Embed Size (px)
Citation preview

1
RENAL FUNCTION TESTS
Dr.ANKUR PURIDept. Of Pediatrics
13-09-2012
2
Introduction
• The kidneys are two bean shaped organs lying retroperitoneally on each side of the vertebral column slightly above the level of umblicus.
• The range in length & weight, respectively, from approximately 6cm & 24gms in a full term infant to more than equal to 12cm & 150gms in an adult
3
NEPHRON
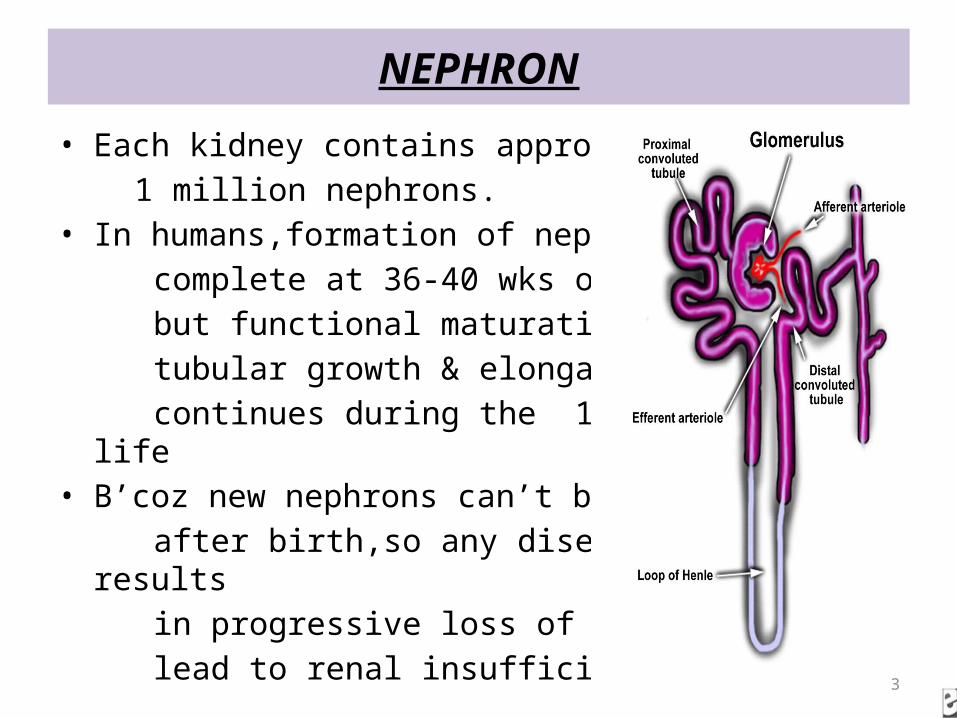
• Each kidney contains approx. 1 million nephrons.• In humans,formation of nephron is complete at 36-40 wks of gestation., but functional maturation with tubular growth & elongation continues during the 1st decade of life• B’coz new nephrons can’t be formed after birth,so any disease that results in progressive loss of nephrons can lead to renal insufficiency.
4
Cont..
• A decreased number of nephrons secondary to LBW,prematurity &/or unknown genetic or environmental factor is hypothesised to be a risk factor for the development of primary HT & Progressive Renal Dysfunction in adulthood.
5
Cont…
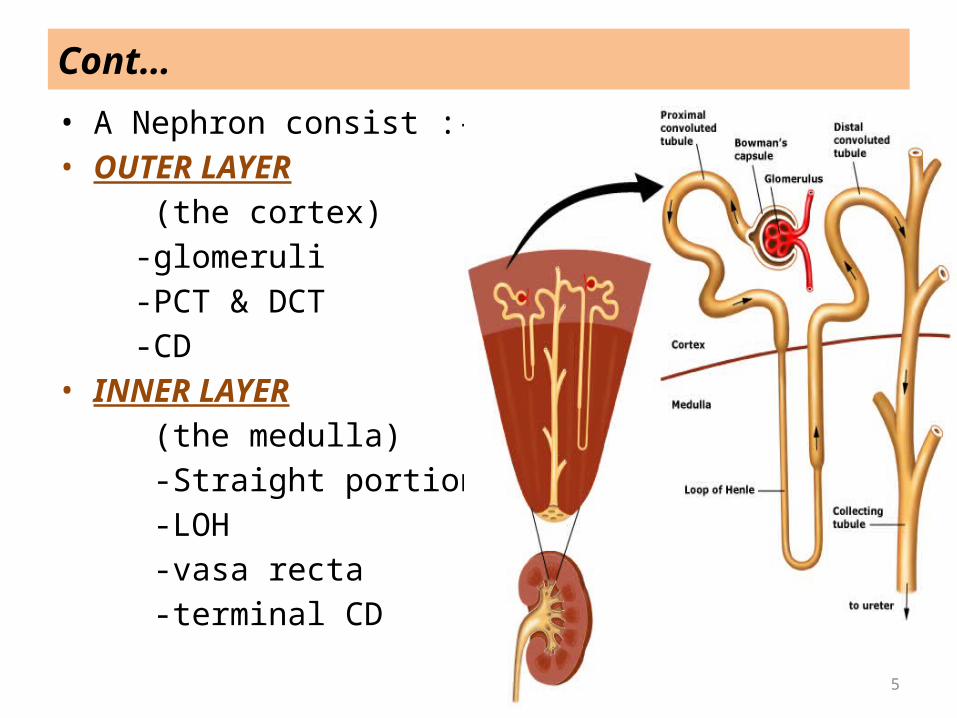
• A Nephron consist :-• OUTER LAYER (the cortex) -glomeruli -PCT & DCT -CD• INNER LAYER (the medulla) -Straight portion of tubules -LOH -vasa recta -terminal CD
6
JUXTAGLOMERULAR APPARATUS
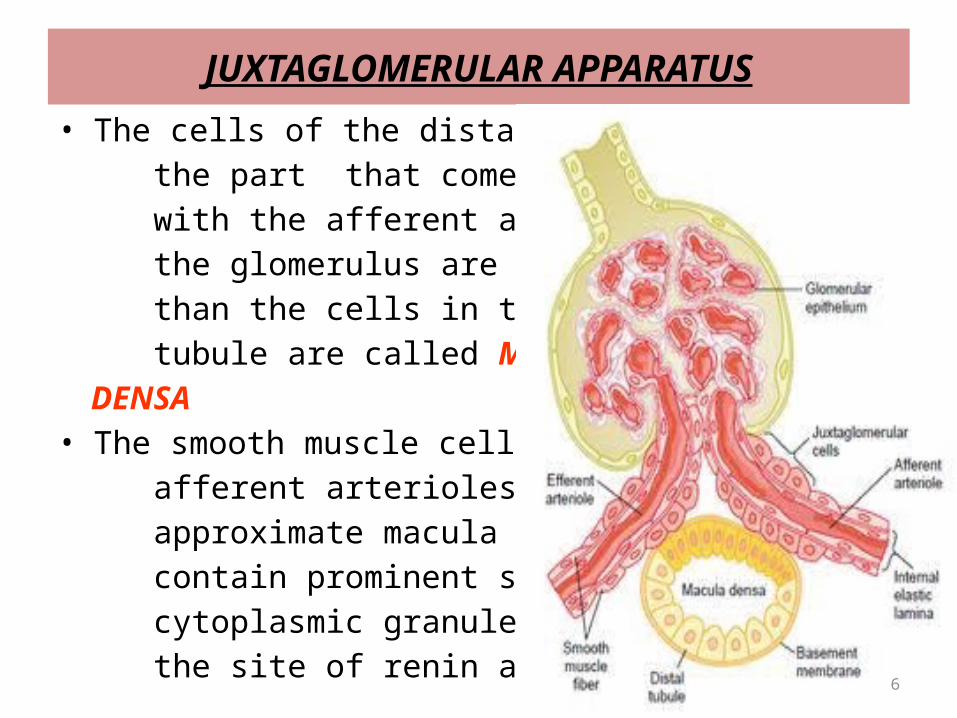
• The cells of the distal tubule in the part that comes in contact with the afferent arterioles of the glomerulus are more dense than the cells in the rest of tubule are called MACULA DENSA• The smooth muscle cells of afferent arterioles that approximate macula densa contain prominent secretory cytoplasmic granules which are the site of renin activity.
7
Cont…
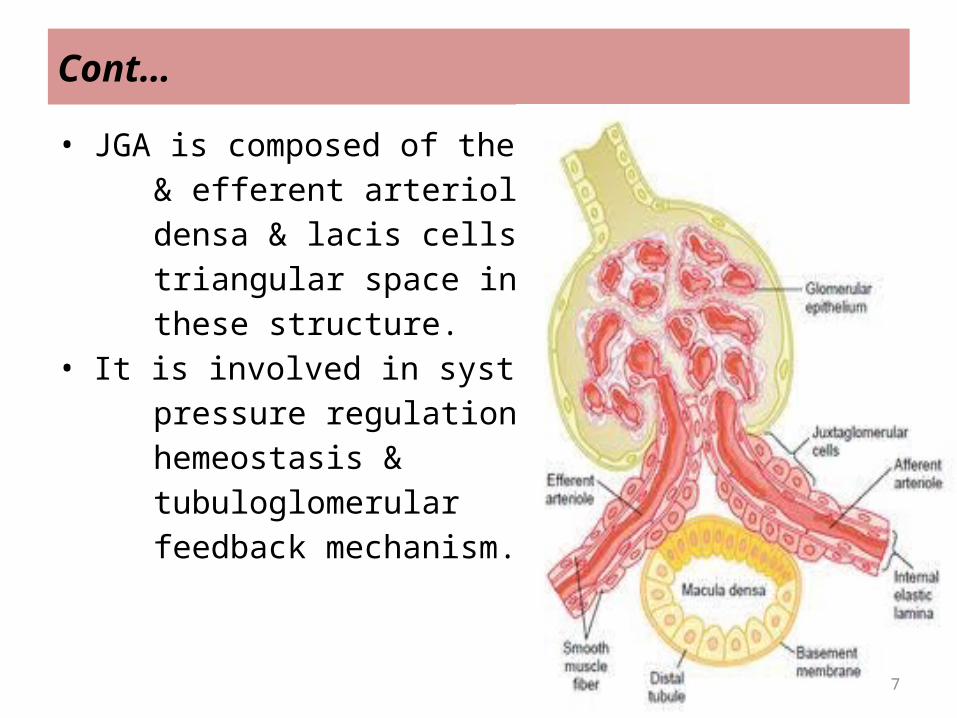
• JGA is composed of the afferent & efferent arterioles,the macula densa & lacis cells located in the triangular space in between these structure.• It is involved in systemic blood pressure regulation,electrolyte hemeostasis & tubuloglomerular feedback mechanism.
8
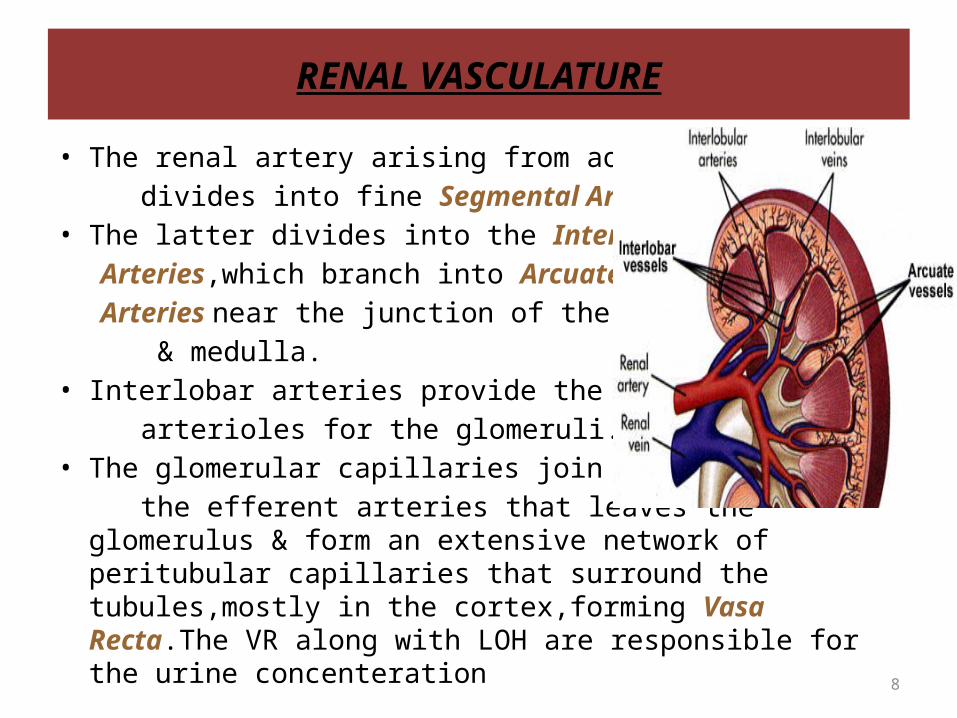
RENAL VASCULATURE
• The renal artery arising from aorta divides into fine Segmental Arteries.• The latter divides into the Interlobar Arteries,which branch into Arcuate Arteries near the junction of the Cortex & medulla.• Interlobar arteries provide the afferent arterioles for the glomeruli.• The glomerular capillaries join to form the efferent arteries that leaves the glomerulus & form an
extensive network of peritubular capillaries that surround the tubules,mostly in the cortex,forming Vasa Recta.The VR along with LOH are responsible for the urine concenteration
9
RENAL FUNCTIONS
10
DIAGNOSTIC EVALUATION
• Urine Examination -routine & -microscopic• Evaluation of Renal Function• Renal Biopsy• Imaging
11
URINE EXAMINATION
• It is the most important step for the diagnosis of renal disease.
• COLLECTION OF SAMPLE : -the 1st morning specimen is preferred -collected in a clean container -for culture, the specimen should be collected in a sterile container & sent to the lab. Immedietly, where it should be plated within 15minutes or stored in a refrigerator at 4 degree celsius.Bacteria multiply rapidly at room tempt., which may give false positive results.
12
Method of urine collection• Midstream urine : a clean-catch midstream specimen is widely used. In older children who can
cooperate, midstream specimen is obtained after proper local cleaning .The initial part of urine is discarded.
• Bag collection : in neonates & infants, urine can be collected in sterile bags. Not used for microscopic
exam.• Bladder catheterisation : a urine specimen can also be safely obtained, in infants, by strict
bladder catheterisation but requires some skills & experience.• Suprapubic bladder aspiration : the only reliable way to obtain reliable urine
specimen in neonates & young infants. In children <2 yrs of age it is most suitable method for a definitive diagnosis of UTI.
13
URINE ROUTINE EXAMINATION
• SPECIFIC GRAVITY : full term infants have a limited concentrating ability with a maximum sp.gravity of 1.021 – 1.025.It is measured with clinical Hydrometer. Increase in sp.gravity may be ass. with dehydration, diarrhea, emesis, excessive sweating etc. while decrease in sp.gravity may be ass. with renal failure, DI, ATN, interstitial nephritis &
excessive fluid intake.
• pH : tested with pH meter. Routine lab reports of pH are of no importnace.UTI with urea splitting organisms make urine highly Alkaline. Normal pH ranges from 4.6 -8.0. In fasting, the concentrated urine sample is highly Acidic .
14
Cont…
-A high urine may be due to RTA(type I),UTI,Vomitng & a low urinary pH may be due to DKA,diarrhea & starvation.
• PROTEIN : Boiling test : satisfactory but cumbersome.10-15 ml of urine
is taken in a test tube & upper portion is boiled. If turbidity appears 3 drops of concentrated acetic acid are added & specimen is boiled again. A zero to +4 grading is used.
15
Cont…
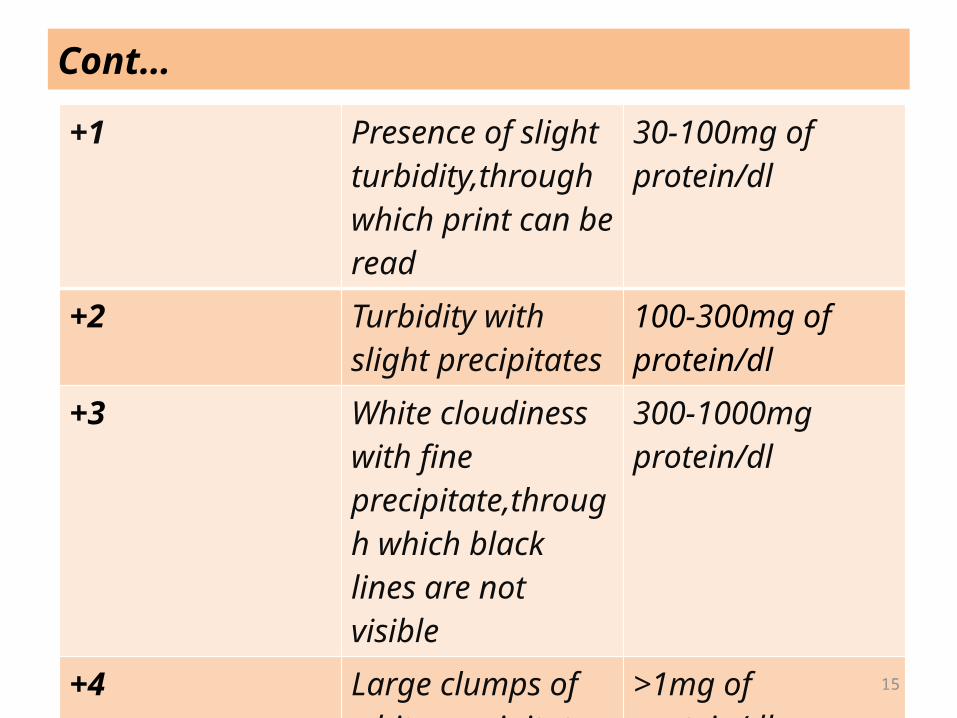
+1 Presence of slight turbidity,through which print can be read
30-100mg of protein/dl
+2 Turbidity with slight precipitates
100-300mg of protein/dl
+3 White cloudiness with fine precipitate,through which black lines are not visible
300-1000mg protein/dl
+4 Large clumps of white precipitates
>1mg of protein/dl
16
Cont…
Dipstick methods(e.g uristix) : widely used test for Proteinuria, more convenient &equally reliable.-Colour changes from yellow to green.-light chain proteins & LMW tubular proteins are not detected by this method.-Trace react. 5 to 20 mg/dl urinary prtn +1 30 mg/dl +2 100 mg/dl +3 300 mg/dl +4 > 1000 mg/dl
17
Cont…
• Proteinuria in patients with Nephrotic Syndrome is massive (+3 or +4 by dipstick) & selective,constituted predominantly
of Albumin,without loss of proteins of higher molecular wt.• In the presence of tubular damage or physical injury to the
glomerular barrier, the proteinuria is non selective.• In renal parenchymal diseases,proteinuria is often quantified
to assess degree of glomerular injury.• Selective Proteinuria : intermediate sized(<1000kDa)
proteins(albumin,transferrin) leaks through glomerulus.• Nonselective proteinuria : range of different sized proteins
leak through,including larger proteins(immunoglobulin)
18
Cont…
• Quantitative Measurement of Urine Protein -Accurate collection of urine over 24hr period is required to
quantitate protein excretion. -A value of >4mg/m2/hr is considered abnormal, & >40/m2/hr
indicates heavy proteinuria. -The range proteinuria in nephrotic so is massive
proteinuria(>3.5gm/24hrs) while the range in nephritic s o is mild to moderate
proteinuria(<3gm/24hrs)
19
Cont…
• Urine Protein/Creatinine Ratio : an approx. estimate of the severity of proteinuria also can be made by measurement of urine protein & urine creatinine on random urine sample.
-Values >2 indicate Heavy Proteinuria <0.2 are insignificant. -Such measurements are of use in following response to therapy in various disorders, but seldom necessary in children with nephrotic syndrome.
20
Cont…
• GLUCOSE :the older methods(e.g benedict test) that detected reducing substance have mostly been replaced by Dipstick test,which is based on Glucose Oxidase Peroxidase linked reaction.
• BLOOD :detection of Hb by dipstick is based on an reaction, with a spotted +ve reaction indicating intact red blood cells & uniform +vity suggesting presence of free Hb.However the use of dipstick to detect hematuria is discouraged,b’coz reactions may often be false +ve(e.g myoglobinuria,oxidising substances,bacterial colonisation) or false –ve (e.g ascorbic acid,other reducing substances)
21
MICROSCOPIC EXAMINATION
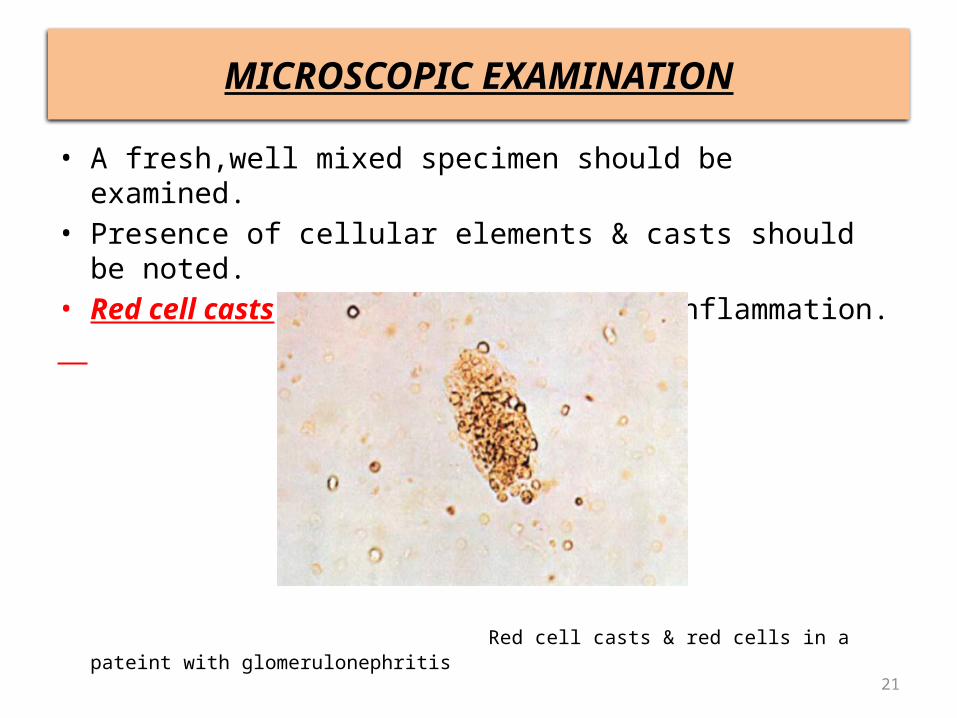
• A fresh,well mixed specimen should be examined.• Presence of cellular elements & casts should be noted.• Red cell casts : indicate glomerular inflammation.
Red cell casts & red cells in a pateint with glomerulonephritis
22
Cont…
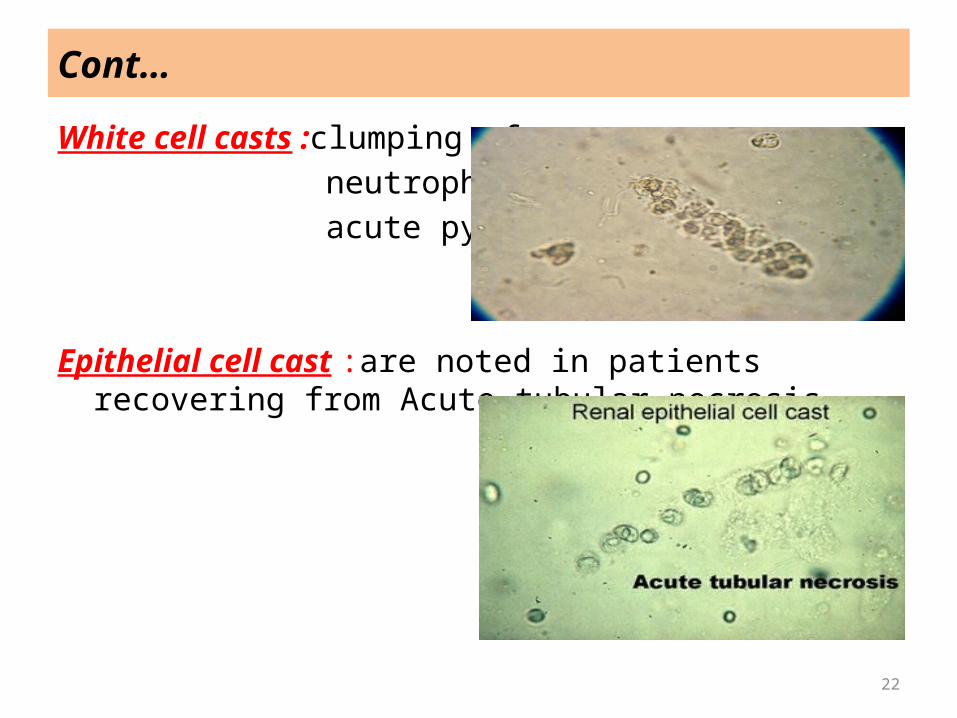
White cell casts :clumping of neutrophils suggests acute pyelonephritis
Epithelial cell cast :are noted in patients recovering from Acute tubular necrosis
23
Cont…
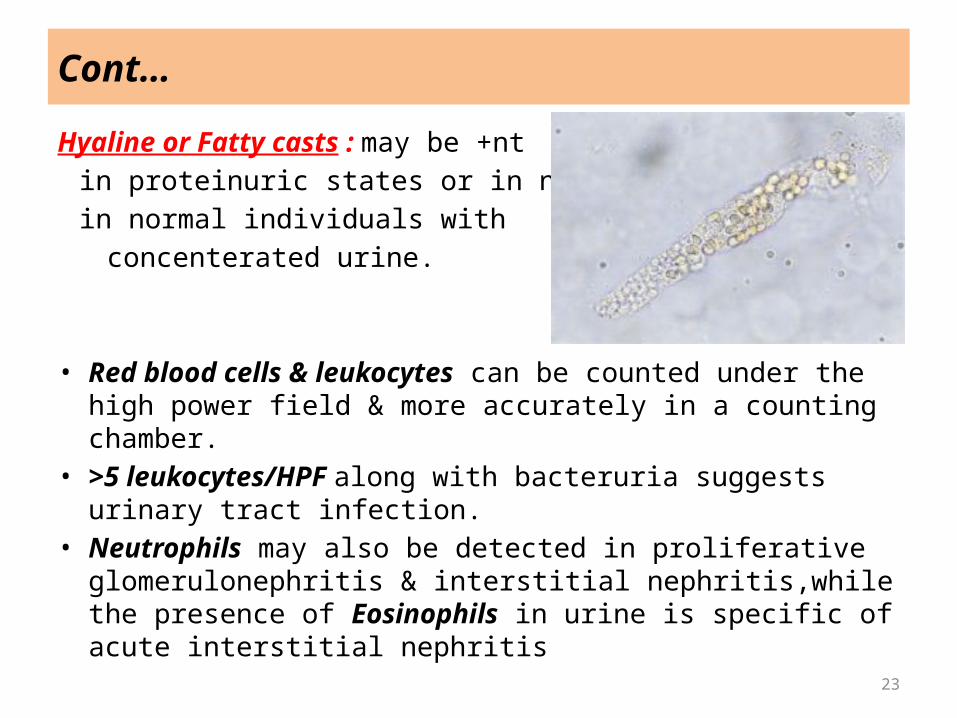
Hyaline or Fatty casts : may be +nt in proteinuric states or in normal in normal individuals with concenterated urine.
• Red blood cells & leukocytes can be counted under the high power field & more accurately in a counting chamber.
• >5 leukocytes/HPF along with bacteruria suggests urinary tract infection.
• Neutrophils may also be detected in proliferative glomerulonephritis & interstitial nephritis,while the presence of Eosinophils in urine is specific of acute interstitial nephritis
24
Cont…
• Hematuria is defined as presence of >5RBS/HPF in a centrifuged specimen.
• RBC morphology is useful in distinguishing bet. Glomerular & non glomerular causes of hematuria.
• The site of injury is likely to be the lower urinary tract if <25% urine correlates well with a colony count of over 105 organisms/ml indicating significant bacteriuria.
25
URINE CULTURE
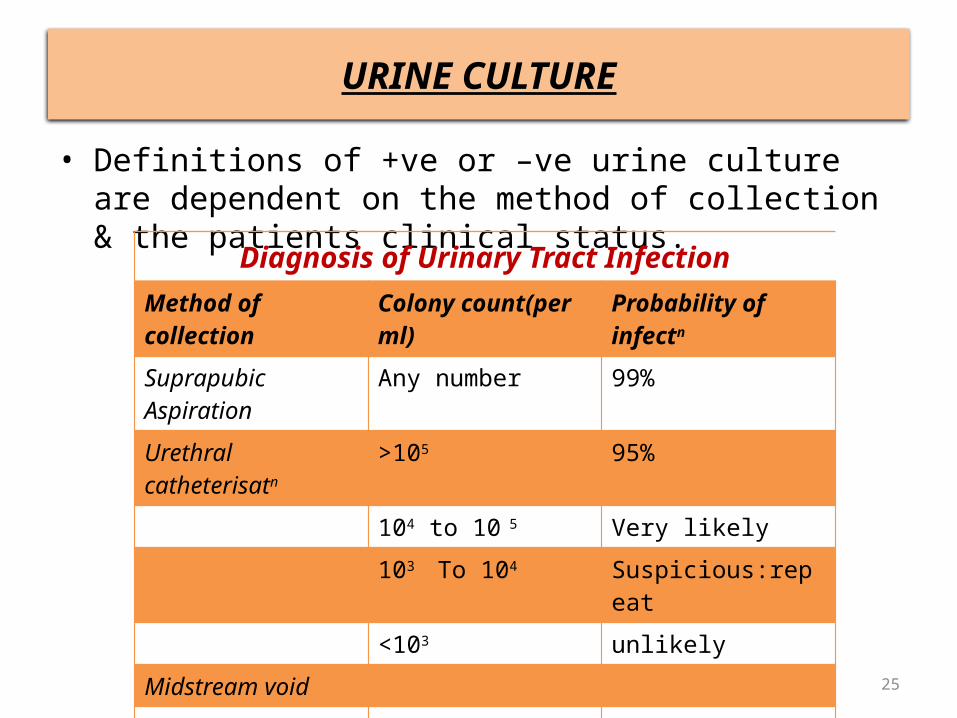
• Definitions of +ve or –ve urine culture are dependent on the method of collection & the patients clinical status.
Diagnosis of Urinary Tract InfectionMethod of collection Colony count(per ml) Probability of infectn
Suprapubic Aspiration Any number 99%Urethral catheterisatn >105 95%
104 to 10 5 Very likely103 To 104 Suspicious:repeat<103 unlikely
Midstream voidBoys >104 Very likelyGirls >105 90-95%
104 to 105 Suspicious:repeat<104 unlikely
26
EVAULUATION OF RENAL FUNCTION
• Various aspects of renal function are -GFR(Glomerular Filtration Rate) -RPF(Renal Plasma Flow) -Reabsorption & Excretion of various substances like Na+, K+,
Ca+2, inorganic phosphate, glucose, urea, a.a, H2O & osmoles.• In clinical practice -determination of Creatinine Clearance is a measure of GFR -water deprivation & vasopressin administration tests to determine urinary concentrating ability, & -bicarbonate & ammonium chloride loading test to examine urinary acidification are usually sufficient for diagnostic evaluation & measurement of kidney function.
27
Cont…
• The results of these tests are important in assessing the excretory function of the kidneys. For example, grading of chronic renal insufficiency and dosage of drugs that are excreted primarily via urine are based on GFR (or creatinine clearance).
28
GLOMERULAR FUNCTION TEST
• The concept of clearance is based upon the fact that the rate of removal of a substance from the plasma must equal its simultaneous rate of excretion in urine.
• Thus if the urinary excretion rate & plasma concentration of a substance are known, we can calculate the volume of plasma from which that substance would have been completely removed. INULIN has been taken as a reference substance.
• The standard formula for clearance is : C = U x V PC = clearence/min(ml/min)U = urinary concenteration(mg/dl)P = plasma concenteration(mg/dl)V = urine volume/min(ml/min)
29
Cont…
• If a given substance is freely filtered & neither reabsorbed nor excreted, its clearance rate would accurately reflect GFR.
• The GFR can be estimated by measuring s.creatinine level & height.The formula proposed by SCHWARTZ is useful for children :
• GFR(ml/min/1.73m2) = K x Height(cm) S.Creatinine(mg/dl) K = 0.34 (in preterm infant) = 0.45 (in term infants) = 0.55 (in children & adoloscent girls) & = 0.7 (in adoloscent males)
30
Cont…
• Serum Creatinine & Creatinine Clearance :• Creatinine is derived from the metabolism of creatine &
phosphocreatine,the bulk of which is in muscle.• Since creatinine is chiefly excreted by glomerular
filteration,S.creatinine levels reflects changes in GFR.• S.creatinine values are low when the muscle mass is
decreased, as in malnutrition.• Bilirubin interferes with creatinine measurements.
31
Cont…
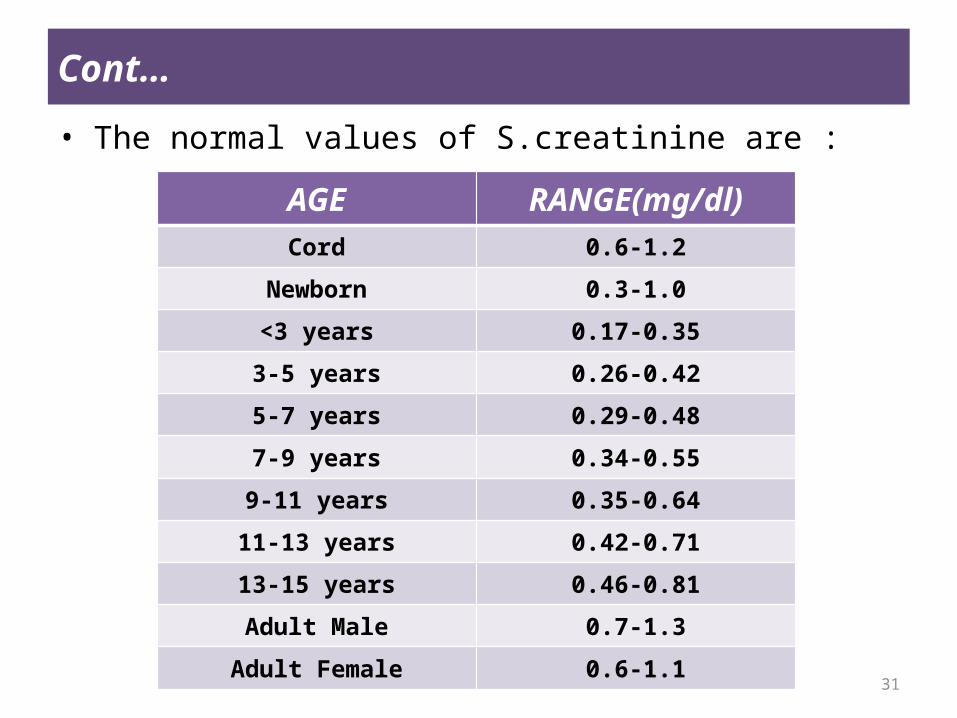
• The normal values of S.creatinine are :
AGE RANGE(mg/dl)Cord 0.6-1.2
Newborn 0.3-1.0
<3 years 0.17-0.35
3-5 years 0.26-0.42
5-7 years 0.29-0.48
7-9 years 0.34-0.55
9-11 years 0.35-0.64
11-13 years 0.42-0.71
13-15 years 0.46-0.81
Adult Male 0.7-1.3
Adult Female 0.6-1.1
32
Cont…
• CYSTATIN C : It is a LMW nonglycosylated protein produced at a constant rate by all nucleated cells in the body, freely filtered by the glomeruli, not secreted, but totally reabsorbed by the renal tubules.
• Little or no cystatin is excreted in urine.• Normal adults have circulating level of approx. 1mg/l.• This is better indicator of renal function as compared to
creatinine in early stages of GFR impairment as it is independent of age,gender,body composition & muscle mass.
• Cystatin C can be estimated in blood by enzyme immunoassays or immunoturbidometry.Both techniques are currently kit based & expensive.
33
Cont…
• SINGLE INJECTION TECHNIQUE : in clinical practice, radionuclides are often used to estimate total GFR or to measure difference in clearance bet. one kidney compared to other in the same patient.
• The technique is based on use of a single injection, plasma disappearance curves to estimate the true GFR.
• Briefly, the radionuclide dye is injected & the signal from radiolabelled form is used to obtain measurment.
• The most commonly used Radionuclides for GFR are -DTPA (Diethyl triamine Penta-acetic acid) -EDTA (ethylene diamine tetra acetic acid) & -Iothalamate• Iohexol,a non ionic non radioactive LMW radiocontrast
agent,as an alternative to inulin,measured easily by HPLC(high performance liquid chromatography)
34
Cont…
• BLOOD UREA : A normal level of blood urea is often mistakenly regarded to indicate normal kidney function.
• In a steady state the blood urea may not rise beyond the upper range of normal(40mg/dl) even when 75% of the renal function is lost.
• On the other hand, prerenal factors that decreases renal perfusion & GFR,such as dehydration,causes an increase in blood urea levels.
• There may be transient rise in blood urea level due to : -high protein intake & excessive protein catabolism( e.g with
severe infections,tissue break down,trauma,use of large doses of corticosteroids or tetracyclines)
-gastrointestinal bleeding & inhibition of anabolism.
35
RENAL BLOOD FLOW
• Renal blood flow measurements are performed using the clearance of PAH(para aminohippurate)
• >90% PAH is extracted from the plasma during the 1st pass through the kidneys.Therefore, renal clearance of PAH is commonly used as an estimate of renal plasma flow(RPF).
• Plasma clearance following single injection of 131I-hippuran or 99mTc-mercaptoacetyltriglycine(MAG-3)is an alternative method.
• Renal Blood Flow is calculated by dividing RPF by [1-hematocrit].
• Normal value ranges from 500 to 600 ml/min(abt. 1200ml/min/1.73m2).
• Other methods-Color Doppler US,Contrast Enhanced US & MRI.
36
URINARY CONCENTERATION
• Osmolality dependes upon the number of particles in a solution & not on their size or density.
• The maximal urinary concentration capacity varies with age - in neonates its abt. 700 mOsm/kg - in older children & adults it an rise up to 1200mosm/kg.• Hyposthenuria(inability to increase urine osmolality > than
that of plasma) is characteristic of Diabetes Insipidus as well as Diseases of Renal Medulla such as obstructive uropathy.
• Polyuria & polydipsia are stricking features.• In chronic Renal Failure urine osmolality does not rise much
above 400mOsm/kg & polyuria & polydipsia are not prominent.
• Osmolality = 2[Na+] + [Glucose]/18 + [ BUN ]/2.8
37
Cont…
• URINARY CONCENTERATION TEST : Urinary concentrating ability needs to be tested in a setting of polyuria.If the 1st morning void after 12hrs of overnight fasting has osmolality exceeding 700 mOsm/kg,no further testing is required.In others, Water Deprivation Testing is done.
• Response to Vasopressin : subsequently,to confirm the lack of renal concentrating ability & distinguish Nephrogenic Diabetes Insipidus(NDI) from Central Diabetes Insipidus(CDI),a vasopressin test is performed.
-Desamino-8-D-arginine Vasopressin(dDAVP,desmopressin) is administered nassly(5-10 ug in neonates & infants,20 ug in children) or by an I.M injection(0.4-1.0 ug in infants & young children,2 ug in older children).
• The changes in urine osmolality seen are :
38
Cont…
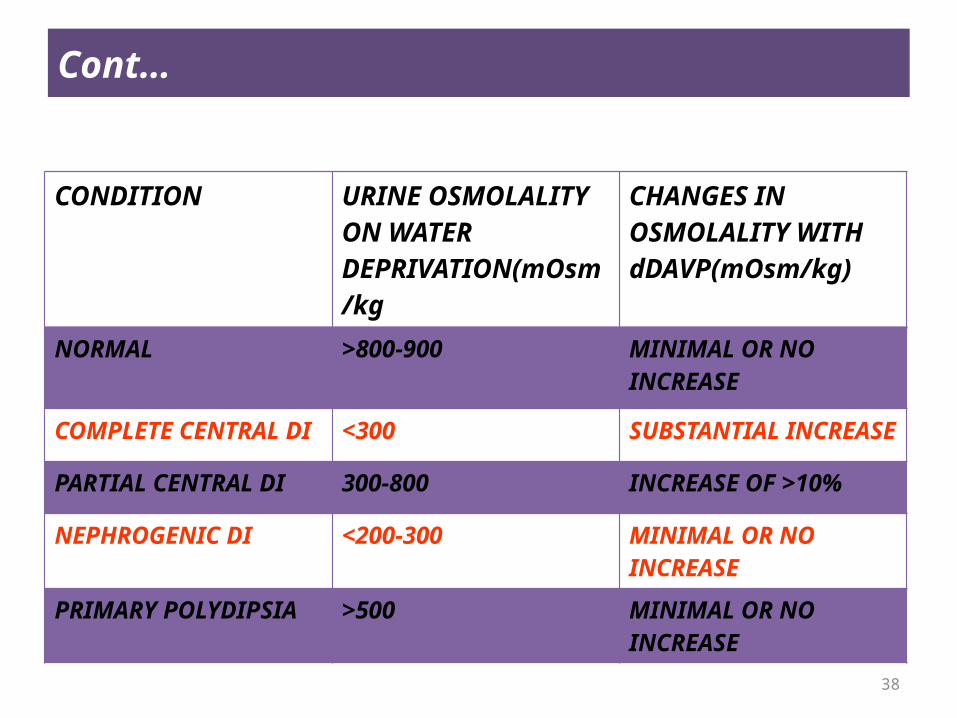
CONDITION URINE OSMOLALITY ON WATER DEPRIVATION(mOsm/kg
CHANGES IN OSMOLALITY WITH dDAVP(mOsm/kg)
NORMAL >800-900 MINIMAL OR NO INCREASE
COMPLETE CENTRAL DI <300 SUBSTANTIAL INCREASE
PARTIAL CENTRAL DI 300-800 INCREASE OF >10%
NEPHROGENIC DI <200-300 MINIMAL OR NO INCREASE
PRIMARY POLYDIPSIA >500 MINIMAL OR NO INCREASE
39
Tests Of Urinary Acidification
• Renal acidification mechanism are usually examined in children with suspected renal tubular acidosis.
• Urine pH : The pH of a fresh specimen of urine is tested with pH meter. A concentrated, fasting, morning sample of urine is acidic.A pH of <5.5 virtually excludes distal renal tubular acidosis.
• Urine Anion Gap : Urine anion gap is the difference between concentration of principal urinary cations(Na + k) & anion(cl)This difference is expected to estimate the unmeasured anions & cation,which normally include ammonium & bicarbonate.Since the latter is mostly reabsorbed ,urine anion gap is chiefly measure of ammonium excretion.
40
Cont…
• In presence of systemic metabolic acidosis,ammonium excretion is expected to be stimulated while the bicarbonate excretion is minimal,hence,the urine anion gap should be –ve due to obligatory chloride excretion with ammonium.
• In patients with renal tubular acidosis the gap remains +ve due to impaired ammonium production.
• Sodium Bicarbonate Loading Test : The Bicarbonate threshold is the plasma bicarbonate level at which bicarbonate appears in urine.
-The bicarbonate threshold is determined by infusion of bicarbonate & increasing the plasma bicarbonate in a stepwise manner to elevate he serum bicarbonate level to 23-26mEq/l.
41
Cont…
-3-5ml/kg sodium bicarbonate is administered orally or Intravenously,which increase the urine pH to more than 7.4.
-Levels of bicarbonate & creatinine are measured in blood & random urine specimens.
-Normally there is no bicaorbonaturia unless the plasma bicarbonate level exceeds 23-24mEq/l.
-the urinary bicarbonate threshold is reduced is proximal renal tubular acidosis.The Fractional Excretion of bicarbonate (FEHCO3) is calculated by the formula :
FEHCO3 = urine HCO3 X plasma creatinine X 100
plasma HCO3 X urine creatinine
-The normal level of FEHCO3 are <5%.In proximal RTA,the FEHCO3 usually exceed 15%.
42
Cont…
• Other tests for urine acidification are -Urine PCO2
-Ammonium Chloride Loading test
43
Cont…
OTHER INVESTIGATIONS• S.proteins : S.albumin level• S.cholesterol: in Nephrotic So—hypercholesterolemia.• Anti Streptococcal Antibody Titer : antibody titer against
hemolytic streptococcs is important for the diagnosis of Poststreptococcal GN(PSGN).A titer of >200 IU/ml is +ve.
• S.complement : measurement of C3 & C4 levels in bld. is important for diagnosis of Postinfectious GN, Membranoproliferative GN & Lupus Nephritis, where decrease in C3 levels are +nt. The levels of C3 are increased in active Rheumatoid arthritis. The normal range of S.C3 is 70 to 120 mg/dl & C4 20-50 mg/dl.
• S.immunoglobulins : S.IgA levels are increased in abt 30-40%patients with IgA nephropathy & HSP.
44
Cont…
• Antineutrophil cystoplasmic antibodies : are typically detected in Wegner’s granulomatosis & In Pauci-Immune Cresentric GN.
45
RENAL BIOPSY
• Expert evaluation of renal histology is important in the diagnosis of various renal parenchymal disease involving glomeruli, tubulo-interstitium & small blood vessels.
• The procedure has become has become much simpler with the use of automatic (biopsy gun,tru cut) devices & ultrasono -graphic visualization of kidney.• INDICATIONS : Renal biopsy has a limited role in children.Significant Value-Streoid resistant nephrotic So
-Acute Renal Failure of Unknow Cause-Rapidly Progressive Renal Failure
46
Cont…
-Systemic disease(Henoch-schonlein Purpura,Lupus Hemolytic Uremic So ,IgA nephropathy)
-Inherited Nephropathies e.g Alport So
-Renal allograft dysfunction-Detection Of Calcineurin toxicityLess Value-Chronic renal Failure to ascertain etiology-Non Nephrotic Range Proteinuria-Microscopic Hematuria-Steroid Sensitive Nephrotic So
A Renal Biopsy Is not required in uncomplicated cases of Postinfectious GN & corticosteroid responsive nephrotic So
47
Cont…
• BIOPSY PROCEDURE-A renal biopsy is usually made percutaneously-A history of bleeding & clotting disorders should be obtained.-PT, BT, Coagulation time & Platelet count is measured.-BP should be in normal range-In Patients with acute renal failure,dialysis should be done to
reduce azotemia & correct biochemical abnormalities before the biopsy.
-Renal size & location are confirmed with an US before biopsy.-The Patient should be kept fasting for abt 3-4 hrs.-Local anaesthesia can be used
48
Cont…
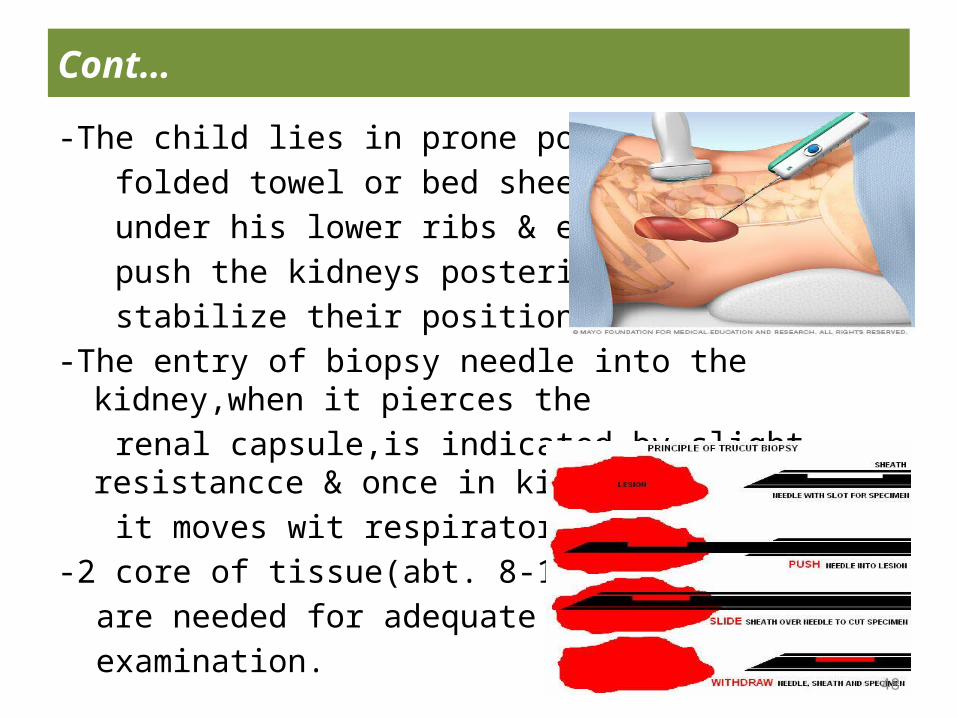
-The child lies in prone position with a folded towel or bed sheet placed under his lower ribs & epigastrium to push the kidneys posteriorly & stabilize their position.-The entry of biopsy needle into the kidney,when it pierces the renal capsule,is indicated by slight resistancce & once in kidney it moves wit respiratory excrusions -2 core of tissue(abt. 8-10 mm long) are needed for adequate histological examination.
49
Cont…
-One core is fixed in buffered formaline & other in saline(for immunofluorescencs study)
Interpretation of Renal Biopsy• The histology should be examined by light microscopy using
Hematoxylin & eosin(H & E),Periodic Schiff (PAS) & Silver Methanamine staining In all cases, & special stains as necessary.
• Electron microscopy is very useful in several disorders e.g Alport So, Membranoproliferative GN & thin Basement Membrane Disease.
50
IMAGING
• DIAGNOSTIC PROCEDURES• RADIONUCLIDE STUDIES
51
DIAGNOSTIC PROCEDURES
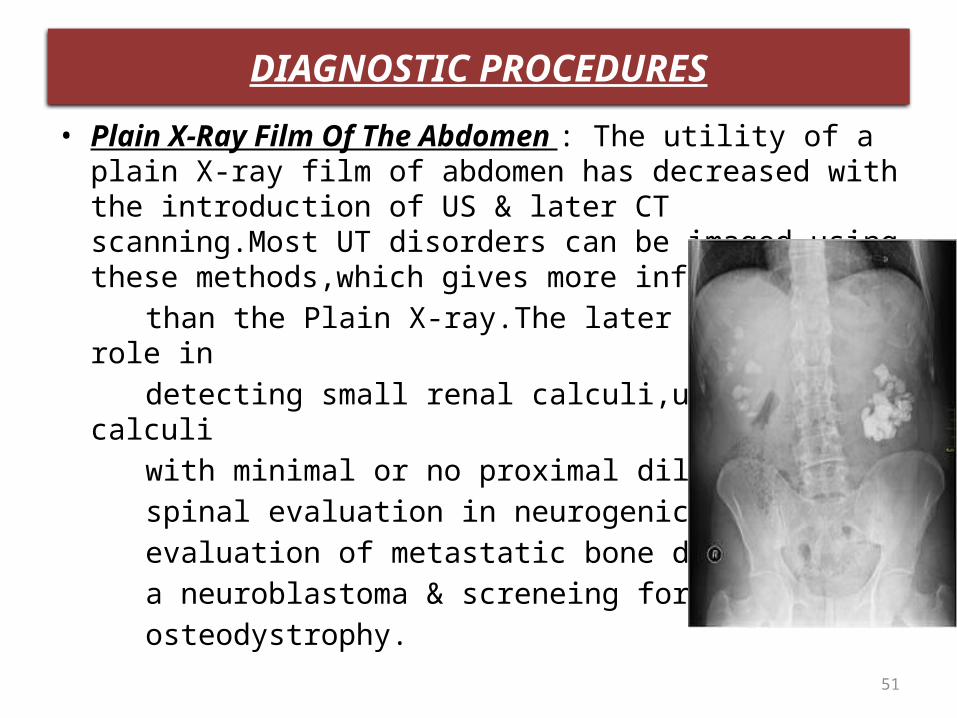
• Plain X-Ray Film Of The Abdomen : The utility of a plain X-ray film of abdomen has decreased with the introduction of US & later CT scanning.Most UT disorders can be imaged using these methods,which gives more information
than the Plain X-ray.The later still has a role in detecting small renal calculi,ureteric calculi with minimal or no proximal dilatation, spinal evaluation in neurogenic states, evaluation of metastatic bone disease from a neuroblastoma & screneing for renal osteodystrophy.
52
Cont…
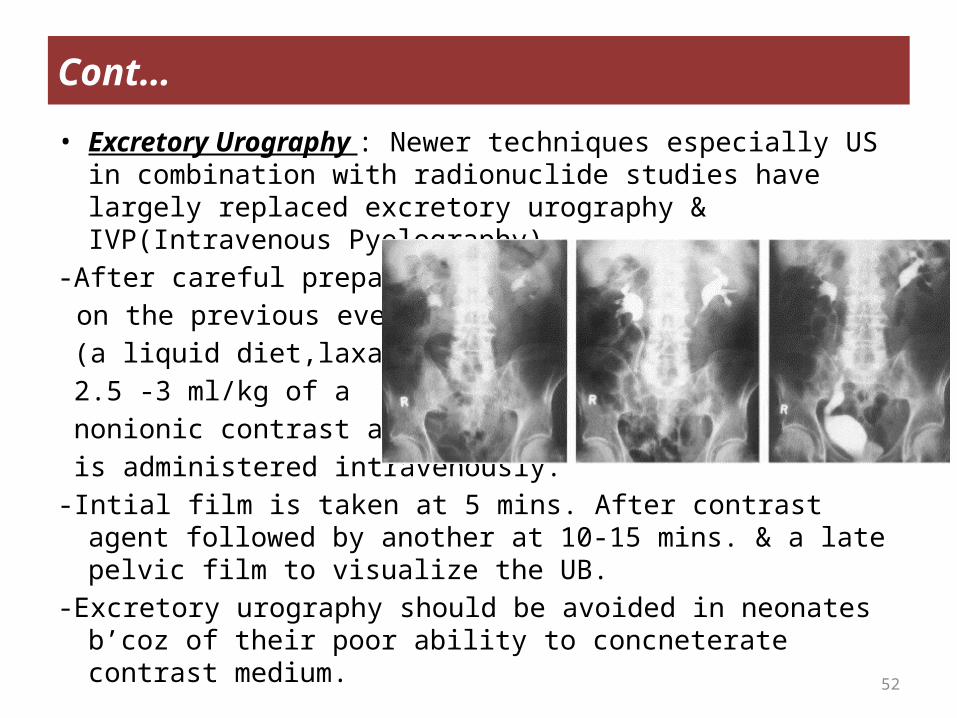
• Excretory Urography : Newer techniques especially US in combination with radionuclide studies have largely replaced excretory urography & IVP(Intravenous Pyelography).
-After careful preparatn
on the previous evening (a liquid diet,laxative) 2.5 -3 ml/kg of a nonionic contrast agent is administered intravenously.-Intial film is taken at 5 mins. After contrast agent followed by
another at 10-15 mins. & a late pelvic film to visualize the UB.-Excretory urography should be avoided in neonates b’coz of
their poor ability to concneterate contrast medium.
53
Cont…
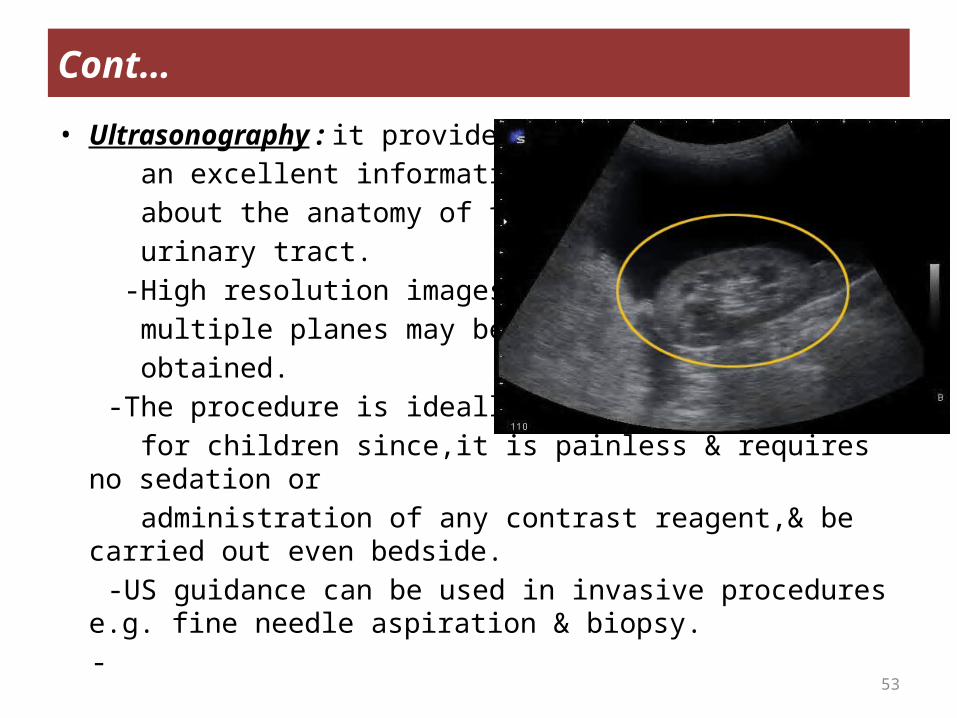
• Ultrasonography : it provides an excellent information about the anatomy of the urinary tract. -High resolution images in multiple planes may be obtained. -The procedure is ideally suited for children since,it is painless & requires no sedation or administration of any contrast reagent,& be carried out even
bedside. -US guidance can be used in invasive procedures e.g. fine needle
aspiration & biopsy. -
54
Cont…
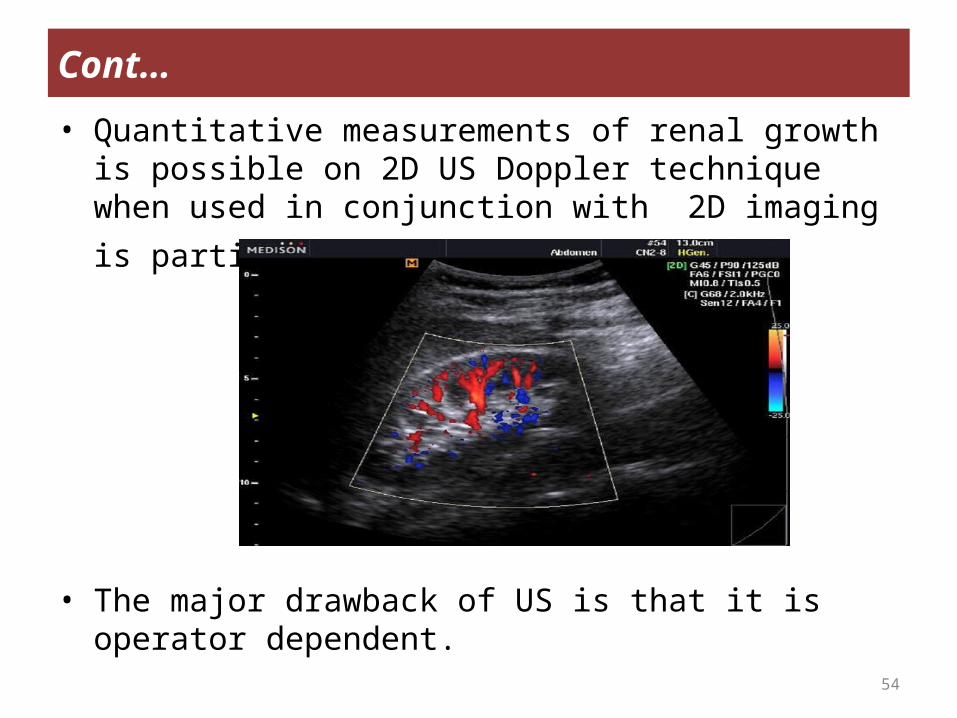
• Quantitative measurements of renal growth is possible on 2D US Doppler technique when used in conjunction with 2D
imaging is particularly informative.
• The major drawback of US is that it is operator dependent.
55
Cont…
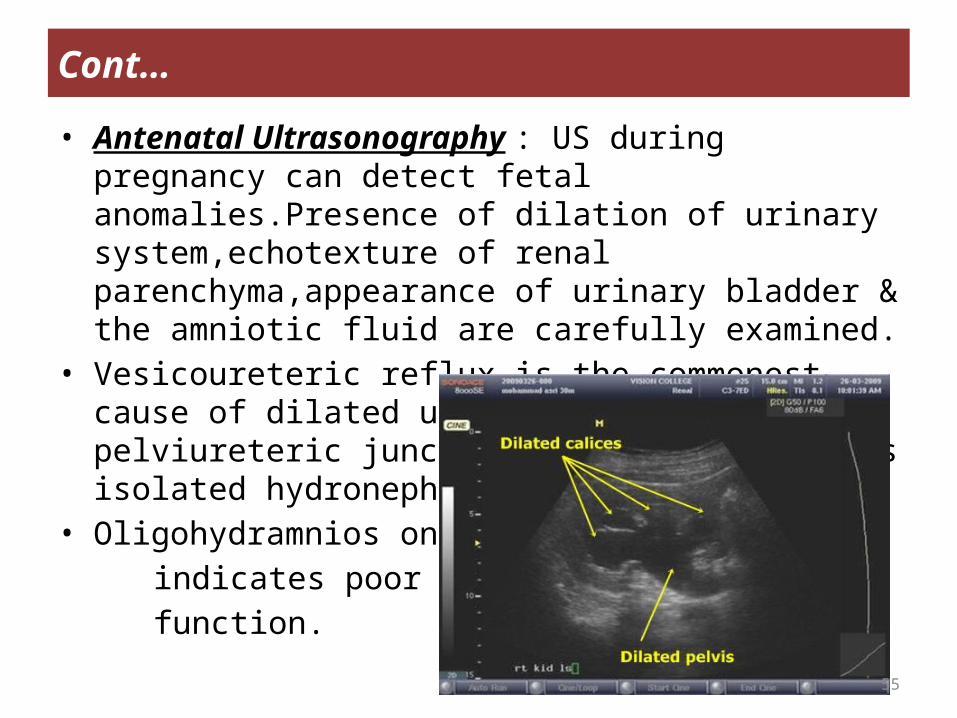
• Antenatal Ultrasonography : US during pregnancy can detect fetal anomalies.Presence of dilation of urinary system,echotexture of renal parenchyma,appearance of urinary bladder & the amniotic fluid are carefully examined.
• Vesicoureteric reflux is the commonest cause of dilated urinary tract & pelviureteric junction obstruction that is isolated hydronephrosis.
• Oligohydramnios on US indicates poor renal function.
56
Cont…
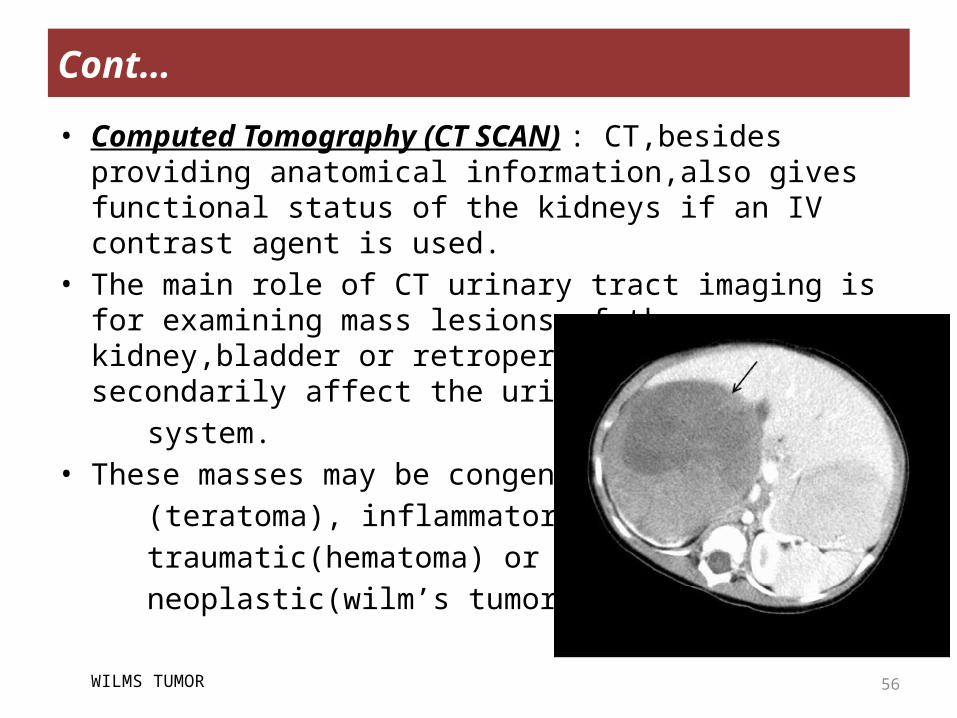
• Computed Tomography (CT SCAN) : CT,besides providing anatomical information,also gives functional status of the kidneys if an IV contrast agent is used.
• The main role of CT urinary tract imaging is for examining mass lesions of the kidney,bladder or retroperitoneum that secondarily affect the urinary
system.• These masses may be congenital (teratoma), inflammatory(abscess), traumatic(hematoma) or neoplastic(wilm’s tumor).
WILMS TUMOR
57
Cont…
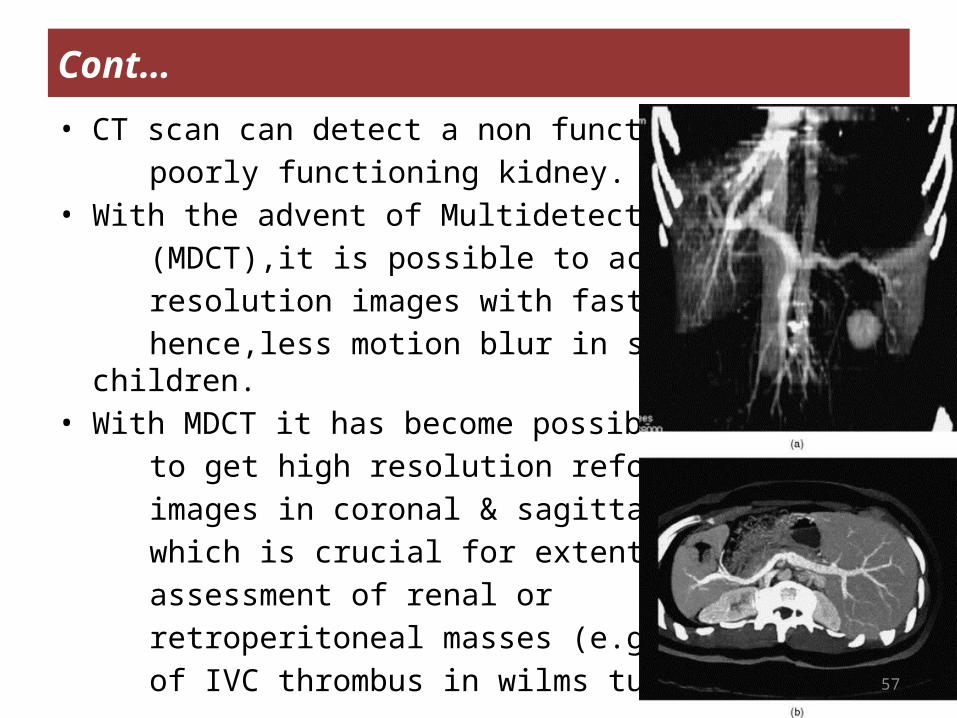
• CT scan can detect a non functioning or a poorly functioning kidney.• With the advent of Multidetector Row CT (MDCT),it is possible to acquire high resolution images with faster speed & hence,less motion blur in small children.• With MDCT it has become possible to get high resolution reformatted images in coronal & sagittal planes; which is crucial for extent assessment of renal or retroperitoneal masses (e.g. extent of IVC thrombus in wilms tumor)
58
Cont…
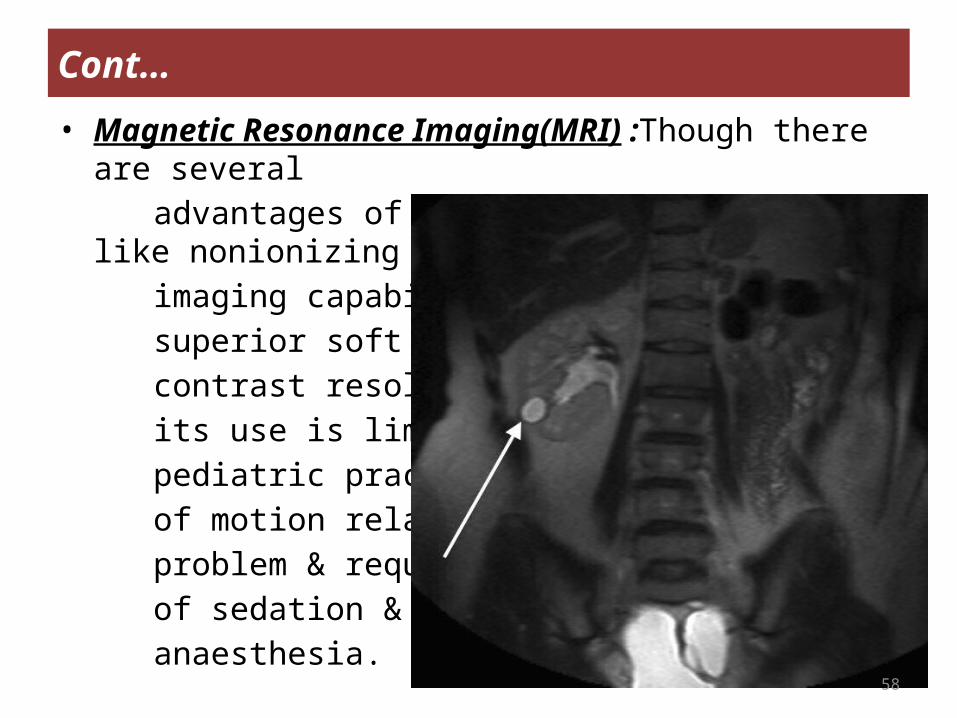
• Magnetic Resonance Imaging(MRI) :Though there are several advantages of this imaging modality like nonionizing
nature,multiplaner imaging capability & superior soft tissue contrast resolution, its use is limited in pediatric practice b’coz of motion related problem & requirement of sedation & general anaesthesia.
59
Cont…
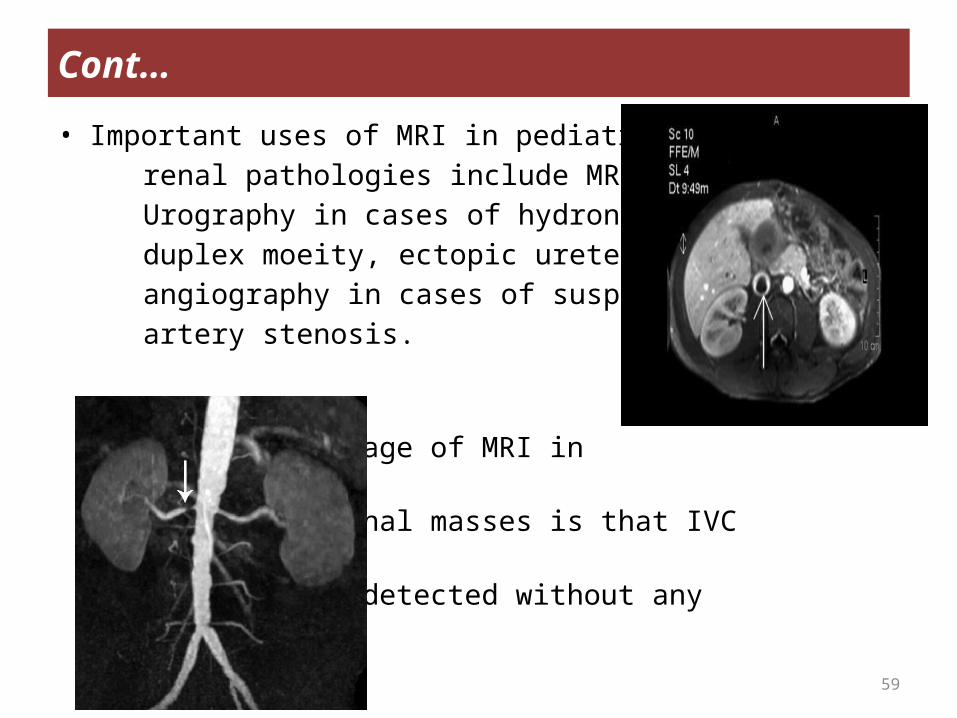
• Important uses of MRI in pediatric renal pathologies include MR Urography in cases of hydronephrosis, duplex moeity, ectopic ureter : MR angiography in cases of suspected renal artery stenosis. The added advantage of MRI in evaluation of renal masses is that IVC thrombus can be detected without any contrast.
60
Cont…
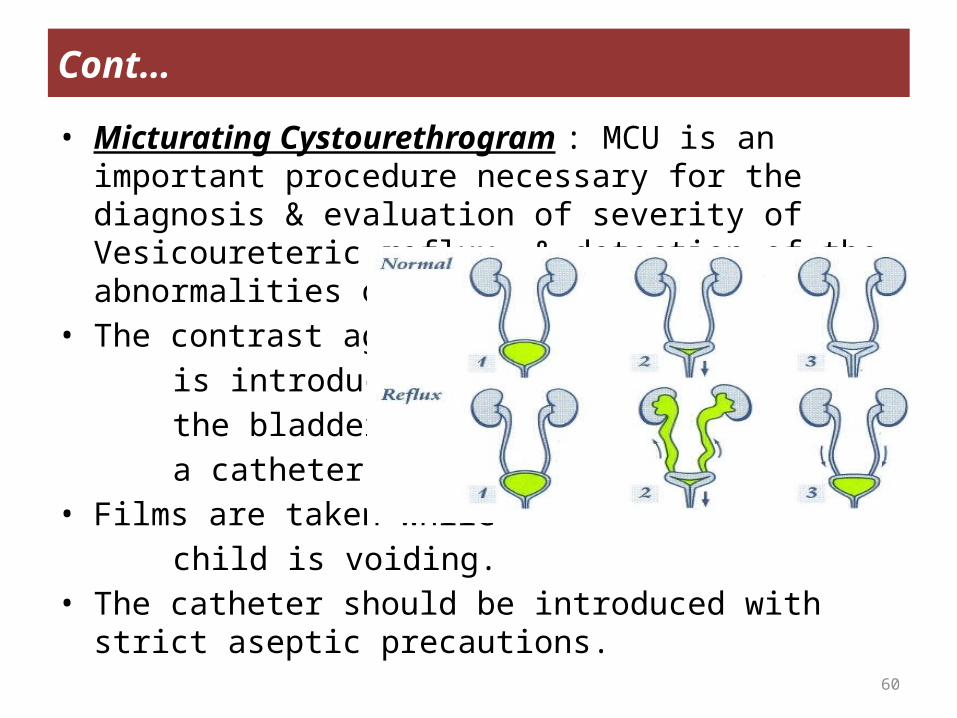
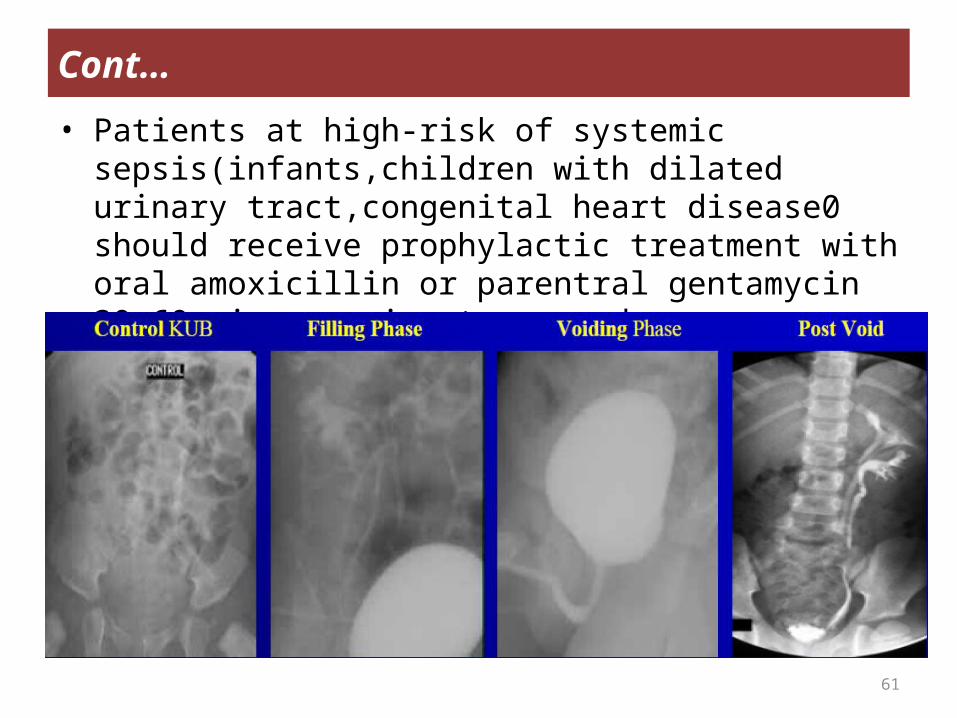
• Micturating Cystourethrogram : MCU is an important procedure necessary for the diagnosis & evaluation of severity of Vesicoureteric reflux, & detection of the abnormalities of bladder & urethra.
• The contrast agent is introduced into the bladder through a catheter.• Films are taken while child is voiding. • The catheter should be introduced with strict aseptic
precautions.
61
Cont…
• Patients at high-risk of systemic sepsis(infants,children with dilated urinary tract,congenital heart disease0 should receive prophylactic treatment with oral amoxicillin or parentral gentamycin 30-60 mins. prior to procedure.
62
Cont…
• Special Imaging Procedures : -Several other imaging procedures are employed to visualize
the urinary system. -these include nephrostogram, ureterostogram, retrograde
pyelogram & angiography.CHOICE OF IMAGING PROCEDURES• US evaluation is usually the 1st procedure in patient with
suspected urinary tract disease.• It is often diagnostic ( e.g. hydronephrosis,cystic disease of
kidney ) or provides enough information to suggest the next appropriate investigation.
63
RADIONUCLIDE STUDIES
• Radionuclide studies are complementary to structural imaging methods of the pediatric urinary tract.
• Nuclear medicine procedures are relatively noninvasive, requring only an i.v injection.
• They require neither fasting nor bowel preparation.• They can be performed on an outpatient basis without the
need for anaesthesia.• They have neither systemic toxic effects(e.g. osmotic
effect,hemodynamic overload) nor allergic reactions,with minimal absorbed radiation dose.
• Radionuclide studies & US evaluation of genitourinary morphology have significantly reduced the need for i.v urography.
64
Cont…
• Radiopharmaceuticals : radiopharmaceuticals used for evaluation of the kidneys may be classified into three principle groups.
A) Radiopharmaceuticals that are rapidly eliminated by the kidneys & thus enable evaluation of filteration & drainage function(Renal Dynamic Scintigraphy) namely 99mTc-DTPA,99mTc-MAG & 99mTc-LL-EC.
B) Radiopharmaceuticals that concentrate in the renal parenchyma for a sufficiently long time to enable detailed scintigraphic mapping of regional functioning renal parenchyma(Renal Cortical scintigraphy) namely 99mTc-DMSA.
65
Cont…
C) Radiopharmaceuticals are either used exclusively for non-imaging clearance studies namely GFR (51Cr-EDTA) or ERPF(131I-OIH) measurements or used for both (99mTc-DTPA, 99mTc-MAG3 & 99mTc-LL-EC)
66
Cont…
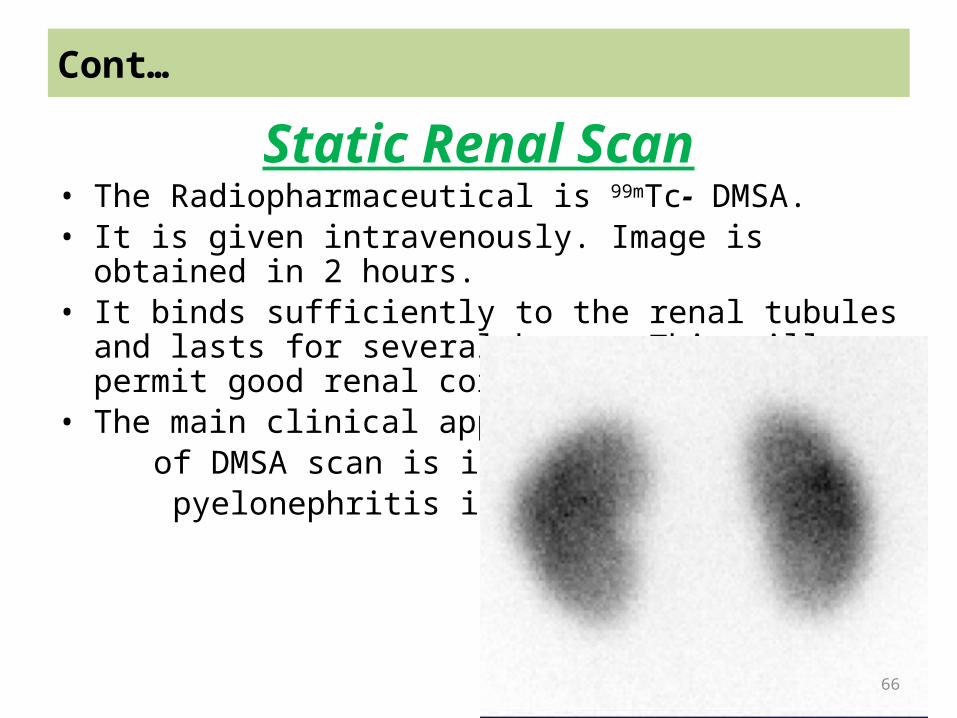
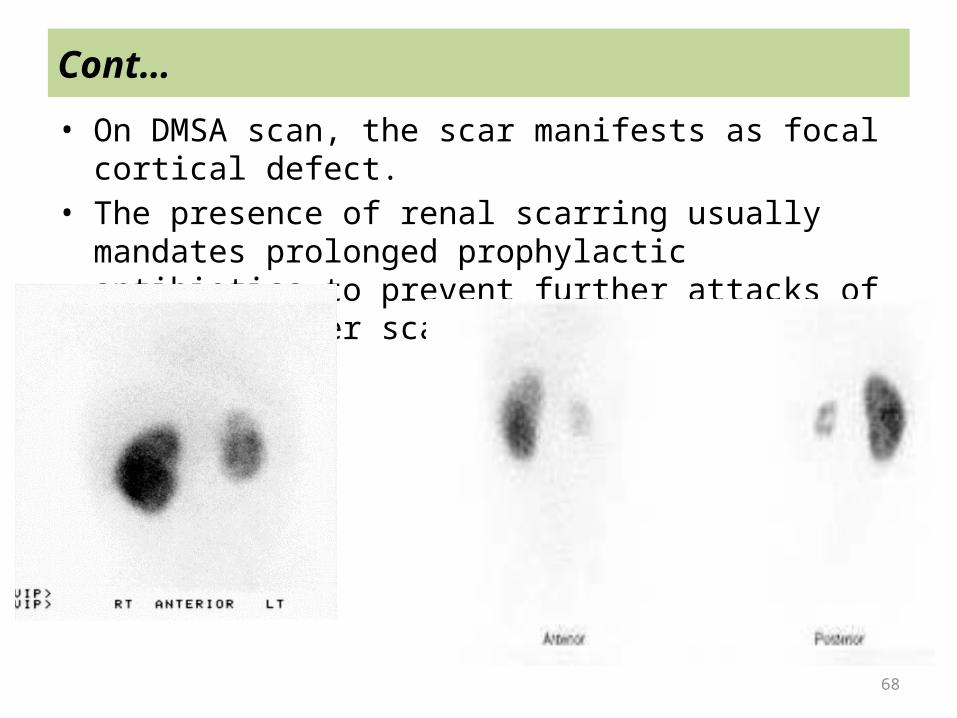
Static Renal Scan• The Radiopharmaceutical is 99mTc- DMSA.• It is given intravenously. Image is obtained in 2 hours.• It binds sufficiently to the renal tubules and lasts for several
hours. This will permit good renal cortical imaging.• The main clinical application of DMSA scan is in acute pyelonephritis in children.
67
Cont…
• Acute Pyelonephritis in Children -The diagnosis of AP in children is difficult based on clinical and
laboratory findings. -Intravenous urography and renal sonography have a low
sensitivity and underestimate the degree of parenchymal involvement.
-DMSA scan is highly sensitive for the diagnosis of acute pyelonephritis in children.
-In acute stage of AP, segmental renal infection causes inflammatory process which results in edema. Edema causes focal vasculature pressure. This will result in ischemia.
-This stage manifests on the scan as focal reduced uptake. -Later on, ischemia resolves completely in most cases or may
progress and scar develops in few cases
68
Cont…
• On DMSA scan, the scar manifests as focal cortical defect.• The presence of renal scarring usually mandates prolonged
prophylactic antibiotics to prevent further attacks of AP and further scarring.
69
Cont…
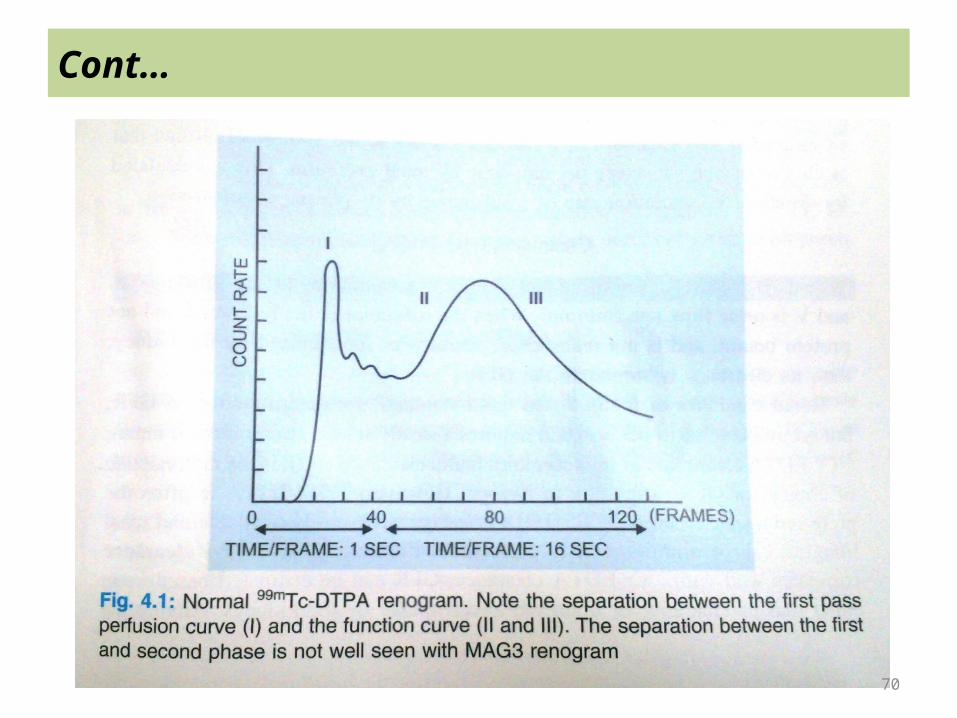
Renal Dynamic Imaging• Renogram is graphical representation of the arrival, uptake & elimination of radiopharmaceutical by the kidneys.• Usually a tracer is injected as a bolus & data collection starts immediately.• The flow of activity through kidneys is recorded for 35-45 mins. & computer reconstructs the renogram when user marks the region of interest over the kidneys.• Renogram has a characteristic shape,& may be considered as having three distinct phases.• Radiopharmaceuticals :Filtered agents (DTPA) Tubular agents (MAG3)
70
Cont…
71
Cont…
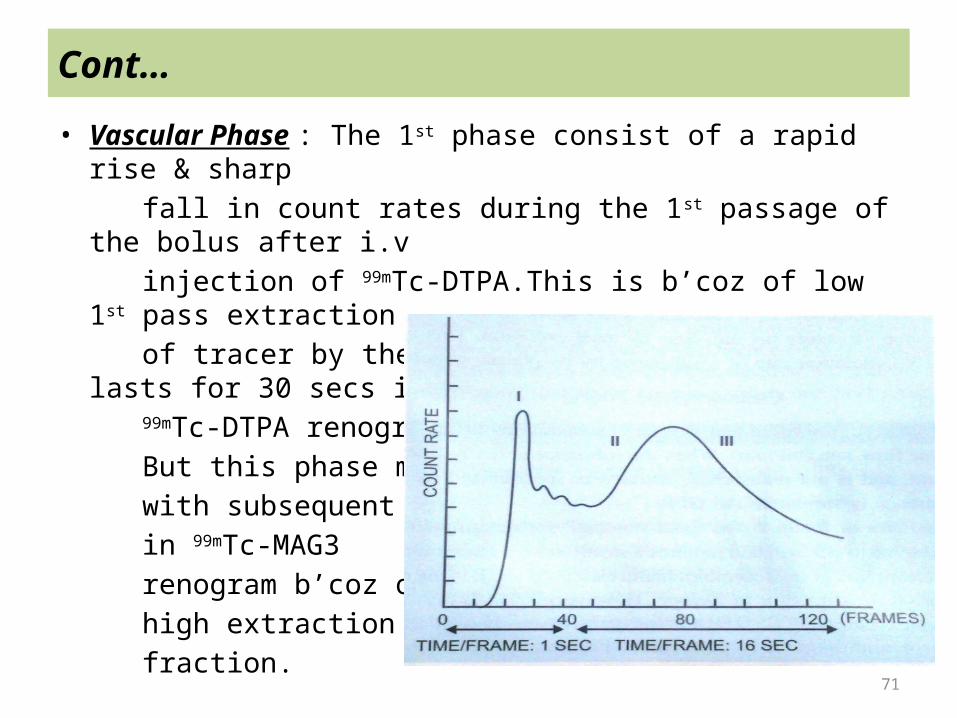
• Vascular Phase : The 1st phase consist of a rapid rise & sharp fall in count rates during the 1st passage of the bolus after i.v injection of 99mTc-DTPA.This is b’coz of low 1st pass extraction of tracer by the kidney.This phase normally lasts for 30 secs in 99mTc-DTPA renogram. But this phase merges with subsequent phase in 99mTc-MAG3 renogram b’coz of high extraction fraction.
72
Perfusion/Vascular phase : 30-60 images are taken over 1 minute immediately post injection.This phase givens an idea
about renal vasculature
Renal Perfusion (Qualitative)
8 mCi 99mTc8 mCi 99mTc--MAG3; imaged @ 2 sec/frameMAG3; imaged @ 2 sec/frame
73
Cont…
• Cortical Transit Phase : This phase corresponds to the renal handling of the radionuclide as it is taken up by the kidneys & passes through the nephrons.In a well hydrated subject,the second phase,the time to reach the peak lasts approximately 180-300 secs after the injection.The time to reach the peak may be delayed by a variety of conditions,such as :
a) An obstructive process preventing or delaying excretion of the tracer.
b) Renal artery stenosis causing a decrease in supply of tracer to the kidney,
c) Dehydrated states producing low urine flow rate, ord) Renal parenchymal disease.
74
Uptake Phase : Image is taken every 15 seconds.This phase represents radiopharmaceutical extraction from
blood stream.Peak uptake is expected in 4-6 minutes post injection
Renal Function (Qualitative and Quantitative)
8 mCi 99mTc8 mCi 99mTc--MAG3; MAG3; imaged @ 4min/frameimaged @ 4min/frame
75
Cont…
• Excretory Phase : The period of declining amplitude after the peak is the 3rd phase of renogram.The beginning of this phase of the renogram corresponds to the time at which activity starts moving away from the region-of-interest & appears in the bladder.The 3rd phase of the renogram curve reflects predominantly the excretory function function of the kidney & measured in terms of its half time(t1/2), i.e the time taken for the counts to decline to one half of the maximum count rate.The excretory phase normally begins 5 mins after injection & usually approaches the baseline about 20 mins after the injection
76
Renal perfusion phase
77
Renal uptake phase
78
Excretory Phase
79
Cont…
• Intraventions During Renogram -Diuretic Renogram :Frusemide is used to produce a rapid
diuresis & helps to differentiate obstructive dilatation from nonobstructive dilatation of upper urinary tract. In the, latter there is prompt clearing of the radionuclide.
-Captopril Renogram : ACE I temporarily dilates the efferent arteries, which are normally vasoconstricted,& thus reduces net filtration pressure & GFR, which is reflected in the renogram.This is the basis of its use in patients with suspected renal artery stenosis.
80
Cont…
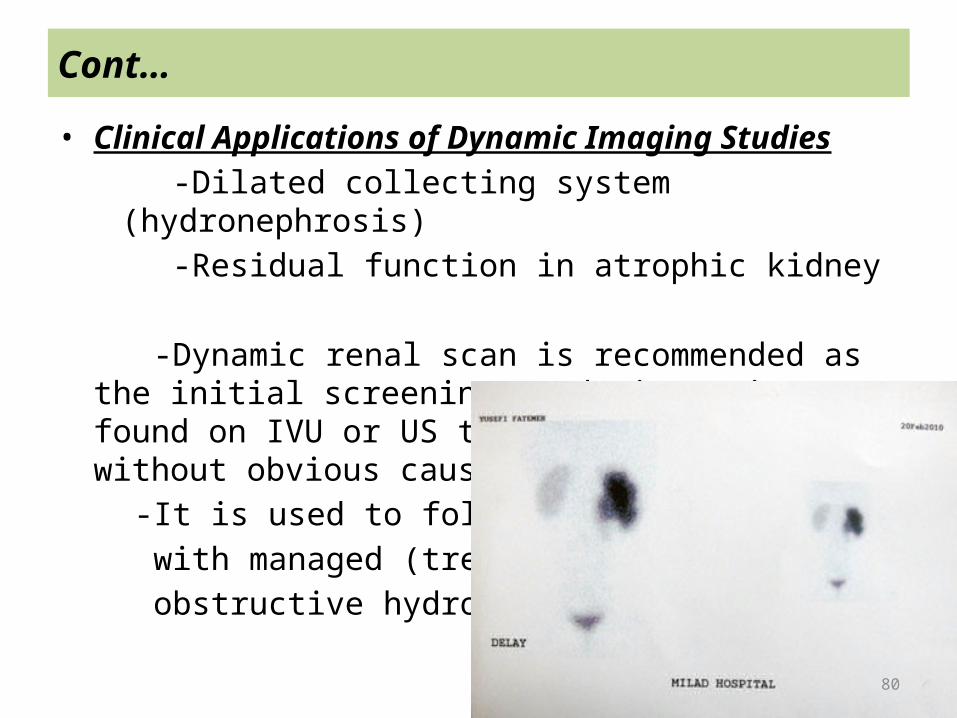
• Clinical Applications of Dynamic Imaging Studies -Dilated collecting system (hydronephrosis) -Residual function in atrophic kidney -Dynamic renal scan is recommended as the initial screening
study in patients found on IVU or US to have hydronephrosis without obvious cause ..
-It is used to follow patients with managed (treated) obstructive hydronephrosis
81
Cont…
GLOMERULAR FILTERATION RATE• The most useful measure of kidney function is the glomerular
filtration rate(GFR).• The total kidney GFR is equal to the sum of the filtration rates in
each of the functioning nephrons• GFR is measured indirectly through the concept of clearance.
Clearance = Ux X V Px Where Ux & Px are urine & plasma concenteration of the
substance X & V is urine flow rate(ml/min).• When a substance is freely filtered & not protein bound,& is not reabsorbed,secreated or metabolised by the kidney,then its clearance is similar to GFR.
82
Cont…
• Renal Clearance of INULIN is the Gold Standard for determination of GFR.
• 51Cr-EDTA clearance closely resembles Inulin clearance & it is the radionuclide of choice for GFR estimation in Europe.
• However, 99m Tc-DPTA is often the preferred agent, because 99m
Tc-DPTA is inexpensive,easily available & renal imaging can be simultaneously performed.
• GFR can be estimated based upon either plasma clearance or upon the tracer uptake by the kidneys.
• The kidney of the newborn & young infant has several functional limitations including a relatively low GFR
• The increases from13-15ml/min/1.73m2 in the premature infant to 15-60ml/min/1.73m2 in the full term infant,to 63-80ml/min/1.73m2 at 8 wks of life.
83
Cont…
• Along with increase in GFR, tubular function of the kidney gradually mature & reach adult level by 1-2 yrs of life.
• Renal uptake of dynamic tracers may be lower in newborns than older children & adults.
• A normal dynamic radionuclide study in newborns during the 1st or 2nd week of life may demonstrate faint,delayed renal uptake of the tracer with or without appearance in the bladder at the expected time.

84
Cont…