Embed Size (px)
Citation preview
Dr. Hani Alrefai 04/11/2014

Dr. Hani Alrefai18/11/2014
Dr. Hani Alrefai 04/11/2014
Importance of pentose shunt Importance of uronic acid pathwayHormonal regulation of blood glucose level Causes of hypergylcemia Types of DMMetabolic changes of DM Complications of DMDiagnosis of DM
Importance of pentose shunt Importance of uronic acid pathwayHormonal regulation of blood glucose level Causes of hypergylcemia Types of DMMetabolic changes of DM Complications of DMDiagnosis of DM
Dr. Hani Alrefai 04/11/2014
Def..:It is a pathway by which glucose is converted to
pentose phosphate with production of twomolecules of NADPH.H+.
Site:Occurs in cytoplasm of many tissues include liver,
adipose tissues, adrenals, ovaries, testis, redcells and retina.
Def..:It is a pathway by which glucose is converted to
pentose phosphate with production of twomolecules of NADPH.H+.
Site:Occurs in cytoplasm of many tissues include liver,
adipose tissues, adrenals, ovaries, testis, redcells and retina.
Dr. Hani Alrefai 04/11/2014
I- HMP can account for complete oxidation ofglucose and giving 12 molecules of NADPHA- Reduction of oxidised glutathioneB- Synthesis of : FA, Cholesterol and sphingolipidsC- Activation of folic acid
II- It provides the body with ribose-5-phosphate: Synthesis of nucleotides and nucleic acids. Synthesis of co-enzymes, NAD and FAD
I- HMP can account for complete oxidation ofglucose and giving 12 molecules of NADPHA- Reduction of oxidised glutathioneB- Synthesis of : FA, Cholesterol and sphingolipidsC- Activation of folic acid
II- It provides the body with ribose-5-phosphate: Synthesis of nucleotides and nucleic acids. Synthesis of co-enzymes, NAD and FAD
Dr. Hani Alrefai 04/11/2014

Due to genetic deficiency of glucose-6-phosphate dehydrogenase (G6PD); the redblood cell capacity to protect itself fromoxidative damage is markedly decreased (dueto decreased concentration of NADPH).
Administration of certain drugs (premaquine,aspirin or sulfonamides), which stimulate theproduction of H202 or eating Fava beans(contain oxidizing agents) produce lysis ofthe fragile red cells.
The only treatment is to avoid the abovefactors and by blood transfusion during theattack of haemolysis.
Due to genetic deficiency of glucose-6-phosphate dehydrogenase (G6PD); the redblood cell capacity to protect itself fromoxidative damage is markedly decreased (dueto decreased concentration of NADPH).
Administration of certain drugs (premaquine,aspirin or sulfonamides), which stimulate theproduction of H202 or eating Fava beans(contain oxidizing agents) produce lysis ofthe fragile red cells.
The only treatment is to avoid the abovefactors and by blood transfusion during theattack of haemolysis.
Dr. Hani Alrefai 04/11/2014
Definition: It is an alternative pathway forglucose oxidation resulting in production ofglucuronic acid.
Site: It occurs mainly in the cytosol of livercells.
Importance: production of UDP-Glucuronic a Biosynthesis of mucupolysaccharides Detoxication of : - Steroids
- Drugs- Bilirubin
Definition: It is an alternative pathway forglucose oxidation resulting in production ofglucuronic acid.
Site: It occurs mainly in the cytosol of livercells.
Importance: production of UDP-Glucuronic a Biosynthesis of mucupolysaccharides Detoxication of : - Steroids
- Drugs- Bilirubin
Dr. Hani Alrefai 04/11/2014
Insulin
Glucagon
AdrenalinGlucocorticoids
GHThyroid hormones
Dr. Hani Alrefai 04/11/2014

A. Insulin:leads to decrease of blood glucose level ↓↓Gluconeogenesis ↑↑ Glucose entrance to the cells and oxidation. ↑↑glycogenesis (ms. & liver)---↓↓Glycogenolysis ↑↑ Lipogenesis ----------------------↓↓ lipolysis ↑↑ Protein synthesis ↓↓Ketogenesis
A. Insulin:leads to decrease of blood glucose level ↓↓Gluconeogenesis ↑↑ Glucose entrance to the cells and oxidation. ↑↑glycogenesis (ms. & liver)---↓↓Glycogenolysis ↑↑ Lipogenesis ----------------------↓↓ lipolysis ↑↑ Protein synthesis ↓↓Ketogenesis
Dr. Hani Alrefai 04/11/2014
B. Glucagon: ↑↑Gluconeogenesis(in the liver only) ↑↑Glycogenolysis ----------------↓↓glycogenesis
C. Adrenaline: ↑↑Gluconeogenesis ↑↑Glycogenolysis ----------------↓↓glycogenesis ↓↓ Insulin secretion.
E. Growth hormone: ↓↓ Glucose uptake by the tissues. ↑↑ Lipolysis which ↑↑ FFA leading to ↓↓ glucose utilization
(glucose sparing effect)D. Glucocorticoids: ↑↑ Gluconeogenesis Facilitate the action of glucagons, adrenaline and
growth H.
B. Glucagon: ↑↑Gluconeogenesis(in the liver only) ↑↑Glycogenolysis ----------------↓↓glycogenesis
C. Adrenaline: ↑↑Gluconeogenesis ↑↑Glycogenolysis ----------------↓↓glycogenesis ↓↓ Insulin secretion.
E. Growth hormone: ↓↓ Glucose uptake by the tissues. ↑↑ Lipolysis which ↑↑ FFA leading to ↓↓ glucose utilization
(glucose sparing effect)D. Glucocorticoids: ↑↑ Gluconeogenesis Facilitate the action of glucagons, adrenaline and
growth H.
Dr. Hani Alrefai 04/11/2014
Def.It is the rise of blood glucose level above the normal level.
Causes Deficiency of insulin: Diabetes mellitus. Pancreatictomy (total or subtotal).
Increase of anti-insulin hormones: Adrenaline as in emotion or in case of pheochromocytoma Glucocorticoids as in adrenal tumors and Cushing syndrome. Thyroxin as in hyperthyroidism. Pituitary growth hormone as in acromegally.
Alimentary causes:It is due to increased rate of glucose absorption as in case of
gastrectomy.
Def.It is the rise of blood glucose level above the normal level.
Causes Deficiency of insulin: Diabetes mellitus. Pancreatictomy (total or subtotal).
Increase of anti-insulin hormones: Adrenaline as in emotion or in case of pheochromocytoma Glucocorticoids as in adrenal tumors and Cushing syndrome. Thyroxin as in hyperthyroidism. Pituitary growth hormone as in acromegally.
Alimentary causes:It is due to increased rate of glucose absorption as in case of
gastrectomy.
Dr. Hani Alrefai 04/11/2014

Def:It is a state of chronic hyperglycemia due to
disturbances in carbohydrate Lipid and proteinmetabolism.
Types: Primary Type I (insulin dependent diabetes mellitus or IDDM) Type II (non-insulin dependent diabetes mellitus or
NIDDM) Secondary Adrenaline in case of pheochromocytoma Glucocorticoids as in adrenal tumors and Cushing
syndrome. Thyroxin as in hyperthyroidism. Pituitary growth hormone as in acromegally.
Def:It is a state of chronic hyperglycemia due to
disturbances in carbohydrate Lipid and proteinmetabolism.
Types: Primary Type I (insulin dependent diabetes mellitus or IDDM) Type II (non-insulin dependent diabetes mellitus or
NIDDM) Secondary Adrenaline in case of pheochromocytoma Glucocorticoids as in adrenal tumors and Cushing
syndrome. Thyroxin as in hyperthyroidism. Pituitary growth hormone as in acromegally.
Dr. Hani Alrefai 04/11/2014
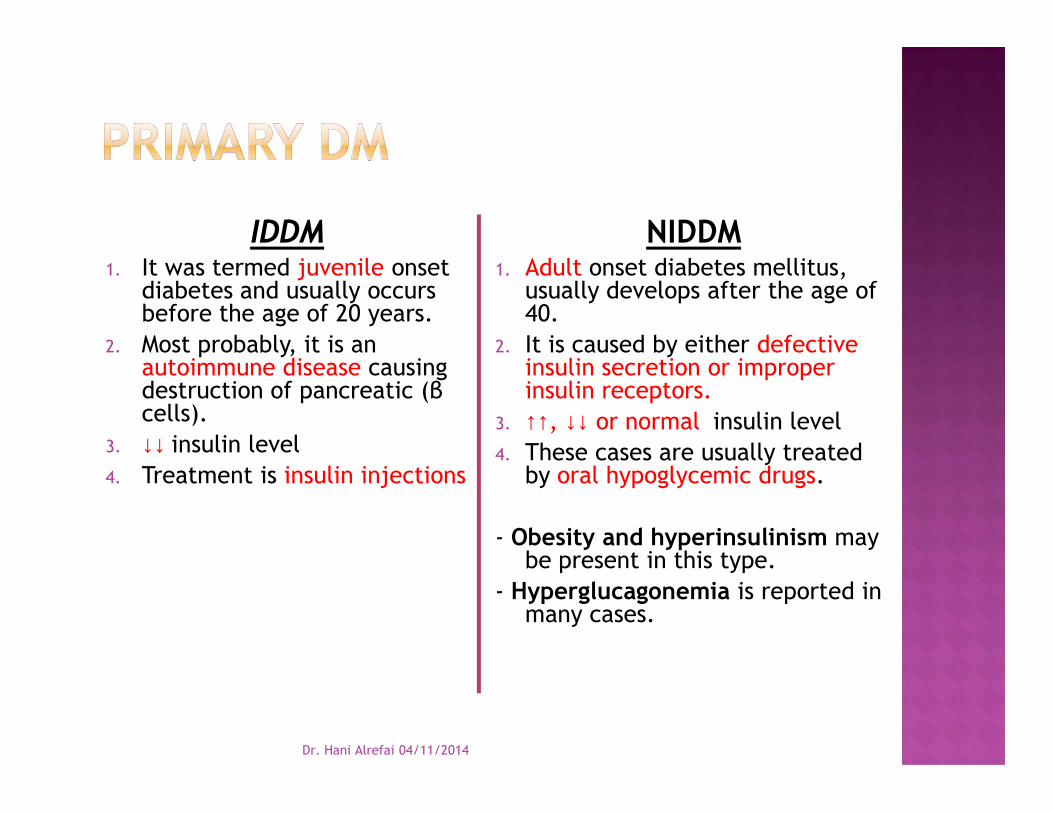
IDDM1. It was termed juvenile onset
diabetes and usually occursbefore the age of 20 years.
2. Most probably, it is anautoimmune disease causingdestruction of pancreatic (βcells).
3. ↓↓ insulin level4. Treatment is insulin injections
NIDDM1. Adult onset diabetes mellitus,
usually develops after the age of40.
2. It is caused by either defectiveinsulin secretion or improperinsulin receptors.
3. ↑↑, ↓↓ or normal insulin level4. These cases are usually treated
by oral hypoglycemic drugs.
- Obesity and hyperinsulinism maybe present in this type.
- Hyperglucagonemia is reported inmany cases.
IDDM1. It was termed juvenile onset
diabetes and usually occursbefore the age of 20 years.
2. Most probably, it is anautoimmune disease causingdestruction of pancreatic (βcells).
3. ↓↓ insulin level4. Treatment is insulin injections
NIDDM1. Adult onset diabetes mellitus,
usually develops after the age of40.
2. It is caused by either defectiveinsulin secretion or improperinsulin receptors.
3. ↑↑, ↓↓ or normal insulin level4. These cases are usually treated
by oral hypoglycemic drugs.
- Obesity and hyperinsulinism maybe present in this type.
- Hyperglucagonemia is reported inmany cases.
Dr. Hani Alrefai 04/11/2014

1- Hyperglycemia (hyperglycemia is ↑ ↑ bl.glucose morethan 180 mg/dL). it is due to:- ↓↓ glucose utilization by different tissues.- ↓↓ rate of glucose transport to certain tissues as muscles
and adipose tissues.- ↓↓ glycogenesis-↑↑ gluconeogenesis.
2- Glucosuria, polyuria, polydepsia and polyphagia.-↑ glucose loss in urine --> ↑ sp. gravity of urine --> ↑ urine
excretion-Polyurea is associated with loss of H2O soluble vitamins
as well as electrolytes as K+, Na+.3- ↑ rate of catabolism of triglycerides with
mobilization of free fatty acids from adipose tissues --> loss of weight.
1- Hyperglycemia (hyperglycemia is ↑ ↑ bl.glucose morethan 180 mg/dL). it is due to:- ↓↓ glucose utilization by different tissues.- ↓↓ rate of glucose transport to certain tissues as muscles
and adipose tissues.- ↓↓ glycogenesis-↑↑ gluconeogenesis.
2- Glucosuria, polyuria, polydepsia and polyphagia.-↑ glucose loss in urine --> ↑ sp. gravity of urine --> ↑ urine
excretion-Polyurea is associated with loss of H2O soluble vitamins
as well as electrolytes as K+, Na+.3- ↑ rate of catabolism of triglycerides with
mobilization of free fatty acids from adipose tissues --> loss of weight.
Dr. Hani Alrefai 04/11/2014
4- ↑↑ fatty acids oxidation --> ↑ ketone bodies formation -*ketonemia and ketonurea with acidosis.
5- ↑↑ protein catabolism --> muscle wasting.6- ↓↓ protein synthesis --> ↓↓ antibodies formation --> the
patients liable for infections and poor wound healing.7- A number of tissues don't require insulin for the entry of
glucose into cells --> hence the intracellular glucose ofthe tissues attains a level similar to that of blood, thenexcess glucose can be reduced to sorbital byaldose'reductase and part of it is oxidized to fructose bysorbital dehydrogenase. Large amounts of sorbitol andfructose inside the cells will causing hypertonicity andwater retention.
These are associated with pathological complication of D.M.as cataract, neuropathy, nephropathy and retinopathy.
4- ↑↑ fatty acids oxidation --> ↑ ketone bodies formation -*ketonemia and ketonurea with acidosis.
5- ↑↑ protein catabolism --> muscle wasting.6- ↓↓ protein synthesis --> ↓↓ antibodies formation --> the
patients liable for infections and poor wound healing.7- A number of tissues don't require insulin for the entry of
glucose into cells --> hence the intracellular glucose ofthe tissues attains a level similar to that of blood, thenexcess glucose can be reduced to sorbital byaldose'reductase and part of it is oxidized to fructose bysorbital dehydrogenase. Large amounts of sorbitol andfructose inside the cells will causing hypertonicity andwater retention.
These are associated with pathological complication of D.M.as cataract, neuropathy, nephropathy and retinopathy.
Dr. Hani Alrefai 04/11/2014

1-The glucose tolerance test2- Glycated haemoglobin3- Glycated plasma proteins4- Microalbuminuria
1-The glucose tolerance test2- Glycated haemoglobin3- Glycated plasma proteins4- Microalbuminuria
Dr. Hani Alrefai 04/11/2014
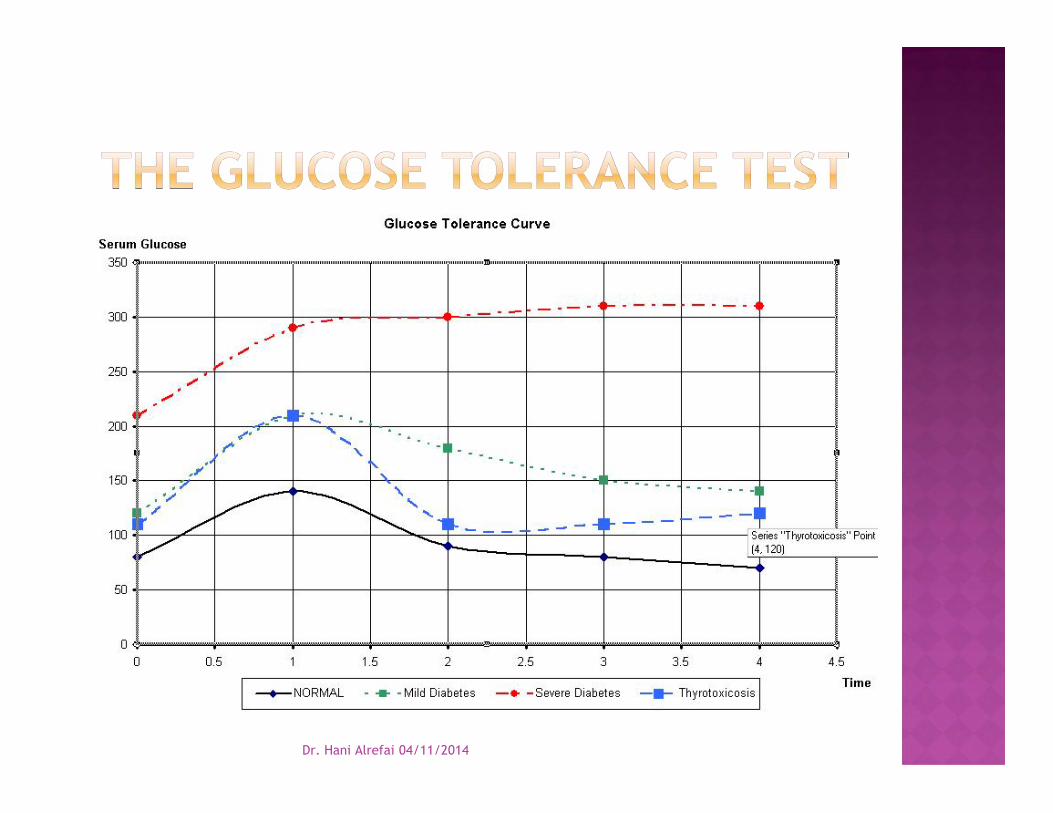
Rational of test Performance of the test Results and interpretation
Rational of test Performance of the test Results and interpretation
Dr. Hani Alrefai 04/11/2014
Dr. Hani Alrefai 04/11/2014
1. Diabetic nephropathy.2. Diabetic neuropathy.3. Diabetic retinopathy.4. Cataract5. Peripheral vascular disease.
1. Diabetic nephropathy.2. Diabetic neuropathy.3. Diabetic retinopathy.4. Cataract5. Peripheral vascular disease.
Dr. Hani Alrefai 04/11/2014
Microvasculopathy
Osmoticpressure

Dr. Hani Alrefai 04/11/2014





























