Embed Size (px)
Citation preview
Dr Ajay Katoch
Assistant Professor, Veterinary Medicine
Introduction
The kidneys are
responsible for the
excretion of nitrogenous
and other metabolic
waste products and for
the regulation of water,
electrolyte and acid-base
balance
The kidney has a biosynthetic role,
and is involved in the production of
renin, erythropoietin, prostaglandins
and Vitamin D3
Gluconeogenesis under conditions
of starvation and is an important site
for degradation of some peptide
hormones
Essential terminology
Renal disease
Renal failure
Azotemia
Uremia
Renal disease
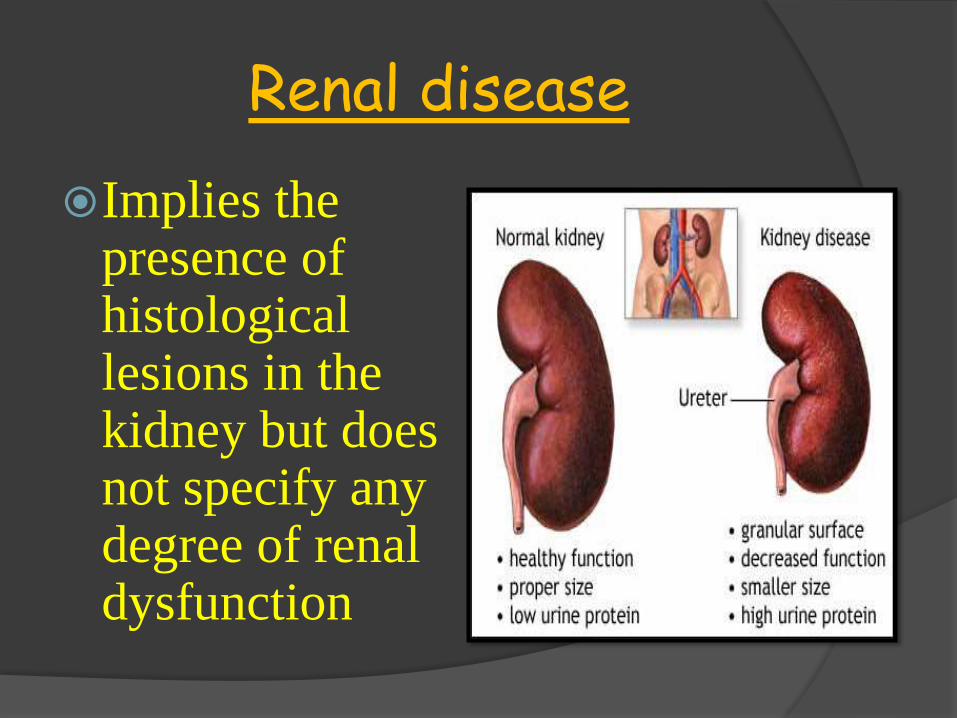
Implies the presence of histological lesions in the kidney but does not specify any degree of renal dysfunction
Renal failure
Inability of the kidney to maintain the homeostasis leading to :
The buildup of the nitrogenous waste in blood (azotemia)
The loss of urine concentrating ability
Disturbances of fluid, electrolyte, and acid-base balance
75% of the total nephron population has become non-functional
Azotemia
Increased concentration of non-
protein nitrogenous waste
products (e.g. urea, creatinine) in
the blood
Uremia
Uremia is the poly systemic toxic
syndrome, which develops with
the progression of renal failure
and is characterized by the
presence of clinical signs in
association with azotemia
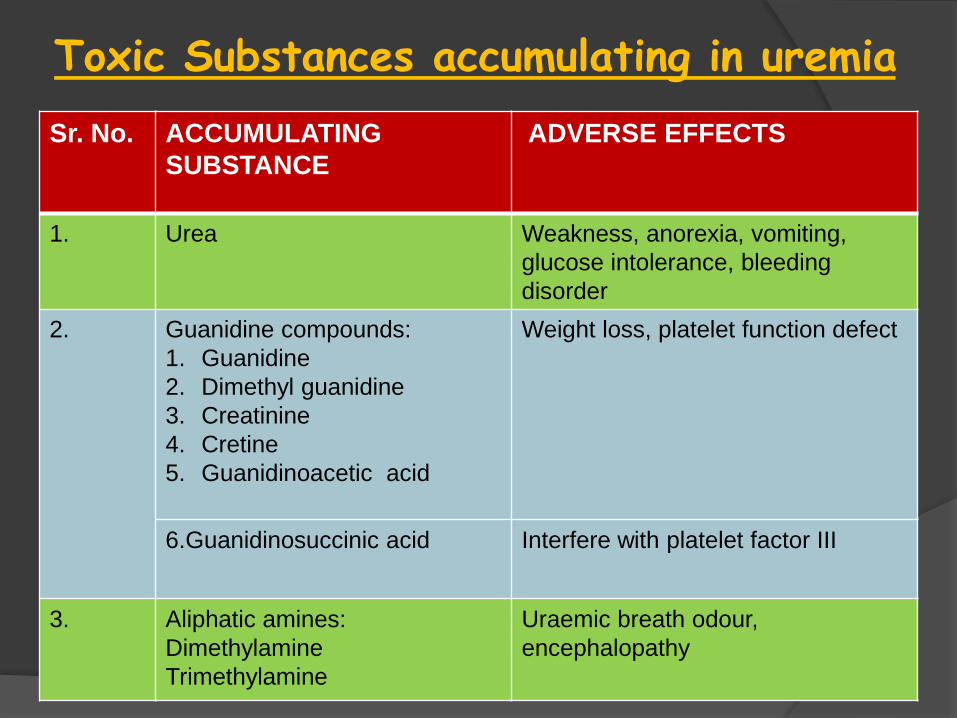
Toxic Substances accumulating in uremia
Sr. No. ACCUMULATING
SUBSTANCE
ADVERSE EFFECTS
1. Urea Weakness, anorexia, vomiting,
glucose intolerance, bleeding
disorder
2. Guanidine compounds:
1. Guanidine
2. Dimethyl guanidine
3. Creatinine
4. Cretine
5. Guanidinoacetic acid
Weight loss, platelet function defect
6.Guanidinosuccinic acid Interfere with platelet factor III
3. Aliphatic amines:
Dimethylamine
Trimethylamine
Uraemic breath odour,
encephalopathy
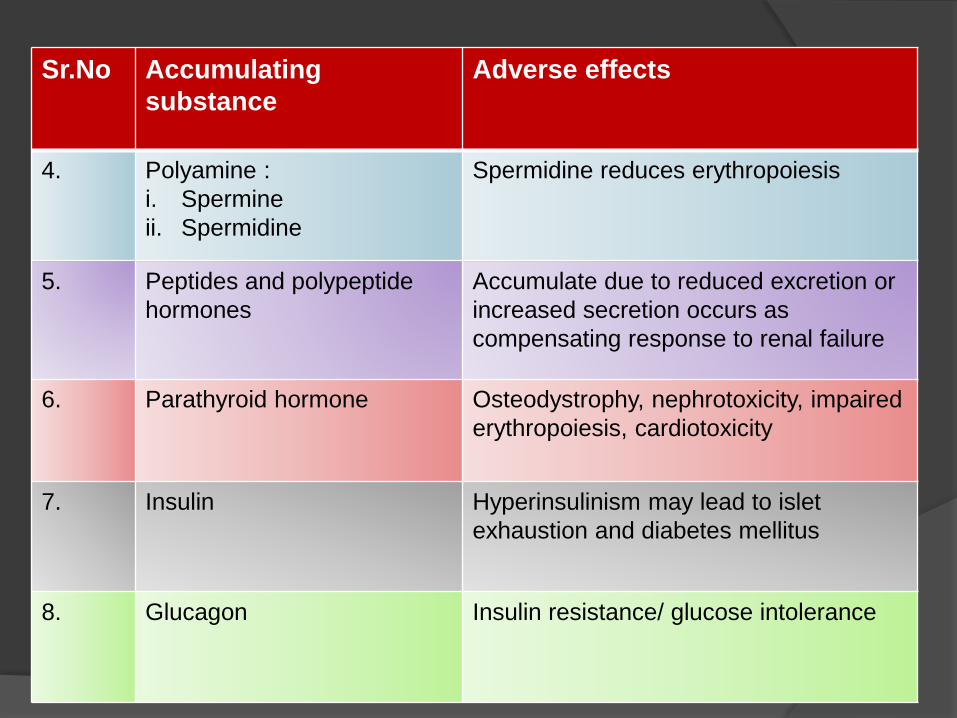
Sr.No Accumulating
substance
Adverse effects
4. Polyamine :
i. Spermine
ii. Spermidine
Spermidine reduces erythropoiesis
5. Peptides and polypeptide
hormones
Accumulate due to reduced excretion or
increased secretion occurs as
compensating response to renal failure
6. Parathyroid hormone Osteodystrophy, nephrotoxicity, impaired
erythropoiesis, cardiotoxicity
7. Insulin Hyperinsulinism may lead to islet
exhaustion and diabetes mellitus
8. Glucagon Insulin resistance/ glucose intolerance
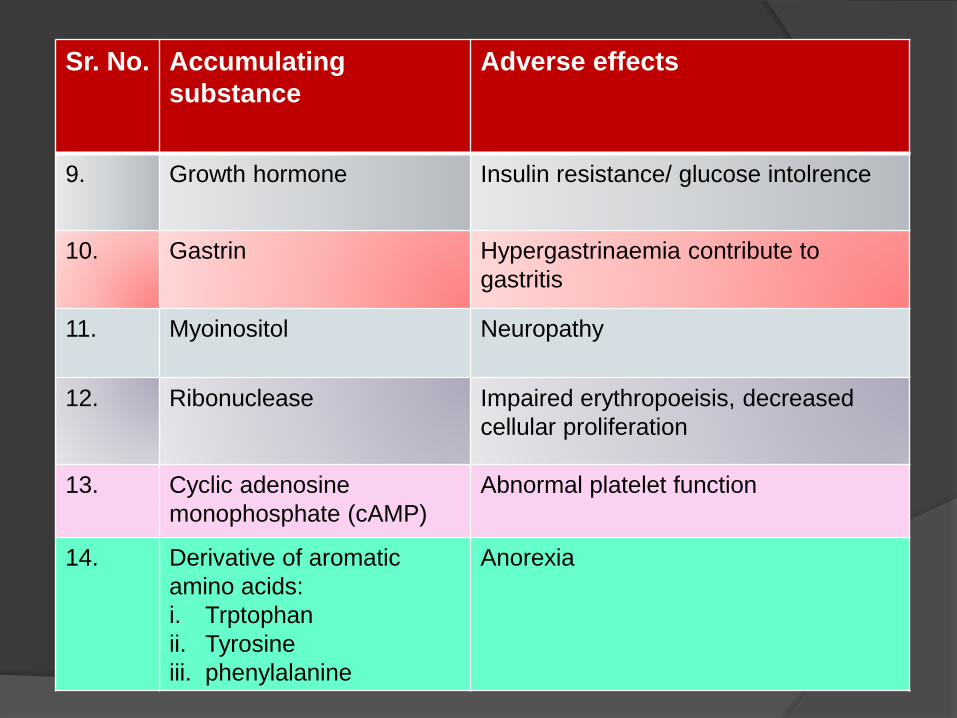
Sr. No. Accumulating
substance
Adverse effects
9. Growth hormone Insulin resistance/ glucose intolrence
10. Gastrin Hypergastrinaemia contribute to
gastritis
11. Myoinositol Neuropathy
12. Ribonuclease Impaired erythropoeisis, decreased
cellular proliferation
13. Cyclic adenosine
monophosphate (cAMP)
Abnormal platelet function
14. Derivative of aromatic
amino acids:
i. Trptophan
ii. Tyrosine
iii. phenylalanine
Anorexia
Renal failure
Acute
renal
failure
Chronic
renal
failure
Acute renal failure
Acute renal failure (ARF) describes a sudden reduction in renal function associated with a
sudden decrease in the glomerular filtration rate (GFR) and the rapid development of
azotemia and uremia
Causes
Pre renal (functional )
Shock
Dehydration
Heart failure
Hypoadrenocorticism
Thrombosis of the renal artery or massive blood
loss
Renal intrinsic ( structural)
Acute tubular necrosis
Ischemia Toxin Tubular
factors
Renal intrinsic ( structural)
Acute interstitial Necrosis
Inflammation Oedema
Renal intrinsic ( structural)
Glomerulonephritis
Damage to
intrinsic
mechanisms
Post renal (obstructive)
Urolithiasis
Neoplasm
Herniation
Damage to lower urinary tract
Anatomical abnormalities
Some Nephrotoxins causing renal damage
Ethylene glycol (in antifreeze)
Antibiotics: Amino glycosides, Tetracycline,
Cyclosporin
Chemotherapeutics: Amphotericin B, cis-
platinum, Doxorubicin
Heavy metals: Lead, Thallium, Zinc, Arsenic,
Mercury
Hypercalcemia: Malignancies,
Hyperparathyroid, Vitamin D toxicity
Other causes: Carbon tetrachloride,
Chloroform, Iodinated contrast media
Clinical signs of ARF
Hyperkalemia
Nausea/Vomition
Pulmonary edema
Clinical signs of ARF
Ascites
Dehydration
Clinical signs of ARF
Encephalopathy
Kidney pain
Oliguria
Shock
Disseminated intravascular coagulation (DIC)
Respiratory distress
Neurologic disturbances
Coma and death
Other signs include -
Diagnosis
History and clinical signs
Laboratory findings -
i. Rising creatinine and urea
ii. Rising potassium
iii. Acidosis
iv. Hyponatraemia
v. Hypocalcemia
Management of ARF
Early recognition of disease
Identification and treatment of specific underlying cause
Sodium bicarbonate to correct metabolic acidosis
Provide nutritional support – Non protein calories but high quality protein in limited amount
Management of ARF -
Promote urine output if still anuric.-
Frusemide, Mannitol
Dialysis to remove excess fluid &
waste products.
Gastric protectants and anti-emetics to
alleviate gastrointestinal disturbances
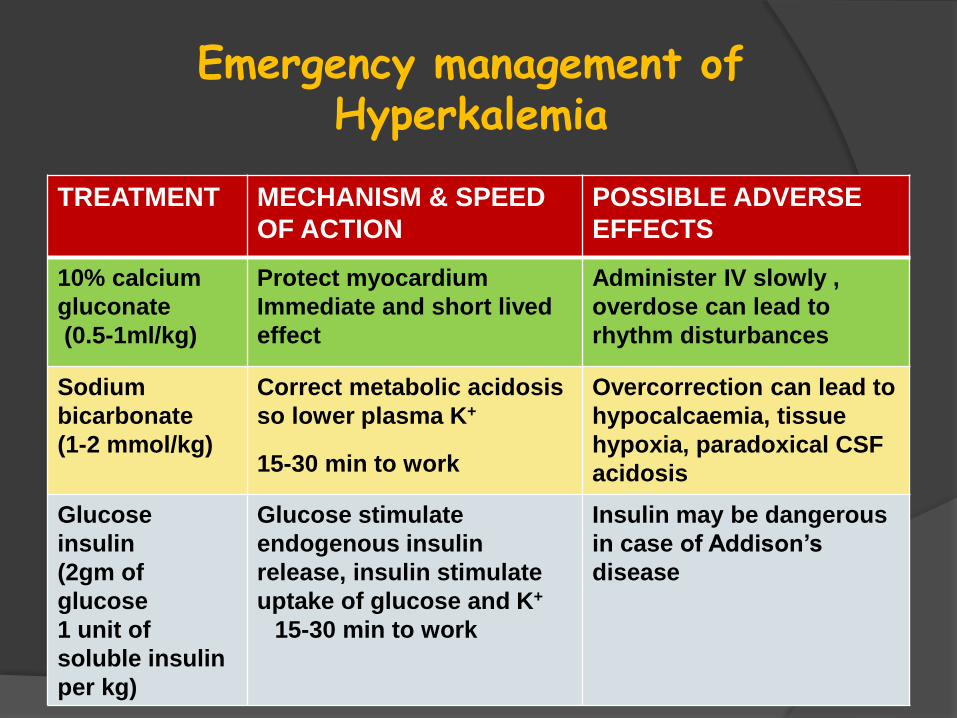
Emergency management of Hyperkalemia
TREATMENT MECHANISM & SPEED
OF ACTION
POSSIBLE ADVERSE
EFFECTS
10% calcium
gluconate
(0.5-1ml/kg)
Protect myocardium
Immediate and short lived
effect
Administer IV slowly ,
overdose can lead to
rhythm disturbances
Sodium
bicarbonate
(1-2 mmol/kg)
Correct metabolic acidosis
so lower plasma K+
15-30 min to work
Overcorrection can lead to
hypocalcaemia, tissue
hypoxia, paradoxical CSF
acidosis
Glucose
insulin
(2gm of
glucose
1 unit of
soluble insulin
per kg)
Glucose stimulate
endogenous insulin
release, insulin stimulate
uptake of glucose and K+
15-30 min to work
Insulin may be dangerous
in case of Addison’s
disease
Chronic renal failure
Chronic renal failure is a relatively common
syndrome in older dogs and represents the end
stage of a number of renal disease
Clinical signs of CRF are not usually apparent
until at least 65% to 75% of renal tissue is
destroyed; so early cases often go undetected
Cause
Pyelonephritis
Chronic nephritis
Renal amyloidosis
Renal urolithiasisHydronephrosisPrimary renal
neoplasia
Glomerulonephritis
Clinical signs
Polyuria and Polydipsia
Weight loss/loss of
muscle mass/poor hair coat
Anorexia with vomition
Weakness, lethargy & depression
Pallor & dryness of mucous membranes
Oral ulceration
Clinical signs
Hypertension
Diarrhoea
Pruritis (itching)
Edema
Anaemia
Neurologic changes
Diagnosis
I. History
II. Clinical findings
III. Laboratory findings:
Urinalysis-
Sp. gravity<1.025
Proteinuria, WBC,RBC
Blood- Lymphopenia, Non-
regenerative anaemia.
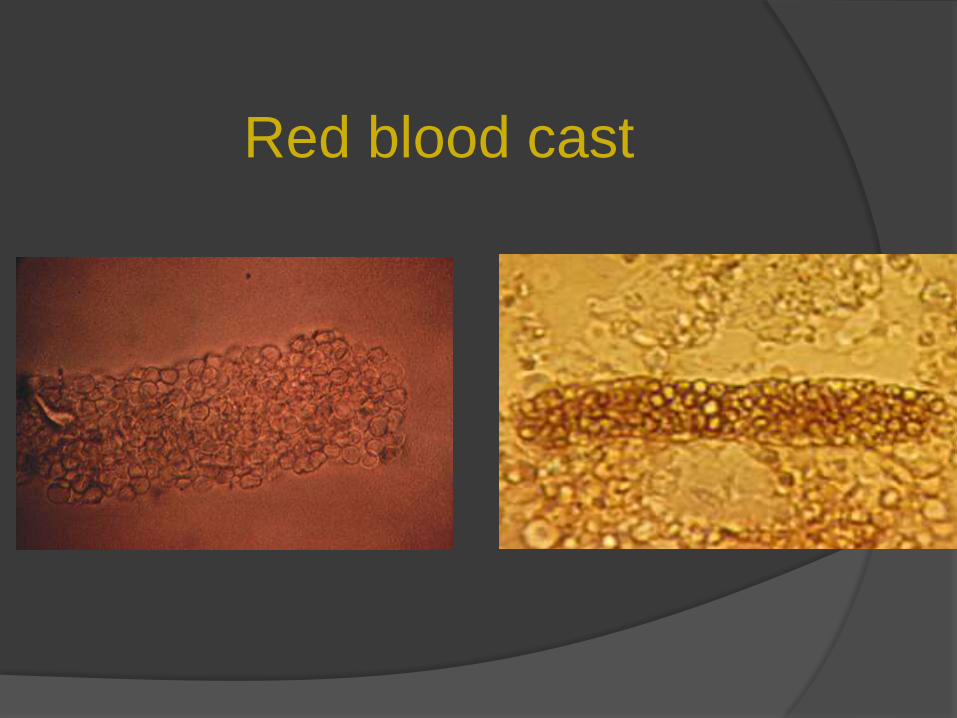
Red blood cast

WBC cast
Diagnosis :IV. Blood Biochemistry:
Blood urea >40mg/dl
Creatinine level > 2mg/dl
Elevated phosphorus level
Elevated Cholesterol
Elevated or decreased calcium level
Acidosis
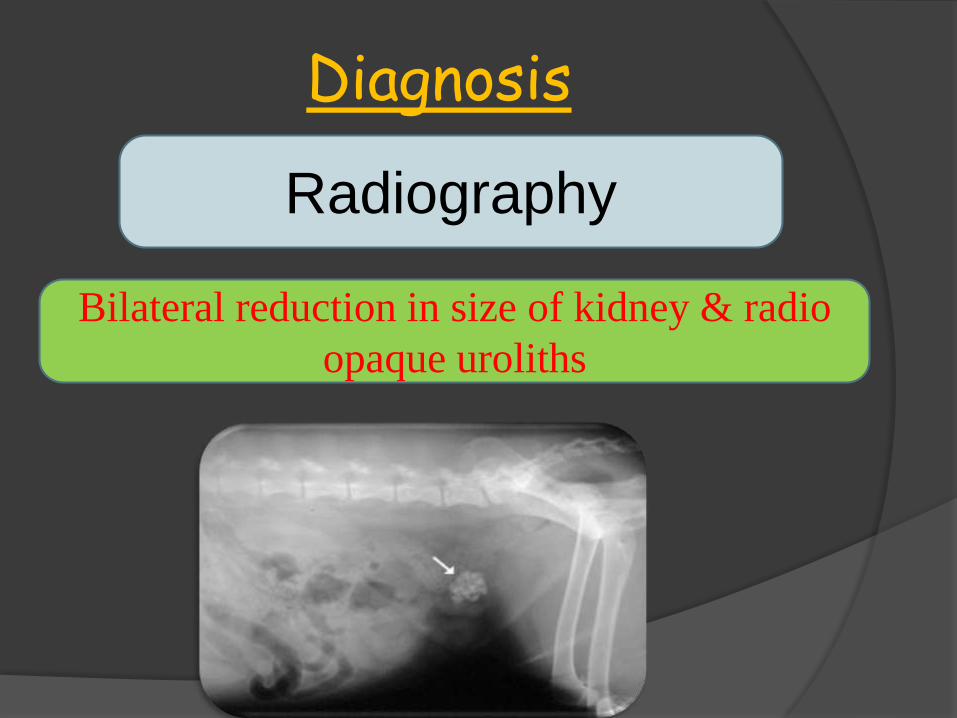
Diagnosis
Radiography
Bilateral reduction in size of kidney & radio
opaque uroliths
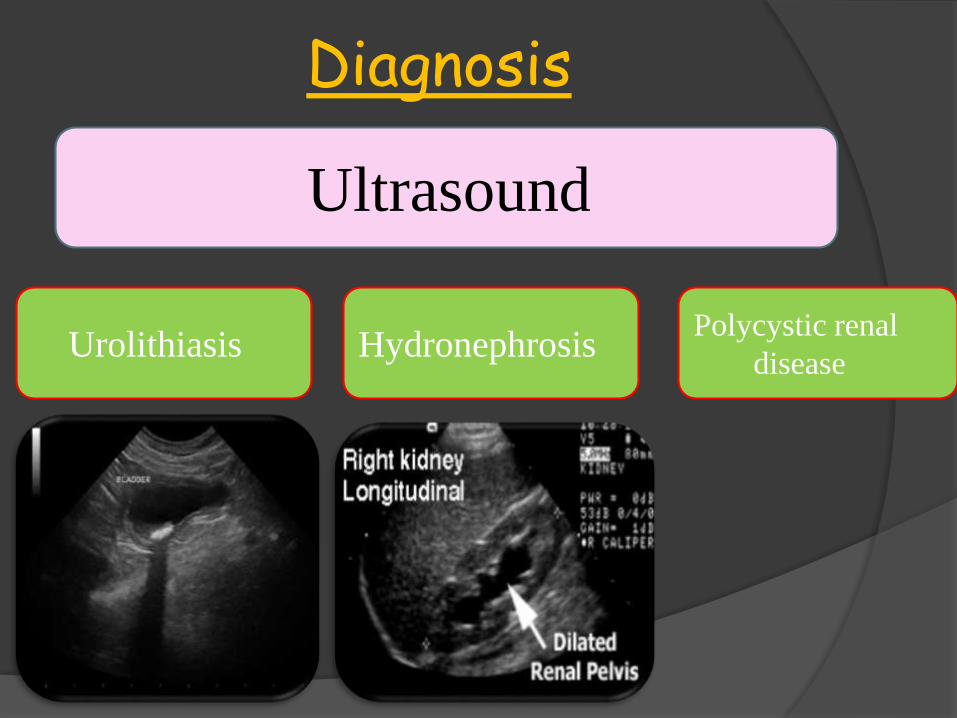
Diagnosis
Ultrasound
UrolithiasisPolycystic renal
disease Hydronephrosis
Management of CRF
Fluid therapy
Dietary restrictions
(protein; phosphorus) -
Protein intake should be
low but first class protein
should be provided to
prevent tissue breakdown.
Calcium supplements
Management of CRF
Blood pressure treatment: Angiotensinconverting enzyme (ace) inhibitors - e.g. enalapril / vasotec
Gastrointestinal protectant
Dialysis
Kidney transplant

Drug to be avoided in RF
Aminoglycosides
Nalidixic acid
Aspirin
Amphotericin
Neomycin
Nitrofurantoin,
Sulphonamides
Tetracycline and Magnesium salt
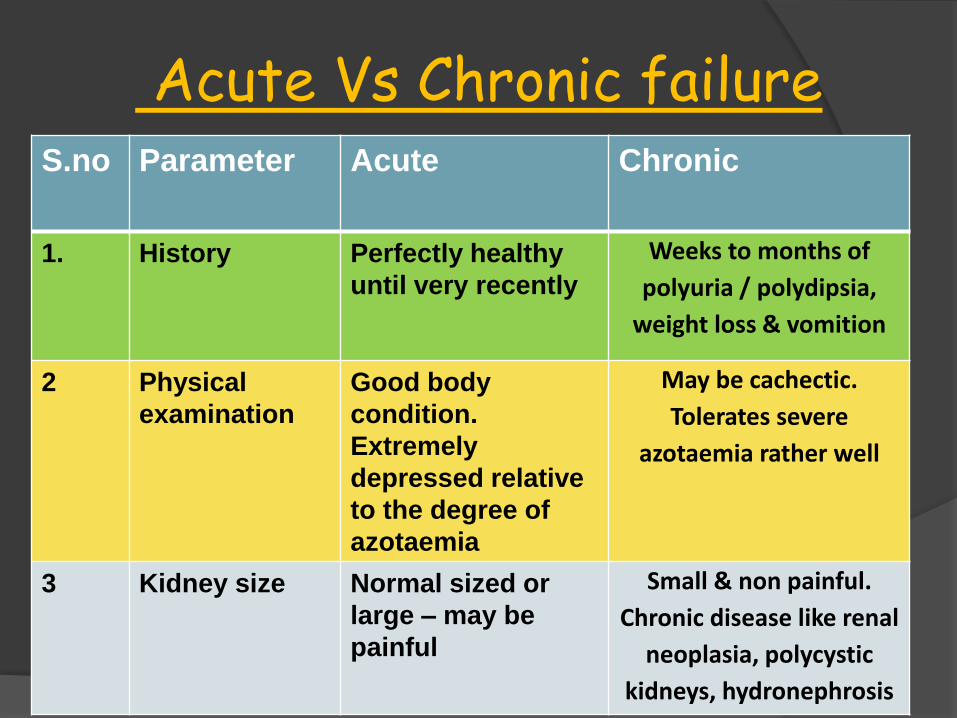
Acute Vs Chronic failure S.no Parameter Acute Chronic
1. History Perfectly healthy
until very recently
Weeks to months of
polyuria / polydipsia,
weight loss & vomition
2 Physical
examination
Good body
condition.
Extremely
depressed relative
to the degree of
azotaemia
May be cachectic.
Tolerates severe
azotaemia rather well
3 Kidney size Normal sized or
large – may be
painful
Small & non painful.
Chronic disease like renal
neoplasia, polycystic
kidneys, hydronephrosis
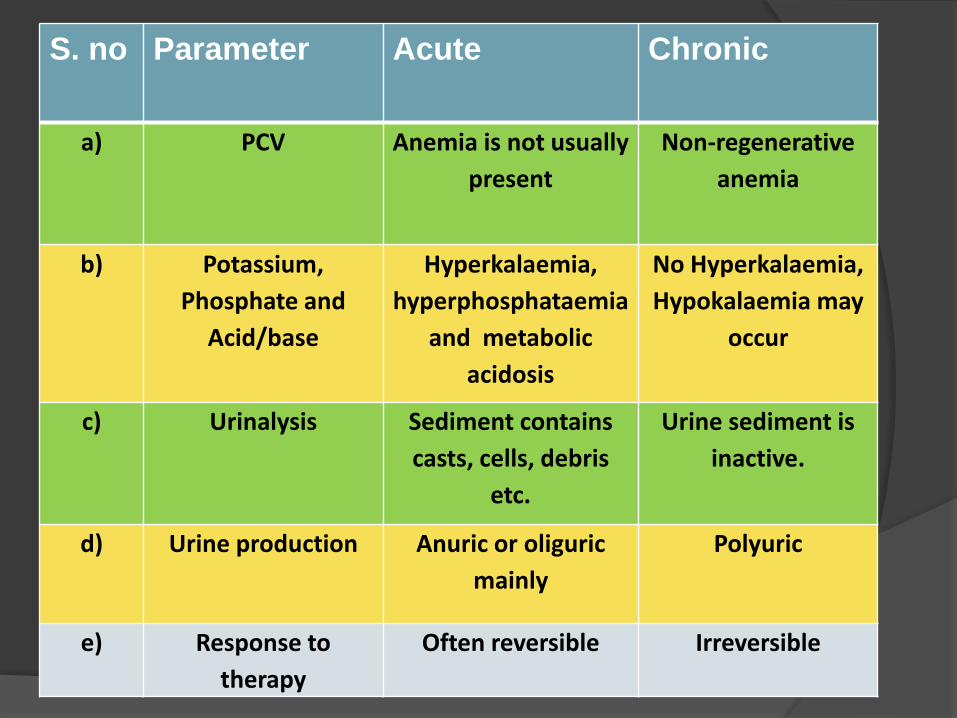
S. no Parameter Acute Chronic
a) PCV Anemia is not usually
present
Non-regenerative
anemia
b) Potassium,
Phosphate and
Acid/base
Hyperkalaemia,
hyperphosphataemia
and metabolic
acidosis
No Hyperkalaemia,
Hypokalaemia may
occur
c) Urinalysis Sediment contains
casts, cells, debris
etc.
Urine sediment is
inactive.
d) Urine production Anuric or oliguric
mainly
Polyuric
e) Response to
therapy
Often reversible Irreversible
Breeds prone to Renal Failure
Bull terrier
Doberman Pinscher

Breeds prone to RF
Lhasa Apso Norwegian Elkhound
Soft coated wheaten terrier

Breeds prone to RF
Standard poodle Cairn terrier
Beagle