Embed Size (px)
Citation preview
HIV Treatment Access
in Middle-Income Countries
Project by ITPC-led
Consortium and funded by
UNITAID
Solange Baptiste
May 11, 2015
ITPC
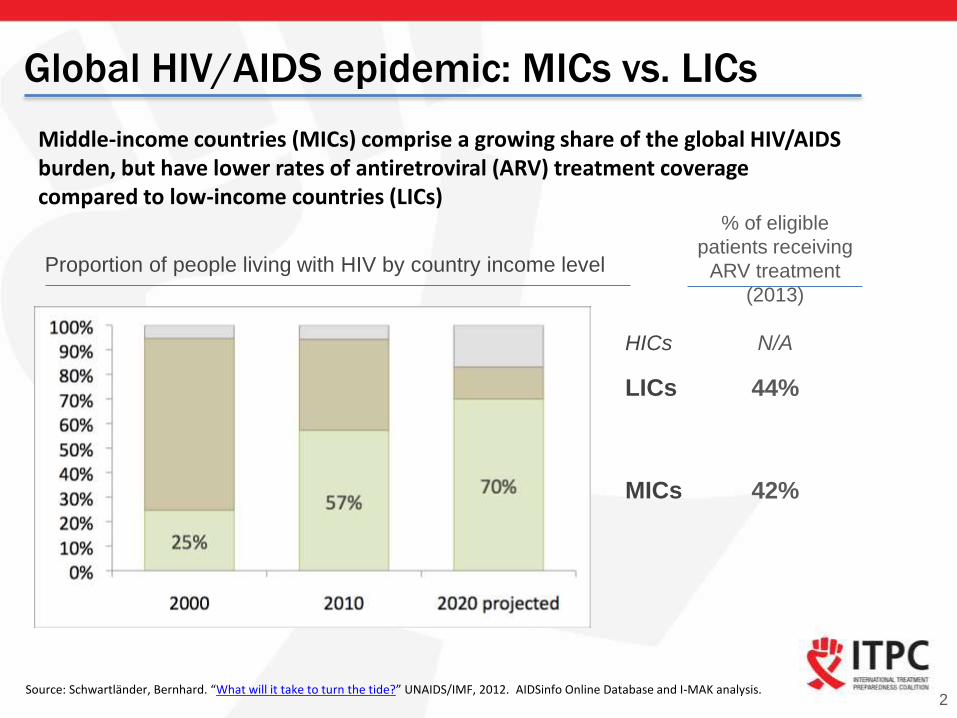
Global HIV/AIDS epidemic: MICs vs. LICs
2
Middle-income countries (MICs) comprise a growing share of the global HIV/AIDS burden, but have lower rates of antiretroviral (ARV) treatment coverage compared to low-income countries (LICs)
Proportion of people living with HIV by country income level
Source: Schwartländer, Bernhard. “What will it take to turn the tide?” UNAIDS/IMF, 2012. AIDSinfo Online Database and I-MAK analysis.
% of eligible
patients receiving
ARV treatment
(2013)
44%
42%MICs
LICs
HICs N/A
Why focus on middle-income countries?
3
“Ensuring universal HIV treatment access in middle-
income countries remains a major challenge”– 2013 UNAIDS Global Report on the AIDS Epidemic
• They are home to almost half of the world's population, 1/3 of people living on less
than $2 per day, and a large and growing share of HIV infections (currently 62%)
• They pay exorbitantly high ARV prices1, which makes closing the treatment gap
unaffordable. This is due to:
─ Patent monopolies: ARV companies file more patents in MICs than LICs, effectively
blocking generic competition which would dramatically lower prices. However, many of
these patents are unmerited.2
─ Exclusion from drug access initiatives: ARV companies offer tiered pricing or
generic licenses to LICs, but most MICs1 are excluded from these programs.
• They represent a large unmet need – no other global HIV interventions focus on
MICs
Source: World Bank, AIDSinfo online database and I-MAK analysis.
Notes: 1 Statements are most applicable to MICs outside of sub-Saharan Africa (SSA), as MICs in SSA are typically included in
originator drug access programs. 2 Many patents do not meet the lawful criteria for inventiveness. Under TRIPS, countries may
deny patents if a drug is not truly inventive, e.g. when companies make minor modifications and apply for follow-on patents – a
practice known as evergreening.
MIC intervention overview
4
Remove patent barriers to generic competition in four
focus MICs by reforming their patent laws, challenging
undeserved patents, and advocating for the selective use of
compulsory licenses1.
Increase access to more affordable generic ARVs,
generating $150M annual savings across the four
countries, which can be used to treat 130,000 additional
patients.
Influence other countries to follow these precedents and
achieve similar results.
Objectives
Intended
outcomes
1 A compulsory license is an authorization granted by the government to use another's intellectual property without the consent
of the patent holder, while paying a reasonable royalty to the patent holder. Subject to certain conditions, the TRIPS agreement
allows developing countries to issue compulsory licenses for medicines if the country cannot otherwise access the medicine at
an affordable price.
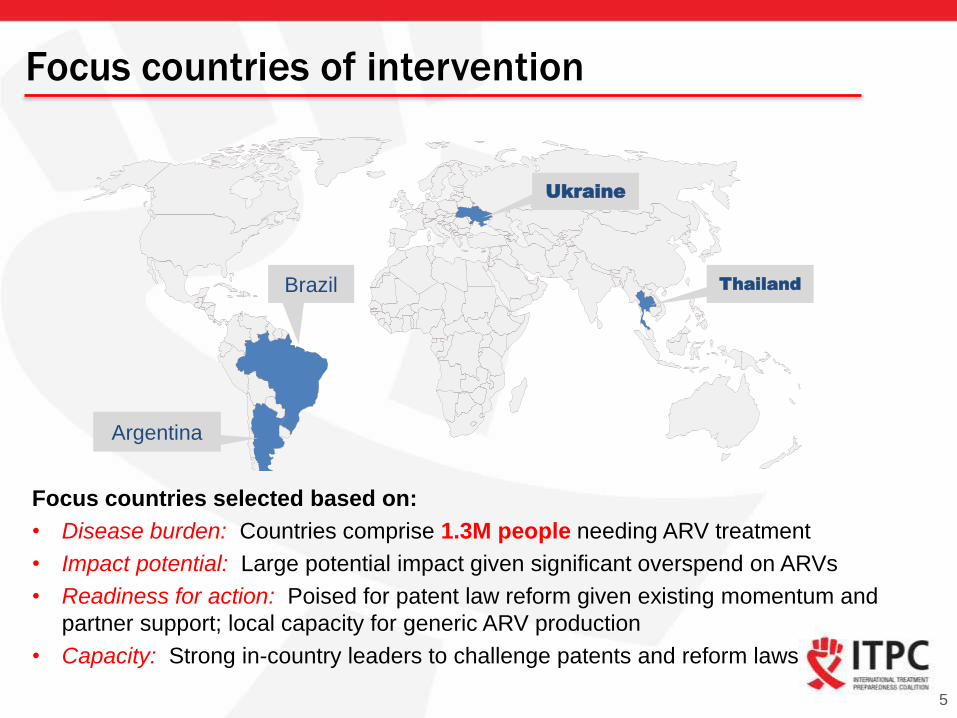
Focus countries of intervention
5
Figure 3: Map of project countries
Focus countries selected based on:
• Disease burden: Countries comprise 1.3M people needing ARV treatment
• Impact potential: Large potential impact given significant overspend on ARVs
• Readiness for action: Poised for patent law reform given existing momentum and
partner support; local capacity for generic ARV production
• Capacity: Strong in-country leaders to challenge patents and reform laws
Argentina
Brazil Thailand
Ukraine
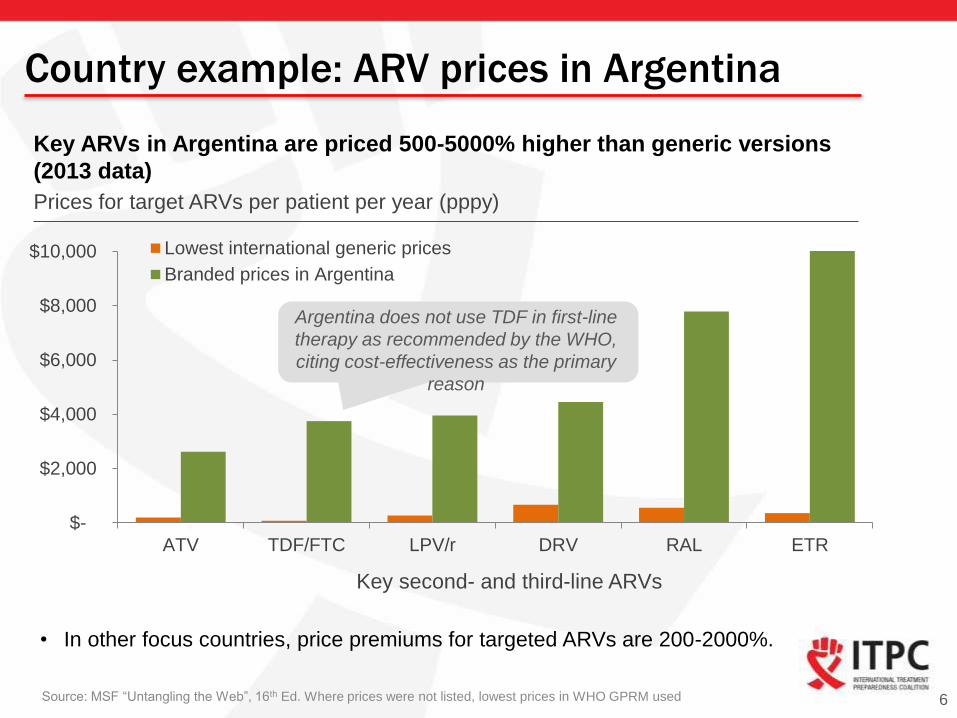
Country example: ARV prices in Argentina
6
Key ARVs in Argentina are priced 500-5000% higher than generic versions
(2013 data)
Source: MSF “Untangling the Web”, 16th Ed. Where prices were not listed, lowest prices in WHO GPRM used
Prices for target ARVs per patient per year (pppy)
$-
$2,000
$4,000
$6,000
$8,000
$10,000
ATV TDF/FTC LPV/r DRV RAL ETR
Lowest international generic prices
Branded prices in Argentina
Key second- and third-line ARVs
Argentina does not use TDF in first-line
therapy as recommended by the WHO,
citing cost-effectiveness as the primary
reason
• In other focus countries, price premiums for targeted ARVs are 200-2000%.
Coalition members: Country leadership
7
Fundación Grupo Efecto Positivo (Argentina)
• Promotes HIV treatment access through political/social
engagement and policy dialogue on ARV patents, working
with broad network of gov. & civil society partners
All-Ukrainian Network of PLWH (Ukraine)
• Largest PLHIV organization in Ukraine with strong
government relationships that intervenes on key ARV patent
litigations
Associação Brasileira Interdisciplinar de AIDS (Brazil)
• 25 year old organization, globally recognized as a leading
HIV and human rights NGO, with deep experience in patent
oppositions and law reform
AIDS Access Foundation (Thailand)
• Over 20 years experience working closely with government
and community, including on policy, free trade agreements,
compulsory license issuance, and patent litigation

Coalition members: Global leadership
8
International Treatment Preparedness Coalition (ITPC)
• Global grassroots network of people living with HIV and
their supporters united in promoting access to treatment
• Pioneer in treatment access advocacy, community
education and capacity building around ARV access
Initiative for Medicines, Access & Knowledge (I-MAK)
• Expert team of lawyers and scientists that challenge
invalid drug patents to facilitate generic competition,
catalyze price reductions and improve access
• Provides technical support to country partners to
challenge patents and reform patent systems
• Leading global patent oppositions unit in the public
interest
Log Frame at-a-glance
GOAL (Impact) : Reduction in ARV treatment costs
Outcome : IP barriers to generic market entry are challenged
OUTPUTS
1: Inclusion of public health safeguards in draft patent law amendments
2: Prevention of TRIPS-plus provisions in patent laws
3: Public Health approaches to patent examination supported in beneficiary countries
4: Pre-grant oppositions/invalidation actions filed on priority ARVs
5: Opportunities for Compulsory Licenses identified
6: Functional information exchange platform to disseminate knowledge about IP
9
Plan of action
10
File patent oppositions1 on key
ARVs that do not represent true
innovations
1
Reform patent laws to improve
patentability criteria/anti-
evergreening2 measures; expand
patent opposition mechanisms; and
strengthen compulsory licensing
grounds and procedures
2
Advocate for selective use of
compulsory licenses by
dialoguing with government and
pursuing necessary law reforms
3
Create technical working groups
and strategy guides to support the
success of IP interventions build
capacity with government & civil
society partners
4
1 Patent s can be opposed either before or after they are granted (known as pre-grant and post-grant oppositions) by providing patent offices with
evidence that the product does not demonstrate inventiveness and/or enhanced therapeutic efficacy. 2 Evergreening occurs when companies make minor product modifications and apply for follow-on patents.
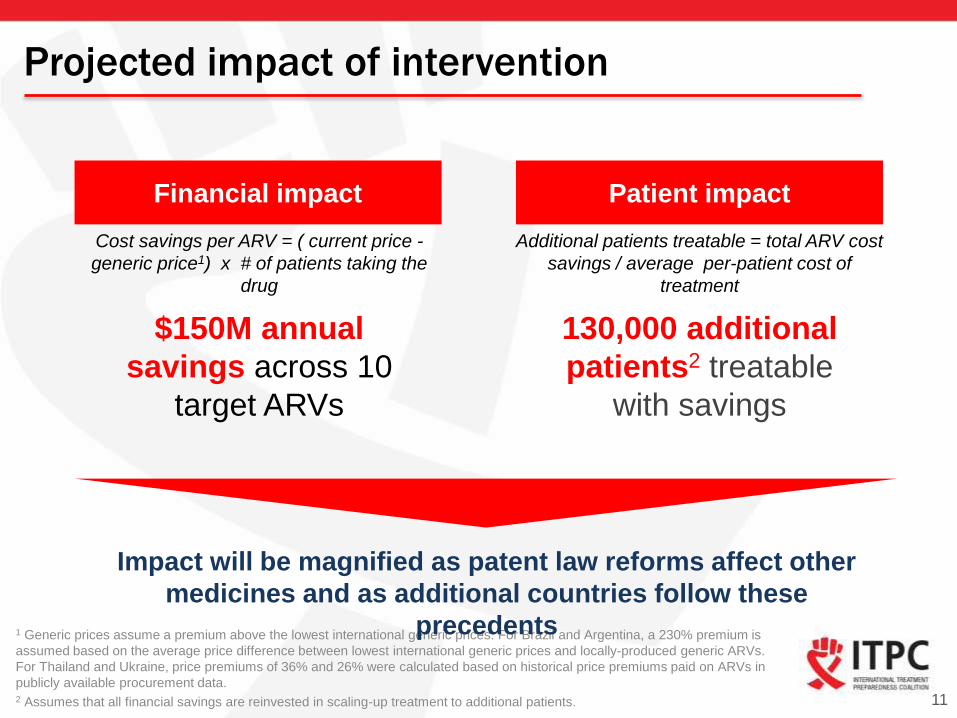
Projected impact of intervention
11
Financial impact Patient impact
Cost savings per ARV = ( current price -
generic price1) x # of patients taking the
drug
Additional patients treatable = total ARV cost
savings / average per-patient cost of
treatment
$150M annual
savings across 10
target ARVs
130,000 additional
patients2 treatable
with savings
1 Generic prices assume a premium above the lowest international generic prices. For Brazil and Argentina, a 230% premium is
assumed based on the average price difference between lowest international generic prices and locally-produced generic ARVs.
For Thailand and Ukraine, price premiums of 36% and 26% were calculated based on historical price premiums paid on ARVs in
publicly available procurement data.2 Assumes that all financial savings are reinvested in scaling-up treatment to additional patients.
Impact will be magnified as patent law reforms affect other
medicines and as additional countries follow these
precedents
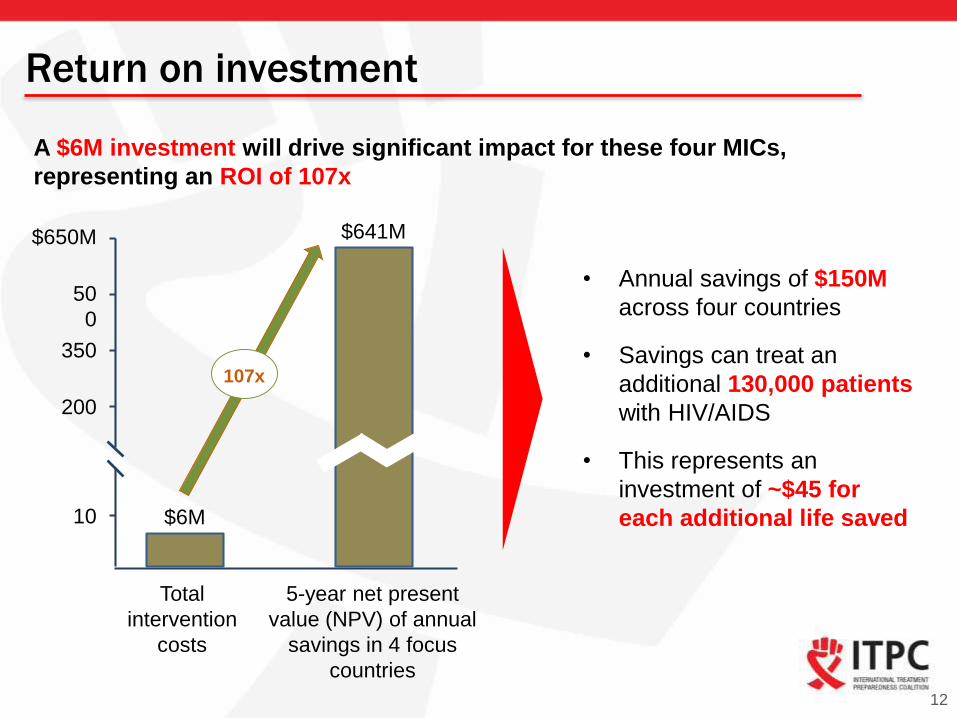
Return on investment
12
$650M
10
$641M
$6M
200
50
0
Total
intervention
costs
5-year net present
value (NPV) of annual
savings in 4 focus
countries
107x
• Annual savings of $150M
across four countries
• Savings can treat an
additional 130,000 patients
with HIV/AIDS
• This represents an
investment of ~$45 for
each additional life saved
A $6M investment will drive significant impact for these four MICs,
representing an ROI of 107x
350
Process for Log Frame development – Internal
consortium
• Very involved coordination and thought
partnership process with many partners
• All partners developed workplans, budgets,
attended frequent calls, skype meetings
(bilaterally and as a full group)
• Issues specific to the nature of working in a
consortium of organizations that never worked
together formally
– Deciding what to do
– How to bring it all together
– Time constraints
– Budget congruency and negotiations
– Clarity needed on interpretation and presentation of data in
log frame13
Process for Log Frame development – With UNITAID
Challenges included:
• Process and log frame changed 2 to 3x – undue
burden
• Lack of clarity on who as the guide on log frames
(seemed to be a lack of internal UNITAID department
cohesion)
• During the project plan phase the log frame evolution
was smoother and we really credit being able to work
with Jane (and the M&E team) who were all working in
sync, coordinating together, providing feedback in a
timely manner, and offering concrete suggestions to the
finish line
• Request to consider last minute changes very carefully
especially for grantees working with many partners and
in many different countries.14

Thank You