Embed Size (px)
Citation preview


Varied collection of protozoal diseases Named after Leishman - First identified the
organisms in 1901 Smears taken from a man who had died of
“Dum Dum” fever Annually - Two million cases worldwide Has emerged as an AIDS - associated
opportunistic infection

1. Cutaneous
2. Diffuse cutaneous
3. Mucocutaneous
4. Visceral Leishmaniasis (Kala Azar)
Endemic in 88 countries on five continents Cutaneous Leishmaniasis cases occur in Iran,
Afghanistan, Syria, Saudi Arabia, Brazil and Peru
Visceral Leishmaniasis cases occur in Bangladesh, Brazil, India and Sudan
World Health Organization estimates that 350 million people are at risk

2.4 million disability - adjusted life years
Around 7,00,000 deaths per year
WHO South East Asia Region - 200 million
people in the Region are “at risk”

World’s largest foci of Visceral Leishmaniasis, accounting for 50% of the total burden
Endemic in 4 states in India: Bihar- 32 districts Jharkhand- 4 districts West Bengal- 11 districts Uttar Pradesh- 5
districts
An estimated 165.4 million population is at risk About 1,00,000 cases occur annually


19 protozoan species Genus Leishmania Amastigote- obligate intracellular parasites
and divide in macrophages- diagnostic phase
Promastigotes- extracellular present in the arthropod vectors- infective phase
Absence of cross immunity

Leishmania donovani complex Leishmania donovani, L. infantum and L.
chagasi Leishmania mexicana complex
L. mexicana, L. amazonensis and L. venezuelensis
Leishmania tropica Leishmania major Leishmania aethiopica In India: Leishmania donovani


Female sand flies of the genus Lutzomyia in the Americas and Phlebotomus in other parts of the world
Sandflies breed in cracks and crevices in the soil and buildings, tree holes and caves
Sandflies are active in the evening and night - time hours
In India, Phlebotomus argentipes is a proven vector of KalaAzar.

Cutaneous form mainly zoonotic, - humans are accidentally exposed
Indian Kala - Azar is anthroponotic with humans being the only known reservoir of infection
Peak age of infection is 5 to 9 years Males Poor socio-economic background Common in various farming practices,
forestry, mining and fishing

Mostly confined to the plainsOvercrowding,Poor ventilationHigh relative humidity, warm temperatureAccumulation of organic matter in the
environment facilitates transmission

Transmitted by the bite of infected female sandflies
Rarely: initiated by amastigotes via blood (shared needles, transfusion, transplacental spread) or organ transplantation

Incubation period: Extremely variable (10 days - 3 to 8
months – 2 yrs)Varied presentation:
Ulcerative skin lesions Destructive mucosal inflammation Disseminated visceral infection

Typical lesion : Develops at the site where
promastigotes are injected by the vector A papule - papule enlarges – ulcerates
Multiple lesions may be present


Infected with Leishmania braziliensis Begins with nasal stuffiness and
inflammation Ulceration of the nasal mucosa and
septum follows. The lips, cheeks, soft palate, pharynx
and larynx may eventually be involved, resulting in substantial disfigurement
More common among immunosuppressed with neoplasms or AIDS

Recurrent fever Loss of appetite, pallor and weight loss with
progressive emaciation Weakness Splenomegaly - spleen enlarges rapidly to
massive enlargement, usually soft and non-tender
Liver - enlargement not to the extent of spleen, soft, smooth surface, sharp edge


Death often occurs due to a secondary bacterial infection, such as
Pneumonia, Septicemia, Dysentery, Tuberculosis, Measles Other viral infections

Anaemia, Neutropenia, Thrombocytopenia and pronounced hypergammaglobulinemia.
The anaemia is usually normocytic, normochromic, unless there is concomitant iron deficiency
Leukopenia can be profound with white blood cell counts below 1000/mL
The globulin level can reach 9 or 10 g/dl.

Some patients in India and Africa develop skin lesions following treatment, ranging from hyperpigmented macules to frank nodules
Skin lesions typically appear 1 or 2 years after treatment and may persist for as long as 20 years.
Persistence of lesions beyond one year is associated with high anti - leishmanial antibody titers and negative leishmanial skin test responses
Anti - leishmanial treatment is indicated in Indian PKDL

Immunocompromised individuals progress to develop the disease far more often than immunocompetent people
It quickly accelerates the onset of AIDS and shortens the life expectancy of HIV - infected people.
Visceral Leishmaniasis is considered a major contributor to a fatal outcome HIV in co - infected patients

Parasite Identification: Wright-Giemsa stain is used for identifying
amastigotes in tissue sections Serology:
Anti-leishmanial antibody titers are typically present in:▪ High titer in people with Visceral Leishmaniasis
and ▪ Low titer or undetectable in those with
Cutaneous Leishmaniasis. Assays such as ELISA, IFAT and agglutination
assays, rk-39 rapid diagnostic test
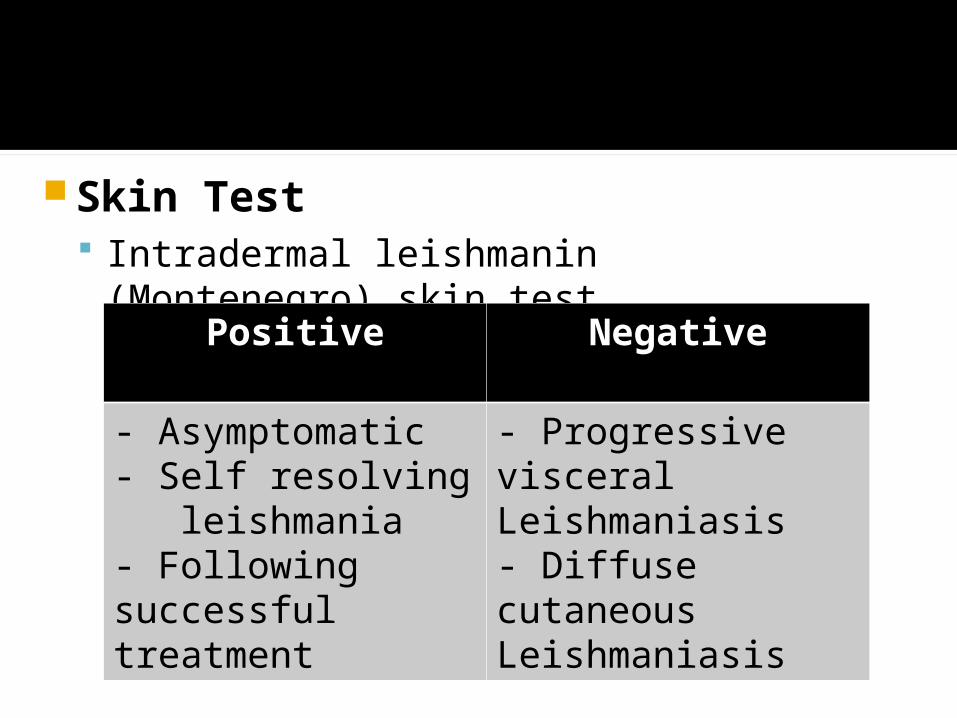
Skin Test Intradermal leishmanin (Montenegro)
skin test Positive Negative
- Asymptomatic- Self resolving leishmania- Following successful treatment
- Progressive visceral Leishmaniasis- Diffuse cutaneous Leishmaniasis

Aldehyde test Napier is a simple test 1 to 2 ml of serum from a case of kala-
azar is taken and a drop or two of 40 per cent formalin is added. A positive test is indicated by jellification to milk- white opacity like the white of a hard-boiled egg so that in ordinary light newsprint is invisible through it

FIRST LINE OF DRUGS
SHORT TERM LONG TERM
SSG SENSITIVITY >90%
SSG SENSITIVITY <90%
SSG 20 mg/Kg i.m or i.v for 20 days
Amphotericin B 1mg/kg i.v daily or alternate days
SSG RESISTANCE >20%
SSG SENSITIVITY >80%
MILTEFOSINE 100mg/day divided doses for 4 weeks
SSG 20mg/kg/ day i.m/i.v for 30 days
CONTROL OF RESERVOIR

SECOND LINE OF DRUGS
SSG FAILURE SSG AND MILTEFOSINE FAILURE
Amphotericin B 1mg/kg i.v daily or alternate
LIPOSOMAL AMPHOTERICIN B

Treatment of PKDL : SSG in usual dosage for kala azar Could be given for 120 days. Repeated 3-4 courses of Amphotericin B
can be given in patients failing SSG treatment.

Sandfly Control: using residual insecticides, DDT used as the first choice BHC may be used as second line of defence Santation measures like removal of breeding
places
Personal prophylaxis: The short - term visitor to an endemic area should use personal protective measures to avoid sand fly bites
The application of DEET (diethyltoluamide) Use of fine mesh nets Application of insect repellants

1. The disease is endemic in following three countries of the WHO South East Asia Region except: (a). Bangladesh (b) India (c) Nepal (d) Sri lanka
2. The disease is reported in _________ no of districts in India:(a) 51 (b) 52 (c) 53 (d) 54

3. State which accounts for more than 90 per cent of the cases in India (a) Uttar Pradesh (b) Bihar (c) Assam (d) M.P
4. Leishmania donovani complex comprises of all except (a) Leishmania infantum (b) Leishmania chagasi (c) Leishmania venezuelensis (d) Leishmania donovani5. Cutaneous Leishmaniasis is also known as all the following except (a) Oriental sore (b) Aleppo evil (c) Delhi boil (d) EspundiaAnswers : (1) d; (2) b; (3) b; (4) c; (5) a.