Embed Size (px)
Citation preview

GENERAL PATHOLOGYGENERAL PATHOLOGY
DR NADEEM REYAZ
UNIVERSITY OF HEALTH SCIENCES

Where there is love of medicine,
there is love of
humankind

PATHOLOGYPATHOLOGY
is the scientific study of disease or is is the scientific study of disease or is the study of structural and functional the study of structural and functional abnormalities that are expressed as abnormalities that are expressed as
diseases of organ and systemdiseases of organ and system

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
Literally means how physiology is altered by disease

PATHOGENESISPATHOGENESIS
• of a disease is the sequence of events at the organ, cellular, ultrastructural, and molecular levels, by which the disease develops

PERSPECTIVE PATHOLOGYPERSPECTIVE PATHOLOGY
• is the study of cell injury and the expression of a preexisting capacity to adapt to such injury on the part of the either injured or intact cell

•WHAT HURTS CELLS?

HYPOXIAHYPOXIA
loss of the ability to carry on sufficient aerobic oxidative respiration, is the most common cause of cell injury and death. It
is still the prototype

CAUSES OF HYPOXIACAUSES OF HYPOXIA
• ISCHAEMIA• HYPOXAEMIA• FAILURE OF THE CYTOCHROMES• POOR NUTRITION• INFECTIOUS AGENT• IMMUNE INJURY• CHEMICAL AGENTS• PHYSICAL AGENTS

• Ischemia ("ischemic hypoxia"; "stagnant hypoxia"): Loss of arterial blood flow (* literally, "holding back the blood")
• Local causes – Occlusion of the arteries that bring in fresh blood – Occlusion of the veins which allow blood to leave, so
that fresh blood can flow in – Shunting of arterial blood elsewhere ("steal
syndromes"; "Robin Hood" syndromes)
• Systemic causes – Failure of the heart to pump enough blood

Hypoxemia: Too little available oxygen in the blood
Oxygen problems ("hypoxic hypoxia") Too little oxygen in the air Failure to properly ventilate the lungs Failure of the lungs to properly oxygenate the blood Failure of the heart to pump enough blood through the lungs Tremendously increased dead space (i.e., pulmonary thromboembolus)
Hemoglobin problems ("anemic hypoxia") Inadequate circulating red cell mass ("anemia") Inability of hemoglobin to carry the oxygen (carbon monoxide poisoning, methemoglobinemia) "High affinity" hemoglobins that will not give up their oxygen to the tissues

Failure of the cytochromes ("histotoxic hypoxia")
•Cyanide poisoning
•Dinitrophenol poisoning
•Other curious poisons

POOR NUTRITION
INFECTIOUS AGENT eg, Clostridia
IMMUNE INJURY eg, Antibody and T cell mediated
CHEMICAL AGENTS eg, salts, overwater,
PHYSICAL AGENTS eg, fire, freezing, electricity, radiation

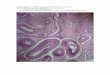
ATROPHYATROPHY
• clinically atrophy is explained as diminution in the size or function of an
organ or decrease in cell size


Here is the centrilobular portion of liver next to a central vein. The cells have reduced in size or been lost from hypoxia. The pale brown-yellow pigment is lipochrome that has accumulated
as the atrophic and dying cells undergo autophagocytosis.

HYPERTROPHYHYPERTROPHY
• Increase in the sizes of cells, and hence the size of the organ ultimately increase in the amount of functioning
tissue mass

• HYPERTROPHY may be due to
• Hormonal (physiological) demand
• Increased functional demand

Hypertrophy of the muscles of a strength athlete

Hypertrophy of the Uterus

Hypertrophy of cardiac muscles


HYPERPLASIAHYPERPLASIA
• "An increase in the number of cells in a tissue or organ. It occurs in tissues with cells that are capable of mitotic division "
•




METAPLASIAMETAPLASIA
• "(Adaptive) substitution of one type of adult or fully differentiated cell for another type of adult (or fully differentiated) cell"
• "A reversible change in which one adult cell type replaced by another adult cell type.“
• "Conversion of a differentiated cell type into another".


DYSPLASIADYSPLASIA
• "Bad growth". By convention today, this implies a very abnormal epithelium with "loss of uniformity of the individual cells, as well as a loss of their architectural orientation". This includes "atypical hyperplasia" and "atypical metaplasia" as well as the unfortunately-named newer term "intra-epithelial neoplasia".

• Dysplasia is a precancerous lesion, in the sense that it is a necessary stage in the multi step cellular evaluation to
cancer. It is characterized by deranged cell growth of a specific
tissue

INTRACELLULAR STORAGE INTRACELLULAR STORAGE
• is the retention of material within the cell • Fat• Glycogen• Cholesterol• Abnormal Proteins e.g Lewy bodies,
Neurofibrillary tangles (tan protein), Mallory bodies
• Lipofuscin, Melanin, Exogenous pigments like Tattoos, Iron and other metals

Mallory bodies (the red globular material) composed of cytoskeletal filaments in liver cells

The brown coarsely granular material in macrophages in this alveolus is hemosiderin

These renal tubules contain large amounts of hemosiderin, as demonstrated by the Prussian blue iron stain

NECROSISNECROSIS
• is the gross and light-microscopic appearances that indicate cell death.
• It refers to cell death in an organ or tissue that is still part of a living person

Necrosis with inflammatory cells

Many nuclei have become pyknotic (shrunken and dark) and have then undergone karorrhexis (fragmentation) and karyolysis (dissolution). The cytoplasm and cell borders are not recognizable.

• Autolysis is the dead cell being self-digested by its lysosomal enzymes, while heterolysis is the cell being digested by
the body's living white cells.


TYPES OF NECROSIS TYPES OF NECROSIS
• COAGULATION NECROSIS
• LIQUEFACTIVE NECROSIS
• CASEOUS NECROSIS

COAGULATION NECROSISCOAGULATION NECROSIS
• Death of groups of cells (most often from loss of blood supply), with persistence of their shapes for at least a few days.

• Grossly, the dead area is likely to be soft and pale. After a while, it is likely to shrink (catabolism) and turn yellow (its lipids are freed up to form little micelles, trapping the tryptophan metabolites that impart the yellow color to normal body fat).

• The microscopy is distinctive. After loss of their nuclei, the cytoplasm of the cells remains intact for days. The "tombstones" reveal the structure of the living tissue. If the patient lives, the edges of the necrotic area become inflamed, and eventually the dead cells will be removed by white cells and their noxious proteases. RULE: Unless otherwise specified in this section, the death of a group of cells will result in coagulation necrosis



APOPTOSISAPOPTOSIS
• ("shrinkage necrosis", "single-cell coagulation necrosis", "natural death in
contrast to necrosis") is a distinct reaction pattern which represents programmed
single-cell suicide. Cells actually expend energy in order to die.


• Apoptotic nuclear pyknosis, karyorrhexis, and karyolysis look, morphologically, like what you see in other necrosis. The difference is that apoptosis features individual cells dying off, and a lack of inflammation.

LIQUEFACTIVE NECROSISLIQUEFACTIVE NECROSIS
• (* "colliquative necrosis" in Europe): The result of hydrolysis. When the cells die, they are rapidly destroyed by lysosomal enzymes, either their own or those from neutrophilic leukocytes (i.e., bacterial infections), or clostridia or snake poison. Acid and lye burns represent the extreme of liquefaction.


The two lung abscesses seen here are examples of liquefactive necrosis in which there is a liquid center in an area of tissue injury. One abscess appears in the upper lobe and one in the lower lobe. Liquefactive necrosis is typical of organs in which the tissues have a lot of lipid (such as brain) or when there is an abscess with lots of acute inflammatory cells whose release of proteolytic enzymes destroys the surrounding tissues.

Lung Abscess: Microscopic appearance (Liquefactive Necrosis)

ENZYMATIC FAT NECROSIS ENZYMATIC FAT NECROSIS
• When pancreatic enzymes are released into the body's tissues, they digest them wholesale. Lipase releases free fatty acids (saponification) from the local lipids (membranes, depot triglyceride). This complexes with calcium ions to form salts (calcium stearate, etc.)



CASEOUS NECROSISCASEOUS NECROSIS
• ("cheese" and "casein"): All of the cells in an area die, the tissue architecture is obliterated, and they turn into a crumbly ("friable"), readily-aerosolized powder

• This is characteristic of a poorly-understood subtype of immune injury, and generally it is seen in certain granulomatous diseases, notably tuberculosis and certain fungal infections (coccidioidomycosis, blastomycosis, and histoplasmosis)


Caseous necrosis with granulomatous inflammation

Caseous necrosis with Giant cells

GUMMATOUS NECROSISGUMMATOUS NECROSIS•
• is, for our purposes, coagulation necrosis seen in granulomas in syphilis.

FIBRINOID NECROSISFIBRINOID NECROSIS
• is a time-honored term for damage to of the walls of arteries which allows plasma proteins to seep into, and precipitate in, the media (some pathologists call this "insudation").


NECROBIOSISNECROBIOSIS
• is a curious term for necrosis of fibroblasts within still-intact dense fibrous tissue. It's characteristic of two lesions --
necrobiosis lipoidica and granuloma annulare

CAVITATIONCAVITATION
• results from removal of necrotic material (i.e., draining a huge abscess, coughing up caseous debris in tuberculosis, physiologic removal of debris in a cerebral infarct, etc.)

GANGRENEGANGRENE
• ("gangrenous necrosis") is not a separate kind of necrosis at all, but a term for necrosis that is advanced and visible grossly. The word gangrene comes from the Latin word gangraena, an eating sore. Gangrene is death and decay of a body part

• Gangrene is defined as the gradual destruction of living tissue, due to an obstruction in the supply of blood and oxygen to an area of the body (Pipkin and Janelli, 2000)

TYPES OF GANGRENETYPES OF GANGRENE
• .DRY GANGRENE
• .WET GANGRENE
• .GAS GANGRENE

DRY GANGRENEDRY GANGRENE
• If there's mostly coagulation necrosis, (i.e., the typical blackening, desiccating foot which dried up before the bacteria could overgrow)

• Dry gangrene. This variety is free of infection. It is usually brought on by a blood clot, frostbite, or poor circulation that causes the tissues to become dry and shriveled

“Dry Gangrene”

WET GANGRENEWET GANGRENE
• If there's mostly liquefactive necrosis (i.e., the typical foul-smelling, oozing foot infected with several different kinds of bacteria), or if it's in a wet body cavity

"wet gangrene in patient with Diabetes millitus”

CLOSTRIDIAL GANGRENECLOSTRIDIAL GANGRENE
• (including "gas gangrene"), a dread complication of dirty, blood-deprived wounds. The clostridia digest tissue enzymatically and rapidly, often transforming it into a bubbly soup.

FOURNIER'S GANGRENEFOURNIER'S GANGRENE
• Fournier's gangrene, bacterial gangrene of the scrotum (the dreaded "black sack disease")


PATHOLOGICALPATHOLOGICAL CALCIFICATION CALCIFICATION
deposition of mineral salts of calcium in tissues other than osteoid or enamel

• Dystrophic calcification refers to the macroscopic deposition of calcium salts in in dead or degenerate tissues
• Metastatic calcification reflects deranged calcium metabolism in contrast to dystrophic calcification and is associated with increase serum calcium level

This is dystrophic calcification in the wall of the stomach. At the far left is an artery with calcification in its wall

“Metastatic calcification" in the lung of a patient with a very high serum calcium level (hypercalcemia).

HYALINEHYALINE
• is a term that refers to any material that exhibits a reddish, homogenous appearance when stain with H&E. It stand for describing diverse and unrelated lesions.

REVERSIBLE CELL INJURYREVERSIBLE CELL INJURY
• It occurs when environmental changes exceed the capacity of the cell to maintain normal hemostasis. If the stress is removed in tissue or if the cell withstand the assult the injury is reversible

IRREVERSIBLE CELL INJURYIRREVERSIBLE CELL INJURY
• If the stress remains the severe, the cell injury becomes irreversible and lead to cell death


FREE RADICALS FREE RADICALS
• A common "final pathway" in a variety of forms of cell injury, including injury brought about by inflammatory cells, is generation of free radicals, i.e., molecular species with a single unpaired electron available in an outer orbital. Single free radicals initiate chain reactions which destroy large numbers of organic molecules

FREE-RADICAL GENERATION FREE-RADICAL GENERATION
• 1. Oxidation of unsaturated fatty acids in membranes ("lipid peroxidation", etc.) * Basic biologists: These are the same reactions that make unsaturated fats turn rancid.
• 2. Cross-linking of sulfhydryl groups of proteins.
• 3. Genetic mutations

• Free radicals may be generated in the following ways:
• 1. By absorbing radiant energy (UV, x-rays; striking water, these generate a hydrogen atom and a hydroxyl radical; when hydrogen peroxide contacts ferrous iron, it is cleaved into two hydroxyl radicals (* the Fenton reaction).
• 2. As part of normal metabolism (for example, xanthine oxidase and the P450 systems generate superoxide; our white cells use free radicals to attack and kill invaders)
• 3. As part of the metabolism of drugs and poisons (the most famous being CCl3.-, from carbon tetrachloride; even O2 in high concentrations generates enough free radicals to gravely injure the lungs).

• The most important free radicals are probably those derived from oxygen, i.e., superoxide (O.-2) and hydroxyl radical (OH.); hydrogen peroxide, though not a free radical, is two hydroxyl radicals joined.

THE END