pain lasting seconds to minutes
vomiting –undigested food ,Stools- dark red and mucoid(redcurrant jelly)
Physical Findings
well- looking/ drowsy/ dehydrated
abdominal mass may be difficult to palpate
in a distended abdomen
Abdominal distension is a late sign
INTUSSUSCEPTION
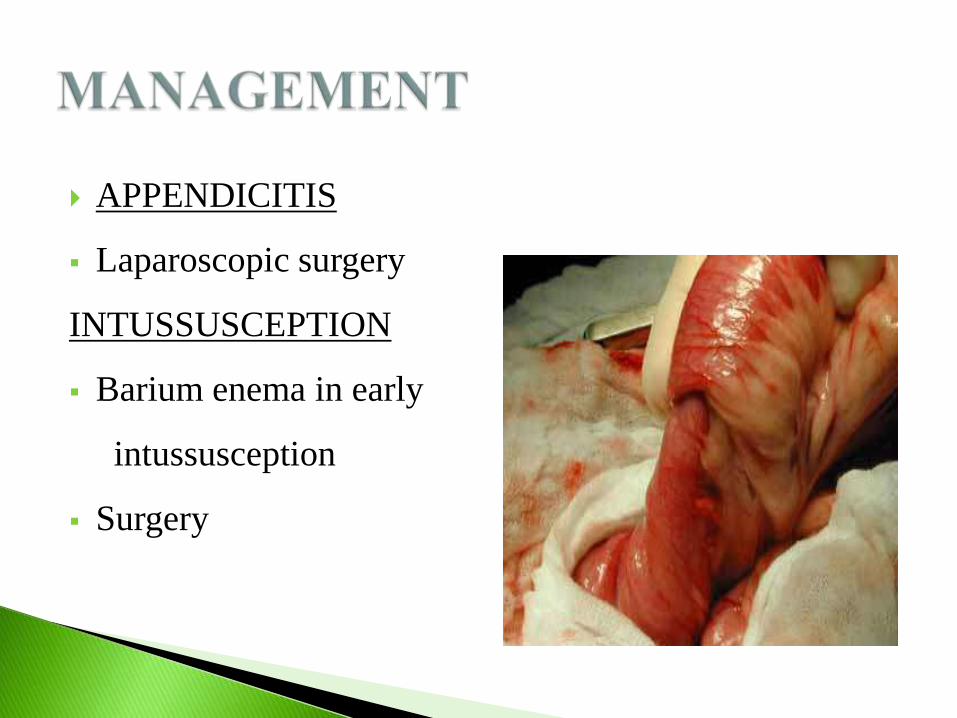
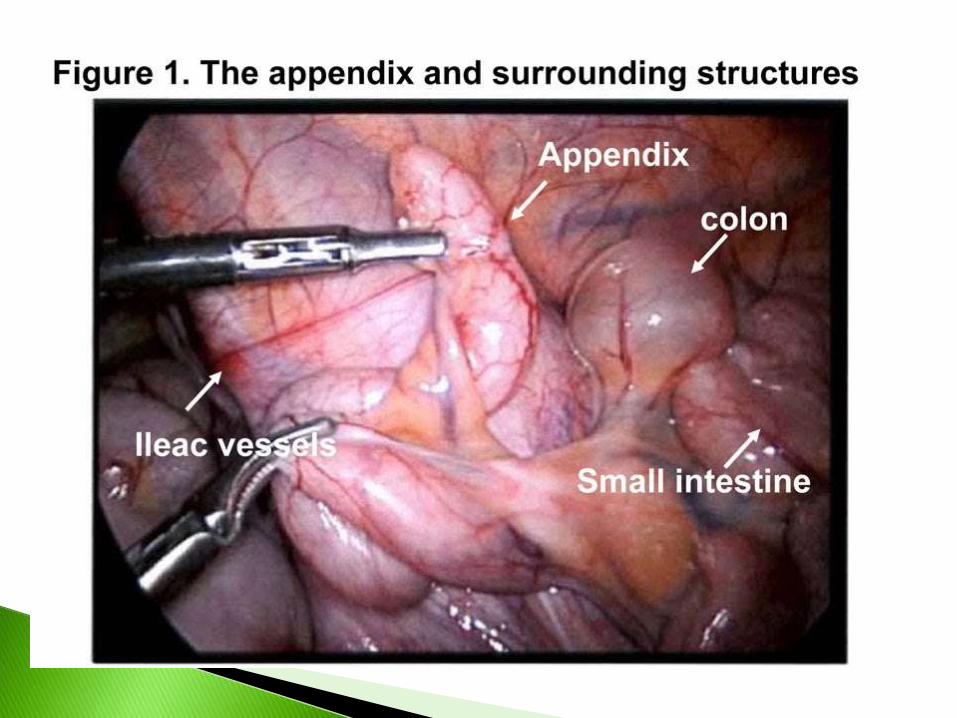
APPENDICITIS
Laparoscopic surgery
INTUSSUSCEPTION
Barium enema in early
intussusception
Surgery
DEFINITION CRITERIA
Occurrence of multiple
episodes of abdominal
pain over at least 3
months that are severe
enough to cause some
limitation of activity
At least 3 bouts of
significant abd. pain
over 3 months
Severe phase lasting at
least 3 mins
Usually in children
above 3 yr old.
DIAGNOSTIC APPROACH
When taking history, pediatrician should ask about the
warning signs for underlying diseases
If any warning signs are presents, further investigation
is necessary.
Even if they are absent, some laboratory evaluation is
warranted.
Vomiting
Abnormal
screening lab.
study
feverBilious emesis
Growth failure
Pain awakening child
from sleep
Weight loss
Location away from periumbilical
region
Blood in stools or emesis
Delayed puberty
CBC
ESR
Amylase, lipase
Urinalysis
Abdominal ultrasound
Trial of 3- day lactose-
free diet
CT scan
Celiac disease serology
Barium upper GI
Endoscopy
Colonoscopy
INVESTIGATIONSFOLLOW UP
Functional abdominal pain* -
IBS*
Chronic pancreatitis
Gallstones
Peptic disease - duodenal ulcer, gastric ulcer, esophagitis
Lactose intolerance*
Fructose malabsorption
Inflammatory bowel disease* - crohn’s disease, ulcerative colitis
Constipation*
Obstructive uropathy
Congenital intestinal malformation – stricture or web, malrotation, duplication cyst
Celiac disease*
Pain that characteristically occurs daily or nearly every
day
Not assoc. with or relieved by eating/ defecation
Assoc. with sig. loss of ability to function normally.
These kids have personality traits that include tendency
towards anxiety & perfectionism – results in stress
Parents noted that child enjoys going to school, but the
pain often worst at the start of school day & before
returning to school after vacations.
• cramping, abdominal pain, bloating, constipation, and diarrhea.
• Pain begin with a change in stool frequency
/consistency.
• A stool pattern fluctuating between diarrhea and
constipation.
• Relief of pain with defecation
• Symptom are link to gut motility
• Modulated by psychosocial factor such as stress and
anxiety.
- Treat underlying conditions
- Allows children to resume with daily activities
- Reassures that the although pain is there, will not harm
the children physically (in case of FAP)
- IBS-can control symptoms with diet, stress management, and prescribed medications.


![GIS - K21 DIARRHOEA .ppt [Read-Only]ocw.usu.ac.id/course/download/1110000120...diarrhoea - freq. ≥3 x /day - changing of consistency - with/ without vomiting - with/without bloody](https://img.pdfslide.net/doc/110x75/5ea22a74b6bee67fea1b7254/gis-k21-diarrhoea-ppt-read-onlyocwusuacidcoursedownload1110000120.jpg)













![Evidence-Based Complementary and AlternativeMedicine · 2019. 7. 31. · Evidence-Based Complementary and AlternativeMedicine vomiting, diarrhoea, ulceration, and bleeding [ ]. Gas-trointestinal](https://img.pdfslide.net/doc/110x75/613baed6f8f21c0c826922b1/evidence-based-complementary-and-alternativemedicine-2019-7-31-evidence-based.jpg)