Embed Size (px)
DESCRIPTION
for pathophysiology
Citation preview

Fluid, Electrolyte, and Fluid, Electrolyte, and Acid-Base BalanceAcid-Base Balance
11

Body Fluid CompartmentsBody Fluid Compartments60% of average adult60% of average adult’s weight is fluid’s weight is fluid
IntracellularIntracellular 2/3 body water2/3 body water
ExtracellularExtracellular Contains remaining 1/3 of body waterContains remaining 1/3 of body water Fluid outside the cells Fluid outside the cells Interstitial fluid (between cells & outside bld Interstitial fluid (between cells & outside bld
vessels).vessels). Intravascular fluid (plasma w/in vascular system).Intravascular fluid (plasma w/in vascular system). Transcellular fluid (CSF, GI, pleural, synovial and Transcellular fluid (CSF, GI, pleural, synovial and
peritoneal fluid). peritoneal fluid).
22

33

Composition of Body FluidsComposition of Body Fluids
Electrolyte:: An element or compound that, when An element or compound that, when
dissolved or dissociated in water or solvent, dissolved or dissociated in water or solvent, separates into ionsseparates into ions
Ions:: Cations: positively charged (Na+, K+, CaCations: positively charged (Na+, K+, Ca²²+)+) Anions: negatively charged (ClAnions: negatively charged (Clˉ, HCOˉ, HCO33ˉ, ˉ, SOSO44ˉ̄))
44

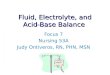
•Osmolality is a measure of the solute concentration per kg in a solution.
•Solute is a substance dissolved in a solvent
•Solvent is a substance that is capable of dissolving a solute (liquid or gas).
•Tonicity is the tension or effect that the osmotic pressure of a solution with impermeable solutes exerts on cell size due to water movement across the cell membrane.
55

66

Tonicity
77

Movement of Body FluidsMovement of Body Fluids
Capillary permeabilityCapillary permeability: the movement of fluid: the movement of fluidcomponents (i.e. electrolytes, glucose, minerals)components (i.e. electrolytes, glucose, minerals)between organs & between cells.between organs & between cells. Movement depends on the ability of the cell Movement depends on the ability of the cell
membrane to allow the passage of fluid components membrane to allow the passage of fluid components with in the vascular system. with in the vascular system.
Occurs because of one of 4 transport mechanisms: Occurs because of one of 4 transport mechanisms: OsmosisOsmosis DiffusionDiffusion FiltrationFiltration Active Transport Active Transport
88

Movement of Body FluidsMovement of Body Fluids
OsmosisOsmosis::Movement of water across a Movement of water across a semipermeable membrane semipermeable membrane from an area of from an area of lesserlesser toto one one of of greatergreater concentration concentration
DiffusionDiffusion::Random movement of a Random movement of a solute through a solute through a semipermeable membrane semipermeable membrane from from higher to lowerhigher to lower concentrationconcentration
Capillary FiltrationCapillary Filtration::Movement of water through Movement of water through capillary pores due to capillary pores due to mechanical forces mechanical forces
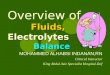
Active transportActive transport::Movement of ions against Movement of ions against their concentration gradient. their concentration gradient. Requires energy Requires energy
99

Osmosis through semipermeable Osmosis through semipermeable membranemembrane
1010

Diffusion across a Diffusion across a semipermeable membranesemipermeable membrane
1111

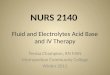
Filtration & Hydrostatic pressureFiltration & Hydrostatic pressure
1212

Active Transport: Active Transport: Na+/K+ PumpNa+/K+ Pump
1313

Hydrostatic Pressure Hydrostatic Pressure
Fluid pushing force inside the capillary Fluid pushing force inside the capillary Inside capillaries hydrostatic pressure and Inside capillaries hydrostatic pressure and
capillary filtration pressure are equalcapillary filtration pressure are equal
1414

Colloidal Osmotic Pressure Colloidal Osmotic Pressure Pulling force created by particles (i.e. plasma Pulling force created by particles (i.e. plasma
proteins) that do not pass through capillary proteins) that do not pass through capillary porespores
Capillary colloidal pressure is greater than Capillary colloidal pressure is greater than interstitial colloidal pressure interstitial colloidal pressure
1515

Lymph Drainage Lymph Drainage
Return of fluids and osmotically active Return of fluids and osmotically active plasma proteins from interstitium into the plasma proteins from interstitium into the lymphatic system to return to circulationlymphatic system to return to circulation
1616

Factors Causing Edema Factors Causing Edema
Increased capillary filtration pressure Increased capillary filtration pressure Decreased capillary colloidal osmotic Decreased capillary colloidal osmotic
pressure pressure Increased capillary permeabilty Increased capillary permeabilty Obstruction of lymph flowObstruction of lymph flow
1717

LymphedemaLymphedema
1818

Regulation of Body FluidsRegulation of Body Fluids
Fluid intakeFluid intake:: Thirst regulates Thirst regulates fluid intakefluid intakeThirst-control Thirst-control center: the center: the hypothalamushypothalamus Intake is about Intake is about 2200 to 2700 2200 to 2700 ml/dayml/day
HormonalHormonal:: Antidiuretic Antidiuretic hormone (ADH)hormone (ADH) Renin-Renin-angiotensin-angiotensin-aldosterone aldosterone mechanismmechanism Atrial natriuretic Atrial natriuretic peptidepeptide
Fluid outputFluid output:: Fluid is lost Fluid is lost through kidneys, through kidneys, skin, lungs, and GI skin, lungs, and GI tracttract Insensible lossInsensible loss
Goal is the maintain Goal is the maintain homeostasishomeostasis!!1919

2020

2121

Regulation of ElectrolytesRegulation of Electrolytes
CationsCations:: Sodium (NaSodium (Na++)) Potassium (KPotassium (K++)) Calcium (CaCalcium (Ca2+2+))
Magnesium (MgMagnesium (Mg2+2+))
AnionsAnions:: Chloride (ClChloride (Cl--)) Bicarbonate (HCOBicarbonate (HCO33
––)) Phosphate (POPhosphate (PO44
33--))
2222

Sodium Sodium Na+: 135-145 mEq/L
- the most abundant cation in ECF
- functions: maintain water balance, nerve
impulse transmission, regulate acid-base
balance, and participate in cellular
chemical reactions.
- regulated by dietary intake & aldosterone
secretion
2323

Antidiuretic Hormone (ADH)Antidiuretic Hormone (ADH)
AKA: vasopressin AKA: vasopressin Levels controlled by ECF volume and Levels controlled by ECF volume and
osmolality osmolality Some conditions favor abnormal Some conditions favor abnormal
increases in ADH increases in ADH ETOH inhibits ADH ETOH inhibits ADH
2424

Diabetes Insipidus (DI) Diabetes Insipidus (DI) ADH deficiency or decreased response to ADH deficiency or decreased response to
ADHADH Excretion of large volumes of urine Excretion of large volumes of urine
Inability to concentrate urineInability to concentrate urine Excessive thirst Excessive thirst
May lead to hypertonic dehydration and May lead to hypertonic dehydration and increased serum osmolality increased serum osmolality
2 types: 2 types: 1.1. Neurogenic (or central) DINeurogenic (or central) DI
2.2. Nephrogenic Nephrogenic 2525

Diabetes Insipidus (DI) Diabetes Insipidus (DI)
Clinical ManifestationsClinical Manifestations PolyuriaPolyuria Intense thirst (fluid intake 2-20 L/day) Intense thirst (fluid intake 2-20 L/day) Hypernatremia & dehydration Hypernatremia & dehydration
2626

Syndrome of Inappropriate Syndrome of Inappropriate Antidiuretic Secretion (SIADH)Antidiuretic Secretion (SIADH)
Failure of negative feedback that regulates Failure of negative feedback that regulates release and inhibition of ADH release and inhibition of ADH
Water retention and dilutional Water retention and dilutional hyponatremia w/ decreased serum osmohyponatremia w/ decreased serum osmo
Causes:Causes: Response to stress Response to stress Chronic conditions: lung tumors & CNS Chronic conditions: lung tumors & CNS
disorders disorders
2727

Syndrome of Inappropriate Syndrome of Inappropriate Antidiuretic Secretion (SIADH)Antidiuretic Secretion (SIADH)
Clinical Manifestations Clinical Manifestations Due to dilutional hyponatremia Due to dilutional hyponatremia ↓ ↓ UOP UOP ↓ ↓ serum osmo serum osmo ECF volume expansion causes: ↓ Hct, serum ECF volume expansion causes: ↓ Hct, serum
Na+, and BUN Na+, and BUN Severity dependent on extent of Na+ Severity dependent on extent of Na+
depletion & water intoxication depletion & water intoxication
2828

HyponatremiaHyponatremiaNa+ < 135 mEq/L Na+ < 135 mEq/L
Causes:
sodium loss (GI, renal,
& skin losses);
pshychogenic
polydipsia; water
intoxication; SIADH
S & SS & S::
N/V, abdominal N/V, abdominal
cramping, edema, cramping, edema,
disorientation,disorientation,
convulsions, coma. convulsions, coma.
2929

HypernatremiaHypernatremiaNa+ > 145mEq/LNa+ > 145mEq/L
CausesCauses::
Excess salt intake, aldosterone secretions, DI, increased sensible & insensible water loss, water deprivation.
S & SS & S::
thirst, dry & flushed thirst, dry & flushed skin, dry & sticky skin, dry & sticky m.m., postural m.m., postural hypotension, fever, hypotension, fever, agitation, decreased agitation, decreased reflexes, convulsions, reflexes, convulsions, restlessness, & restlessness, & irritability. irritability.
3030

Fluid for thought…hmmmFluid for thought…hmmm
If you were walking across the Sahara If you were walking across the Sahara Desert with an empty canteen, the amount Desert with an empty canteen, the amount of ADH secreted would most likely:of ADH secreted would most likely:
a.a. increase. increase.
b.b. decrease. decrease.
c.c. stay the same.stay the same.
3131

Fluid for thought…hmmmFluid for thought…hmmm
AnswerAnswer: A: A
Because your body would probably be Because your body would probably be dehydrated, it would try to retain as much fluid dehydrated, it would try to retain as much fluid as possible. To retain fluid, ADH secretion as possible. To retain fluid, ADH secretion increases. increases.
3232

More fluid for thought…hmmm!More fluid for thought…hmmm! If you placed two containers next to each If you placed two containers next to each
other, separated only by a semipermeable other, separated only by a semipermeable membrane, and the solution in one membrane, and the solution in one container was hypotonic relative to the container was hypotonic relative to the other, fluid in the hypotonic container would: other, fluid in the hypotonic container would:
a.a. move out of the hypotonic container into the move out of the hypotonic container into the other. other.
b.b. pull fluid from the other container into the pull fluid from the other container into the hypotonic container.hypotonic container.
c.c. stay unchanged within the hypotonic stay unchanged within the hypotonic container.container.
3333

More fluid for thought…hmmm!More fluid for thought…hmmm!
Answer:Answer: A A
Fluid would move out of the hypotonic containerFluid would move out of the hypotonic container
into the other container to equalize theinto the other container to equalize the
concentration of fluid within the two containers. concentration of fluid within the two containers.
3434

ScenarioScenario
A man with hypernatremia was severely A man with hypernatremia was severely confusedconfused
Question:Question: The doctor said this was due to a change in the size of his The doctor said this was due to a change in the size of his
brain cells. Why would this happen?brain cells. Why would this happen? A medical student suggested giving him a hypotonic IV. A medical student suggested giving him a hypotonic IV.
Why?Why? The doctor said that might worsen the change in his brain The doctor said that might worsen the change in his brain
cell size, and that his blood osmolarity should be corrected cell size, and that his blood osmolarity should be corrected very slowly. Why?very slowly. Why?

PotassiumPotassium K+K+: 3.5 – 5 mEq/L : 3.5 – 5 mEq/L
- principle cation in ICF compartment - principle cation in ICF compartment - - functionsfunctions: transmission & conduction of: transmission & conduction of nerve impulses, normal cardiac nerve impulses, normal cardiac conduction, skeletal/smooth muscleconduction, skeletal/smooth muscle contraction, and regulates metaboliccontraction, and regulates metabolic activities. activities. - Regulated by dietary intake & renal - Regulated by dietary intake & renal excretion. excretion.
3636

PotassiumPotassium
Role in acid base balance:Role in acid base balance: AcidosisAcidosis- potassium shift occurs from the - potassium shift occurs from the
ICF to the ECF as hydrogen ions move into ICF to the ECF as hydrogen ions move into cells, aldosterone deficiency leads to cells, aldosterone deficiency leads to hyperkalemia. hyperkalemia.
AlkalosisAlkalosis- potassium shift from ECF to ICF in - potassium shift from ECF to ICF in exchange for hydrogen ions, thus lowering exchange for hydrogen ions, thus lowering potassium in the ECF. potassium in the ECF.
3737

3838

3939

HypokalemiaHypokalemiaK+ < 3.5 mEq/L K+ < 3.5 mEq/L
CausesCauses: :
Use of K+ wasting Use of K+ wasting diuretics, polyuria, GI diuretics, polyuria, GI losses (vomiting, losses (vomiting, diarrhea, diarrhea, NG/colostomy NG/colostomy outputs), alkalosis, Tx outputs), alkalosis, Tx of DKA with insulin. of DKA with insulin.
S & SS & S: :
SSkeletal muscle keletal muscle weakness weakness
UU wave/ ECG changes wave/ ECG changes
CConstipation, ileusonstipation, ileus
TToxic effects of digoxinoxic effects of digoxin
IIrregular, weak pulserregular, weak pulse
OOrthostatic hypotensionrthostatic hypotension
NNumbness (paresthesias) umbness (paresthesias)
4040

4141

HyperkalemiaHyperkalemiaK > 5 mEq/LK > 5 mEq/L
CausesCauses::Renal failure, fluid Renal failure, fluid volume deficit, volume deficit, massive cellular massive cellular damage (burns & damage (burns & trauma), acidosis (esp trauma), acidosis (esp DKA), rapid infusion DKA), rapid infusion of stored blood, use of stored blood, use of K+-sparing of K+-sparing diuretics, salt diuretics, salt substitutes. substitutes.
S & SS & S::ECG changes (tall, ECG changes (tall, tented T wave), tented T wave), paresthesias, muscle paresthesias, muscle weakness, abdominal weakness, abdominal cramping, diarrhea.cramping, diarrhea.
4242

Calcium Calcium CaCa22++: 8.5 – 10.5 mg/dL
- 50% bound to bound to albumin, 40%
free ionized.
- functions: bone & teeth formation, blood
clotting, hormone secretion, cardiac conduction, nerve impulse transmission, & muscle contraction.
- PTH & Vitamin D responsible for maintaining “Parathyroid pulls… Calcitonin keeps”
4343

HypocalcemiaHypocalcemia CaCa22++< 8.5 mg/dL< 8.5 mg/dL
CausesCauses::Rapid administration Rapid administration of blood containing of blood containing citrate, citrate, hypoalbuminemia, hypoalbuminemia, hypoparathyroidism, hypoparathyroidism, vitamin D deficiency, vitamin D deficiency, alkalosis, pancreatitis, alkalosis, pancreatitis, CRF, chronic CRF, chronic alcoholismalcoholism
S & SS & S: : numbness & tingling of numbness & tingling of fingers and circumoral fingers and circumoral (around mouth) region, (around mouth) region, hyperactive reflexes, hyperactive reflexes, +Trousseau+Trousseau’s (nerve ’s (nerve excitability/tetany) & excitability/tetany) & +Chvostek’s sign, muscle +Chvostek’s sign, muscle cramps, fractures (if cramps, fractures (if chronic). ECG: chronic). ECG: prolonged ST & QT…prolonged ST & QT…
4444

HypercalcemiaHypercalcemia Ca Ca22++> 10.5 mg/dL> 10.5 mg/dL
CausesCauses::
HyperparathyroidismHyperparathyroidism, , CancerCancer, Paget, Paget’s ’s disease, osteoporosis, disease, osteoporosis, prolonged prolonged immobilization, thiazide immobilization, thiazide diuretics. diuretics.
S & SS & S: :
Anorexia, abdominal Anorexia, abdominal pain & constipation, pain & constipation, muscle weakness, muscle weakness, hypoactive reflexes, hypoactive reflexes, lethargy, flank pain (if lethargy, flank pain (if kidney stones), kidney stones), ECG: ECG: shortened QT & ST shortened QT & ST segment segment
4545

MagnesiumMagnesium
MgMg++++: : 1.5 – 2.5 mEq/L1.5 – 2.5 mEq/L the second most abundant cation in ICF the second most abundant cation in ICF regulated by dietary intake, renal mechanisms, regulated by dietary intake, renal mechanisms,
and actions of PTH. and actions of PTH. FunctionsFunctions: enzyme reactions during : enzyme reactions during
carbohydrate metabolism, helps produce ATP, carbohydrate metabolism, helps produce ATP,
role in protein synthesis, and affects cardiac and role in protein synthesis, and affects cardiac and skeletal muscle excitability. skeletal muscle excitability.
4646

HypomagnesemiaHypomagnesemiaMgMg++ < 1.5 mEq/L++ < 1.5 mEq/L
CausesCauses::inadequate intake, inadequate intake, inadequate inadequate absorption, excessive absorption, excessive loss from GI tract or loss from GI tract or urinary system. urinary system. Alcoholics Alcoholics
S & SS & S: : Similar to Similar to hypocalemia…hypocalemia…The 3 Ts (tremors, The 3 Ts (tremors, twitching, tetany) & twitching, tetany) & hyperactive DTRs. hyperactive DTRs. +Chvostek+Chvostek’s & ’s & Trousseau’s sign. Trousseau’s sign. CNS irritation…CNS irritation…
lethargy, confusion, lethargy, confusion, seizures. seizures. Dysrythmias, N/V Dysrythmias, N/V
4747
Acronym: S.T.A.R.V.E.DAcronym: S.T.A.R.V.E.D

HypermagnesemiaHypermagnesemiaMg++ > 2.5 mEq/LMg++ > 2.5 mEq/L
CausesCauses: :
Renal failure, Renal failure, excessive intakeexcessive intake
S & SS & S::
hypoactive DTRs, hypoactive DTRs,
weakness, weakness, drowsiness, drowsiness, decreased rate/depth decreased rate/depth of respirations, of respirations, bradycardia, bradycardia, hypotension, flushing. hypotension, flushing.
4848
Acronym: R.E.N.A.LAcronym: R.E.N.A.L

ACID-BASE BALANCE ACID-BASE BALANCE
4949

Regulation of Acid-Base BalanceRegulation of Acid-Base Balance
pHpH: indirectly measures H+ concentration : indirectly measures H+ concentration & reflects balance between CO2 (which is & reflects balance between CO2 (which is regulated by the lungs), and HCO3regulated by the lungs), and HCO3¯ (a ¯ (a base regulated by the kidneys). base regulated by the kidneys).
pH is a scale. Measures the acidity or pH is a scale. Measures the acidity or alkalinity of a fluid. alkalinity of a fluid.
5050

Acid-Base BalanceAcid-Base Balance
normal arterial blood values = 7.35-7.45normal arterial blood values = 7.35-7.45 Represents balance between the percentage Represents balance between the percentage
of hydrogen ions & bicarbonate ionsof hydrogen ions & bicarbonate ions AcidAcid-molecule that releases, or donates, H+-molecule that releases, or donates, H+
Carbonic acid (H2CO3)Carbonic acid (H2CO3) BaseBase-molecule that accepts H+-molecule that accepts H+
Bicarbonate (HCO3-)Bicarbonate (HCO3-) 5151

Regulation of Acid-Base BalanceRegulation of Acid-Base Balance
AcidosisAcidosis pH < 7.35pH < 7.35 Contains greater Contains greater
amounts of H+amounts of H+ Results from too Results from too
much COmuch CO22 or not or not enough HCOenough HCO33ˉ ˉ
AlkalosisAlkalosis pH > 7.45pH > 7.45 Contains lesser Contains lesser
amounts of H+amounts of H+ Results from too Results from too
much HCOmuch HCO33ˉ or not ˉ or not enough COenough CO22
5252

Regulation of Acid-Base BalanceRegulation of Acid-Base Balance
Chemical Chemical Buffer Systems Buffer Systems
::Bicarbonate-Bicarbonate-buffer system buffer system •Kidneys: HCOKidneys: HCO33--•Lungs: HLungs: H22COCO33
Respiratory Respiratory System System
FunctionFunction::•Regulate CORegulate CO2 2 (& (& thus Hthus H22COCO3)3)
•ChemoreceptorsChemoreceptors
Kidney Kidney FunctionFunction::
•Make long-term Make long-term changes to pHchanges to pH •Produce Produce HCOHCO33--•Reabsorb or Reabsorb or excrete acids / excrete acids / bases bases
5353

Regulation of pHRegulation of pH
Respiratory systemRespiratory system Control the elimination of CO2Control the elimination of CO2
Renal systemRenal system Eliminate H+ and regulates the elimination Eliminate H+ and regulates the elimination
and production of HCO3- and production of HCO3-
5454

Respiratory SystemRespiratory System
Regulation of CO2Regulation of CO2 Hyperventilation leads to Hyperventilation leads to “blowing off” “blowing off”
CO2CO2 Hypoventilation leads to Hypoventilation leads to “retaining” CO2“retaining” CO2 If CO2 is elevated, hydrogen ion If CO2 is elevated, hydrogen ion
concentration is elevated and pH concentration is elevated and pH decreasesdecreases
Rapid actingRapid acting Does not fully return pH to normal Does not fully return pH to normal
5555

Renal SystemRenal System
Bicarbonate secretion/excretionBicarbonate secretion/excretion Hydrogen ions secretion/excretion Hydrogen ions secretion/excretion Regulate urine pHRegulate urine pH Can fully return pH to normalCan fully return pH to normal
5656

ABGABG
Provide values of acid-base balanceProvide values of acid-base balance Oxygenation status Oxygenation status Arterial blood Arterial blood compensationcompensation
5757

ABG Values ABG Values
PaO2 80-100 mmHg
pH 7.35-7.45
PaCO2 35-45 mmHg
HCO3 22-26 mEq/L
Oxygen saturation 96-100%
5858

Metabolic vs. RespiratoryMetabolic vs. Respiratory
ImbalanceImbalance pHpH pCOpCO22 HCOHCO33
Respiratory Respiratory acidosisacidosis
7.357.35 4545 NormalNormal
Respiratory Respiratory alkalosisalkalosis
7.457.45 3535 NormalNormal
Metabolic Metabolic acidosisacidosis
7.357.35 NormalNormal 2222
Metabolic Metabolic alkalosisalkalosis
7.457.45 Normal Normal 2626
5959

Respiratory AcidosisRespiratory Acidosis
Increase in PCO2, carbonic acidIncrease in PCO2, carbonic acid HypoventilationHypoventilation Decrease in pHDecrease in pH Compensatory mechanismCompensatory mechanism
Kidneys conserve bicarbonate and secrete Kidneys conserve bicarbonate and secrete hydrogen ion into the urine. hydrogen ion into the urine.
6060

Respiratory Acidosis Etiology Respiratory Acidosis Etiology
Lung disease Lung disease Chest injuryChest injury Respiratory failureRespiratory failure Non functioning respiratory musclesNon functioning respiratory muscles SepsisSepsis Airway obstructionAirway obstruction COPDCOPD
6161

6262

Respiratory Alkalosis Respiratory Alkalosis
Decrease in PCO2Decrease in PCO2 Increase in pHIncrease in pH HyperventilationHyperventilation Anxiety/Panic attacks Anxiety/Panic attacks Fever Fever Mechanical ventilationMechanical ventilation
6363

6464

Metabolic acidosis Metabolic acidosis
Base bicarbonate deficiencyBase bicarbonate deficiency Compensatory mechanismCompensatory mechanism
Increase in respiratory rate (Kussmaul Increase in respiratory rate (Kussmaul respiration) respiration)
““blow off” CO2 & H2CO3blow off” CO2 & H2CO3
6565

Metabolic Acidosis Etiology Metabolic Acidosis Etiology
Diabetic ketoacidosisDiabetic ketoacidosis Lactic acid accumulationLactic acid accumulation Starvation Starvation Renal Failure Renal Failure Severe diarrhea Severe diarrhea Increases in chloride Increases in chloride
6666

Metabolic Alkalosis Metabolic Alkalosis
Base bicarbonate excessBase bicarbonate excess Prolonged vomitingProlonged vomiting Gastric suctionGastric suction Compensatory mechanismCompensatory mechanism
Decrease in respiratory rate in order to Decrease in respiratory rate in order to increase CO2increase CO2
Renal excretion of bicarbonate Renal excretion of bicarbonate
6767

Oxygen saturation
Gives you an idea about how the patient is Gives you an idea about how the patient is breathing/oxygenatingbreathing/oxygenating
Has absolutely nothing to do with acid Has absolutely nothing to do with acid base balancebase balance
Adequate saturation may not be indicative Adequate saturation may not be indicative of adequate oxygenation of adequate oxygenation
6868

ABGs…ABGs…
Lets review!!Lets review!!
6969

Respiratory (PaCO2)Respiratory (PaCO2)
PaCO2 is an acid, the higher the PaCO2, PaCO2 is an acid, the higher the PaCO2, the more acid you have on board the more acid you have on board
Normal values 35-45 mm HgNormal values 35-45 mm Hg Abnormal values: > 45 mm Hg is acidosisAbnormal values: > 45 mm Hg is acidosis
< 35 mm Hg is alkalosis< 35 mm Hg is alkalosis
7070

Metabolic (HCO3)Metabolic (HCO3)
Bicarbonate is a base. The higher the Bicarbonate is a base. The higher the HCO3 you have on board, the more HCO3 you have on board, the more alkaline (base) you have.alkaline (base) you have.
Base neutralizes acids.Base neutralizes acids. Normal values: 22-26 mEq/LNormal values: 22-26 mEq/L Abnormal values: > 26 mEq is alkalosisAbnormal values: > 26 mEq is alkalosis
< 22 mEq is acidosis < 22 mEq is acidosis
7171

ABG Interpretation ABG Interpretation
Step 1Step 1
Look at the PaO2 level and answer the Look at the PaO2 level and answer the question, Does it reflect hypoxemia?question, Does it reflect hypoxemia?
Step 2Step 2
Look at the pH level and answer the Look at the pH level and answer the question, Is the pH level on the acid or question, Is the pH level on the acid or alkaline side?alkaline side?
7272

ABGABG’s’s
Step 3Step 3Look at the PaCO2 level and answer the Look at the PaCO2 level and answer the
question, does this show respiratory question, does this show respiratory acidosis, alkalosis or is it normal?acidosis, alkalosis or is it normal?
Step 4Step 4Look at the HCO3 level and answer the Look at the HCO3 level and answer the
question, does the HCO3 show metabolic question, does the HCO3 show metabolic acidosis, alkalosis or is it normal?acidosis, alkalosis or is it normal?
7373

ABGABG’s’s
Step 5Step 5
Look back at the pH level and answer the Look back at the pH level and answer the question, does the pH show question, does the pH show compensation?compensation?
When the pH is back to normal, the patient When the pH is back to normal, the patient has full compensation.has full compensation.
7474







![Acid Base & Fluid & Electrolytes[1]](https://img.pdfslide.net/doc/110x75/577d35b91a28ab3a6b913ace/acid-base-fluid-electrolytes1.jpg)