Embed Size (px)
Citation preview

Applications of Social Network Analysis
Lecture 4: Health Networks
Dharmi Kapadia
PhD Student, Social Statistics

How is health studied in the social sciences?• Broad topic: medical sciences, psychology, sociology, • Physical and mental health – generally studied separately. • What affects your health – individual
physiology, characteristics (age, gender), neighbourhood characteristics
• Poor health and relationship with poverty, health inequalities (Tudor-Hart, 1971; Marmot & Wilkinson, 2005)– Theories of how poor health might spread e.g. obesity
(Christakis & Fowler, 2007) [Elisa will over this next week – see Week 5 outline]
• Separate question of how people go about managing their health and navigating health services and what might be at play here.
• Individualistic and structural aspects – but what about the social network approach?

Methods
• Whole network approach
• Ego-centric approach – tend to be more studies that use this way of collecting data but we have examples of both
• WORKSHOP: What are the advantages and disadvantages of each approach?

Social Ties and Mental Health• Kawachi and Berkman (2001):
– “smaller social networks, fewer social relationships, and lower perceived adequacy of social support have all been linked to depressive symptoms” (p.458)
– Protective effects of networks (Cohen & Wills, 1985)
– BUT networks are not always supportive, they can also be a source of stress, perhaps especially for women.
– What comes first – type of network or the mental health problems? Cross sectional data does often allow us to test for this adequately.
– But can the network be looked at in isolation when considering the impact of it on mental health? What about societal structures?

Romantic and Sexual networks
• Large study in one US high school in midwest, in mid-sized town (n=832). Predominantly White. Taken from Wave I of National Longitudinal Study of Adolescent Health (Add Health). See http://www.cpc.unc.edu/projects/addhealth for details.

Data Collection• Adolescents asked to describe their 3 most
current relationships (and 3 individuals with whom they had a nonromantic sexual relationship). Collected via CASI (Computer Assisted Self-Interviewing) – audio version for sensitive data.
• Most of the relationships were within school (90% +), asked to identify partners from school roster
• This is a whole network approach (as opposed to a sample of ego-centric reports). What is the benefit of this?


Implications/ Applications of Research• One large component (spanning tree) is highly conducive
to disease transmission. Potential for transmitting disease – note: the researchers did not collect data on the infection in the sample.
• Series of tests to check if the structure that is observed in Jefferson High is different than what would be expected by chance i.e. if there was random mixing.
• Highly dense, centralised, large mean geodesic length• So if it not due to random chance, what is going on in
these networks which gives rise to the observed structure? Through use of simulated networks– Homophily: students select partners with similar SES, college
plans, attachment to school, drinking behaviour, IQ, sexual experience
– NON-homophilous on sex and age.

Implications/ Applications of Research• One main finding: absence of cycles of 4
• Seems to be taboo to date your old partner’s current partner’s old partner. Would the researchers have been able to ascertain this simply by asking the students?
• Generalisability of findings – might not hold in adult populations where relationships are not carried out in such closed networks and under scrutiny.
• What do we do with this research? Does it matter that the sexual health of these adolescents was not collected?
• Sexual health education is not simply about targeting the students with the greatest number of partners. For a tree spanning network, targeting individuals who have fewer links within a larger component could make substantial breaks in the network.

Self-management of health conditions• Previous example did not focus on how people who are actually ill might
utilise/ mobilise/ capitalise on their networks
• Came out of a need to redress balance between individualistic approaches to patients’ management of poor health and wider societal influences.
• Using theoretical construct of illness work (Corbin & Strauss, 1985)• Patients with long term health conditions (diabetes, chronic heart disease
(CHD)) recruited from Greater Manchester between April 2010 - January 2011 (n=300)
• Specific interest in their social network in relation to question:“Who do you think is most important to you in relation to managing your health condition?”
• Mixed methods: qualitative interview nested within a survey

Self-management of health conditions

Methods & Results• Visual method to map ego-network (Kahn & Antonucci, 1980; Pahl and
Spencer, 2004). • Name generator: collect attribute data about each alter as well as the amount
of work (illness, practical and emotional) that the alter is perceived to do by ego. Gives indication of the types of people that are involved in chronic illness management.
• Goes beyond relying on measurement of individual characteristics to explain how people manage their health – deeper explanation of who is involved and how.
• Statistical modelling: multilevel model using network members (alters) nested within ego networks (if interested in this method, see de Miguel Luken & Tranmer, 2010)
• Partners/ spouses, female alters, children who lived nearby, those in frequent contact, living close by – provided more support to patients
• Some structural aspects of networks were predictive of the amount of work that alters did: – More diverse networks provided more emotional support– Networks with higher density provided more illness work
• WORKSHOP: Possible to feed these findings into governmental health policy? What are the advantages/ disadvantages of highlighting that social networks are helpful in managing long term health conditions?

Pets in chronic illness management
• Something a little bit different! But based on the same sample of patients.• Sub analysis of networks where patients had named a pet as being helpful in
the management of their condition. • Mixed methods but focus on the qualitative aspects of the paper• 19% of sample identified a pet as part of their illness management network.

Main themes• Pets, relationships and relatedness
– Patients spoke of pets anthropomorphically– No need to “pay back” pets, normal terms of reciprocity
suspended
• The nature of work undertaken by pets– Emotional support most evident in those networks where
human relationships were absent or viewed negatively
• Pets as mediators of social relationships– Providing opportunity to forge new relationships and
maintaining existing relationships. Go-betweens facilitating interactions with “familiar strangers”
• If data had not been collected within a network perspective overall, would not have been able to examine the role of pets (this was not asked as a survey question, independently of the network map).

The role of social networks in accessing mental health services
• Network Episode Model - Pescosolido (1992, 1998a, 1998b)– “…social interaction is the basis of social life, and social networks provide the
mechanism (interaction) through which individuals learn about, come to understand, and attempt to handle difficulties. This approach shifts the focus from individual ‘choice’ to socially constructed patterns of decisions, including consultation with others” (1992: p1096)
– “interaction in social networks form the principal mechanism through which individuals recognize health problems, contact health facilities, and comply with medical advice” (1998a: p1057)
• Choices about seeking mental health care come from the social world in which the individual is embedded – resorting to a member of one’s social network can be a decision or action in itself. Further, people do not turn to their network just for advice on help-seeking, they are carers and advisors themselves.
• Gourash (1983): 4 ways in which a network could work in relation to help seeking for mental health services
1. Buffer stress, thereby reducing the need to use MH services2. Provide emotional support when unwell3. Refer to services4. Transmit values and attitudes relating to services

Research Findings• In this field there have been mixed findings: smaller networks AND
larger networks relate to being more likely to access mental health services. Much of this research has been with samples of patients with more severe mental illnesses (schizophrenia, bipolar disorder)
• Where the advice comes from also might have a role in shaping whether someone accesses mental health services (Horwitz, 1978): Friends are more likely than relatives to suggest seeking help from professionals. But perhaps relative are providing the required support (cf. Albizu-Garcia et al., 2001- people who had more relatives to rely on/ speak to, less likely to use mental health services.
• Considerable stigma attached to seeking help for mental health problems (cf. Thornicroft, 2006)– probably more than for most physical health problems (but not all e.g. HIV). – WORKSHOP: Across different ethnic groups, cultures, ages, sexes, stigma
could be worse – where does this stigma come from? The social network? Another example of the negative effect of networks?

My PhD• Research Questions
– How do social networks influence usage of mental health services for Pakistani women?
– How does this association differ between Pakistani women and women from other ethnic groups?
• English survey data: Ethnic Minority Psychiatric Illness Rates in the Community (EMPIRIC, 2000)
• N=4281 (2340 females, 387 Pakistani ethnic group)
• 6 ethnic groups: White, Irish, Black Caribbean, Bangladeshi, Indian and Pakistani

Data: Social Network Variables1. Number of close people
2. Relatives
i. Regular contact (Yes/No)
ii. Frequency of contact (5 options)
iii. Frequency of face to face contact (5 options)
iv. Number seen once a month or more
3. Friends
i. 4 categories as above
4. Relationship type of 2 nominated closest people (3 categories: partner/spouse, friend and relative)
(cont…)

Data: Social Network Variables“Thinking about the person that you are closest to, please say how you would rate the practical and
emotional support they have provided to you in the last 12 months. How much in the last 12 months…”
Options: 1: Not at all, 2: A little, 3: Quite a lot, 4: A great deal.
a …did this person give you information, suggestions and guidance that you found helpful?
b …could you rely on this person? Was this person there when you needed them?
c …did this person make you feel good about yourself?
d …did you share interests, hobbies and fun with this person?
e …did this person give you worries, problems and stress?
f …did you want to confide in, talk frankly or share feelings with this person?
g …did you confide in this person?
h …did you trust this person with your most personal worries and problems?
i …would you have liked to have confided more in this person?
j …did talking to this person make things worse?
k …did he/she talk about his/her personal worries with you?
l
…did you need practical help from this person with major things, for example looking after you when ill,
help with finances, children?
m …did this person give you practical help with major things?
n …would you have liked more practical help with major things from this person?
o
…did this person give you practical help with small things when you needed it, for example, chores,
shopping, watering plants etc. ?

.05
.1.1
5.2
P (
usin
g a
MH
se
rvic
e)
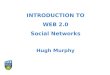
0 1 2 3 4 5 6 7 8 9 10 11 12Negative aspects of support
White Irish
Black Caribbean Bangladeshi
Indian Pakistani
Mental health service use by negative aspects of support

Next week
• Remember to hand in 2 sided essay plan. Printed hard copy and references should be included

References• Albizu-Garcia, C. E., Alegría, M., Freeman, D., & Vera, M. (2001). Gender and health
services use for a mental health problem. Social Science & Medicine, 53(7), 865–78.• Bearman, P. S., Moody, J., & Stovel, K. (2004). Chains of Affection: The Structure of
Adolescent Romantic & Sexual Networks. American Journal of Sociology, 110 (1), 44-91.• Brooks, H. L., Rogers, A., Kapadia, D., Pilgrim, J., Reeves, D., & Vassilev, I. (2012).
Creature comforts: personal communities, pets and the work of managing a long-term condition. Chronic illness, 9(2), 87-102. doi:10.1177/1742395312452620
• Cohen, S., & Wills, T. A. (1985). Stress, social support and the buffering hypothesis. Psychological Bulletin, 98, 310-357.
• Corbin, J. & Strauss, A. (1985). Managing chronic illness at home: three lines of work. Qualitative Sociology, 8, 224-247.
• de Miguel Luken, V. & Tranmer, M. (2010). Personal Support Networks of Immigrants to Spain: a Multilevel Analysis. Social Networks, 32(4), 253-262.
• Gourash, N. (1978). Help-Seeking: A Review of the Literature. American Journal of Community Psychology, 6(5), 413-423.
• Horwitz, A. (1978). Family, kin, and friend networks in psychiatric help-seeking. Social Science & Medicine, 12, 297–304.
• Kahn, R. L. & Antonucci, T. C. (1980). Convoys over the life course: Attachment, roles, and social support. In P.B. Baltes & O. Brim (Eds.) Life-span development and behavior (Vol. 3, pp. 253-268). New York: Academic Press

References (cont.)• Kawachi, I. & Berkman, L. F. (2001). Social Ties and Mental Health. Journal of Urban Health,
78(3), 458-467.• Marmot, M., & Wilkinson, R. (2005). Social determinants of health. Oxford: Oxford University
Press. • Pahl, R. & Spencer, L. (2004). Personal Communities: Not Simply Families of ‘Fate’ or ‘Choice’.
Current Sociology, 52(2), 199-221. • Pescosolido, B. A., Wright, E. R., Alegría, M., & Vera, M. (1998a). Social Networks and
Patterns of Use Among the Poor with Social Networks Mental Health Problems in Puerto Rico. Medical Care, 36(7), 1057-1072.
• Pescosolido, B. A., Gardner, C. B., & Lubell, K. M. (1998b). How people get into mental health services: Stories of choice, coercion and “muddling through” from “first-timers.” Social Science & Medicine, 46(2), 275-286.
• Pescosolido, B. A. (1992). Beyond Rational Choice: The Social Dynamics of How People Seek Help. American Journal of Sociology, 97(4), 1096-1138.
• Thornicroft, G. (2006). Shunned: Discrimination against People with Mental Illness. Oxford: Oxford University Press.
• Tudor Hart, J. (1971). The Inverse Care Law. The Lancet, 297(7696), 405-412.• Vassilev, I., Rogers, A., Blickem, C., Brooks, H., Kapadia, D., Kennedy, A., Sanders, C., et al.
(2013). Social networks, the “work” and work force of chronic illness self-management: a survey analysis of personal communities. PloS One, 8(4), e59723. doi:10.1371/journal.pone.0059723