Embed Size (px)
Citation preview

ANATOMY AND EXAMINATION OF THE KNEE
Dr.G.Sri HarshaP.G. In Orthopaedics
MODERATORSDR.G.NAGARAJ SirDR.RAVI.G.O Sir

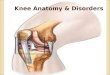
ANATOMY INTRODUCTION• Knee joint is the largest synovial joint in the body.• It has• 1.Tibiofemoral joint. • 2.Patellofemoral joint.
• The articulation between the femur and tibia is weight-bearing, and the articulation between the patella and the femur allows the pull of the quadriceps muscle to be directed anteriorly over the knee to the tibia without tendon wear.
• Basically the joint is a hinge joint that allows mainly flexion and extension

The Structures around the Knee are broadly classified into
• Osseous Structures.• Extraarticular Tendinous Structures.• Extraarticular Ligamentous structures• Intraarticular Structures.

Osseous Structures• Osseous Structures around the Knee consist of the Patella,
Femoral Condyles and Tibial Plateus or Condyles.• The Femoral Condyles are two rounded structures that are
eccentrically curved. Anteriorly the condyles are flattened which creates a larger surface for contact and weight transmission.
• The groove found anteriorly between the femoral condyles is the Patellofemoral groove or the Trochlea
• Posteriorly they are separated by Intercondylar notch.

• The proximal end of the tibia forms two flat surfaces the condyles or plateaus that articulate with the femoral condyles.
• They are separated from each other by an intercondylar eminence with its medial and lateral intercondylar tubercles.
• Anterior and Posterior to the intercondylar eminence are the areas that serve as attachment for cruciate ligaments and menisci.

• The patella is triangular sesamoid bone that is wider at the proximal pole than the distal pole.
• The articular surface of the patella is divided by a vertical ridge,resulting in a smaller medial and larger lateral articular facet or surface.

Extra-Articular Tendinous StructuresThese are the quadriceps,the medial and lateral hamstring groups,the popliteus, the gastrocnemius and the iliotibial band.


The Popliteus muscle has 3 origins intracapsularly.
A.Lateral femoral condyle.B.Posterior horn of the lateral meniscus.C.Fibula,The femoral and fibular origins form the arms of an oblique Y shaped ligament.It is inserted into a broad triangular area above the soleal line on the posterior surface of the tibia.

• The Semimembranosus muscle has 5 distal expansions.
1.The oblique popliteal ligament.2.A second tendinous attachment. 3.Anterior or deep head.4.The direct head and,5.The distal portion of the semimembranosus.

Extra-Articular Ligamentous Structures
• The Capsule is a sleeve of fibrous tissue extending from the patella and patellar tendon anteriorly to the medial,lateral and posterior expanses of the joint.
• On the medial side of the knee joint, the capsule blends with the tibial collateral ligament and is attached on its internal surface to the medial meniscus.
• Laterally the capsule is separated by a space from the fibular collateral ligament and is not attached to the lateral meniscus

• The medial capsule is divided into 3 regions.• Antero-medial portion protects the anteromedial portion of
the knee and reinforced by medial patellar retinacula.• Mid-medial capsule is the deep layer of the medial
collateral ligament.

• Postero-medial capsular region or the Posterior oblique ligament extends from posterior edge of the medial collateral ligament to the insertion of the direct head of semimembranosus.
• The distal attachment is composed of 3 arms.
• Central arm or the Tibial arm-thickest part.
• Superior arm or Capsular arm.• Inferior arm or Superficial arm.

Medial Collateral Ligament is divided into 2 parts,1.Superficial MCL or Tibial Collateral Ligament.2.Deep MCL.
• Medial aspect of the knee is divided into 3 layers.
• 1st layer-Deep fascia containing the sartorius fascia.
• 2nd Layer-Superficial MCL or Tibial collateral ligament.
• 3rd Layer-Deep MCL which blends with the joint capsule.

• Lateral collateral ligament or Fibular collateral ligament stretches obliquely downward and forward from lateral femoral condyle proximally to the head of the fibula distally
• In contrast to the medial collateral ligament it neither fuses with the capsular ligament or the lateral meniscus thus making it more susceptible to be torn in the knee injuries.
• It is the prime stabilizer of the knee against the varus forces.
Lateral aspect of the knee is divided into 3 distinct layers• 1st layer-contains Iliotibial tract and superficial portion of the
biceps tendon and common peroneal nerve.• 2nd layer-Retinaculum of the quadriceps.• 3rd layer-Lateral part of the joint capsule.

Intra-Articular Structures SYNOVIAL MEMBRANE• The synovial membrane of the knee joint attaches to the
margins of the articular surfaces and to the superior and inferior outer margins of the menisci.
• Posteriorly, it reflects off the fibrous membrane of the joint capsule on either side of the posterior cruciate ligament.
• Anteriorly the synovial membrane is separated from the patellar ligament by an infrapatellar fat pad.

Bursae associated with the knee include the,Suprapatellar bursa,Prepatellar bursa, Infrapatellar bursa, and numerous other bursae associated with tendons and ligaments around the joint.

ANTERIOR CRUCIATE LIGAMENT• It is the primary restraint to anterior tibial translation.• It is an extrasynovial but intracapsular structure.• It courses from the femur to the tibia anteriorly, medially and
distally.
Femoral attachment-It is at the posterior part of the inner surface of the lateral femoral condyle.It has been described as a segment of the circle with straight anterior border and convex posterior surface.Tibial attachment-The ACL fibres fans out as they reach the tibial attachment.it gets inserted on a depressed area infront and lateral to the medial intercondylar tubercle.

• The ACL is divided into two parts-the Anteromedial and the Posterolateral bands.
• The fascicle of the AMB originate at the posterior and proximal aspect of the femoral attachment and insert at the anteromedial aspect of the tibial attachment.
• The fascicle of the PLB originate at the distal aspect of the femoral attachment and insert at the posterolateral aspect of the tibial attachment.
• Vascular supply of the ACL is by branches from the middle genicular artery. Additional supply is by the retropatellar fat via the inferior medial and lateral genicular arteries.
• Nerve supply of the ACL is from posterior articular nerve a branch of the posterior tibial nerve.


POSTERIOR CRUCIATE LIGAMENT.• It is also extrasynovial and intracapsular structure.• The PCL originates from the junction of the femoral notch roof
and the medial femoral condyle roughly 1 cm proximal to the articular surface.
• It inserts on the posterior aspect of the proximal tibia at the fovea,a depression between the tibial plateaus.
• It consists of two bundles, the anterolateral and posteromedial bundles.
• Vascular supply of the PCL is by the middle genicular artery mainly.
• Nerve supply is by the posterior articular nerve o branch of the posterior tibial nerve.


MENISCI• Menisci are two crescent shaped structures,triangular in cross
section and covers one half to two thirds of the articular surface of the tibial plateaus.
• They are composed of collagen fibers which are primarily circumferential, they also contain radial and perforating fibers.
• The peripheral edges of the menisci are convex,fixed and attached to the inner surface of the joint capsule.They are attached to the tibial plateaus by coronary ligaments.
• The menisci are largely avascular except at their peripheral attachment to the coronary ligaments.

Medial Meniscus is a “C” shaped structure larger in radius than the lateral meniscus and the posterior horn is wider than the anterior horn.• The anterior horn is attached firmly to the tibial surface anterior
to the tibial eminence and the ACL.• The posterior horn is attached just in front of the attachment of
the PCL and posterior to the intercondylar eminence.• The peripheral border of the meniscus is attached firmly to the
medial capsule and through the coronary ligament to the tibial plateau.
• The medial meniscus is larger in diameter,thinner in periphery and narrower in body and doesn’t not attach to either of the cruciate ligaments,but loosely attaches to the medial capsular ligaments.

Lateral meniscus is more circular than the medial meniscus and covers upto 2/3rds of the articular surface of the tibial plateau.• The anterior horn is attached to the tibia medially in front of the
intercondylar eminence and posterior horn is attached to the posterior aspect of the intercondylar eminence and in front of the posterior attachment of the medial meniscus.
• The lateral meniscus is smaller in diameter, thicker in periphery and more mobile than the medial meniscus.
• It is attached to both the cruciate ligaments and posteriorly to the medial femoral condyle by Ligament of Humphry(Ant. Meniscofemoral Lig.) of Ligament of Wrisberg(Post. Meniscofemoral Lig.)

• The blood supply of the menisci are predominantly from the lateral and medial genicular arteries.
• The vessels are arranged in a circumferential pattern with the radial branches directed toward the center of the joint.
• The depth of peripheral vascular penetration is approx.10% to 30% of the width of the medial meniscus and 10% to 25% of the width of the lateral meniscus.


POPLITEAL FOSSA• The popliteal fossa is a diamond-shaped space behind the knee joint
formed between muscles in the posterior compartments of thigh and leg.
• The margins of the upper part are formed medially by the distal ends of the semitendinosus and semimembranosus muscles and laterally by the distal end of the biceps femoris muscle.
• The margins of lower part of the space are formed medially by the medial
head of the gastrocnemius muscle and laterally by the plantaris muscle and the lateral head of the gastrocnemius muscle.
• The floor of the fossa is formed by the capsule of the knee joint and
surfaces of the femur and tibia, and, more inferiorly, by the popliteus muscle.
• The roof is formed by deep fascia, which is continuous above with the
fascia lata of the thigh and below with deep fascia of the leg.

Contents:• The major contents of the popliteal fossa are the popliteal
artery, the popliteal vein, and the tibial and common fibular nerves and popliteal group of lymph nodes.

BLOOD SUPPLY and INNERVATION.• Vascular supply to the knee joint is predominantly through
branches from the femoral, popliteal arteries.• The knee joint is innervated by branches from the obturator,
femoral, tibial, and common fibular nerves. LYMPHATIC DRAINAGE OF THE KNEE-• Knee drains into the popliteal group of lymph nodes and in turn
into the deep inguinal group of lymph nodes.

Examination of the Knee

Symptoms• Pain.• Swelling.• Stiffness.• Locking.• Deformity.• Giving away/felling of instability.• Limp.• Loss of function.

Signs-Inspection• For the proper examination of the knee the patients’ lower
limbs must be fully exposed from groin to the toes but covering the genitals.
• The patient has to be examined in standing,sitting and supine positions.

GaitWith the stiff knee the affected leg will swing outwards during walking.• In other affections of the joint the patient will limp with lurching on
the sound side to avoid the weight bearing.• Stance phase should be examined whether the knee extends fully
and note for any fixed flexion deformity.• Swing phase should be examined and note whether the knee
moves freely or held in fixed position.Attitude• In arthritic conditions the knee assumes a position of moderate
flexion which is the optimum position(25-30 deg of flexion) of the knee joint.
• In case of tubercular arthritis-stage 4 there will be destruction of the cruciate ligaments and the collateral ligaments and results in a “triple displacement”-flexion,posterior subluxation and lateral rotation of the tibia due to the contraction of the hamstring muscles.

Signs with patient standingDeformity can be best demonstrated with the patient in standing and bearing weight and feet pointing forward.Normally the knees and ankles touch in the midline,which means the knees are in slight valgus position(about 7 deg.for women and 5 deg.in men).• The Commonest deformities are1.Genu Valgum(Knock Knees)-The patient has to stand with the knees touching each other and the intermalleolar distance is measured.Normally it should be <8cms. 2.Genu Varum(Bow Legs)-The patient has to stand with the medial malleoli touching each other and the intercondylar distance measured.Normally it should be <6 cms.3.Genu Recurvatum-Hyperextension at the Knee joint

Signs with the patient Sitting• The patient should be made to
sit on a couch with knee dangling in 90 deg of flexion and examined from sideways.
• In this position the patella should be facing straight forwards.
• Patella alta is a condition where the patella is seated above than normal.
• Patella baja is a condition where the patella is seated below than normal.
• Patellar alignment can be measured by the Q angle.

• Q angle-it is subtended by a line drawn from the ASIS to the center of the patella and another from patella to the tibial tubercle.
• It is normally about 13-14 deg in men and 17-18 deg in women.
• An increasing Q angle is seen in Patella Alta and is a predisposing factor for the development of the Chondromalacia.

Signs with the patient in Supine position• Swellings-• Note for the presence of a diffuse
swelling confined to the limits of the synovial cavity and suprapatellar pouch indicating effusion.
• Note for the presence of the localised swellings around the knee joint.
• 1.Prepatellar bursitis(House-maid’s Knee).
• 2.Infrapatellar bursitis(Clergyman’s Knee).
• 3.Meniscal cysts-In the joint line.• 4.Exostosis(Diaphyseal aclasis).



• Discoloration around the knee joint• Look for any bruising around the knee joint suggesting
trauma to the superficial soft tissues or the ligaments around the knee joint.
• Meniscal injuries doesn’t show any bruising.• Look for the scars around indicating previous surgeries.• Sinuses around the knee joint indicating the infections.• Examine the quadriceps for wasting and loss of bulk.• Evidence of skin rash indicating the possibility of psoriatic
arthritis.

Palpation• Look for local rise of temperature.For the Tenderness-• Begin by flexing the knee and looking at hollows at the sides of the
patellar ligament,which lie over the joint line.Localised tenderness around the joint line indicates injuries to the meniscus,collateral ligament and fat pad injuries.
• Tenderness over the tibial tubercle is seen in Osgood schlatters disease and acute avulsion injuries of the patellar ligament.
PATELLA: • The patellar continuity should be checked in trauma cases to look
for fractures.• Displace the patella medially and laterally and palpate the articular
surfaces.Tenderness is found in Chondromalacia patellae.• Move the patella in all the directions.Reduced mobility is found in
Retropatellar arthritis.• Tenderness over the lower pole of patella is found in Sinding-
Larsen-Johansson disease.

Fairbank’s Apprehension Test- • Done for dislocation of the patella.• In this the patient is in supine position and the quadriceps
relaxed.The examiner flexes the knee while he slowly pushes the patella laterally.If there is tendency for dislocation the patient will be apprehensive and stops the test.
Tenderness over the quadriceps tendon is found in quadriceps tendinitis.• Tenderness over the femoral condyles is found in
Osteochondritis dissecans,more on the medial side.• This can be elicited by WILSONS test.For this the knee has to
be flexed and foot internally rotated and extend the knee completely.If the pain occurs at full extension and relieved by external rotation then its positive

• Examine the tone of quadriceps by placing a hand below the knee and asking the patient to press the leg against the examining hand.
• Examine the extensor apparatus-loss of active extension of the knee follows the rupture of the quadriceps tendon,patellar fracture ,rupture of patellar ligament and avulsion of the tibial tubercle.
• Look for the gaps in various structures of the extensor apparatus .

Effusion• The first sign of effusion is bulging at the sides of the patellar
ligament and obliteration of the hollows at the medial and lateral edges of the patella.
• With greater amount of effusion the suprapatellar pouch becomes distended.
• Patellar tap test(Ballottement test)-Squeeze the synovial fluid from the suprapatellar pouch starting at 15 cms above the knee
• Place the tips of the thumb and three fingers of the free hand on the patella and jerk it quickly downwards-A click of the patella on the femoral condyles indicates the presence of effusion.

• Fluid displacement test-This is used to detect small effusions.Start by squeezing fluid from the suprapatellar pouch and first stroke the medial side of the joint to displace it laterally.Now stroke the lateral side of the joint and see for the filling of the medial side of the joint.
• Cross fluctuation test-With the thumb on one side and fingers on the other side compress the knee joint to empty the hollows at the side of the joint.Now with the other hand forcefully push the fluid distally into the joint,which lifts the compressing hand.

• Haemarthrosis usually have a doughy feel on the suprapatellar pouch and occurs within half an hour of injury.
• Pyarthrosis usually have a diffuse tenderness and develops slowly and also associated with quadriceps wasting.

• Synovial thickening-pick up the skin and the relaxed quadriceps in the suprapatellar pouch to assess the synovial thickening which usually is spongy or boggy to touch.
• Synovial thickening is seen in inflammatory conditions like rheumatoid arthritis and villonodular synovitis.
• Transillumination test is performed on the swellings around the knee joint-positive in bursae and cystic swellings like the bakers cyst.
• Check for the Compressibility of the swelling by applying a gentle pressure over it-positive in Baker’s cyst and Popliteal aneurysm.

Examination of the popliteal fossa• Examination of the knee is incomplete without the
examination of the popliteal fossa.• With the patient standing look for the Baker’s cyst which is
a herniation of the synovial membrane posteriorly through the oblique popliteal ligament,just below the joint line.
• The pt has to be made lie in prone position and the knee flexed just less than 90 deg.
• The knee joint,popliteal artery and veins,nerves and tendons in the fossa has to be examined.

Movements at the knee joint• All movements are recorded with the help of goniometer.• Extension-the extension at the knee joint is normally 0 deg,but may be -15 deg
in women who are more likely to have a genu recurvatum.• Loss of full extension can be recorded as ‘the knee lacks X deg of extension’.• A springy block to full extension is suggestive of bucket handle meniscus tear.• A rigid block to full extension-the fixed flexion deformity of the knee is found in
arthritic conditions of the knee joint.• Hyperextension(Genu recurvatum)-knee extends beyond the point of femur
and tibial line. It is seen most commonly in girls,patella alta, chondromalacia patella, recurrent dislocation of the patella and tears of ACL,MCL,Medial Meniscus.
• It is recorded as X deg of hyperextension.• Flexion-normal flexion at the knee joint is from 0 deg to 135-140 deg and more
which is measured from 0 deg of extension until the heel touches the buttock.• Other method of estimating is the heel-buttock distance.(1 cm= 1 deg).• During this the examiner should observe for the movement of the patella.

Measurements• Wasting around the knee is common as a result of disuse,
which usually results from chronic inflammatory conditions.• First mark the knee joint line with a marker and make a
second mark at about 15-18 cms or at the point of maximal bulk proximal to the first mark.
• Measure the circumference of the thigh muscles at the level of the second mark.
• Vastus medialis is the first muscle to undergo wasting in chronic knee conditions.
• Compare this by repeating the same on the other leg.• Significant when there is >2cms of difference between both
legs.

Lymph nodes• Knee joint drains into the popliteal group of lymph nodes
and finally into the deep inguinal lymph nodes.• Examine this in the Popliteal fossa• Usually popliteal fossa is difficult to palpate,so check for
the deep inguinal group of lymph nodes also.

Stability Tests of the Knee

Valgus/Abduction Stress Test• Done to detect the tears in the Medial collateral ligament.• Patient is made to lie in supine position and the knee extended fully.• Use one hand as a fulcrum on the lateral aspect of the knee joint
and the hand at the ankle joint.• Apply abduction force on the knee joint which if positive results in
joint space opening up.• If no abnormality is detected with knee extended,flex the knee upto
20-30 deg which relaxes the capsule and repeat the same procedure.
• Hughston et al found that valgus test positive at 30 deg of flexion and negative at 0 deg indicates tear limited to the medial compartment ligaments(MCL with or without the posterior capsule),where as positive at 0 deg indicates tear of both MCL and PCL.

Varus/Adduction Stress Test• Done to detect the tear in the lateral collateral ligament.• With the patient in supine position keep one hand on the medial
aspect of the knee joint and one hand over the ankle.• Start with the knee in full extension and later with knee in 20-30
deg of flexion.• Apply varus force to the knee joint.• Marshall et al found that the test positive only in flexion indicates
tear of the LCL,whereas positive in full extension indicates combined injury to the LCL,popliteus and cruciate ligaments.

Tests for the Anterior Cruciate Ligament Injuries
ANTERIOR DRAWER TEST• The patient is made to lie in supine position and knee flexed to
90 deg,with the foot pointing straight forward and the examiner stabilizing the foot by sitting on it.
• Grasp the leg firmly with thumbs on the tibial tubercle.• Check whether the hamstrings are relaxed.• Jerk the leg anteriorly.• Significant displacement of 6-8 mm confirms the anterior
instability.• In tears the end point is usually softer compared to the firm
endpoint in intact ligament.• When the displacement is marked(>1.5 cm)then we can
suspect the tear in the medial ligament and medial capsule.

Lachman’s Tests• There are three types.• 1.Manipulative Lachman.• 2.The Prone Lachman(Feagin and Cooke’s
Modification).• 3.Active Lachman.

• Manipulative Lachman-in this with the patient is in supine position the knee
is flexed to 15-20 deg .• One hand stabilizes the femur whilst the other lifts the tibia upwards,with
the positive test being the tibia displaced anteriorly with a spongy end point.• The Prone Lachman test(Feagin and Cooke)-useful in patients having fat
thighs.• In this the patient is made to lie in prone position and the tibia is held with
both hands placiing the index and thumbs in the joint line.• Flex the knee upto 20 deg and attempt to push the tibia forwards.• The test is positive with the anterior translation the tibia.• The Active Lachman-the patient in prone position with the knee flexed at 30
deg and suppported underneath.• The patient is asked to extend the knee.• If the test is positive there will be anterior subluxation of the lateral tibial
condyles as the quadriceps contracts and the posterior subluxation as the muscle relaxes.

Tests for the Posterior Cruciate Ligament Injuries.
1.The Godfrey’s Posterior Sag test• In this the patient in supine position and the hips and
knees flexed to 90 deg and supported at the ankles.• In case of the PCL injuries the there will be posterior
subluxation of the tibia in the line of gravity.2. The Posterior Drawer test.If the PCL is lax or torn and if the tibia has not subluxed then backward pressure causes tibial subluxation posteriorly.

Tests for Anterolateral Rotatory Instability Slocum’s Anterior Rotatory Drawer Test.• This is a modification of the Anterior drawer test.• The patient is in Supine position and the knee flexed to 90
deg.• Keep the foot in 30 deg of internal rotation and perform
the anterior drawer test.• The test is positive if there is anterior subluxation of the
lateral tibial condyle.

Lateral Pivot Shift test of Macintosh.• It is used to detect the anterior subluxation of the lateral tibial
condyle.• The patient in supine position.• Fully extend the knee with foot in internal rotation.• Apply a valgus stress.• In this position if there is instability the tibia is in subluxed
position.• As the knee is flexed past the 30 deg the iliotibial band passes
posterior to the center of rotation of the knee and provides a force that reduces the lateral tibial plateau on the lateral femoral condyle.
• An isolated tear of the anterior cruciate ligament produces only minimal subluxation,whereas greater subluxation indicates lateral complex or semimembranosus deficiency.

Losee Pivot Shift Test.• The patient should be completely relaxed in supine
position. And the knee in partial flexion.• Apply a valgus force to the knee and at the same time
pushing the fibular head anteriorly.• Now extend the knee fully and the test is positive if a
clunk occurs as the lateral tibial condyle subluxes forward,if there is rotatory instability.

Jerk test of Hughston and Losee• With the patient in supine position knee is flexed to 90 deg
with the tibia in internal rotation.• The knee is then gradually extended with the valgus stress
applied.• The test is positive if the lateral tibia subluxes anteriorly in the
form of sudden jerk at about 30 deg of flexion.

Tests for Anteromedial Rotatory insability
Slocum’s Anterior Rotatory Drawer Test• In this the patient is in supine position and the knee flexed
to 90 deg.• With the foot in 15 deg of external rotation perform the
anterior drawer test.• Excessive excursion of the medial tibial condyle suggests
positive test.

Tests for Posterolateral Rotatory Instability
The Hughston’s Posterolateral Drawer test.• With the patient in supine position the knee is flexed to
little less than 90 deg and the foot in external rotation.• Apply backward pressure on the tibia.• Excessive travel on the lateral side is indicative of
posterolateral instability(posterior cruciate and lateral complex).

External Rotation Recurvatum Test.• The patient is in supine position.• The examiner stands at the end of the couch.• Now lift the legs holding the great toes on both sides.• The test is positive if knee falls into external rotation,varus and
recurvatum.

Reverse pivot shift Sign of Jakob,Hassler and Staubli.• With the patient in supine position the knee is flexed to 90
deg and foot externally rotated,which subluxes the tibial condyle posteriorly.
• Now apply a valgus force to the knee and extend the knee fully.
• If the test is positive the posteriorly subluxed tibia reduces at about 20 deg.

Tibial External rotation test or Dial Test.• This test can be done with the patient in supine or prone
position,better with the patient in prone position.• It is done with the knee in both 30 & 90 deg.• Grasp the foot and the degree of external rotation of the foot is
measured relative to the axis of the femur.• It is measured noting the foot thigh angle.In addition the tibial
plateaus are palpated to determine whether the external rotation is caused by lateral tibial plateau moving posteriorly or medial tibial plateau moving anteriorly.
• A 10 deg difference between the two knees is considered positive.• If the test is positive only at 30 deg of knee flexion it indicates
isolated PLC injury.• If the test is positive at both 30 & 90 deg,then it indicates injury to
both PLC and PCL.

Tests for PosteroMedial Rotatory Instability
Hughston’s Posteromedial drawer test.• In this the patient in supine position and the knee flexed to
90 deg.• With the foot in internal rotation apply backward pressure
on the tibia.• Excessive excursion of the medial tibial condyle suggests
positive test.

Special Tests for the Menisci

McMurray’s TestMedial Menisci-Place the thumb and the index finger along the joint line.• Flex the knee fully• Externally rotate the foot.• Abduct the lower leg/Apply a valgus stress to the knee.• Now extend the knee gently.Lateral Menisci-Place the thumb and index finger along the joint line.• Flex the knee fully.• Internally rotate the foot.• Adduct the leg/Apply a Varus force at the knee joint.• Now extend the knee gently.

Apley’s Grinding Test.• It consists of two parts• The Distraction and Compression forces.• With the patient in prone position the knee is flexed to 90 deg
and the anterior thigh is fixed against the examining table.• The foot and leg are then pulled up to distract the joint and
rotated to put rotational strain on the ligaments. When the ligaments are torn this part of the test is painful.
• With the knee in same position the knee,the foot and leg are pushed downwards and rotated while the joint is slowly flexed and extended.This part of the test is positive in meniscal injuries.
• Pain localised to the joint line is usually significant.

Squat Test• The patient is made to squat with the foot in both internal
and external rotation.• Pain in the internally rotated foot suggests injury to the
lateral meniscus.• Pain in the externally rotated foot suggests injury to the
medial meniscus.

Thessaly Test• The examiner supports the knee while holding the
outstretched hands of the patient.• The patient should be taught about the test with the unaffected
knee first.• The patient stands on the affected leg with the knee in 5 deg
of flexion.• He then rotates the knee externally and internally 3 times.• The same procedure is carried out with the knee in 10-20 deg
of flexion.• Pain experienced at the joint line suggests of the meniscal
tears.• The diagnostic accuracy of this test is 94% for the medial
meniscus and 96% for the lateral meniscus.