Embed Size (px)
DESCRIPTION
Med viva/revision for Anaes M.Med Part 2
Citation preview

Medical Viva

Diagnosis?

Define QT interval

Define QT intervalTime from the start of the Q wave to the end of the T wave.

What does the QT interval represent?

What does the QT interval represent?
It represents the time taken for ventricular depolarisation and repolarisation.

How does QT relate to the heart rate?

How does QT relate to the heart rate?
QT interval is inversely proportional to heart rate

Why does QT needs to be corrected?

Why does QT needs to be corrected?
This allows comparison of QT values at different heart rates and improves detection of patients at increased risk of arrhythmias.

So what is it corrected to?

So what is it corrected to?
Corrected QT interval (QTc) estimates the QT interval at a heart rate of 60 bpm.

What is the problem with prolonged QTc?

What is the problem with prolonged QTc?
An abnormally prolonged QT is associated with an increased risk of ventricular arrhythmias, especially Torsades de Pointes.

What is normal QTc?

What is normal QTc?< 440ms in men
< 460ms in women

Name me a formula for calculation.

Name me a formula for calculation.
QTC = QT / √ RR

What is the formula called?

What is the formula called?Bazett’s formula

What is the limitation of Bazett’s formula?

What is the limitation of Bazett’s formula?
It over-corrects at heart rates > 100 bpm under-corrects at heart rates < 60 bpm,
(but provides an adequate correction for heart rates ranging from 60 – 100 bpm).

Name some causes of prolonged QTc

Name some causes of prolonged QTc
Hypo-MCTMI
High ICPDrugs

Does hypokalemia cause prolonged QTc?

Does hypokalemia cause prolonged QTc?
Technically no. U wave may cause apparent proloned QTc.
But risk of TdP not there. Severe hypokalemia = asystole, remember?

Name some drugs which cause
prolonged QTc.

Name some drugs which cause
prolonged QTc.OndansetronDroperidol
DiphenhydramineErythromycinAmiodarone

What is shortened QTc?

What is shortened QTc?
< 350ms

Names some causes

Name some causesHypercalcaemia
DigoxinCongential short QT syndrome

Any problems with short QT?

Any problems with short QT?
increased risk of paroxysmal atrial and ventricular fibrillationsudden cardiac death.

BREAK

Diagnosis?
70 year old male. Hypertension. Otherwise asymptomatic.

Brugada

Problem with Brugada?

Problem with Brugada?
Sudden cardiac death

Brugada SignCoved ST segment elevation >2mm in >1 of
V1-V3
followed by a negative T wave

How many types of Brugada?

How many types of Brugada?
3 types:
Type 1: Brugada Sign + Clinical criteria(Documented VT or VF. Family history of sudden cardiac death at <45 years old .Coved-type ECGs in family members. Inducibility of VT with
programmed electrical stimulation. Syncope. Nocturnal agonal respiration.)
Type 2: Type 2 has >2mm of saddleback shaped ST elevation
Type 3: morphology of either type 1 or type 2, but with <2mm of ST segment elevation

Pathophysiology of Brugada?

Pathophysiology of Brugada?
Mutation in the cardiac sodium channel gene.

Treatment of Brugada?

Treatment of Brugada?
AICD implantation

What anaesthetic drug to use with
caution in Brugada?

What anaesthetic drug to use with
caution in Brugada?Propofol!

BREAK

Diagnosis

Inferior infarct + posterior infarct

What else should you look out for?

What else should you look out for?
RV infarct and heart block
Inferior infarct: must look for posterior infarct (V1-3)Inferior infarct: must look for RV infarct

How to diagnose RV infarct with ECG?

How to diagnose RV infarct with ECG?
rV4

Describe the position of rV4

Describe the position of rV4
V4 position on right side

What is significant change in rV4 to be called an RV STEMI?

What is significant change in rV4 to be called an RV STEMI?
0.5 mm or half a square.
Why?

How does the management of RV infarct differ from LV
infarct?

How does the management of RV infarct differ from LV
infarct?Fluid responsive therefore fluid loading may help BP.
Avoid nitrates.

Describe other lead positions you can
place

Describe other lead positions you can
placeV7,8,9

Where are V7,8 and 9 placed?

Where are V7,8 and 9 placed?
Posterior, below scapula along 6th IC space

What is V7,8,9 good for?

What is V7,8,9 good for?
Diagnosis of posterior infarct.

What is the recommended door
to balloon time?

What is the recommended door
to balloon time?60 min

What is the difference between BMS and
DES?

What is the difference between BMS and
DES?Bare metal – more thrombogenic but epithelization more rapid.
Earlier thrombosisDual anti-platelet shorter.
DES – less thrombogenic but epithelization slowerLess thrombosis
Dual anti-platelet longer.

Recommended BMS DAP duration

Recommended BMS DAP duration
4 weeks

BREAK

Diagnosis?

Patient’s asymptomatic. Management?

Patient’s asymptomatic. Management?
Refer EPS

ECG repeated: BP 120/80. Tx?

StableVagal maneuvers
AmiodaroneFleclanide
Procainamide

ECG repeated: BP 70/40. Tx?

UnstableSynchronized cardioversion

Data Intepretation34 yo female intubated and ventilated following
a prolonged generalized tonic-clonic seizure. Initial non-contrast CT brain shows bilateral intracerebral haemorrhages. ABG and GBC post intubation:

Data IntepretationList the abnormalities on the ABG and give the
most likely cause in each case.

Data Intepretation Metabolic acidosis – lactic acidosis induced by
prolonged seizure Respiratory acidosis / inadequate compensation –
inappropriate mechanical ventilation Increased A-a gradient – aspiration pneumonitis
or neurogenic pulmonary oedema

Data Intepretation Give three possible diagnoses for her
presentation based on the history and investigations.

Data Intepretation TTP / HUS Eclampsia Vasculitis

Difference between TTP and HUS?

Difference between TTP and HUS?
TTP : more brain, adult female
HUS: more kidneys, kids, related to E. coli

BREAK

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What is the likely diagnosis?

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What is the likely diagnosis? Supratherapeutic warfarinisation

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What are possible causes of supratherapeutic warfarinisation?

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What are possible causes of supratherapeutic warfarinisation? Overdose Drug interaction Change in diet

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What are possible drug interactions causing high INR in this patient?

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What are possible drug interactions causing high INR in this patient? Antibiotics Omeprazole Amiodarone

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What is the likeliest mechanism for antibiotics to cause high INR in this patient?

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What is the likeliest mechanism for antibiotics to cause high INR in this patient?
Vitamin K metabolism altered due to change in gut flora.

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What is the likeliest mechanism for omeprazole to cause high INR in this patient?

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
What is the likeliest mechanism for omeprazole to cause high INR in this patient?
Liver enzyme inhibition

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
Outline your management of this patient if not bleeding.

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
Outline your management of this patient if not bleeding. Stop warfarin Vitamin K in as low a dose as possible Consider FFP or factor concentrate if high risk of
bleeding

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
How much FFP should be given?

Data Intepretation68-year-old male with chronic AF is noted to
have the following coagulation profile:
How much FFP should be given? At least 10-15ml/kg.

Data IntepretationABG obtained from a patient admitted to the
ICU after a suicide attempt.
What anomaly do you notice in the blood gas report?

Data IntepretationABG obtained from a patient admitted to the
ICU after a suicide attempt.
What anomaly do you notice in the blood gas report? Hypercapnia / resp acidosis. Metabolic acidosis

Data IntepretationABG obtained from a patient admitted to the
ICU after a suicide attempt.
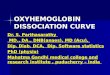
Anything about the P50?

Data IntepretationABG obtained from a patient admitted to the
ICU after a suicide attempt.
Anything about the P50? A left shifted curve despite a high PCO2 and a low
pH.

Data IntepretationABG obtained from a patient admitted to the
ICU after a suicide attempt.
List 2 other investigations you would perform to elucidate the cause of the anomaly.

Data IntepretationABG obtained from a patient admitted to the ICU
after a suicide attempt.
List 2 other investigations you would perform to elucidate the cause of the anomaly. CoHb Measure temperature Measure 2,3 DPG

Data IntepretationABG obtained from a patient admitted to the
ICU after a suicide attempt.
How can you treat carbon monoxide poisoning?

Data IntepretationABG obtained from a patient admitted to the
ICU after a suicide attempt.
How can you treat carbon monoxide poisoning? Supportive 100% oxygen

BREAK

Diagnosis?55 year old man presents with chest pain and
shortness of breath following vomiting four hours earlier.

\

Pneumothorax and pleural effusion on
right side.

This CXR and history: diagnosis?

This CXR and history: diagnosis?
Boerhaave’s syndrome

Management?

Management?supplementary oxygen, IV fluid resuscitation,
appropriate IV antibiotics, an appropriate size chest drain,
urgent surgical referral

BREAK

Diagnosis?

What is the classical description of the
patient?

What is the classical description of the
patient?Lucid interval

Management?

BREAK

Case Scenerio68 year-old man who had cardiac surgery 4
days previously.
He is intubated and ventilated and developed an increasing FiO2 requirement over the course of the day.

Xray yesterday

Xray todayDiagnosis?

Left consolidationBut did you see the right pneumothorax?

BREAK

For Fun:

Situs inversus

BREAK

Case19 year old male admitted after a severe TBI.
Due to refractory intracranial hypertension he has been intubated, sedated and paralysed
You are called to the bedside because he has desaturated to 85% on 100% oxygen.

Describe?Diagnosis?

Left upper, Right lower collapse

Why is the patient hypoxic despite
administration of 100% oxygen?

Why is the patient hypoxic despite
administration of 100% oxygen?
Shunt

How to manage?

How to manage?Bronchoscopy Recruitment manoeuvres

Describe how you recruit?

What are the complications of
recruitment maneuvers?

What are the complications of
recruitment maneuvers?
PneumothoraxHypotension
HypoxiaRaised intracranial pressure

Long Case

Story30 year old male.
ASA 2 smoker. History of childhood respiratory disorder but well since.
Admitted for right ankle fracture following mountain bike accident.
Underwent ORIF of right ankle fracture.
POD1: informs nurse of acute breathlessness and you are contacted for an assessment.

StoryParameters
BP 115 / 75 mmHg HR 95 / min SpO2 97% on room air Temperature 37.5 C
Medication chart PO Paracetamol 1g qds prn PO Synflex 550 mg bd prn PO Oxycodone 5 mg q2h prn IV Ondansetron 4 mg tds prn

What are your differentials?

Describe your approach

Describe your approach
My primary approach is to treat the underlying pathophysiology by first elucidating the cause.
I will d0 so by reassessing the History, performing a directed Physical Examination and ordering targeted
Investigations.

What would you like to know about the
history?

What will you be looking for in the
your physical examination?

What will you be looking for in the
your physical examination?Starting from the Head, I will look for …

How would you investigate this
patient?

Data IntepretationABG (room air)
pH 7.47 pCO2 31 pO2 85 BE -2 HCO3 23 SpO2 97%
Interpret the ABG

Data IntepretationFBC
TWC 12k Hb 12g/dL Platelets 151K
UE Cr 65 K 4.3
Lactate 1

Data Intepretation

Story changesPatient is progressively breathless. Unable to
speak.
Wheezing worsens.

What treatments will you start?

What treatments will you start?
Beta agonistAnticholinergics
MagnesiumAminophylline
KetamineVolatile agents
Steriods

Data IntepretationABG repeated:
pH 7.25 pCO2 52 pO2 65 BE -8 HCO3 23 SpO2 92%

Story continuesPatient worsens and consciousness drops.
You decide to intubate the patient.
Describe your intubation technique and choice of drugs.

Story continuesAfter intubation, describe you would ventilate
this patient?

Data InterpretationFBC
TWC 15 k Hb 11.9 g/dL Platelets 255 K
UE Cr 65 K 3.2
Lactate 8

END