Embed Size (px)
Citation preview
Effect of PCI on Long-Term Survival in Patients with Stable Ischemic Heart
Disease
PublicationSteven P. Sedlis et alNew England Journal of Medicine November 12,2015
Need for the studyThere is controversy regarding the use of PCI in
patients with stable ischaemic CAD
The COURAGE trial showed no mortality benefit in patients that underwent PCI as compared to medical management in a short follow up of 4.6 years.
Later part of the study period –slight improvement in PCI
The study was done to see if there was any long term mortality benefits for patients with PCI as compared to medical management
Other Studies Bypass Angioplasty Revascularization Investigation 2 Diabetes
(BARI 2D 2009) - 2,368 patients with T2DM and stable CAD randomized to CABG, OMT or OMT and PCI. PCI and only OMT groups did not show any difference.
Frye RL, et al. "A Randomized Trial of Therapies for Type 2 Diabetes and Coronary Artery Disease". The New England Journal of Medicine. 2009. 360(24):2503-2515.
FAME (FFR guided PCI vs. angiography guided PCI) and FAME 2 ( FFR guided PCI vs. OMT) -patients with multivessel CAD, an FFR-guided approach reduces the composite of death, nonfatal MI, and need for repeat/urgent revascularization.
De Bruyne B, et al. "Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease". The New England Journal of Medicine. 2012. 367(11):991-1001.
ISCHEMIA trial (2012-2019, 8000 patients) - Initial invasive strategy of cardiac catheterization followed by optimal revascularization with OMT compared with only OMT. Ongoing.
Study DescriptionMulticenter, open-label, parallel-group,
randomized, controlled trialPermuted block randomization N=2,287 – 1211 patients available for follow up
PCI plus OMT (n=1,149) OMT alone (n=1,138)
Setting: 50 centers in US and Canada Follow up done only in the USEnrollment: June 1999 to January 2004
Inclusion criteriaStable CADCanadian Cardiovascular Society (CCS) class
I,II,III or stabilised class IV angina.> 70% stenosis in at least one coronary
artery.
Objective myocardial ischemia, with any of :Substantial changes in ST segment
depression.T wave inversion on the resting EKG.Inducible ischemia with either exercise or
pharmacologic stress test.80% stenosis with classic angina without
provocative testing.
Exclusion criteriaPersistent CCS class IV anginaA markedly positive stress test (substantial
ST-segment depression or hypotensive response during stage 1 of the Bruce protocol)
Refractory heart failure Cardiogenic shock
Ejection fraction <30%
>50% left main disease
Coronary lesions deemed unsuitable for PCI
Optimal Medical Therapy (OMT)1. Antiplatelet agents – Aspirin 81 to 325 mg per day
or 75 mg of Clopidogrel per day, if aspirin intolerance for all patients. Combination in patients with PCI.
2. Beta blockers – Long acting Metoprolol
3. Calcium channel blockers - Amlodipine
4. Nitrates - ISMN
5. ACE/ ARBs – Lisinopril/ Losartan
6. Lipid level reduction – Simvastatin alone or with Ezetimibe for target level of LDL level of60 to 85 mg per deciliter.
7. Guideline based recommendations for smoking cessation, diet and exercise.
Percutaneous Intervention and OMTTarget-lesion revascularization always attempted and complete revascularization was performed as clinically appropriate.
Angiographic success ;Normal coronary-artery flow with 1. < 50% stenosis after balloon angioplasty, or2. < 20% after coronary stent implantation
Clinical success - angiographic success plus absence of in hospital myocardial infarction, emergency CABG, or death.
Drug-eluting stents were used in only 31 patients.
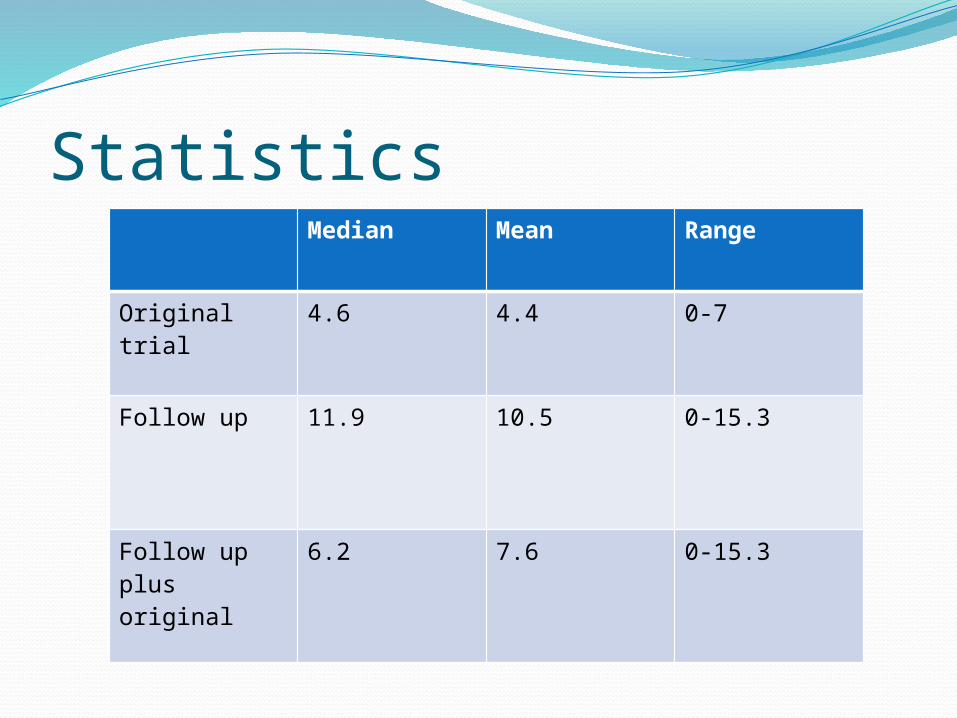
Statistics Median Mean Range
Original trial 4.6 4.4 0-7
Follow up 11.9 10.5 0-15.3
Follow up plus original
6.2 7.6 0-15.3
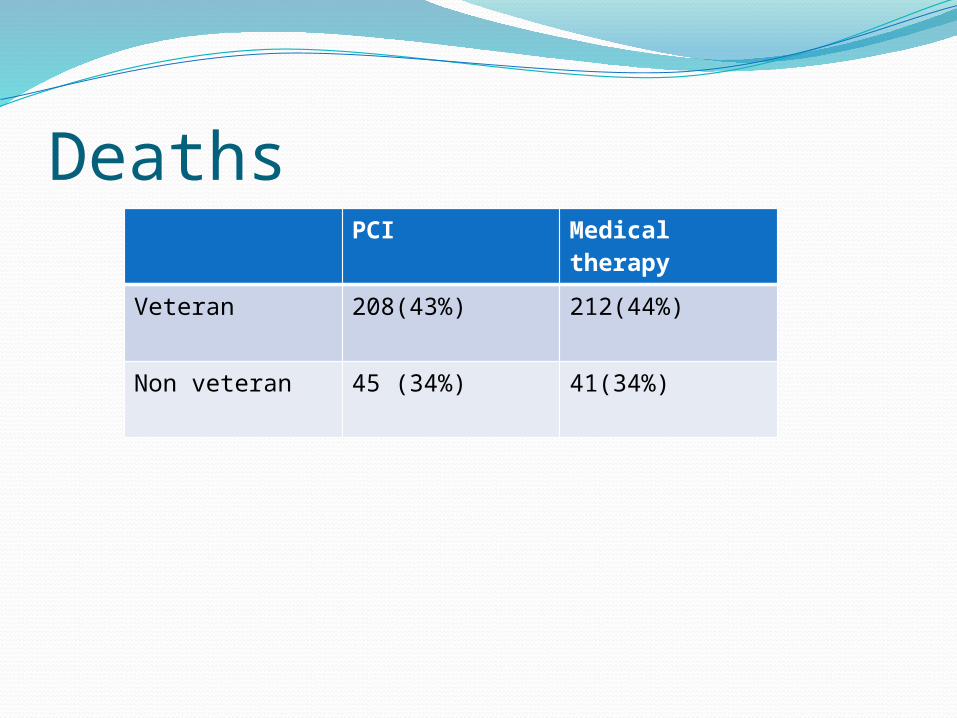
Deaths PCI Medical
therapy
Veteran 208(43%) 212(44%)
Non veteran 45 (34%) 41(34%)
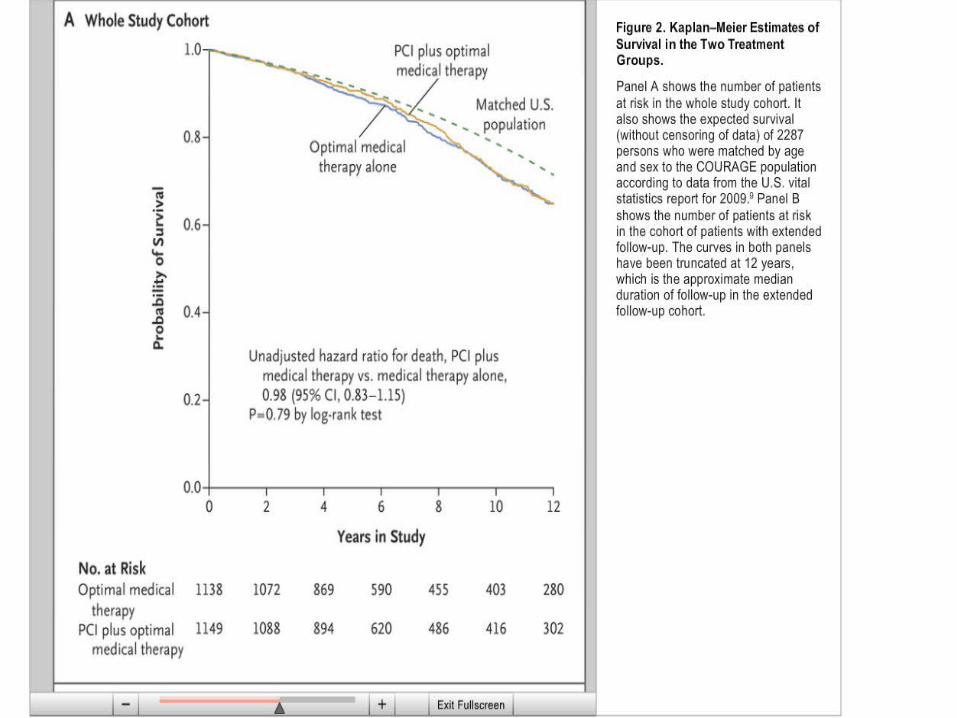
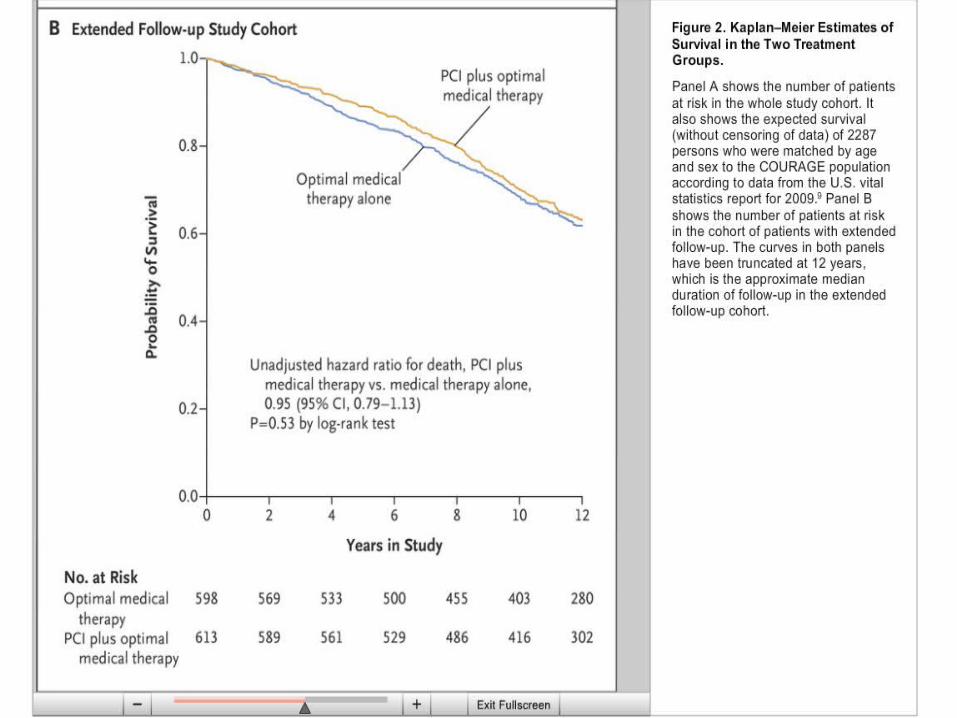
DiscussionAn initial strategy of PCI, as compared with a
strategy of medical therapy alone, was not associated with lower mortality among the patients in the COURAGE trial for whom long-term survival could be ascertained.
LimitationsAlmost one third of the patients (32.6%) in
the COURAGE trial crossed over to coronary revascularization during the original follow-up period of 2.5 to 7 years.
No data on how many patients received subsequent revascularization during the extended follow-up period.
The use of death from any cause as an end point
The evaluated therapies were older.Low percentage of women (15%)Higher percentage of veterans in the follow
up period as compared to the original COURAGE study.





























