Embed Size (px)
Citation preview

Retroperitoneum
Dr. Dhruv Taneja10/04/2012

Retroperitoneum
• The retroperitoneum is the part of the abdominal cavity that lies between the posterior parietal peritoneum and anterior to the transversalis fascia.
• It is divided into three spaces by the peri renal fascia (Fascia's of Gerota and Zukerlandl) and is best visualized using CT or MRI .The Three spaces are:– anterior pararenal space– perirenal space– posterior pararenal space


Retroperitoneal Organs
Retroperitoneal organs– Duodenum and pancreas– Ascending and descending colon– Kidneys and ureters– Bladder and uterus– Great vessels– Rectum

• ARF = Gerota fascia – thinner• PRF = Zuckerkandle fascia -thicker, • Formed of 2 layers 2apposition of ARF and
lateralconal fascia creating potential space


Interfascial Planes
• Tricompartmental anatomy does not completely explain the spread of fluid collections.
• Collections tend to escape site of origin into expandable interfascial planes.

Interfascial Planes
• These interfascial planes are represented by
- Retromesenteric
- Retrorenal
- Lateroconal interfascial plane,
- Combined interfascial planes

Interfascial Planes
The Retromesenteric plane
Expansile plane located between the APR and PRS

Interfascial Planes
The Retrorenal plane
Between the PRS and PPS

Interfascial Planes
The lateral conal interfascial plane
Between layers of the LCF. It communicates with the RMP and RRP at the fascial trifurcation.

Interfascial Planes
The combined interfascial plane
formed by the inferior blending of the RMP and RRP . It continues into the pelvis.

Interfascial Planes
The fascial trifurcation
The point at which the RMP, RRP, and LCF planes communicate mutually

Interfascial Plane Extensions

Interfascial Planes
Medial Extension • RMPs and RRS are continuous across the
midline.

Interfascial Planes
Right superior extension• The superior PRS is in continuity with the bare
area of the liver

Interfascial Planes
Left superior extension• The RMP ,RRP and PRS on the left extend to
the left hemidiaphragm

Anterior Para Renal Space
• Boundaries– Anteriorly: post parietal peritoneum– Posteriorly: ARF– Contents: Ascending and descending colon,
duodenum, pancreas– Continuous across midline, with root of small
bowel mesentery and inferiorly with perirenal, posterior pararenal and prevesical spaces

Retroperitoneal Anatomy
2 . Anterior pararenal space
ColonPancreasDuodenum

Posterior Para renal Space
• Boundaries– Anteriorly: PRF and lateral conal fascia.– Posteriorly: transverse fascia. Limited by and
parallels psoas muscle. – Open laterally to flank and inferiorly to pelvis
– Contents: Fat (no visceral organs)– Continuous (potentially) with each other via pro
peritoneal fat of anterior abdominal wall

Retroperitoneal Anatomy
1 . Posterior pararenal space, Fat connective tissue nerves

• Retro mesenteric - between anterior pararenal and perinephric spaces contiguous across midline and laterally with retro renal and lateral conal space.
• Retro renal - between peri nephric and posterior pararenal spaces·
• Lateral conal – Combined fascial plane continues into pelvis anterolateral
to psoas muscle. – Allowing pathway to pelvis.– Trifurcation of 3 planes - anterioposterior location is variable


Peri Renal Space
• Anterior and post renal fasciae• Extent: Superior, medial, lateral, inferior• Contents:-

Retroperitoneal Anatomy
3. Perirenal space
Kidneys
Adrenal glands
Upper portion of ureters

Extent of Peri Renal Space
• Superior - open to bare area of liver and contiguous with mediastinum.
• Medial - above renal hila perirenal spaces are separate, beginning at level of hila there is communication.
• Lateral - ARF, PRF fuse to form lateral conal fascia
• Inferior - ARF & PRF converge blend about 8 cm below kidney .

Contents of Perirenal Space
Kidney, proximal collecting system, renal septa, adrenal gland, Renal vasculature and perirenal vesselsLymphaticsBridging septa

Spread via Perinephric Bridging Septe
• Thickened septa - nonspecific but may be early sign of renal/perinephric disease
• May preclude complete percutaneous drainage of perinephric fluid collections
• Serve as conduit for spread of fluid, inflammation, neoplasm
• Involvement of septae depends upon rapidity of process

Figure 18. Kidney sweat.
Dyer R B et al. Radiographics 2004;24:S247-S280
©2004 by Radiological Society of North America

Renal Capsule
• Composed of fibrous tissue and smooth muscle.
• Forms a firm, smooth investment for the kidney.
• Will be sharply deflected over margin of a subcapsular collection/mass with flattening and compression of the kidney.

Pathways of Spread of Disease in the Retroperitoneum
• Slowly accumulating, non-aggressive processes confined to 3 main spaces
• Rapidly developing collections accumulate and spread within fascial planes, along bridging septae, and lymphatics

Lymphatic Spread of Disease from Perinephric Space
Small perirenal lymph nodes
Nodes in renal hilum
Periaortic/pericaval nodes

Retroperitoneal collections & their extensions

Types of Collections- hemorrhagic
- bilious
- uriniferous
- enteric
- infectious
- inflammatory
- malignant

Extension of fluid collections
• Fascial planes/adhesions confine retroperitoneal fluid collections to their compartment of origin
• Large or rapidly developing fluid collections may decompress along retroperitoneal fascial planes

Extension of fluid collections
Fluid originating from the APS
Pancreatitis Pancreatic injury Appendicitis abscess of the colonic wall

Extension of fluid collections
Fluid originating from the PRS
Ruptured AAA
Renal injury Hge/urinoma

Extension of fluid collections
Fluid originating from the PPS
bleeding after spinal trauma/surgery

Extension of fluid collections
Pelvic Extension
By the infrarenal retroperitoneal space

Extension of Retroperitoneal Fluid into Pelvis
• Major route - via fused interfascial planes with dorsal extension, medial to iliac vessels (perinephric collections)
• Minor route - dorsal extension lateral to iliac vessels in contact with iliopsoas muscle
• Minor route - medially into prevesical space (anterior parerenal collections)

Infections
• Most originate from kidney• May spread through all spaces and via bare
area to peritoneum and thorax • Xanthogranulomatous pyelonephritis




Collections related to ureteroscopy
• Subcapsular• Perinephric• Pararenal



Para Renal Collection

Hematomas
• Traumatic- MVA, iatrogenic• Spontaneous- tumor, vascular (AAA,AVM,
arteritis), hematologic disorders, end stage kidney
• Spread of hepatic or splenic hematomas to perinephric space without renal injury
• Leaking aortic aneurysm





Acute ureteral calculi
• Secondary findings include: – Thickening of Gerota’s fascia– Perinephric fluid– Renal enlargement– Renal hypodensity.

Retroperitoneal Tumors
• Benign and malignant • Diagnosis is challenging as
– determining tumor location (characterizing the retroperitoneal space and identifying the organ of origin)
– recognizing specific features of various retroperitoneal tumors (evaluating patterns of spread, tumor compo- nents, and vascularity).

Characterization ofthe Retroperitoneal Space
• The first step is to decide whether the tumor is located within the retroperitoneal space.
• Displacement of normal anatomic structures• Anterior displacement of retroperitoneal organs (eg,
kidneys, adrenal glands, ureters, ascending and descending colon, pancreas, portions of the duodenum) strongly suggests that the tumor arises in the retroperitoneum.
• Major vessels and some of their branches are also found in the retroperitoneal cavity, so that displacement of these vessels can be helpful as well.

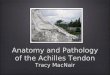
Figure 1. Anterior displacement of the ascending colon.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 2. Anterior displacement of the aorta.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Identification of the Organ of Origin
• Some radiologic signs that are helpful in determining tumor origin include – the “beak sign,” – the “phantom (invisible) organ sign,” – the “embedded organ sign,” and – the “prominent feeding artery sign”

Beak Sign
• When a mass deforms the edge of an adjacent organ into a “beak” shape, it is likely that the mass arises from that organ (beak sign).
• On the other hand, an adjacent organ with dull edges suggests that the tumor compresses the organ but does not arise from it

Figure 4a. Beak sign.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 4b. Beak sign.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 4c. Beak sign.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Phantom (Invisible) Organ Sign
• When a large mass arises from a small organ, the organ sometimes becomes undetectable. This is known as the phantom organ sign.
• However, false-positive findings do exist, as in cases of huge retroperitoneal sarcomas that involve other small organs such as the adrenal gland.

Embedded Organ Sign
• When a tumor compresses an adjacent plastic organ (eg, gastrointestinal tract, inferior vena cava) that is not the organ of origin, the organ is deformed into a crescent shape.
• In contrast, when part of an organ appears to be embedded in the tumor (negative embedded organ sign), the tumor is in close contact with the organ and the contact surface is typically sclerotic with desmoplastic reaction.
• When the embedded organ sign is present, it is likely that the tumor originates from the involved organ.

Figure 5a. Embedded organ sign.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 5b. Embedded organ sign.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 5c. Embedded organ sign.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Prominent Feeding Artery Sign
• Hypervascular masses are often supplied by feeding arteries that are prominent enough to be visualized at CT or MR imaging, a finding that provides an important key to understanding the origin of the mass.

Solid Processes
• RCC-invasion of peri renal fat, thickening of renal fascia
• Lymphoma-multiple renal masses, contiguous retroperitoneal masses, perirenal masses, single renal mass
• Metastasis-to perirenal lymphatics - melanoma, RCC, lung (via pleura/mediastinal connections)
• Fibrosis-AO, IVC, ureters, peri nephric space• Amyloidosis - perirenal soft tissue collections

Specific Patterns of Spread
• Some retroperitoneal tumors have specific patterns of growth and extension that aid in narrowing the differential diagnosis.
• Lesions That Extend Between Normal Structures.— Some tumors grow and extend into spaces between preexisting structures and surround vessels without compressing their lumina. Lymphangiomas and ganglioneuromas are examples of such tumors.

Lymphangiomas
• 1% of all retroperitoneal neoplasms. • Most cases are detected in the first 2 years of life on the
basis of symptoms like abdominal distention or pain; however, they can manifest in older patients as a huge, asymptomatic mass.
• At imaging, they appear as fluid-filled, unilocular or multilocular cystic masses with minimal contrast enhancement.
• Complete excision is the treatment of choice but is often difficult and has high rates of complication and recurrence

Figure 6a. Lymphangioma in a 47-year-old woman.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 6b. Lymphangioma in a 47-year-old woman.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

• Another entity with this growth pattern is lymphoma. This neoplasm tends to surround adjacent vessels, manifesting with the “CT angiogram sign” or “floating aorta sign”

Figure 7. Lymphoma in a 72-year-old woman.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

• Lesions That Extend along Normal Structures.—Tumors of the sympathetic ganglia (ie, paragangliomas, ganglioneuromas) tend to extend along the sympathetic chain and have an elongated shape.

Characteristic Tumor Components
• Some tumor contents can be clearly demonstrated at CT and MR imaging and provide strong clues that help narrow the differential diagnosis.

Fat
• The presence of fat is easily recognized owing to its high attenuation at CT or its high signal intensity at T1-weighted MR imaging with loss of signal intensity on fat-suppressed images. The presence (or absence) of fat limits the differential diagnosis.
• A mass that is homogeneous and well defined and consists almost entirely of fat represents lipoma

Figure 8a. Lipoma.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 8b. Lipoma.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 8c. Lipoma.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Lipo sarcoma• When the mass is somewhat irregular and ill-defined but contains
fat, the diagnosis of liposarcoma should be considered. L• iposarcomas are the most common sarcomas of the
retroperitoneum. • 5th and 6th decades of life, slight female predilection. • They are classified at pathologic analysis into well-differentiated,
pleomorphic, myxoid, and dedifferentiated types. • Well-differentiated liposarcomas usually contain an appreciable
amount of fat, whereas high-grade liposarcomas may not demonstrate appreciable fat, thereby appearing similar to other sarcomas

Figure 9a. Well-differentiated liposarcoma in a 49-year-old woman.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 9b. Well-differentiated liposarcoma in a 49-year-old woman.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Teratoma
• Teratomas are also characterized by the presence of fat, and mature teratomas can be characterized by the presence of fluid attenuation or signal intensity, fat-fluid levels, and calcifications

Radiologic Features
• The morphologic features of teratoma extend from predominantly cystic to completely solid lesions.
• Fat and calcifications, • If the fat appears with the configuration of
sebum (ie, fat attenuation or signal that horizontally interfaces with a nonfatty mate- rial), this feature is thought to be nearly pathognomonic for teratoma

• US is highly sensitive teratomas because the lesions are usually quite large at initial presentation. Typical findings include a complex echogenic mass with solid and cystic components that may or may not have acoustic shadowing, depending on the presence of calcification.
• CT is more reliable in the unequivocal identification of fat. Calcification was detected in patterns that were characterized as congealed, linear, and shard like. A tooth like structure was seen.
• MR imaging demonstrates, A complex mass with both solid and fluid components. The pseudocapsule of the mass is usually easier to identify with MR imaging because of its hypointense rim. This feature is helpful for excluding invasion of adjacent structures. Fat within the lesion characteristically has high signal intensity on T1-weighted images and may be more readily identifiable with MR imaging than with CT. In addition, the chemical shift between fat and water content is a helpful diagnostic finding.

Figure 10b. Mature cystic teratoma in a female infant.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 10a. Mature cystic teratoma in a female infant.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Myxoid Stroma
• Myxoid stroma is characterized pathologically by a mucoid matrix that is rich in acid mucopolysaccharides.
• Myxoid stroma appears hyperintense on T2-weighted MR images and shows delayed enhancement after injection of contrast medium.
• Tumors that commonly contain myxoid stroma include – neurogenic tumors (schwannomas, neurofibromas,
ganglioneuromas, ganglioneuroblastomas, malignant peripheral nerve sheath tumors),
– myxoid liposarcomas, and– myxoid malignant fibrous histiocytoma.

• Schwannomas are the most common tumor of peripheral nerves. • Schwannomas are well encapsulated and contain cells that are identical
to Schwann cells. • Their MR imaging appearance depends on the types of tissue they
contain. Myxoid tissue is hyperintense on T2-weighted images, cellular tissue is hypointense on both T1- and T2-weighted images, and solid fibrous tissue enhances on contrast-enhanced images.
• Neurofibromas tend to have high signal intensity on T2-weighted MR images and are often multiple and associated with neurofibromatosis.
• Ganglioneuromas are typically located along the sympathetic chain and tend to be larger, more rounded, and contain calcification more frequently than nerve sheath tumors. The relatively younger age of affected patients may aid in differentiating ganglioneuromas from other neurogenic tumors.

Figure 11b. Schwannoma in a 70-year-old man.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 12. Neurofibromas in a patient with neurofibromatosis type 1.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 13b. Ganglioneuroma in a 21-year-old man.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 14a. Myxoid liposarcoma as a part of well-differentiated liposarcoma.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 14b. Myxoid liposarcoma as a part of well-differentiated liposarcoma.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Necrosis
• Necrotic portions within tumors have low attenuation without contrast enhancement at CT and are hyperintense at T2-weighted MR imaging.
• Necrosis is usually seen in tumors of high-grade malignancy such as leiomyosarcomas.
• When they occur in the retroperitoneum, leiomyosarcomas tend to develop massive cystic degeneration. They have central necrosis more commonly than other sarcomas, whereas fat and calcifications are not typically present

Figure 15a. Leiomyosarcoma in a 48-year-old woman.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 15b. Leiomyosarcoma in a 48-year-old woman.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Cystic Portion
• Some tumors are completely cystic in appearance. These include lymphangiomas and mucinous cystic tumors.
• Solid tumors with a partially cystic portion include neurogenic tumors

Figure 17a. Retroperitoneal mucinous cystic tumor.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Small Round Cells
• At T2-weighted MR imaging, tumors composed of small round cells often appear as homogeneous masses with relatively hypointense areas representing densely packed cellular components.
• Lymphomas are the most commonly encountered tumors composed of small round cells. They are homogeneous, with minimal contrast enhancement at CT and relatively low signal intensity at T2-weighted MR imaging. An exception is primitive neuroectodermal tumor (PNET), which often appears heterogeneous at MR imaging

Figure 18a. Lymphoma in a 64-year-old woman.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Figure 19a. PNET in a 16-year-old boy.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Vascularity
Vascularity is another important feature of retroperitoneal tumors. Extremely hypervascular tumors include paragangliomas and hemangiopericytomas. Moderately hypervascular tumors include myxoid malignant fibrous histiocytomas, leiomyosarcomas, and many other sarcomas. Hypovascular tumors include low-grade liposarcomas, lymphomas, and many other benign tumors

Figure 20a. Malignant paraganglioma in a 57-year-old man.
Nishino M et al. Radiographics 2003;23:45-57
©2003 by Radiological Society of North America

Retroperitoneal Fibrosis
• Most commonly idiopathic• Other causes: aortic hemorrhage, aortitis,
methysergide toxicity, prior surgery or XRT, collagen vascular disease (Riedel’sthyroiditis, sclerosing mediastinitis)
• Clinical: 40-6 0 yrs, males > females• Hydronephrosis, ureteral narrowing, slight
medial ureteral displacement



Hibernoma
Hibernoma is a rare, benign, soft-tissue tumor composed of brown fat. The name hibernoma is derived from histologic similarities between these tumors and the brown fat identified in hibernating animals. Arise in these locations, which include the thigh, buttock, scapular region, trunk, neck, mediastinum, chest wall, perirenal areas, breast, scalp, and periureteric regions

Radiologic Features
• At US, the lesions appear echogenic, with both well-defined and ill-defined borders. Vascular analysis with Doppler or color flow US demonstrates that these lesions have increased flow in large surface vessels that are also visible with CT.
• At CT, a low-attenuation, well-defined lesion with intratumoral septa is typically seen.
• On C +, the septa will enhance, with generalized enhancement throughout the mass occasionally occurring as well.
• These soft-tissue septations manifest with attenuation that averages slightly above that of subcutaneous fat.
• Calcifications are notably absent

• The spectrum of MR imaging characteristics includes a few cases in which the hibernoma appears very similar to fat (isointense on T1- and T2-weighted images, with minimal if any enhancement).



Neoplastic Cysts • Cystic lymphangiomas are uncommon, congenital benign tumors and
occur due to failure of the developing lymphatic tissue to establish normal communication with the remainder of the lymphatic system.
• Most occur in the head or neck; a retroperitoneal location is unusual. • Cystic lymphangiomas can occur anywhere in the perirenal,
pararenal, or pelvic extra- peritoneal spaces. • Cystic lymphangiomas are more common in men and can occur at
any age.• At CT, cystic lymphangioma typically appears as a large, thin-walled,
multiseptate cystic mass. Its attenuation values vary from that of fluid to that of fat. An elongated shape and a crossing from one retroperitoneal compartment to an adjacent one are characteristic of the mass.


• Primary mucinous cystadenomas are rare retro- peritoneal cystic lesions that occur in women with normal ovaries.
• Primary retroperitoneal mucinous cystadenoma usually manifests as a homogeneous, unilocular cystic mass at CT. Differentiating this mass from cystic mesothelioma, cystic lymphangioma, and nonpancreatic pseudocyst is difficult.


• Cystic mesotheliomas are rare benign neoplasms with a mesothelial origin that originate in the serous lining of the pleural, pericardial, or peritoneal space.
• Unlike malignant mesothelioma, cystic mesothelioma is not related to prior asbestos exposure. It does not metastasize but may recur locally and occurs more frequently in women.
• Cystic mesotheliomas usually appear as non- specific, thin-walled, multilocular cystic lesions at CT. They may be radiologically indistinguishable from lymphangiomas and other retro-peritoneal cysts.

• Urogenital cysts arise from vestiges of the embryonic urogenital apparatus and can be classified into pronephric, mesonephric, metanephric, and mu ̈�llerian types based on their embryonic lines.
• Mu llerian cyst of the retroperitoneum occurs in ̈�women from 19 to 47 years of age.
• At CT, mu llerian cyst manifests as a unilocular or ̈�multilocular thin-walled cyst containing clear fluid. The differential diagnosis includes cystic mesothelioma and cystic lymphangioma


Epidermoid cysts
• At CT, epidermoid cysts generally appear as thin-walled, unilocular cystic masses with fluid attenuation

Tailgut cysts
• Tailgut cysts are rare congenital multicystic lesions that arise from vestiges of the embryonic hindgut and occur between the rectum and sacrum.
• Tailgut cyst is more common in women and usually appears in middle age.
• At CT, tailgut cyst appears as a well-defined multicystic mass with attenuation values varying from that of water to that of soft tissue.

Pseudomyxoma Retroperitonei
• Pseudomyxoma peritonei is a rare condition that is characterized by intraperitoneal accumulation of gelatinous material owing to the rupture of a mucinous lesion of the appendix or ovary
• The imaging findings in pseudomyxoma retro- peritonei are similar to those in pseudomyxoma peritonei. At CT, pseudomyxoma retroperitonei appears as multicystic masses with thick walls or septa that displace and distort adjacent structures

Non Neoplastic Lesions
• Pancreatic Pseudocyst.• Non pancreatic Pseudocyst.• Lymphocoele.• Urinoma• Hematoma.

Thank You !!