Embed Size (px)
DESCRIPTION
nasopharyngeal cancers
Citation preview

NasopharynxPresented by: Dr.Isha Jaiswal Moderator:Dr.Rohini Khurana Date: 11th December 2013

Nasopharynx
-Behind the nasal cavity-Extends from skull Base superiorly to the soft palate inferiorly- Communicates inferiorly with
the oropharynx through the velo-pharyngeal sphincter
- The nasopharyngeal tonsil lies in the roof
- The pharyngeal opening of ET lies in the lateral wall

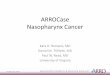
ANATOMICAL EXTENT OF NASOPHARYNX
RoofFloorAnterior wallPosterior wallLateral wall

ROOF: formed by basiocciput & basispenoid.

FLOOR: Formed by soft palate anteriorly; deficient posterior called as nasopharyngeal isthmus via which it communicates with the oropharynx .

Anterior :continuous with the nasal cavity via choanae.

Posterior wall:.
Bounded by: Atlas vertebra Axis vertebraSup. Constrictor msBuccopharyngeal fasciaRetropharyngeal spacePrevertebral fascia

Lateral wall: contain openings of eustachian tube bounded by elevation called as torus tubarius.
LATERAL VIEWMEDIAL VIEW

SINUS OF MORGAGNISpace between base of
skull & sup.connstictor.Through it enters- Eustachian tube Tensor &Levator veli
palatini muscle Asc. Palatine
artery(facial artery)
a-mucosab-pharyngobasilar fasciac-muscular coatd-buccopharyngeal fascia

FOSSA OF ROSENMULLER
Fossa of rosenmuller

What is Waldeyer’s ring?

Arterial supply: External carotid artery• Ascending pharyngeal • Spheno palatine artery• Facial arteries
Venous drainage • The pterygoid venous plexus (superiorly) • The pharyngeal plexus (inferiorly)• Finally drain in int. jugular vein
Nerve supply:Sensory -Ant. to ET opening: maxillary nerve (V2) Post. to ET opening: glossopharyngeal nerve (IX)
Motor –pharyngeal plexus formed by IX,X & cranial part of XI nerve.

LYMPHATICDRAINAGELateral Retropharyngeal L.N also called as nodes of Röuviere, are the first nodes in the lymphatic drainage of Nasopharynx.Extends from base of skull to C3 cervical vertebra.

Lymphatic drainage

MUCOSA OF NASOPHARYNX
respiratory type (ciliated pseudostratified columnar with goblet cells) near the nasal cavities
non-keratinising stratified squamous type near the pharyngeal isthmus




RADIOANATOMY

Radioanatomy

TORUS TUBARIUS

ADENOIDS: nasopharyngeal tonsil

FOSSA OF ROSENMULLER

NASOPHARYNGEAL CANCER

Epidemology
NPC shows a distinct racial and geographical distribution.
The annual incidence rate (per 100,000 per year) ranged from <1 among whites to >20 among Southern Chinese populations.
Incidence common in southern China and Taiwan and they constitute high risk group. USA & rest part of world constitute low risk group.
It is uncommon in India and constitutes 0.5% of all cancers

AGE & SEX DISTRIBUTION
bimodal age distribution is observed in low risk group. First peak incidence at 15 to 25years,second peak at 50 to 59 years of age
incidence in high-risk populations rises after 30 years of age, peaks at 40 to 60 years, and declines thereafter.
Sex ratio; M:F= 2:1 to 3:1

ETIOLOGY OF NPC
GENETIC
ENVIORMENTVIRAL

GENETIC FACTORS
Chinese have higher genetic susceptibility for NPC .
Genomic studies have revealed 3 HLA locus.HLA A2; HLA B46; HLA B17 are associated with
increased risk of NPC

ENVIORMENTAL FACTOR
DIET: Chinese salted fish food contain nitrosamines: carcinogen
Lack of vit C in dietBurning of incense & woods: polyaromatic
hydrocarbon:carcinogenAlcohol consumption & Cigarette smokingoccupational exposure to dust, smoke, and
chemical fumes

VIRUSHPV associated with keratinizing type NPC???EBV associated with NON keratinizing type NPC .EBV-DNA or RNA presence in cell indicates that
the virus has entered the tumor cell before clonal expansion.
EBV’s tumerogenic potential is due to two latent genes: LATENT MEMBRANE PROTEINS (LMP)
EBV-NUCLEAR ANTIGEN (EBNA)

NASOPHARYNGEAL CARCINOMA-NATURAL HISTORY
Inception
silent period
Focal invasion
Primary lymph node station
Genetic, environmental, viral factors
Blood stained mucus, ET blockage
Locoregional spread
retropharyngeal
Systemic spread
Parapharyngeal, skull base

Clinical Manifestation

NPCsymptoms
NASAL
NEURAL
NECK MASS
EAR

SYMPTOMSOF NPC
• Neck mass: may be due to primary tumour or secondary neck nodes. Bilateral metastasis to lymph node is common
Nasal : Discharge, bleeding, obstructionAural: tinnitus, hearing lossCranial nerve palsy : Most common 6th nerveWeight loss

Clinical Manifestation
• Neck lump 60%• Ear (s) plugging & fullness 41%• Hearing loss 37%• Nasal bleeding 30% • Nasal obstruction 29%• Head pain 16% • Ear pain 14%• Neck pain 13%• Weight loss 10%• Diplopia 8%
Symptom & sign of NPC frequency at diagnostic in Mayo clinic series

Extension pathways.

Localized tumour: m.c site FOSSA OF ROSENMULLER may
present as neck mass,dysphagia.


Anterior Spread into nasal cavity

nasal symptoms
Blood-tinge anterior or posteriornasal drainage
Obstruction of nasal pathway EpistaxisHalithosisNasal congestionsinusitis

Posterior spread: into retropharyngeal lymph node.
retropharyngeal lymph node

Post.lateral spread & involvement of prevertebral muscles.

Retropharyngeal & parapharyngeal space involvement
Retropharyngeal L.N involved
Parapharyngeal spread leads to E.T blockade &
serous otitis media.

Large tumour extending into nasal cavity,parapharyngeal & prevertebral space

Superior spread: into base of skull, may involve cavernous sinus

Superior spread: infilteration of orbital cavity via inferior Orbital fissure

RETROPAROTID SYNDROME :also calledas VILLARET SYNDROME. Occur due toenlarged lateral retropharyngeal lymph nodemetastasizing to retroparotid space. Involves 9 to12 cranial nerve & cervical
sympathetic trunk. Patient presents with difficulty in speech
&swallowing, Altered taste sensations in post.1/3 of tongue. Weakness of sternocleidomastoid & trapezius muscle. Unlateral atrophy of tongue & horner’s syndrome
Ophthalmo-neurological SYMPTOMS:

PETROSPHENOID SYNDROME of JACOD: tumour invasion to base of skull may involve II
to VI cranial nerve.(II)nerve involvement lead to decreased
vision,amurosis
VI nerve involvement results in squint and diplopia. III, IV, VI nerve involvement results in
ophthalmoplegia. V nerve involvement results in facial pain & absent
corneal reflex.
Ophthalmo-neurological SYMPTOMS:

TROTTER’S TRIAD
NPC
Hearing loss
Palatal palsyFacial pain

HORNER’S SYNDROME

Inferior Spread: to oropharynx may lead to dysphagia,regurgitation

Lateral spread:otologic symptoms
• Result from eustachian tube involvement • Sensation of ear blockage • Serous otitis media• Conductive hearing loss• Tinitus

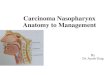
nasopharyngeal tumor with infratemporal fossa extension

LYMPHATIC SPREAD

Frequency of lymph node manifestration
• Upper jugular-94%• Middle juular-85%• Retropharyngeal
node-80%• Posterior cervical -
46%• Lower jugular-19%• Supraclavicular -17%• Submental-17%

• LYMPHATIC SPREAD most common to upper, middle deep cervical & retropharyngeal lymph nodes.


Diagnostic Evaluation

Clinical evaluation
History takingPhysical examination:
-palpation of neck node-Testing of cranial nerve-Vision & hearing assesment-Examination for distant metastasis:palpation of abdomen chest & spine.

CRANIAL NERVE TESTING


The Olfactory nerve (CN I) is simply tested by offering something familiar for the patient to smell and identify.
Olfactory nerve test

fundoscopy should be performed on both eyes.
Visual reflexes comprise direct and concentric light reflexes. -
• OPTIC NERVE TESTING

Occulomotor, trochlear & abducens nerve testing
• The Oculomotor nerve ( III), Trochlear nerve (IV) and Abducent Nerve (VI) are involved in movements of the eye. They supply the extraocular muscles of eye.

Trigeminal nerve (CN V) is involved in sensory supply to the face and motor supply to the
muscles of mastication

Corneal reflex
The corneal reflex should also be examined as the sensory supply to the cornea is from this nerve. Do this by lightly touching the cornea with the cotton wool. This should cause the patient to shut their eyelids.

To test the motor supply, ask the patient to clench their teeth together, observing and feeling the bulk of the
masseter and temporalis muscles.
perform the jaw jerk on the patient by placing your left index finger on their chin and striking it with a tendon hammer. This should cause slight protrusion of the jaw.

Crease up the forehead
The Facial nerve (CN VII) supplies motor branches to the muscles of facial expression. -
Keep eyes closed against resistance
Puff out the cheeks Reveal the teeth

Vestibulocochlear (VIII) nerve test
Rinne test - place tuning fork on the mastoid process .
Webers test - place the tuning fork at centre of the forehead -
Rinne test - place tuning fork beside the ear

Glossopharyngeal nerve (IX) test• The Glossopharyngeal
nerve (CN IX) provides sensory supply to the palate. It can be tested with the gag reflex or by touching the arches of the pharynx.
vagus nerve (CN X) provides motor supply to the pharynx. Ask the patient to speak .The uvula should be observed
before and during the patient saying “aah”. Check that it lies centrally and does not deviate on movement.

Spinal acessory nerve(XI) test
Sternocldeiomastoid ms. test against resistance
Trapezius ms. test against resistance

Hypoglossal nerve (XII) test
Ask the patient to stick their tongue out. If the tongue deviates to either side, it suggests a weakening of the muscles on that side.

Radiologic evaluation
• Nasopharyngoscopy• X Ray head & neck • CT scan head & neck ( for evaluation &
treatment planning ) • MRI ( if intracranial extension )• Bone scan• Pet scan

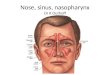
Endoscopic nasopharyngoscopy

MRI.
Advantages: Superior in assessingprimary tumour, invasion intosurrounding soft tissuepharyngobasilar fascia,skull base invasion,intracranial invasion, aswell as cavernous sinusextension andperineural disease
Advantages:Superior to MRI and CT
forassessing lymph nodemetastasis, especiallycervical nodal
metastases,and distant metastases,especially occult
metastatic disease
PETCTImaging techniques

Histopathologic evaluation
• Biopsy• Most common site are roof of nasophalynx
& Rosenmuller fossa• Most common histological type:
squamous cell carinoma ( SCC)KERATINIZING TYPE NON KERATINIZING TYPE –diffretiated & undiffentiated subtypesBASALOID TYPE

Immunology
• Indirect immunofluorescence for IgG & IgA antibodies to viral capsid antigen (VCA) & early antigen (EA)– Most specific test for diagnosis– Highly predictive of the clinical
course:monitoring of EBV DNA in serum of affected pt.using RTPCR is useful for monitoring therapy.
– not yet commercially available