Embed Size (px)
Citation preview

An approach to a child with An approach to a child with microcephalymicrocephaly
Dr.Anita LamichhaneDr.Anita Lamichhane
MD Resident (paediatrics)MD Resident (paediatrics)
Shaikh Zayed Hospital Shaikh Zayed Hospital
LahoreLahore

MicrocephalyMicrocephaly
A child whose head circumference is more than A child whose head circumference is more than
three standard deviations below the mean for three standard deviations below the mean for
age and sexage and sex

Normal head circumference at birthNormal head circumference at birth
Male: 35cm(mean) range = 32---37 cm Male: 35cm(mean) range = 32---37 cm Female: 34cm(mean) Female: 34cm(mean)
Rate of growth of head circumferenceRate of growth of head circumference
2cm/month 12cm/month 1stst three months of life three months of life 1cm/month 4-6 months of age1cm/month 4-6 months of age 0.5cm/month 6-12 months of age0.5cm/month 6-12 months of age 47cm at 1 yr of age47cm at 1 yr of age 49 cm at 2 yrs of age49 cm at 2 yrs of age



HC reflects brain volume, a small skull reflects a small brain.HC reflects brain volume, a small skull reflects a small brain.
Incidence of moderate to severe mental retardationIncidence of moderate to severe mental retardation
HC from 2-3 SD below the age is 33%.HC from 2-3 SD below the age is 33%. HC > 3 SD, incidence is 62%HC > 3 SD, incidence is 62%
Not always associated with mental retardationNot always associated with mental retardation

types of microcephalytypes of microcephaly
Primary microcephaly Primary microcephaly (genetic)(genetic)
primary defect in brain primary defect in brain developmentdevelopment
prenatal onsetprenatal onset postnatal onsetpostnatal onset
Secondary microcephaly (non Secondary microcephaly (non genetic /acquired)genetic /acquired)
prenatal onsetprenatal onset postnatal onsetpostnatal onset

Causes of microcephalyCauses of microcephaly

Primary microcephaly ( genetic)Primary microcephaly ( genetic)
Prenatal onset Prenatal onset chromosomal anomalieschromosomal anomalies
Down syndrome (21 trisomyDown syndrome (21 trisomy))
Edward syndrome (18 trisomyEdward syndrome (18 trisomy
Patau syndrome (13 trisomyPatau syndrome (13 trisomy ))
malformationsmalformations
HoloprosencephalyHoloprosencephaly
LissencephalyLissencephaly

Contd.Contd.
malformation syndromemalformation syndrome
de Lange syndromede Lange syndrome
hereditary conditionshereditary conditions
Autosomal recessive ( familial)Autosomal recessive ( familial) Autosomal dominantAutosomal dominant

Post natal onsetPost natal onset
malformation Syndromesmalformation Syndromes
Aicardi syndromeAicardi syndrome
Angel man syndromeAngel man syndrome
Fanconi syndromeFanconi syndrome
Rubinstein Taybi syndromeRubinstein Taybi syndrome

Contd…Contd…
Prader-willi syndromePrader-willi syndrome
Beckwith wiedemann syndrome Beckwith wiedemann syndrome
Bloom syndromeBloom syndrome
Cri-du-chat ( 5P )Cri-du-chat ( 5P )

Secondary microcephaly Secondary microcephaly (nongenetic /acquired)(nongenetic /acquired)
Prenatal onsetPrenatal onset
Intrauterine TORCH infectionIntrauterine TORCH infection
Fetal alcohol syndromeFetal alcohol syndrome
Maternal phenylketonuriaMaternal phenylketonuria

Contd…Contd…
Post natal onsetPost natal onset
perinatal asphyxia with resultant HIEperinatal asphyxia with resultant HIE
perinatally acquired herpes simplex perinatally acquired herpes simplex encephalitis/meningitisencephalitis/meningitis
head injuryhead injury
endocrine anomaliesendocrine anomalies
hypothyroidismhypothyroidism hypopitutarismhypopitutarism
inherited metabolic disease such as PKUinherited metabolic disease such as PKU

Congenital CNS anomaliesCongenital CNS anomalies
Agenesis of the cerebellar vermisAgenesis of the cerebellar vermis
Agenesis of the corpus callosumAgenesis of the corpus callosum
EncephaloceleEncephalocele
MacrogyriaMacrogyria
PorencephalyPorencephaly
SchizencephalySchizencephaly

Others…..Others…..
HyperthermiaHyperthermia
RadiationRadiation
MalnutritionMalnutrition
DrugsDrugs
Fetal hydantoin syndromeFetal hydantoin syndrome

pathogenesispathogenesis
Occurs as a result of Occurs as a result of
Small brain & poorly growing skull Small brain & poorly growing skull
An abnormal neuronal migration during fetal An abnormal neuronal migration during fetal development. development.
Cytoarchitectural derangements.Cytoarchitectural derangements.
heterotopias of neuronal cells.heterotopias of neuronal cells.

Microcephaly VeraMicrocephaly Vera
an Autosomal recessive disorderan Autosomal recessive disorder
severe hypoplasia of the frontal regions of the brain and skull. severe hypoplasia of the frontal regions of the brain and skull.
severe mental retardation. severe mental retardation.
NoteNote:: HC alone should never be used to establish a prognosis for HC alone should never be used to establish a prognosis for intellectual development.intellectual development.

Aicardi SyndromeAicardi Syndrome
females onlyfemales only
agenesis of the corpus agenesis of the corpus callosumcallosum
infantile Spasms infantile Spasms
Severe mental & Severe mental & development retardationdevelopment retardation
seizures seizures
gray matter heterotopias.gray matter heterotopias.

Bloom SyndromeBloom Syndrome
Autosomal recessiveAutosomal recessive
MicrocephalyMicrocephaly
short stature short stature
DNA fragilityDNA fragility
a butterfly shaped facial rash. a butterfly shaped facial rash.
prone to develop Cancer. prone to develop Cancer.
Genetic diagnosis is available.Genetic diagnosis is available.

Down's SyndromeDown's Syndrome
Trisomy 21 Trisomy 21
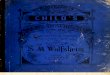
Microcephaly. Microcephaly.
up slanting Fissures, up slanting Fissures,
epicanthal Folds, epicanthal Folds,
flat facial profile, flat facial profile,
small low set ears and small low set ears and
incurving of the fifth finger. incurving of the fifth finger.
a single palmar crease ( simian a single palmar crease ( simian crease)crease)
hypotoniahypotonia

A child with Down SyndromeA child with Down Syndrome

Edward syndromeEdward syndrome Trisomy 18Trisomy 18
MicrocephalyMicrocephaly
Prominent occiputProminent occiput
MicrognathiaMicrognathia
Narrow foreheadNarrow forehead
Cleft lip and palateCleft lip and palate
Low set earsLow set ears
ASD & VSDASD & VSD

Cri-Du-Chat SyndromeCri-Du-Chat Syndrome
MicrocephalyMicrocephaly
shrill cat like cryshrill cat like cry
High arch palateHigh arch palate
small chin small chin

Rubinstein taybi syndromeRubinstein taybi syndrome
Mental & growth retardationMental & growth retardation
Broad thumbs with talpismBroad thumbs with talpism
Microcephaly with Microcephaly with
mandibular & maxillary mandibular & maxillary hypoplasia hypoplasia
anteverted nose &anteverted nose &
antemongoloid slant to antemongoloid slant to palpebral fissurespalpebral fissures

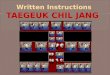
Cornelia de Lange syndromeCornelia de Lange syndrome
Mental & growth retardationMental & growth retardation
SynophrysSynophrys
MicrognathiaMicrognathia
ASD & VSDASD & VSD

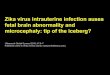
Patau syndromePatau syndrome
Trisomy 13Trisomy 13
MicrocephalyMicrocephaly
Cutis aplasia ( scalp defect )Cutis aplasia ( scalp defect )
Eyes Eyes cataractcataract ColobomataColobomata MicrophthalmiaMicrophthalmia corneal opacitiescorneal opacities
HandsHands
polydactylypolydactyly

PhenylketonuriaPhenylketonuria Deficiency of phenylalanine hydroxylase in the liverDeficiency of phenylalanine hydroxylase in the liver Accumulation of phenylalanine in the blood Accumulation of phenylalanine in the blood
Toxic to brainToxic to brain Causes Causes microcephalymicrocephaly mental retardationmental retardation cerebral palsycerebral palsy eczemaeczema mousy odor of urinemousy odor of urine

Contd…Contd…
Diagnosed by increased serum phenylalanine in Diagnosed by increased serum phenylalanine in
BloodBlood
Guthrie test ( 5Guthrie test ( 5thth– 15– 15thth day of life) day of life)
Treatment A diet low in phenylalanineTreatment A diet low in phenylalanine

How to approach a How to approach a childchild
with microcephalywith microcephaly

HistoryHistory
Family history (for genetic cause)Family history (for genetic cause)
Exposure of radiation during pregnancyExposure of radiation during pregnancy
Maternal drug historyMaternal drug history
Infection during pregnancyInfection during pregnancy
Maternal DM or PKUMaternal DM or PKU

Contd..Contd.. Difficult delivery: Difficult delivery:
forceps delivery, forceps delivery,
meconium stained liquormeconium stained liquor
cord around the neck cord around the neck
and low Apgar Scores all raises the possibility of hypoxic and low Apgar Scores all raises the possibility of hypoxic ischemic encephalopathyischemic encephalopathy
Significant fever during neonatal periodSignificant fever during neonatal period

h/o h/o high-pitched cryhigh-pitched cry
poor feeding poor feeding
seizures seizures
increased movement of the arms increased movement of the arms and legs (spasticity) and legs (spasticity)

ExaminationExamination
Introduction of oneself to the parentsIntroduction of oneself to the parents
Size of the parents & other siblings head circumferenceSize of the parents & other siblings head circumference
Note the child’s alertnessNote the child’s alertness
Look for any Dysmorphic featureLook for any Dysmorphic feature
( intrauterine TORCH, de Lange, ( intrauterine TORCH, de Lange, Rubinstein Taybi)Rubinstein Taybi)

Child’s posture & symmetry of the movementsChild’s posture & symmetry of the movements
( voluntary & involuntary )( voluntary & involuntary )
Inspect the skin for neurocutaneous stigmata Inspect the skin for neurocutaneous stigmata
Head circumferenceHead circumference
Height & weight & plot in the centile chartHeight & weight & plot in the centile chart

Note the child’s overall growthNote the child’s overall growth
generally small generally small
only head smallonly head small
examine the head for any scar marksexamine the head for any scar marks
( surgical repair of Craniosynostosis, ( surgical repair of Craniosynostosis, closure of Encephalocele) closure of Encephalocele)

Contd..Contd..
Shape of the head Shape of the head
flat occiput of Autosomal recessive flat occiput of Autosomal recessive microcephaly microcephaly
Palpate the head for ridging along the suture line & any deformity of Palpate the head for ridging along the suture line & any deformity of skull contourskull contour
(Craniosynostosis) or bony defects ( repaired (Craniosynostosis) or bony defects ( repaired Encephalocele) Encephalocele)


Anterior fontanelleAnterior fontanelle a large AF occurs in a large AF occurs in
trisomiestrisomies
congenital rubellacongenital rubella
hypothyroidism hypothyroidism
Petechiae or skin rash Petechiae or skin rash

Eye Eye
micropthalmos micropthalmos (TORCH)(TORCH)
lens for cataract (lens for cataract (TORCH, trisomiesTORCH, trisomies ) )
fundus for chorioretinitis (fundus for chorioretinitis (TORCH)TORCH)
glaucomaglaucoma ( congenital rubella )( congenital rubella )
red reflex red reflex ( rubella)( rubella)

hypotelorismhypotelorism (Holoprosencephaly)(Holoprosencephaly)
upward slant upward slant ( ( down syndrome)down syndrome)
epicanthi fold epicanthi fold ( trisomies )( trisomies )
squintsquint ( TORCH)( TORCH)
pupils for anisocoria pupils for anisocoria ( cong. Varicella ) ( cong. Varicella )

Ears for hearingEars for hearing
impairment ( TORCH )impairment ( TORCH )
neck for goiterneck for goiter
hypothyroidismhypothyroidism

Systemic examinationSystemic examination
CVSCVS for congenital heart defects ( congenital rubella,trisomies )for congenital heart defects ( congenital rubella,trisomies )
AbdomenAbdomen
hepatosplenomegaly (TORCH)hepatosplenomegaly (TORCH)
GenitaliaGenitalia
micropenis with hypopitutarism structure ( cryptorchidism)micropenis with hypopitutarism structure ( cryptorchidism)
Joint contracturesJoint contractures
Asses the gross and fine motor developmentAsses the gross and fine motor development– 180 degree maneuver– 180 degree maneuver

InvestigationsInvestigations
Serological tests for intrauterine TORCH infectionSerological tests for intrauterine TORCH infection
Chromosomal analysis for Autosomal Trisomy syndromeChromosomal analysis for Autosomal Trisomy syndrome
Neonatal screening tests for PKU & congenital hypothyroidismNeonatal screening tests for PKU & congenital hypothyroidism

Urine testUrine test
Metabolic screening to detect virus Metabolic screening to detect virus excretion with CMVexcretion with CMV
CSFCSF
to detect intrauterine or perinatal TORCH to detect intrauterine or perinatal TORCH infectioninfection

a)a) Skull x raySkull x ray for cerebral calcificationfor cerebral calcification
CMV --- periventricularCMV --- periventricular
Toxoplasmosis—diffuseToxoplasmosis—diffuse
to detect early closure of suturesto detect early closure of sutures

CT SCAN/ MRICT SCAN/ MRI
for cerebral malformationsfor cerebral malformations
evidence of perinatal asphyxia or evidence of perinatal asphyxia or intrauterine infectionintrauterine infection

Genetic studies are indicated in patientsGenetic studies are indicated in patients
with Dysmorphic featureswith Dysmorphic features

Microcephaly may be diagnosed before birth Microcephaly may be diagnosed before birth by prenatal ultrasound.by prenatal ultrasound.
Genetic counseling should be doneGenetic counseling should be done

ManagementManagement
No treatment for microcephalyNo treatment for microcephaly
Baby’s head cannot be returned to a normal size & shapeBaby’s head cannot be returned to a normal size & shape
Includes focusing on preventing or minimizing deformities & Includes focusing on preventing or minimizing deformities & maximizing the child’s capabilities at home & in the community.maximizing the child’s capabilities at home & in the community.

Contd..Contd..
According to the cause.According to the cause.
AnticonvulsantsAnticonvulsants
PhysiotherapyPhysiotherapy
Hearing & speech therapyHearing & speech therapy
Dietary management for failure to Dietary management for failure to thrive thrive
Genetic counseling Genetic counseling