Embed Size (px)
Citation preview

MAXILLOFACIAL TRAUMA
Even trivial blows to the face may
• compromise the airway
• directly or indirectly cause a head injury
• cervical spine injuries
Commonly from sporting activities, accidents and intentional violence.
INTRODUCTION
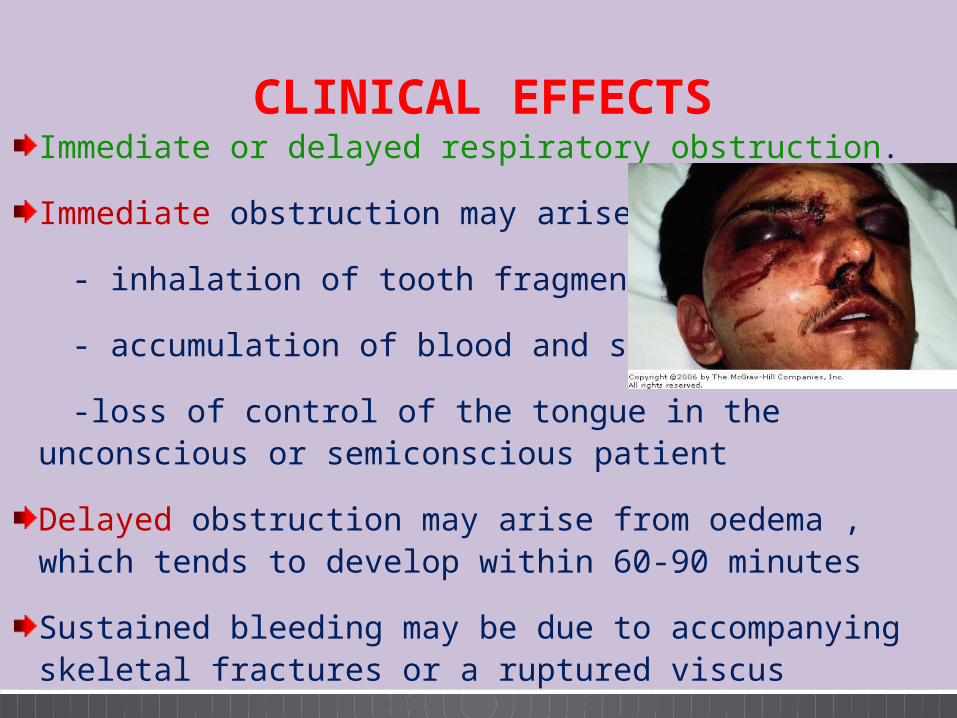
CLINICAL EFFECTSImmediate or delayed respiratory obstruction.
Immediate obstruction may arise from
- inhalation of tooth fragments
- accumulation of blood and secretions
-loss of control of the tongue in the unconscious or semiconscious patient
Delayed obstruction may arise from oedema , which tends to develop within 60-90 minutes
Sustained bleeding may be due to accompanying skeletal fractures or a ruptured viscus
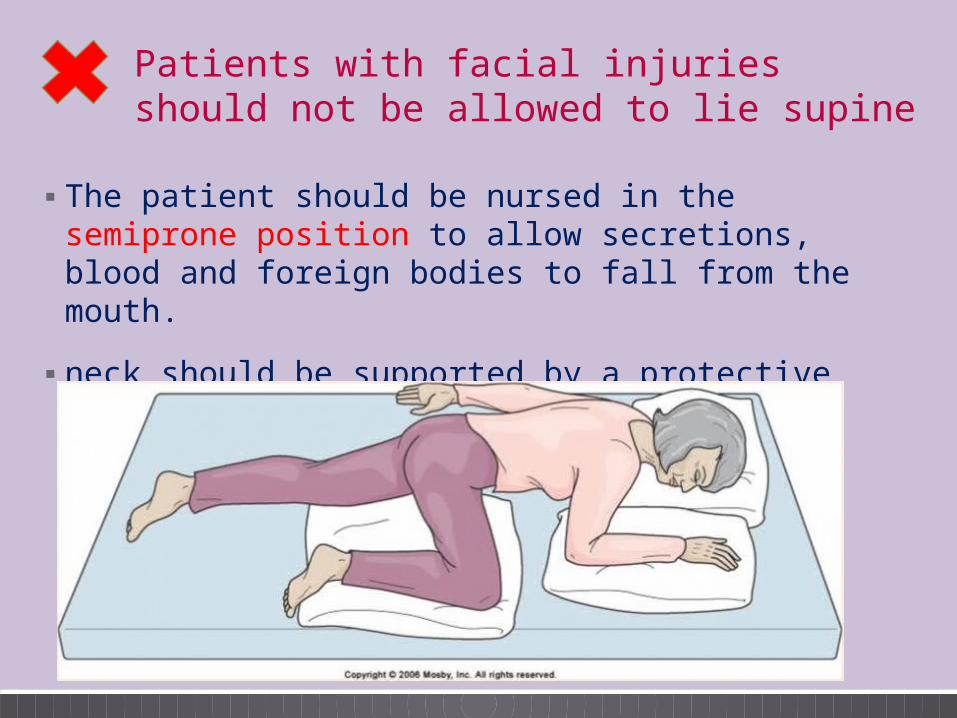
▪ The patient should be nursed in the semiprone position to allow secretions, blood and foreign bodies to fall from the mouth.
▪ neck should be supported by a protective collar
Patients with facial injuries should not be allowed to lie supine
EXAMINATION OF THE PATIENT
Lacerations and Soft tissue injuries
Systemic examination the bones
Dental Occlusion, Palpation of mouth
Cranial Nerves
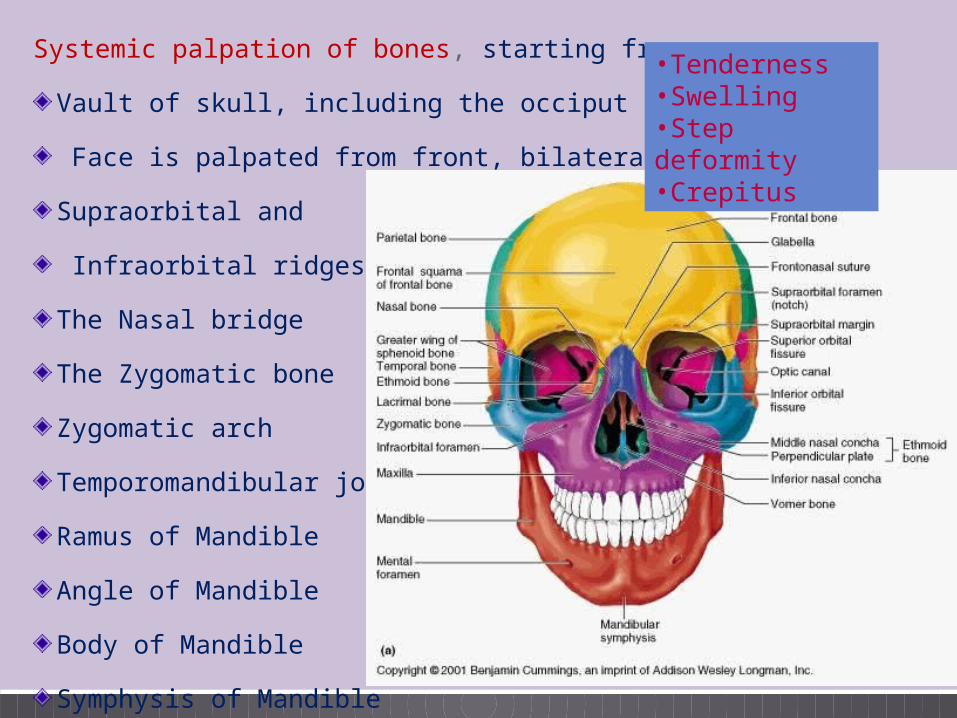
Systemic palpation of bones, starting from,
Vault of skull, including the occiput
Face is palpated from front, bilaterally from,
Supraorbital and
Infraorbital ridges
The Nasal bridge
The Zygomatic bone
Zygomatic arch
Temporomandibular joint
Ramus of Mandible
Angle of Mandible
Body of Mandible
Symphysis of Mandible
•Tenderness•Swelling•Step deformity •Crepitus
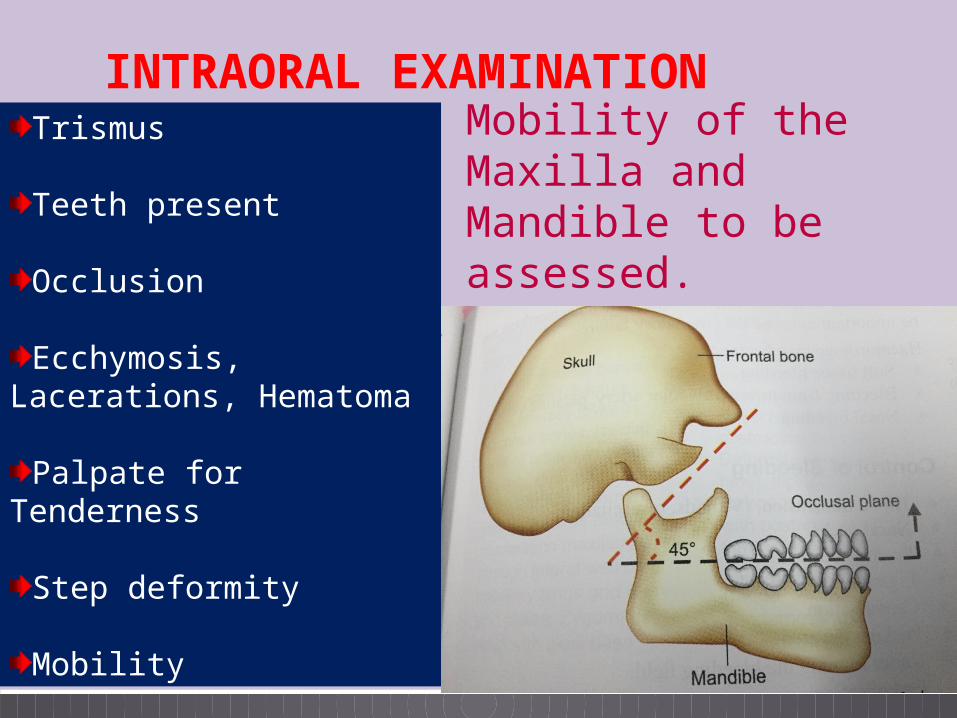
INTRAORAL EXAMINATIONTrismus
Teeth present
Occlusion
Ecchymosis, Lacerations, Hematoma
Palpate for Tenderness
Step deformity
Mobility
Mobility of the Maxilla and Mandible to be assessed.
CRANIAL NERVES▪Paresthesia suggests a fracture proximal along the course of nerve.
▪Facial nerve palsy fractured temporal bone / penetrating parotid injury
▪Pupil size and light reflexes
▪Diplopia
•Cheek , upper lip floor of orbit•Lower lip fracture of mandibular body
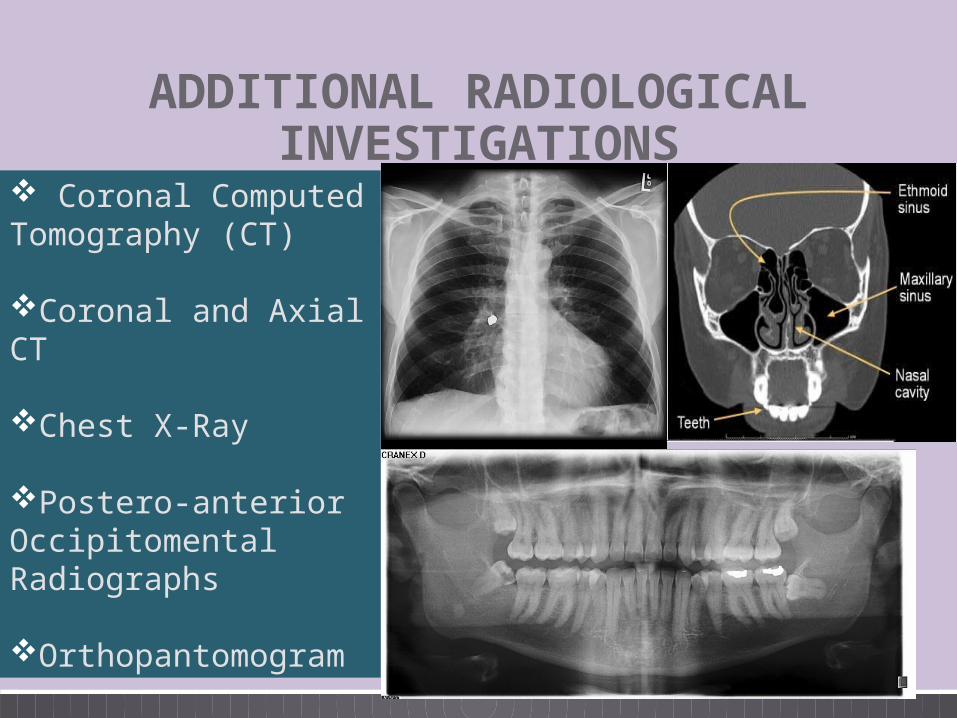
ADDITIONAL RADIOLOGICAL INVESTIGATIONS
Coronal Computed Tomography (CT)
Coronal and Axial CT
Chest X-Ray
Postero-anterior Occipitomental Radiographs
Orthopantomogram
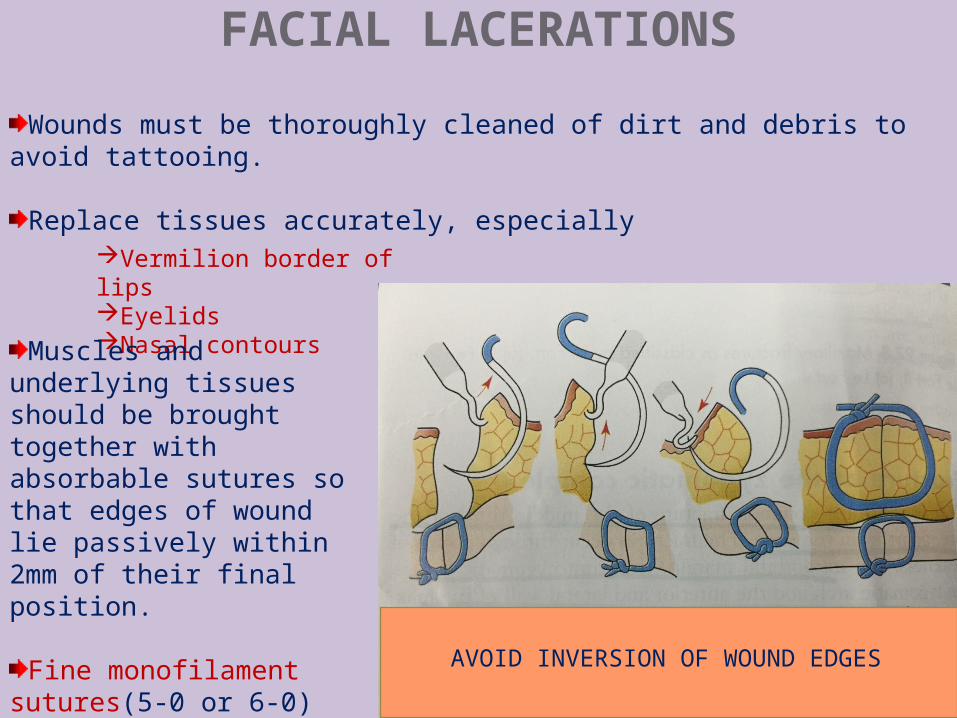
FACIAL LACERATIONS
Wounds must be thoroughly cleaned of dirt and debris to avoid tattooing.
Replace tissues accurately, especiallyVermilion border of lipsEyelidsNasal contours
Muscles and underlying tissues should be brought together with absorbable sutures so that edges of wound lie passively within 2mm of their final position.
Fine monofilament sutures(5-0 or 6-0) are used to bring the wound edges together
AVOID INVERSION OF WOUND EDGES
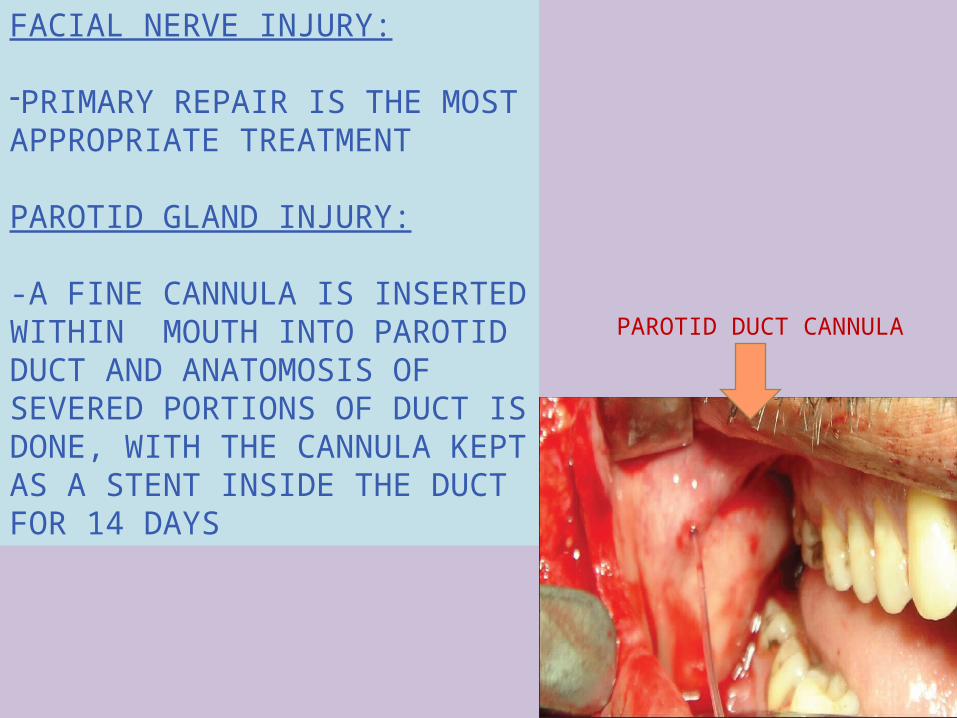
FACIAL NERVE INJURY:
-PRIMARY REPAIR IS THE MOST APPROPRIATE TREATMENT
PAROTID GLAND INJURY:
-A FINE CANNULA IS INSERTED WITHIN MOUTH INTO PAROTID DUCT AND ANATOMOSIS OF SEVERED PORTIONS OF DUCT IS DONE, WITH THE CANNULA KEPT AS A STENT INSIDE THE DUCT FOR 14 DAYS
PAROTID DUCT CANNULA
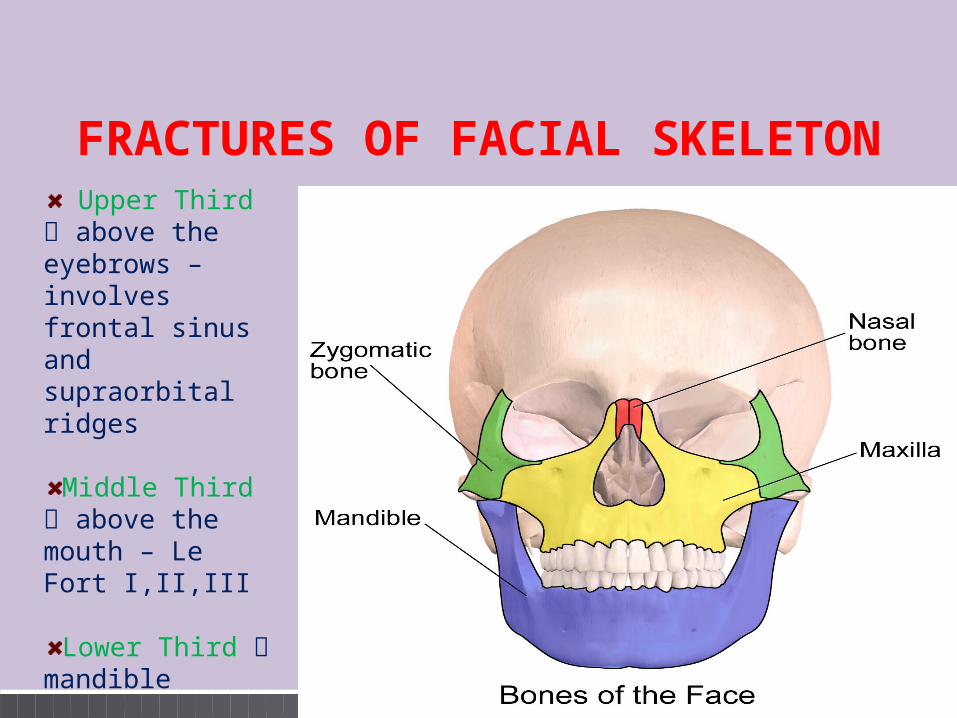
FRACTURES OF FACIAL SKELETON Upper Third
above the eyebrows – involves frontal sinus and supraorbital ridges
Middle Third above the mouth – Le Fort I,II,III
Lower Third mandible
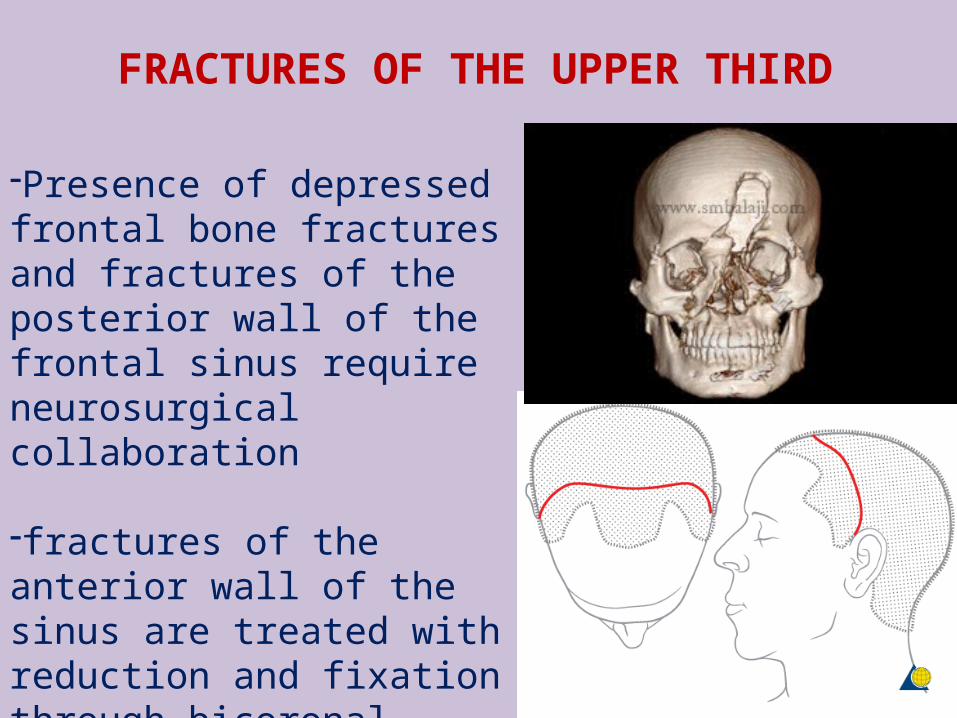
-Presence of depressed frontal bone fractures and fractures of the posterior wall of the frontal sinus require neurosurgical collaboration
-fractures of the anterior wall of the sinus are treated with reduction and fixation through bicoronal scalp flap
FRACTURES OF THE UPPER THIRD
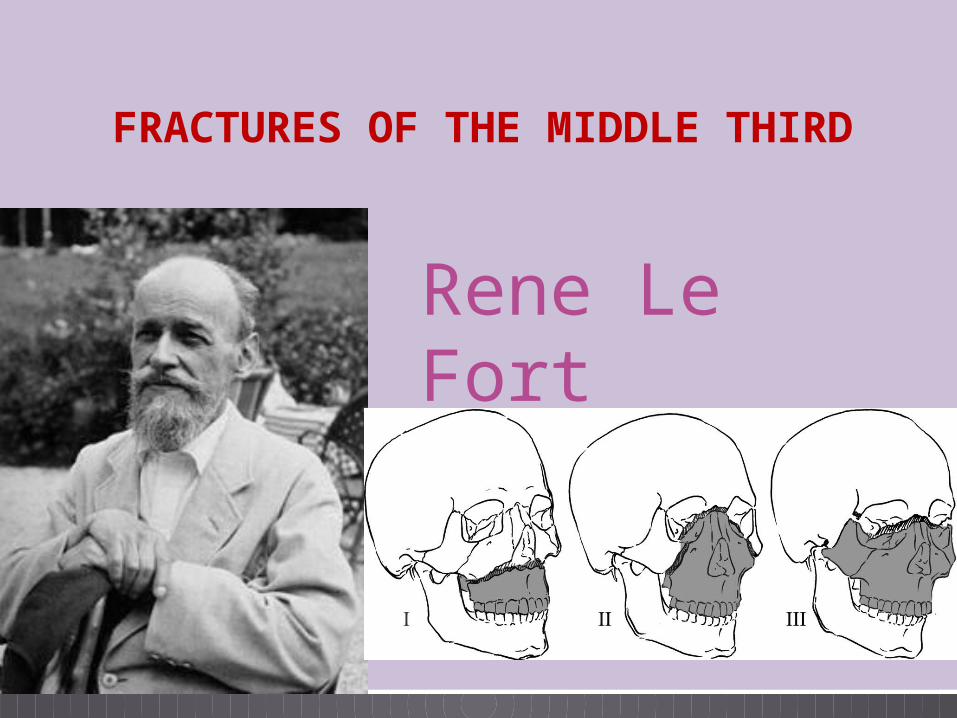
Rene Le Fort
FRACTURES OF THE MIDDLE THIRD
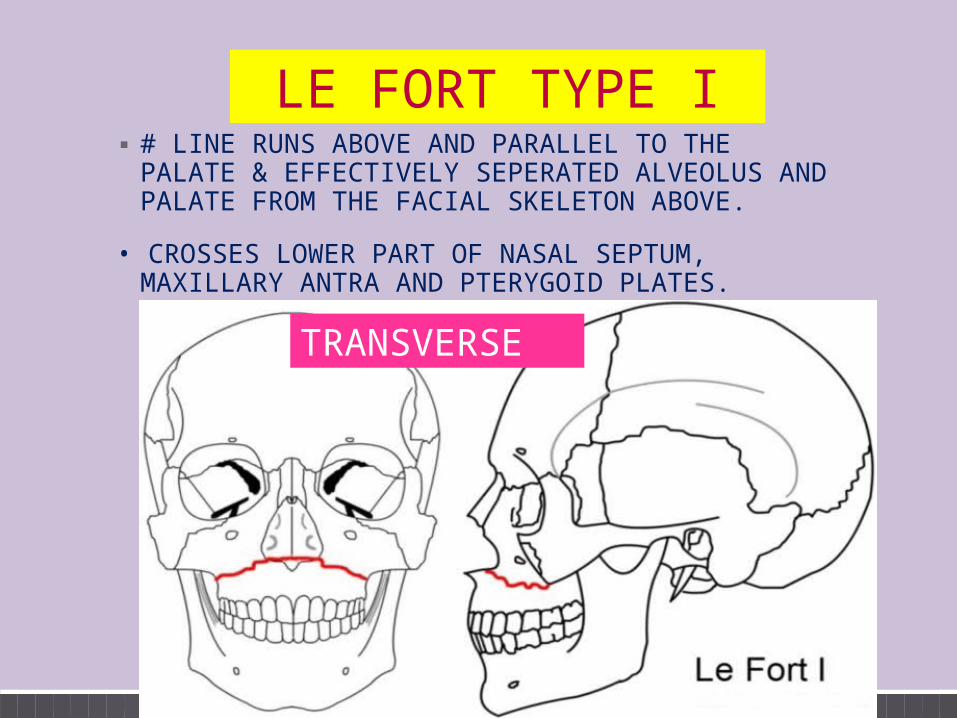
LE FORT TYPE I▪ # LINE RUNS ABOVE AND PARALLEL TO THE PALATE
& EFFECTIVELY SEPERATED ALVEOLUS AND PALATE FROM THE FACIAL SKELETON ABOVE.
• CROSSES LOWER PART OF NASAL SEPTUM, MAXILLARY ANTRA AND PTERYGOID PLATES.
TRANSVERSE
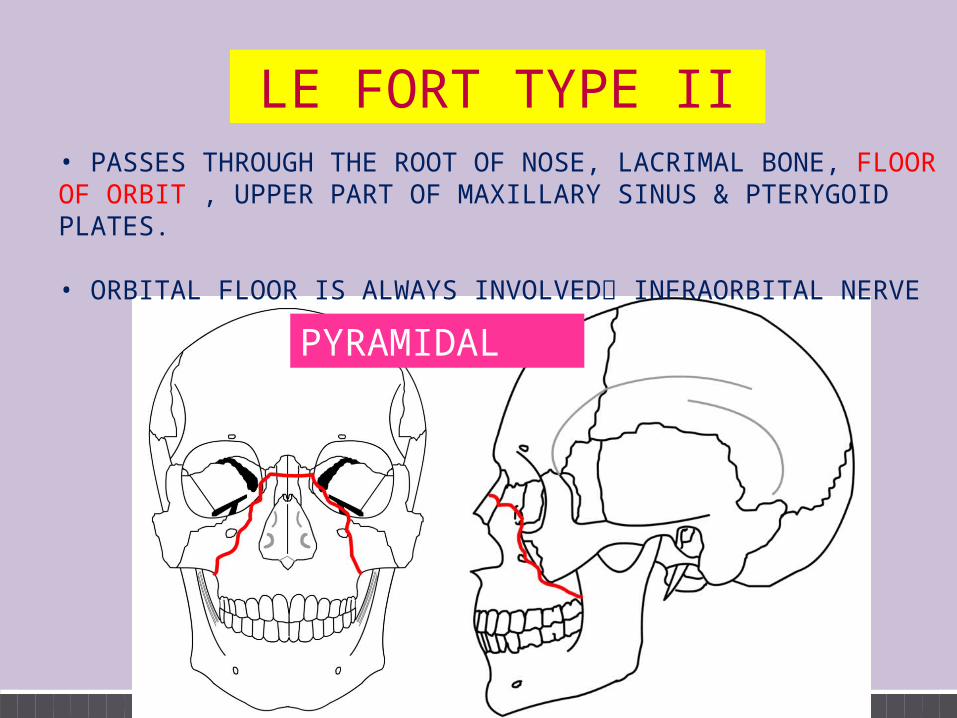
LE FORT TYPE II• PASSES THROUGH THE ROOT OF NOSE, LACRIMAL BONE, FLOOR OF ORBIT , UPPER PART OF MAXILLARY SINUS & PTERYGOID PLATES.
• ORBITAL FLOOR IS ALWAYS INVOLVED INFRAORBITAL NERVE
PYRAMIDAL
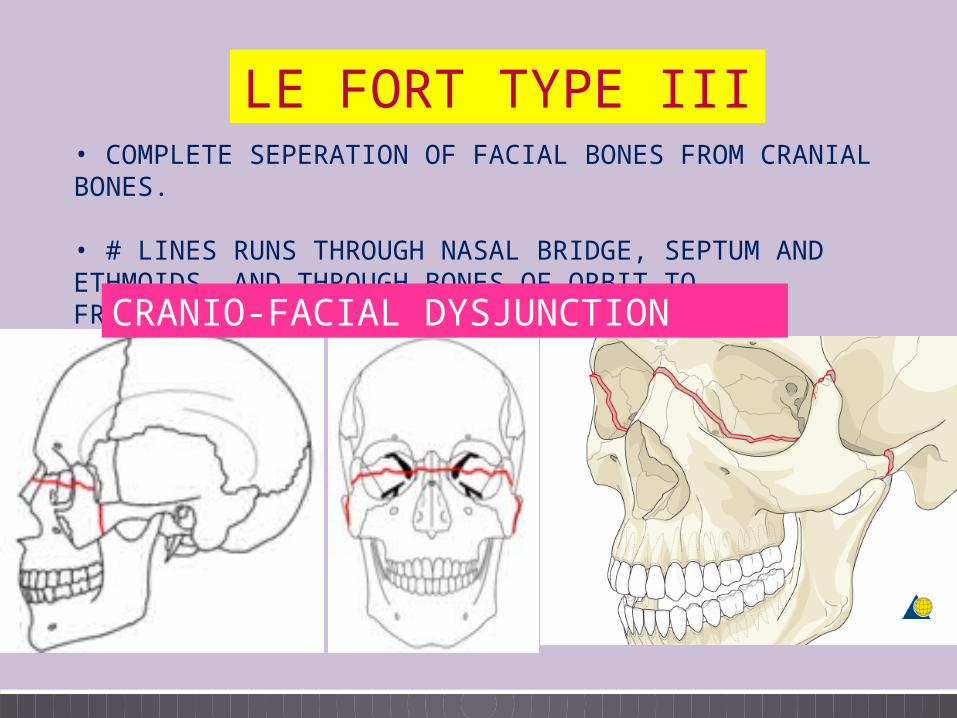
LE FORT TYPE III• COMPLETE SEPERATION OF FACIAL BONES FROM CRANIAL BONES.
• # LINES RUNS THROUGH NASAL BRIDGE, SEPTUM AND ETHMOIDS, AND THROUGH BONES OF ORBIT TO FRONTOZYGOMATIC SUTURE.CRANIO-FACIAL DYSJUNCTION
TREATMENT•Upper part of face is first stabilised by bicoronal approach at the vault of the skull
•Incisions in the lower eyelid are used to explore fractures of orbital floor
•Lower part of Maxilla is approached through a gingival sulcus incison above maxillary teeth.
•Reduction of Maxilla with Rowe’s disimpaction forceps which grasp the palate between the nasal and palatal mucosa
■ Intermaxillary fixation screws or dental arch bars or eyelet wires may be needed to achieve the correct occlusion
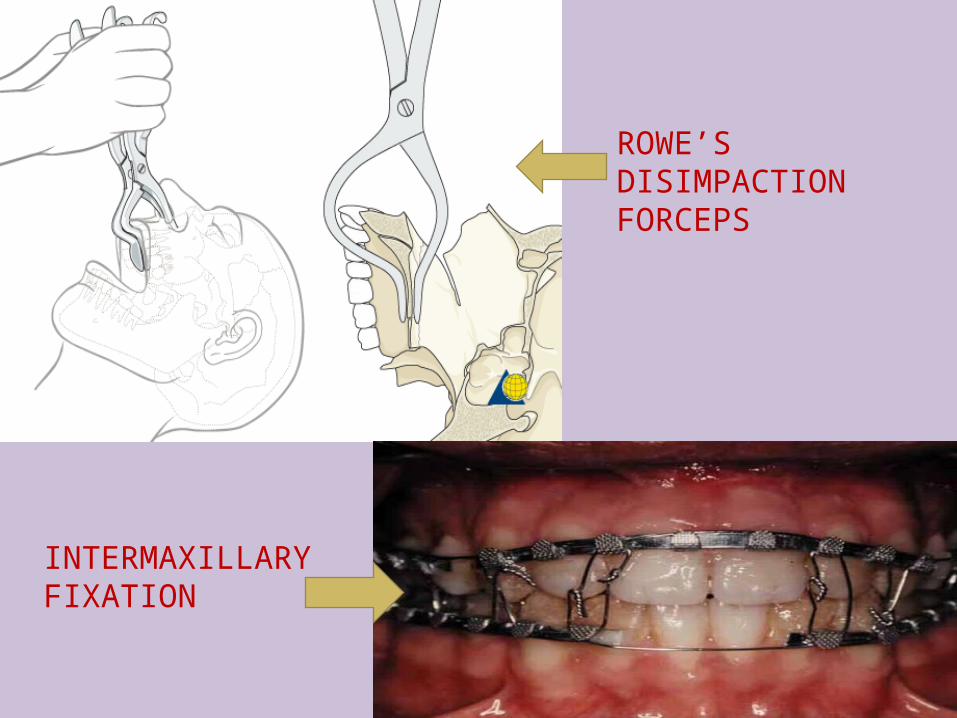
ROWE’S DISIMPACTION FORCEPS
INTERMAXILLARY FIXATION
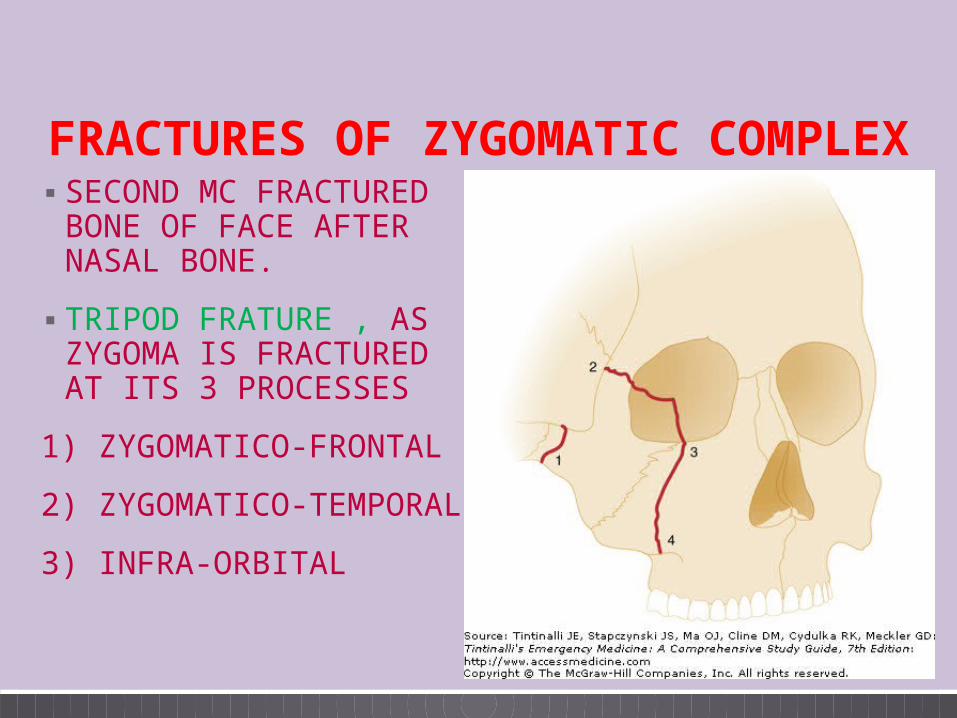
▪ SECOND MC FRACTURED BONE OF FACE AFTER NASAL BONE.
▪ TRIPOD FRATURE , AS ZYGOMA IS FRACTURED AT ITS 3 PROCESSES
1) ZYGOMATICO-FRONTAL
2) ZYGOMATICO-TEMPORAL
3) INFRA-ORBITAL
FRACTURES OF ZYGOMATIC COMPLEX
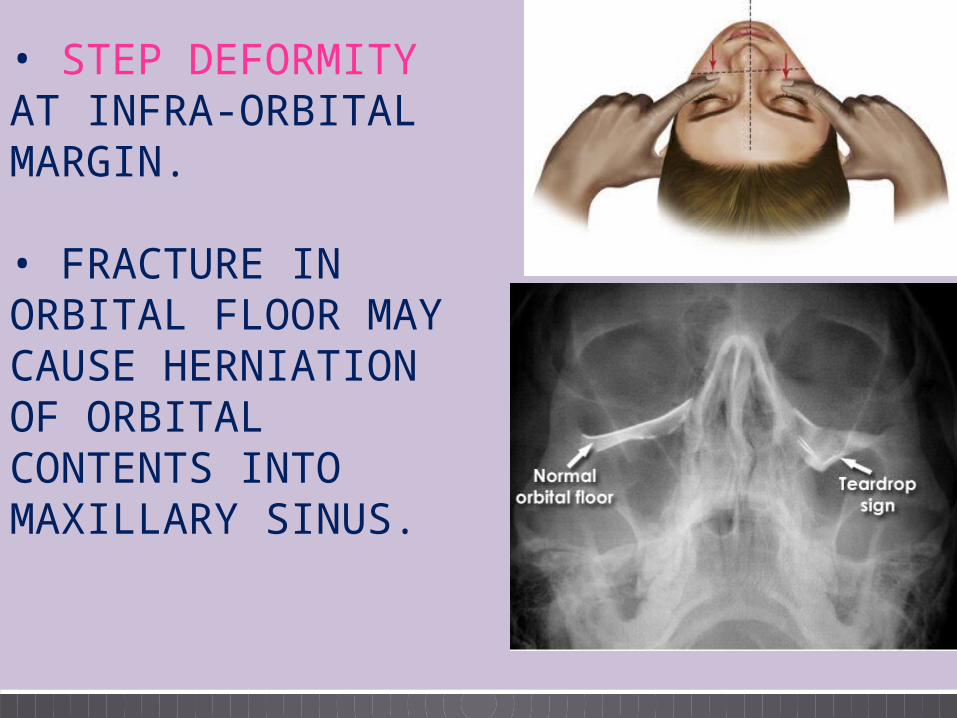
• STEP DEFORMITY AT INFRA-ORBITAL MARGIN.
• FRACTURE IN ORBITAL FLOOR MAY CAUSE HERNIATION OF ORBITAL CONTENTS INTO MAXILLARY SINUS.
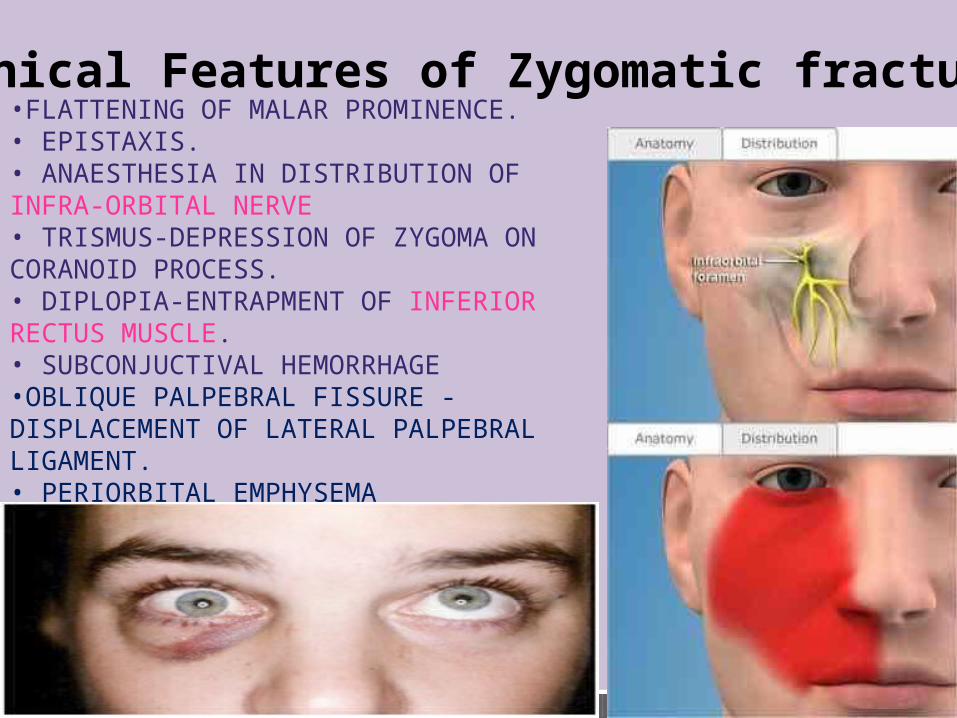
•FLATTENING OF MALAR PROMINENCE.• EPISTAXIS.• ANAESTHESIA IN DISTRIBUTION OF INFRA-ORBITAL NERVE• TRISMUS-DEPRESSION OF ZYGOMA ON CORANOID PROCESS.• DIPLOPIA-ENTRAPMENT OF INFERIOR RECTUS MUSCLE.• SUBCONJUCTIVAL HEMORRHAGE•OBLIQUE PALPEBRAL FISSURE -DISPLACEMENT OF LATERAL PALPEBRAL LIGAMENT.• PERIORBITAL EMPHYSEMA
Clinical Features of Zygomatic fracture
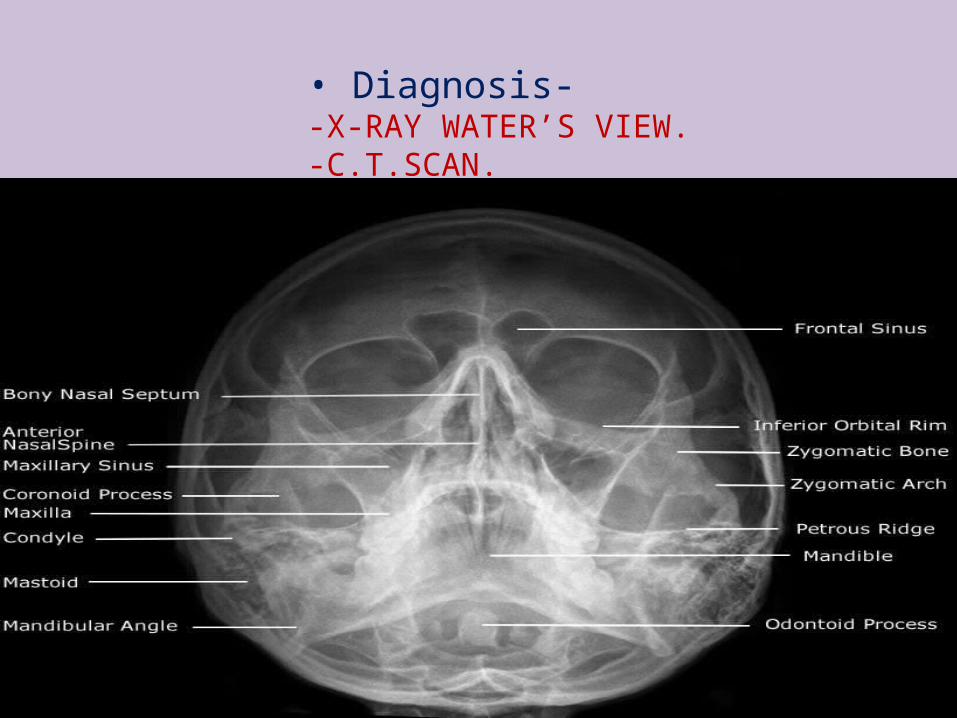
• Diagnosis--X-RAY WATER’S VIEW.-C.T.SCAN.
T REATMENT
• Gillies temporal approachan incision in the hairline, superficial to the temporal fossa, about 15 mm long, at 45° to the vertical.
•Zygomatic arch is elevated by Bristow or Rowe elevator
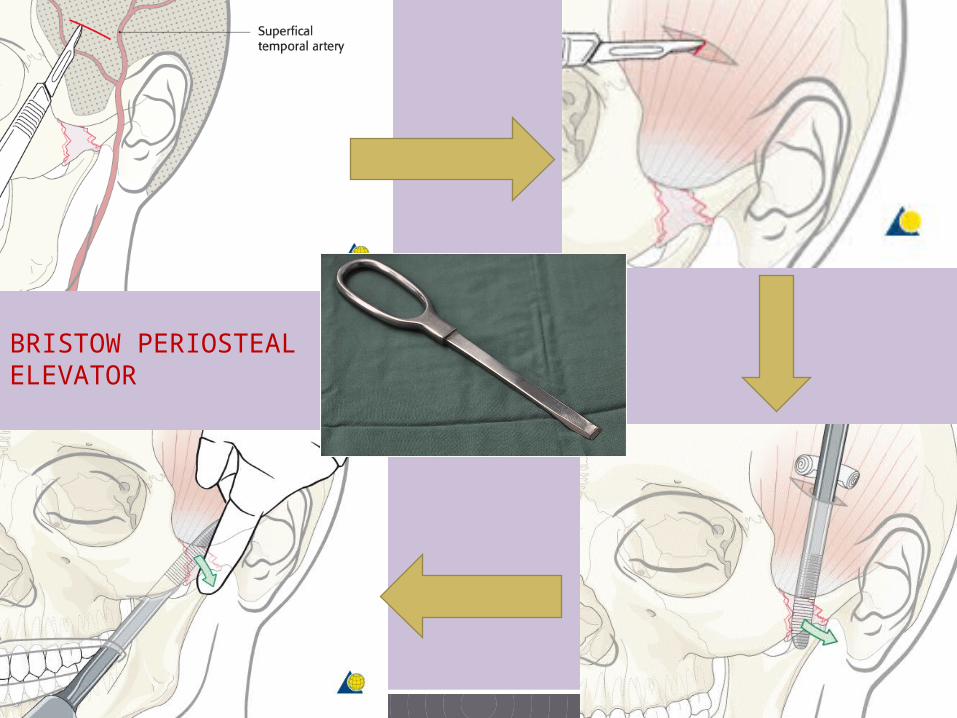
BRISTOW PERIOSTEAL ELEVATOR
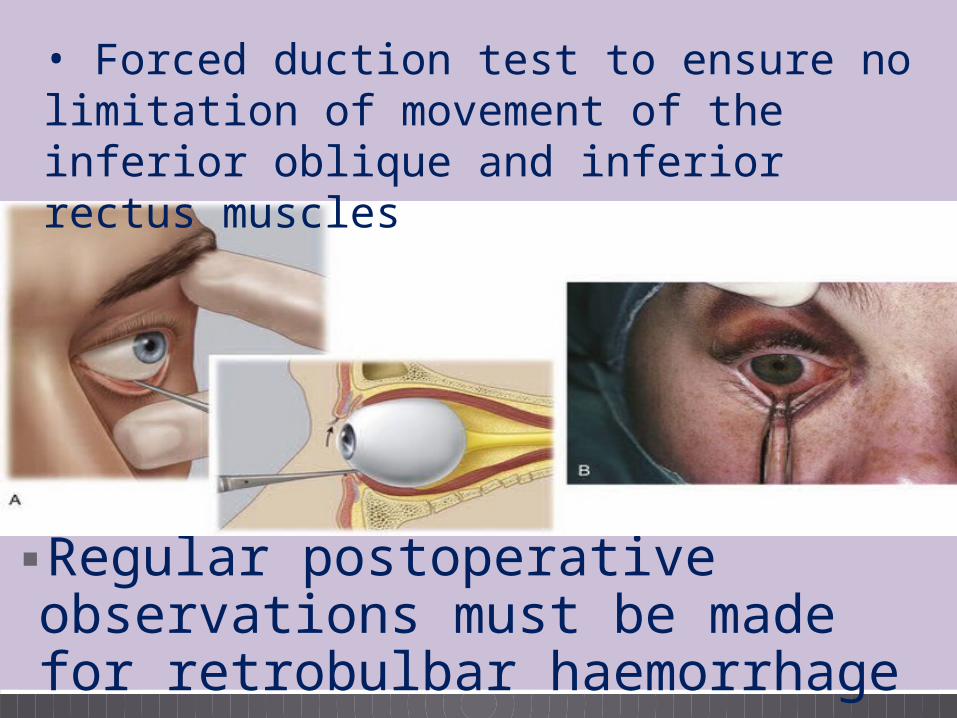
▪Regular postoperative observations must be made for retrobulbar haemorrhage
• Forced duction test to ensure no limitation of movement of the inferior oblique and inferior rectus muscles
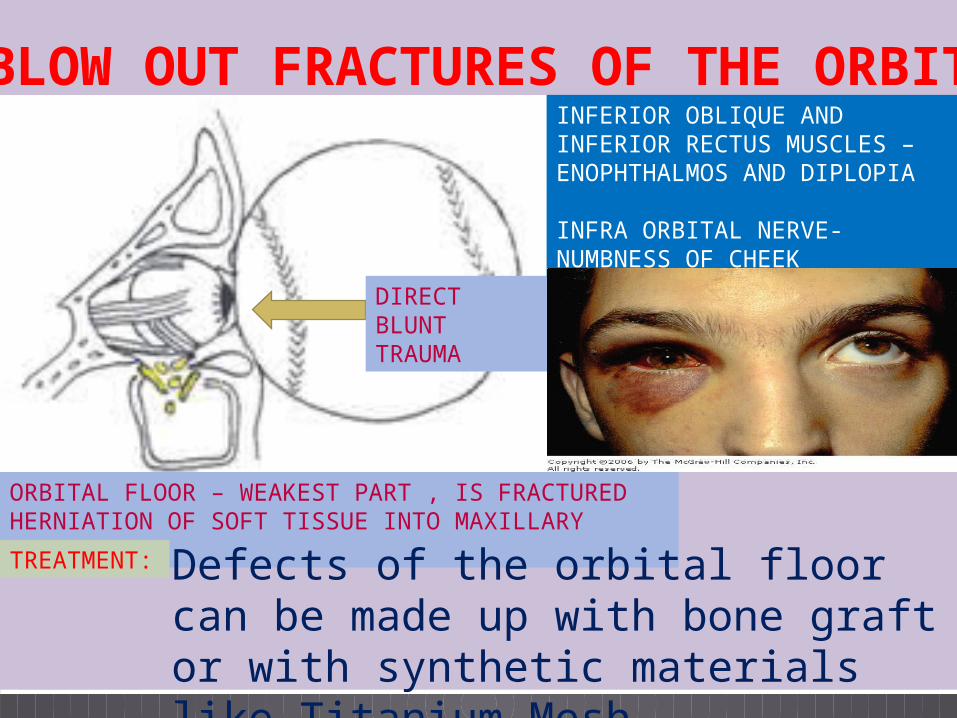
BLOW OUT FRACTURES OF THE ORBIT
DIRECT BLUNT TRAUMA
ORBITAL FLOOR – WEAKEST PART , IS FRACTURED HERNIATION OF SOFT TISSUE INTO MAXILLARY ANTRUM
INFERIOR OBLIQUE AND INFERIOR RECTUS MUSCLES – ENOPHTHALMOS AND DIPLOPIA
INFRA ORBITAL NERVE- NUMBNESS OF CHEEK
TREATMENT: Defects of the orbital floor can be made up with bone graft or with synthetic materials like Titanium Mesh.
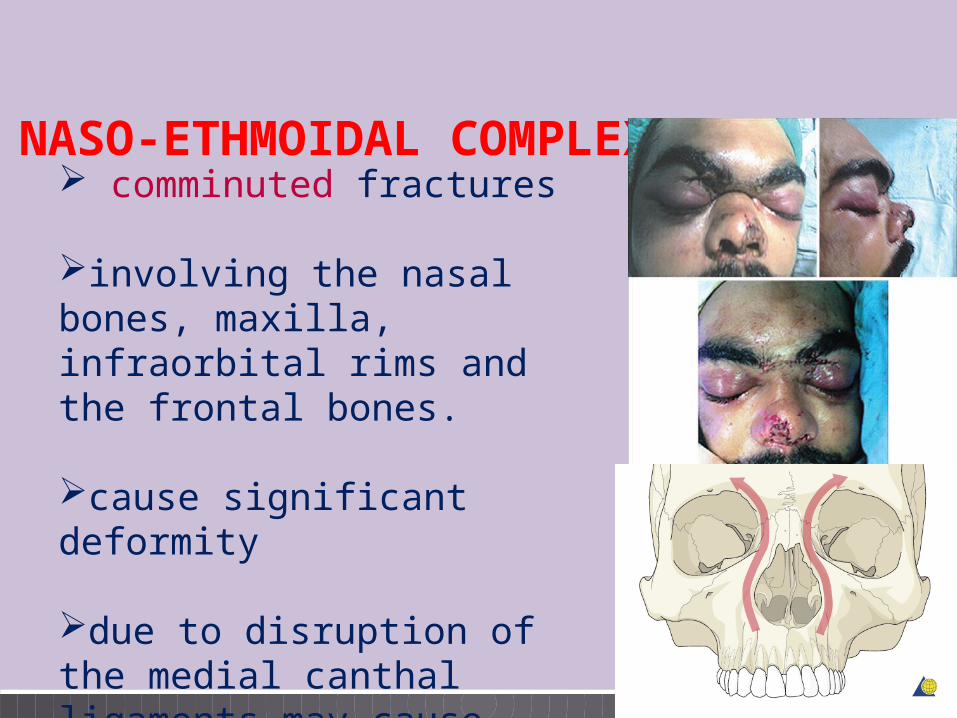
NASO-ETHMOIDAL COMPLEX FRACTURES
comminuted fractures
involving the nasal bones, maxilla, infraorbital rims and the frontal bones.
cause significant deformity
due to disruption of the medial canthal ligaments may cause traumatic telecanthus (widened intercanthal distance)
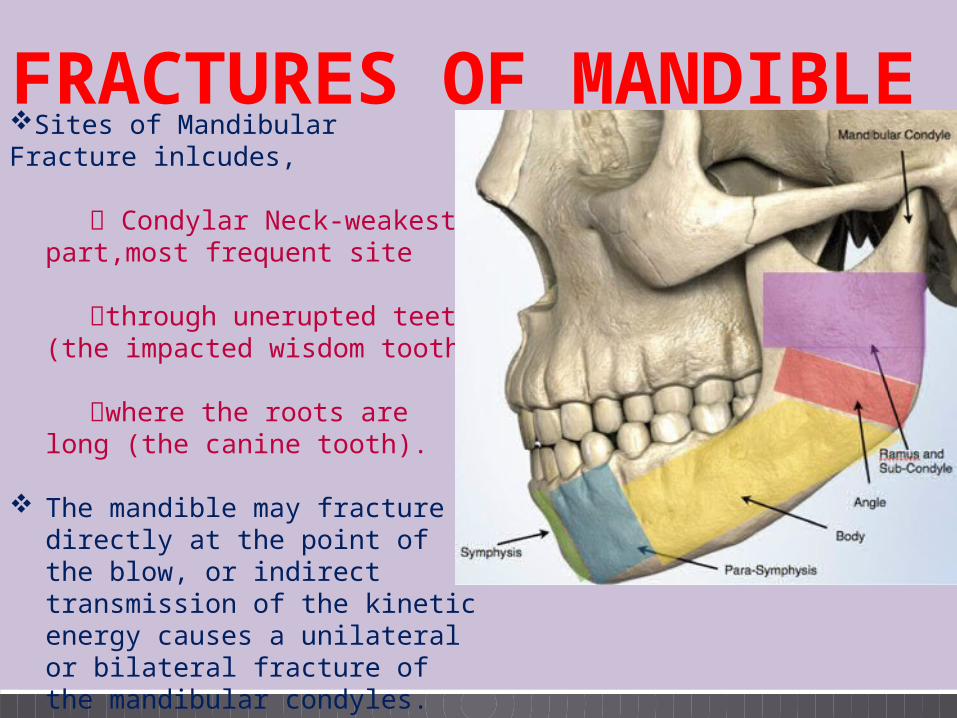
FRACTURES OF MANDIBLESites of Mandibular Fracture inlcudes, Condylar Neck-weakest
part,most frequent site
through unerupted teeth (the impacted wisdom tooth)
where the roots are long (the
canine tooth).
The mandible may fracture directly at the point of the blow, or indirect transmission of the kinetic energy causes a unilateral or bilateral fracture of the mandibular condyles.
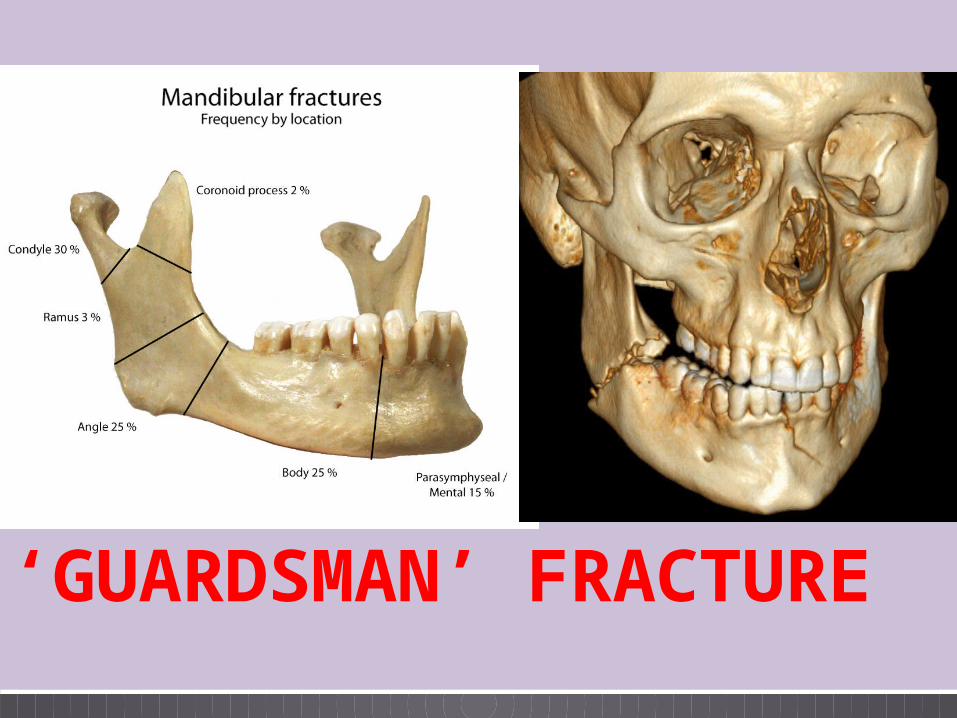
‘GUARDSMAN’ FRACTURE
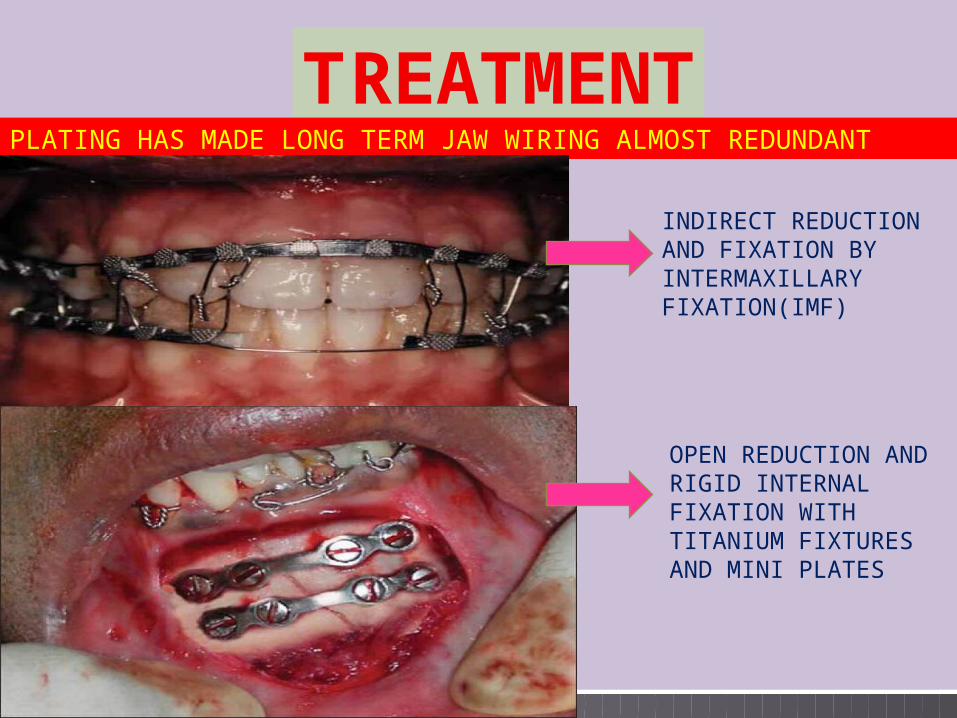
T REATMENTPLATING HAS MADE LONG TERM JAW WIRING ALMOST REDUNDANT
INDIRECT REDUCTION AND FIXATION BY INTERMAXILLARY FIXATION(IMF)
OPEN REDUCTION AND RIGID INTERNAL FIXATION WITH TITANIUM FIXTURES AND MINI PLATES
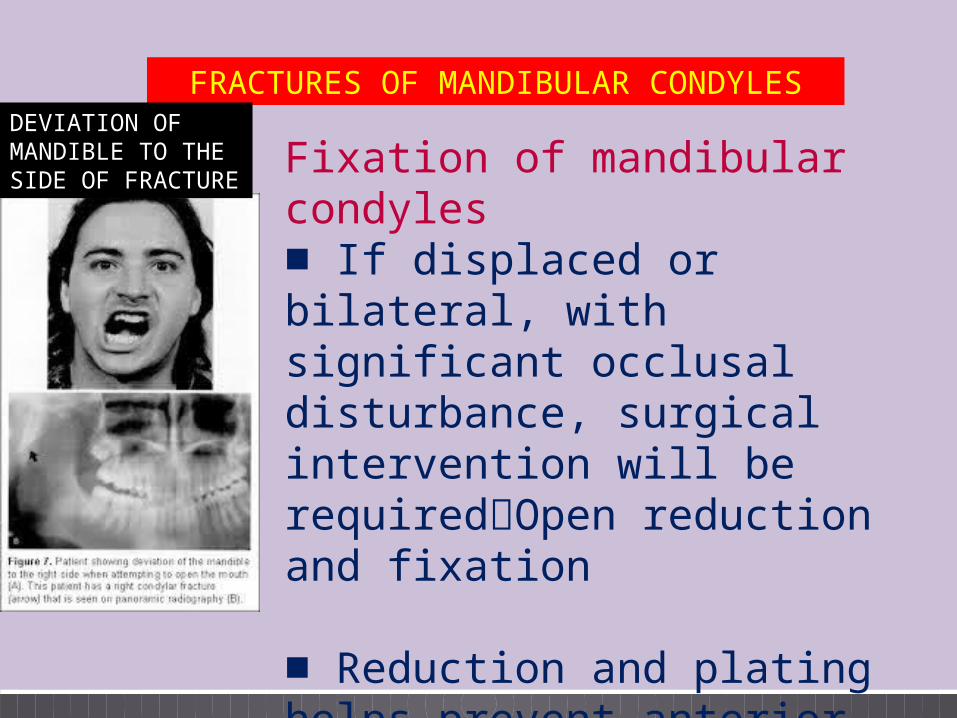
FRACTURES OF MANDIBULAR CONDYLESDEVIATION OF MANDIBLE TO THE SIDE OF FRACTURE
Fixation of mandibular condyles■ If displaced or bilateral, with significant occlusal disturbance, surgical intervention will be requiredOpen reduction and fixation
■ Reduction and plating helps prevent anterior open bite, due to malocculsion
FACIAL INJURIES MAY CAUSE EITHER IMMEDIATE OR DELAYED RESPIRATORY OBSTRUCTION
SEMIPRONE POSITION
AVOID INVERSION OF WOUND EDGES IN SUTURING FACIAL LACERATIONS
FRACTURE OF MAXILLA – LE FORT TYPE I – TRANSVERSE #, TYPE 2- PYRAMIDAL , TYPE 3 – CRANIOFACIAL DYSJUNCTION
ZYGOMATIC FRACTURES ARE TRIPOD FRACTURES
THE CONDYLAR NECK IS THE WEAKEST PART AND MOST COMMON SITE OF MANDIBULAR FRACTURE
SUMMARY
CONCLUSIONProphylactic antibiotics like penicillin / amoxycillin and metronidazone should be given in all facial fractures
Dexamethasone may help to reduce facial oedema
Air bag provision, seat belts, laminated windscreens, and drink/drive laws help to reduce the orofacial injuries