Embed Size (px)
Citation preview

Selecting Optimal Therapeutic Strategies for
Patients With Differentiated and Medullary
Thyroid Cancer
Jochen Lorch, MD, MS
Assistant Professor of Medicine
Harvard Medical School

Disclosures
Dr. Lorch discloses the following commercial
relationships:
◼ Consultant: Eisai
◼ Research Support: Bayer, Bristol-Myers Squibb, Millennium

Learning Objectives
▶ Assess risk-adapted approaches to the
management of thyroid cancer
▶ Evaluate efficacy and safety data on novel
therapies for differentiated and medullary thyroid
cancer
▶ Apply posttreatment monitoring strategies to ensure
optimal outcomes for patients with thyroid cancer

Thyroid Cancer Scope of Problem
▶ Most common endocrine cancer◼ An estimated 56,870 cases per year in US
◼ Incidence rising: 5% increase between 2004-2013
◼ Relatively stable mortality rate at 0.5 deaths per 100,000 people
but may be rising as well
▶ Subtypes◼ Papillary ~80%
◼ Follicular ~10%
◼ Poorly differentiated 5-10%
◼ Medullary 4%
◼ Anaplastic 2%
ACS, 2017; ACS, 2016.

Traditional Approach to
Thyroid Nodules >1-1.5 cm
TSH = thyroid-stimulating hormone.
Haugen et al, 2016.
Initial AssessmentUltrasound
Check TSH
Normal or Elevated
(~95%)Suppressed
(<5%)
Fine Needle Aspiration Thyroid Scan
(Noncancerous)

Thyroid Nodule FNA:
High Rate of Indeterminate Cytology
Courtesy of Erik K. Alexander, MD.
Cooper et al, 2006.
~5%
Malignant (Papillary Carcinoma)
~65-70%
No Malignant Cells
~20-25%
Indeterminate
“Suspicious for
malignancy”
“Suspicious for a follicular
neoplasm”
“Atypical (follicular) lesion
of uncertain significance”
~5%
Nondiagnostic

The Problem: Low Specificity of
Indeterminate Cytology
US = ultrasound; UG-FNA =ultrasound-guided fine-needle aspiration.
Yassa et al, 2007.
~4,595 consecutive thyroid nodules evaluated with US and UG-FNA
Despite recommendations for surgery, >50% of patients with “abnormal”
cytology are proven to have benign disease.
FNA CytologyProportion Cancer on
Histopathology
Suspicious for papillary
carcinoma60%
Suggestive of a follicular
neoplasm28%
Atypical of an undetermined
significance24%

Gene Expression
FNA = fine-need aspiration; AUS/FLUS = atypia (or follicular lesion) of undetermined significance;
FN/SNF = follicular neoplasm/suspicious for follicular neoplasm; NPV = negative predictive value.
Alexander et al, 2012.
Afirma Gene Expression Classifier – 164 Genes
Prospective, blinded, study with nodules >1 cm
1-2 additional samples after FNA (“standard of care approach”)
Comparison with 2-expert, blinded, gold-standard histopathology
n=129
Performance on All
IndeterminateCytology AUS/FLUS Cytology FN/SNF
NPV: 95% NPV: 94%NPV: 93%
n=265 n=81
False-negative rate similar to benign cytology
High NPV prevents unnecessary surgery
95% 94%

Pre-Operative Imaging
▶ Helps avoid incomplete surgery
▶ Recurrence rates up to 35%◼ Most within 5 years
◼ Some due to inadequate surgery
▶ Ultrasound to evaluate primary tumor and nodes
recommended in all patients
▶ Cross-sectional imaging used in a minority of patients◼ Indistinct margins between tumor and major vessels, esophagus,
airway
◼ Bulky nodal disease incompletely imaged with US
◼ Nodal disease in deep structures of the neck or mediastinum
Yeh et al, 2015.

Surgery: Mainstay of Therapy
▶ Total thyroidectomy for tumors
>1 cm◼ ATA guidelines now recommend
lobectomy for low-risk cancers– <4 cm
– No clinical evidence of nodes
– No extrathyroidal extension
▶ Lobectomy for unifocal cancer
<1 cm◼ No clinical evidence of nodes
◼ No history of radiation therapy or
familial thyroid cancer
ATA = American Thyroid Association.
Haugen et al, 2016.

Postoperative Risk Stratification
▶ AJCC staging: Predicts mortality not recurrence
▶ Operative report◼ Gross extrathyroidal extension
◼ Completeness of resection
▶ Specific histology
▶ Mutational status (BRAF?, BRAF + TERT promoter,
PIK3CA, TP53, AKT1)
▶ Postoperative serum thyroglobulin testing
AJCC = American Joint Committee on Cancer.
Omry-Orbach, 2016.

Postoperative Risk Stratification (cont.)
▶ Post-op I123 or I131 scans◼ May be useful in select cases
◼ Avram and colleagues (2015):– I131 scan detected nodal or distant metastatic disease in
29.4% of cases, which lead to management changes
– Many of these also had elevated post-op Tg
▶ Post-op PET/CT◼ FDG+ predicts poorer outcome and radioiodine resistance
◼ Recommended in patients with aggressive histology and
Tg >10 ng/mL
◼ Can have false-positive rate of 0-39%
PET/CT = positron emission tomography/computed tomography;
FDG = fluorodeoxyglucose; Tg = thyroglobulin.
Nascimento et al, 2015; Avram et al, 2015.

Differentiated Thyroid Cancer:
AJCC Staging
Primary tumor (T)
TX Primary tumor cannot be assessed
TO No evidence of primary tumor is found
T1 Tumor size ≤ 2 cm in greatest dimension and is
limited to the thyroid
T1
aTumor ≤ 1 cm, limited to the thyroid
T1
b
Tumor > 1 cm but ≤ 2 cm in greatest dimension,
limited to the thyroid
T2Tumor size > 2 cm but ≤ 4 cm, limited to the thyroid.
T3Tumor size >4 cm, limited to the thyroid or any tumor
with minimal extrathyroidal extension (eg, extension
to sternothyroid muscle or perithyroid soft tissues)
T4
a
Moderately advanced disease; tumor of any size
extending beyond the thyroid capsule to invade
subcutaneous soft tissues, larynx, trachea,
esophagus, or recurrent laryngeal nerve
T4
b
Very advanced disease; tumor invades prevertebral
fascia or encases carotid artery or mediastinal
vessel
Edge et al, 2010.
Regional lymph nodes (N)
Regional lymph nodes are the central compartment, lateral
cervical, and upper mediastinal lymph nodes:
NX Regional nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Regional lymph node metastasis
N1a Metastases to level VI (pretracheal, paratracheal,
and prelaryngeal/Delphian lymph nodes)
N1bMetastases to unilateral, bilateral, or contralateral
cervical (levels I, II, III, IV, or V) or retropharyngeal
or superior mediastinal lymph nodes (level VII)
Distant metastasis (M)
M0Metastases to unilateral, bilateral, or contralateral
cervical (levels I, II, III, IV, or V) or retropharyngeal
or superior mediastinal lymph nodes (level VII)
M1 Distant metastasis is present

Edge et al, 2010.
Papillary and follicular thyroid cancer (age <45y):
Stage T N M
I Any T Any N M0
II Any T Any N M1
Papillary and follicular; differentiated (age > 45y):
Stage T N M
I T1 N0 M0
II T2 N0 MO
III T3 N0 M0
IVAT1-3 N1b M0
T4a N0-1b M0
IVB T4b Any N M0
IVC Any T Any N M!
Differentiated Thyroid Cancer:
AJCC Staging (cont.)

ATA 2009 Risk Stratification
Haugen et al, 2016.

Risk of Recurrence as a Continuum
Haugen et al, 2016.

DTC: Mutational Landscape
▶ 402 cases, whole exome sequencing performed
▶ Low frequency of somatic alterations
▶ Mutation density correlates with age, risk of recurrence, MACIS score
▶ BRAF V600E in 61.7%, RAS (N-, H- and KRAS) 12.9%
▶ Along PI3K axis: 20/402 (5%)
DTC = differentiated thyroid cancer.
Agrawal et al, 2014.

DTC: BRAF vs RAS
Agrawal et al, 2014.

DTC: Metastatic Disease
▶ Metastatic disease frequently affects: ◼ Lungs (49%)
◼ Bones (25%)
◼ Both (15%)
▶ RAI if significant iodine uptake is detected on scans
➔ remission ~30%
▶ May follow indolent course with slow disease
progression on TSH suppression
▶ Disease considered RAI refractory if:◼ At least one lesion with no uptake
◼ Progression within 1 year following RAI
◼ Persistent disease following dose of 600 mCi
RAI = radioactive-iodine refractory.
NCCN, 2017; Haugen et al, 2016.

RAI-Refractory DTC: Characteristics
▶ Inverse relationship between ◼ BRAF and RET mutations/rearrangements
◼ FDG and RAI avidity
Ricarte-Filho et al, 2009; Cantwell-Doris et al, 2011; Xing et al, 2013.

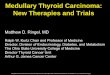
Modulating RAI Uptake in Refractory
Disease Through MEK Inhibition
▶ Selective MAPK pathway antagonists increase the expression of
the sodium-iodide symporter and uptake of iodine in animal models
▶ Selumetinib MAPK kinase inhibitor (MEK1 and MEK2) ◼ 20 patients with RAI-refractory thyroid cancer evaluated:
– 9 BRAF+
– 5 NRAS+
◼ 12/20 patients demonstrated increased uptake of I124
– 4/9 patients with BRAF mutations
– 5/5 patients with NRAS mutations
◼ 8 patients reached the dosimetry threshold for radioiodine therapy, including all
5 patients with NRAS mutations
◼ 5 had confirmed PR and 3 had SD; all patients had decreases in serum
thyroglobulin levels (mean reduction 89%)
◼ No toxicities grade ≥3 attributable to selumetinib observed
PR = partial response; SD = stable disease; MAPK = mitogen-activated protein kinase.
Ho et al, 2013.

Modulating RAI Uptake in
Refractory Disease: Selumetinib
Ho et al, 2013.
RAI RAI + Selumetinib RAI RAI + Selumetinib

RAI-Refractory Metastatic Disease
▶ Doxorubicin◼ Response rate 10-30%
◼ No known impact on survival
▶ Carboplatin, paclitaxel and docetaxel, bleomycin◼ Response rates approximately 10-30%, usually short lived
Until recently, RAI-refractory disease was NOT
considered treatable.
NCCN, 2017.

DECISION Phase III: Sorafenib vs Placebo
in RAI-Refractory DTC
▶ Double-blind, randomized, multicenter phase III
▶ Patients with locally advanced/metastatic RAI-refractory DTC
▶ Progression within 14 months
▶ Randomly assigned 1:1 to sorafenib 400 mg BID PO or placebo, crossover
allowed
▶ Primary end point: PFS
▶ 417 patients randomly assigned (207 to sorafenib and 210 to placebo)
BID = twice daily; PO = by mouth; PFS = progression-free survival.
Brose et al, 2014.
Treatment until progression
or unacceptable toxicity
Locally advanced
or metastatic RAI
refractory DTC
Sorafenib 800 mg
Placebo
1:1 Randomization
PR
OG
RE
SS
ION
Survival follow-up

DECISION: PFS
▶ Median PFS 10.8 mo for sorafenib vs 5.8 mo for placebo ◼ HR=0.59; 95% CI: 0.45-0.76; P<0.0001
▶ No difference in OS (crossover allowed)
Brose et al, 2014.
All Cohorts

DECISION: PFS in BRAF Mutants
WT = wild type.
Brose et al, 2014.
BRAF WT
BRAF V600E
(27% sorafenib,
31.4% placebo)
BRAF V600: 20.5 vs 9.4 mo; HR=0.46; P=0.02
BRAF WT: 8.9 vs 3.8 mo; HR=0.55; P<0.001

SELECT Phase III: Lenvatinib in DTC
▶ Design similar to DECISION study
▶ 392 patients randomly assigned (2:1), double-blind, placebo-controlled
▶ Documented disease progression within 13 months
▶ Crossover to open-label lenvatinib allowed upon progression
▶ Primary end point: PFS
Schlumberger et al, 2015; Stjepanovic & Capdevila, 2013.

SELECT: PFS
▶ PFS 18.3 mo (15.1-NR) vs 3.6 mo (2.2-3.7)
▶ 4 CRs (1.5%)
▶ Benefit similar for BRAF-positive and BRAF-WT cases
▶ No difference in OS except for older (>65 years) patients
OS = overall survival; NR = not reached.
Schlumberger et al, 2015.

Schlumberger et al, 2015.
SELECT: Subgroup Analysis

Nonapproved Therapies

Targeting BRAF: Vemurafenib in
BRAF-Positive PTC
▶ 51 patients with RAI-refractory progressive PTC positive for BRAF
V600E mutation
◼ Cohort 1 (n= 26) if TKI treatment naive
◼ Cohort 2 (n= 25) if previously treated with TKIs
▶ Cohort 1 vs Cohort 2 results:
◼ PRs in 38.5% and 27.3%, no complete response
◼ Clinical benefit rate (CR + PR + SD = 6 months) was 58% and 36%
◼ Median PFS at the time of data cut-off for the analysis was 18.2 mo
(95% CI: 15.5-29.3) and 8.9 mo (95% CI: 5.5-NE)
◼ Cutaneous squamous cell cancer in 27% and 20%
▶ Other grade 3/4 toxicity: Liver 4%
▶ 2 deaths reported on study, not felt to be treatment related
PTC = papillary thyroid cancer; TKI = tyrosine kinase inhibitor; CR = complete response. NE = not estimable.
Brose et al, 2016.

Everolimus in DTC:
Key Eligibility Criteria
▶ Main cohort: ◼ RAI-refractory DTC (n=33)
▶ Disease progression within 6 months prior to
enrollment
▶ PS 0-2
PS = performance status.
Lorch et al, 2013.

Everolimus in DTC: PFS
▶ PFS 12.3 mo (95% CI: 10-NR)
▶ Disease stability for 6 mo achieved in 19/33 patients
▶ Disease stability for 12 mo or more in 11/33 patients
Lorch et al, 2016.
Progression-Free Survival
Months
Su
rviv
al
0 5 10 15 20 25
25
50
75
100

Future Directions in RAI-Refractory DTC
▶ Lenvatinib plus PD-1 inhibition◼ ITOG study opening 2017/18
▶ Second-generation mTOR inhibitors◼ MLN0128
▶ Immunotherapy with PD-1/CTLA-5 inhibitors◼ Pembrolizumab in 22 patients with RAI-refractory thyroid cancer
– 2 patients had a PR for an ORR (confirmed) of 9.1%
(95% CI:1.1-29.2)
ITOG = International Thyroid Oncology Group; ORR = overall response rate.
Mehnert et al, 2016.

Medullary Thyroid Cancer
▶ Derived from parafollicular C cells
▶ Usually presents with solid mass
▶ Frequently secretes:◼ CEA, calcitonin
◼ VIP ➔ diarrhea
◼ ACTH ➔ Cushing’s disease
▶ Metastatic disease frequently affects
mediastinum, lung, bone, and liver
▶ Growth rate ranging from indolent to
extremely aggressive
Courtesy of Justine Barletta, MD and Cheryl Adackapara, MD.
NCCN, 2017; Haugen et al, 2016.

Medullary Thyroid Cancer (cont.)
▶ Sporadic MTC accounts for 75% of cases, familial MTC
25%
▶ Familial MTC occurs in association with multiple
endocrine neoplasia (MEN) type 2A and 2B syndromes,
but non-MEN familial MTC can also occur
▶ Sporadic and familial cases usually involve mutation of
RET proto-oncogene
MTC = medullary thyroid cancer.
Zbuk & Eng, 2007.
Sporadic MEN2A/B
RET mutation Somatic Germline
Age (Average years) 40-45 15-25
Associated tumors –
MEN2A: MTC, pheochromocytoma, parathyroid hyperplasiaMEN2B:
MTC, pheochromocytoma, intestinal/mucosal ganglioneuromatosis,
marfanoid habitus

MTC Therapy
▶ Aggressive surgery: Complete thyroidectomy with bilateral central
compartment node dissection and unilateral neck dissection
▶ Adjuvant radiotherapy considered largely ineffective with no impact
on survival
▶ Local recurrence treated surgically
▶ Systemic disease: ◼ Often indolent with no significant progression over long period
of time
◼ Increase in calcitonin without radiographic evidence for disease
progression does not indicate need for systemic therapy
NCCN, 2017; Haugen et al, 2016.

Phase III: Vandetanib in MTC
▶ Double-blind, placebo-controlled trial◼ 331 patients with advanced MTC
◼ Measurable disease (no progression required),
calcitonin level >500 pg/mL
◼ Vandetanib 300 mg (n=231) or placebo (n=100)
◼ Crossover allowed
◼ Primary end point: PFS
Wells et al, 2012.
Treatment until progression
or unacceptable toxicity
Locally advanced
or metastatic RAI
refractory MTC
Vandetanib 300 mg
Placebo
1:1 Randomization
PR
OG
RE
SS
ION
Survival follow-up

Vandetanib in MTC: PFS
▶ 54% reduction in the rate of progression (HR=0.46; P=0.001)
▶ PFS NR in vandetanib arm, 19.3 mo for placebo
▶ Objective response rate (ORR) 45% vs 13% (P<0.001)
Wells et al, 2012.
P=0.001

Vandetanib in MTC: OS
▶ No difference in OS
▶ Subgroup analysis showed
no association with patient
characteristics (but small n
in some categories)
Wells et al, 2012.
Overall
Male
Female
White
Other
PS 1-2
PS 0
Hereditary
Sporadic or unknown
Locally advanced
Metastatic
≥1 prior Rx
No prior therapy
Response to prior Rx
No response to prior Rx
Unknown

Phase III: Cabozantinib in MTC
▶ Randomized, placebo-controlled study
▶ 330 patients with locally advanced or metastatic MTC
▶ Documented RECIST progressive disease within
14 mo of screening
▶ No limit on prior therapy
▶ Primary end point: PFS
Schöffski et al, 2012.
Treatment until progression
or unacceptable toxicity
Locally advanced
or metastatic MTC
with documented
RECIST
progression
Cabozantinib 140 mg
Placebo
1:1 Randomization
PR
OG
RE
SS
ION
Survival
follow-upNo Cross-over
No Unblinding

Cabozantinib in MTC: PFS
Elisei et al, 2013.
PFS: 11.2 vs 4.0 mo (HR=0.28 95%; CI: 0.19-0.40; P<0.001)

Cabozantinib in MTC:
Subgroup Analysis
▶ RET M918T subgroup
greatest PFS benefit from
cabozantinib vs placebo
(HR=0.15; 95% CI: 0.08-
0.28; P<0.0001)
Elisei et al, 2013; Sherman et al, 2016.

Vandetanib vs Cabozantinib in MTC:
Adverse Events
GI = gastrointestinal.
Wells et al, 2012; Schöffski et al, 2012.
Vandetanib
N=231
Cabozantinib
N=214
Adverse EventAll
n (%)
Grade ≥3
n (%)
All
n (%)
Grade ≥3
n (%)
Hypertension 73 (32) 20 (9) 70 (33) 18 (8)
Fatigue 55 (24) 13 (6) 87 (41) 20 (9)
Diarrhea 130 (56) 25 (11) 135 (63) 34 (16)
Hemorrhage NR NR 54 (25) 7 (3)
Venous thrombosis NR NR 12 (6) 8 (4)
GI perforation NR NR 7 (3) 7(3)
Non-GI fistula NR NR 8 (4) 4 (2)
QT prolongation 33(14) 18 (8) NR NR

MTC Trials
▶ RET inhibitors: Ponatinib
▶ Regorafenib open since spring 2016
▶ Immunotherapy?
Clinicaltrials.gov, 2016; Clinicaltrials.gov, 2017a.

Anaplastic Thyroid Cancer
▶ Typically a tumor of older adults
▶ Presence of pre-existing or co-existing well-differentiated carcinoma in 23-78%
of cases, usually papillary thyroid cancer
▶ History of long-standing goiter is common
▶ Clinical presentation: Rapidly growing neck mass, hoarseness, vocal cord
paralysis, dysphagia
▶ Early hematogenous metastasis, cure rate 0-10%, median survival 4-6 mo
Images courtesy of Justine Barletta, MD & Cheryl Adackapara, MD.
NCCN, 2017; Haugen et al, 2016.
Spindle Cell Pattern Pleomorphic Giant Cell PatternSquamoid Pattern

Mutational Landscape in ATC
ATC = anaplastic thyroid cancer.
Kunstman et al, 2015.

ATC Therapy
▶ Thyroidectomy or debulking thyroid surgery
with neck dissection if possible
▶ Adjuvant radiotherapy or chemoradiotherapy
▶ Metastatic disease frequent, affecting
mediastinum, lung, bone, and liver
▶ Prognosis poor with 5-yr survival 0-14%
Kebebew et al, 2005; Edge et al, 2010.
All anaplastic carcinomas are considered stage IV:
T4a Intrathyroidal anaplastic carcinoma
T4bAnaplastic carcinoma with gross
extrathyroid extension
Anaplastic carcinoma (all anaplastic
carcinomas are considered stage IV):
Stage T N M
IVA T4a Any N M0
IVB T4b Any N M0
IVC Any T Any N M1

Metastatic ATC Therapy
▶ Doxorubicin + cisplatin:◼ 7/30 (23%) response rate
◼ PFS 10 months
▶ Sorafenib:◼ 2/15 (13%) PR
◼ 4/15 (27%) SD
▶ Axitinib:◼ 1/2 PR
No generally accepted standard for
treatment of metastatic ATC.
De Crevoisier et al, 2004; Nagaiah et al, 2009; Cohen et al, 2008.

FACT Phase II/III: Fosbretabulin in ATC
OS = overall survival.
Sosa et al, 2011; Sosa et al, 2014.
Design
◼ Multicenter, open-label, 2:1 randomized trial
◼ 80/180 planned patients randomly assigned. Trial stopped early
because of slow accrual
◼ Up to 6 cycles of carboplatin and paclitaxel ± CA4P
◼ Primary end point: OS
Results
◼ 75/80 randomly assigned patients received treatment
◼ Median follow up of 4.7 (0.1-32.6) mo
◼ Median survival time for the CA4P arm was 5.2 mo vs. 4.0 mo control
(HR=0.65; 95% CI: 0.38-1.10)
◼ 1-year survival was 27% on the CA4P arm vs 9% (P=0.065)
Adverse Events◼ Grade 1/2 hypertension and grade 3-4 neutropenia were more
common on the CA4P arm

ATC Trials
▶ Clinical Trials: MLN0128
▶ Everolimus: Among 7 patients, 1 had near
complete response, 1 case with PFS of 26 mo
▶ Lenvatinib: 3/9 responses
▶ Immunotherapy?
Clinicaltrials.gov, 2017b. Takahashi et al, 2014; Wagle et al, 2014.

Exceptional Response With Everolimus
H & E = hematoxylin and eosin.
Wagle et al, 2014.
H & E at Diagnosis
▶ 57-year-old patient with ATC
▶ Response to everolimus x 18 mo
Prior 6 months Progression

Response and Resistance
▶ Sequencing shows TSC2 mutation Q1178* in all samples
▶ Resistant sample with a new mutation in mTOR conveying
resistance
Wagle et al, 2014; Takei et al, 2014.

Case Study 1
A 35-year-old man presented with a right-sided neck mass to his primary care physician
and was administered an antibiotic. The neck mass persisted, however, and a thyroid
ultrasound showed a 3-cm nodule in the right lobe of the thyroid. FNA revealed malignant
cells consistent with PTC. A complete thyroidectomy with central neck dissection was
performed, which revealed a 3.3-cm well differentiated PTC with extracapsular extension
and lymphovascular invasion. Three out of 25 lymph nodes tested positive for metastatic
thyroid cancer. A chest x-ray was negative for metastatic disease.
Which of the following treatment options would you now recommend?
a. No further treatment
b. RAI to ablate thyroid remnants and eliminate possible micrometastatic disease
c. External beam radiotherapy
d. Start sorafenib 400 mg PO twice daily
e. Bilateral neck dissection levels II-IV followed by concurrent chemoradiotherapy

Case Study 1
A 35-year-old man presented with a right-sided neck mass to his primary care physician
and was administered an antibiotic. The neck mass persisted, however, and a thyroid
ultrasound showed a 3-cm nodule in the right lobe of the thyroid. FNA revealed malignant
cells consistent with PTC. A complete thyroidectomy with central neck dissection was
performed, which revealed a 3.3-cm well differentiated PTC with extracapsular extension
and lymphovascular invasion. Three out of 25 lymph nodes tested positive for metastatic
thyroid cancer. A chest x-ray was negative for metastatic disease.
Which of the following treatment options would you now recommend?
a. No further treatment
b. RAI to ablate thyroid remnants and eliminate possible micrometastatic
disease
c. External beam radiotherapy
d. Start sorafenib 400 mg PO twice daily
e. Bilateral neck dissection levels II-IV followed by concurrent chemoradiotherapy

Case Study 1:
Correct Answer Rationale
▶ Patient has locally advanced PTC. Because of the size of the
lesion and presence of involved lymph nodes, treatment with RAI is
indicated. Prognosis is excellent based on favorable histology and
young age (<45 years)
▶ External beam radiotherapy delivers less radiation to cancer cells
than RAI and carries more acute and chronic side effects.
Furthermore, it does not address potential micrometastatic distant
disease
▶ Sorafenib is an option in RAI-refractory disease, which is an
unlikely scenario in this case
▶ Further surgery is not indicated in the absence of clinically
suspicious areas of disease

Case Study 2
A 52-year-old woman noticed a lump on the left side of her thyroid area and presented to her primary
care physician. She was referred for a ultrasound and FNA, which revealed a 4.2-cm MTC in the left
lobe of the thyroid. Her calcitonin was 2,342 pg/mL. A CT scan showed 2 left level III enlarged lymph
nodes but no distant metastatic disease. She underwent a complete thyroidectomy, central neck
dissection, and left neck dissection. There was no extracapsular extension but 4/34 lymph nodes were
positive for metastatic carcinoma. Follow-up CT scans 6 months after surgery showed new lung
nodules bilaterally, up to 2.4 cm in diameter and several enlarged mediastinal lymph nodes.
Calcitonin, which dropped to 135 pg/L following surgery, rose to 547pg/L. She was asymptomatic.
Which of the following treatment options would you now recommend?
a. No further treatment
b. Radioactive iodine
c. Start vandetanib 300 mg daily
d. Start doxorubicin
e. Surgical removal of lung metastases

Case Study 2
A 52-year-old woman noticed a lump on the left side of her thyroid area and presented to her primary
care physician. She was referred for a ultrasound and FNA, which revealed a 4.2-cm MTC in the left
lobe of the thyroid. Her calcitonin was 2,342 pg/mL. A CT scan showed 2 left level III enlarged lymph
nodes but no distant metastatic disease. She underwent a complete thyroidectomy, central neck
dissection, and left neck dissection. There was no extracapsular extension but 4/34 lymph nodes were
positive for metastatic carcinoma. Follow-up CT scans 6 months after surgery showed new lung
nodules bilaterally, up to 2.4 cm in diameter and several enlarged mediastinal lymph nodes.
Calcitonin, which dropped to 135 pg/L following surgery, rose to 547pg/L. She was asymptomatic.
Which of the following treatment options would you now recommend?
a. No further treatment
b. Radioactive iodine
c. Start vandetanib 300 mg daily
d. Start doxorubicin
e. Surgical removal of lung metastases

Case Study 2:
Correct Answer Rationale
▶ Patient has widely metastatic MTC with evidence of rapid disease
progression
▶ While metastatic MTC can follow an indolent course and watchful
waiting is often appropriate, therapy should be initiated in this case
▶ Vandetanib is approved for MTC
▶ MTC is derived from parafollicular C-cells and is not RAI avid
▶ Doxorubicin has some activity and is no longer considered
appropriate first-line therapy
▶ Surgical removal of metastatic disease is a consideration for
symptom control or debulking of mass that is encroaching on vital
structures

Case Study 3
A 56-year-old woman noticed a rapidly enlarging lump at the base of her neck approximately 2 weeks
ago. She presented with hoarseness and 10-lb weight loss. Laryngoscopy revealed a paralyzed right
vocal cord. A CT scan of the neck showed a 7-cm neck mass originating from the thyroid causing
displacement and compression of the trachea. A CT scan of the chest revealed numerous pulmonary
nodules. Needle biopsy of the neck mass was consistent with anaplastic thyroid cancer.
Which of the following treatment options would you now recommend?
a. Surgical debulking followed by chemoradiotherapy
b. Radioactive iodine
c. Start sorafenib 400 mg twice daily
d. No therapy
e. Radiofrequency ablation of thyroid tumor and lung metastases

Case Study 3
A 56-year-old woman noticed a rapidly enlarging lump at the base of her neck approximately 2 weeks
ago. She presented with hoarseness and 10-lb weight loss. Laryngoscopy revealed a paralyzed right
vocal cord. A CT scan of the neck showed a 7-cm neck mass originating from the thyroid causing
displacement and compression of the trachea. A CT scan of the chest revealed numerous pulmonary
nodules. Needle biopsy of the neck mass was consistent with anaplastic thyroid cancer.
Which of the following treatment options would you now recommend?
a. Surgical debulking followed by chemoradiotherapy
b. Radioactive iodine
c. Start sorafenib 400 mg twice daily
d. No therapy
e. Radiofrequency ablation of thyroid tumor and lung metastases

Case Study 3:
Correct Answer Rationale
▶ ATC is very aggressive with early distant metastasis and poor
prognosis. Fortunately, it is also quite rare
▶ Surgical debulking to prevent airway compromise is standard of care,
irrespective of the presence of metastatic disease. To reduce or—if
possible—eradicate regional disease and prevent or delay recurrence,
radiotherapy or concurrent chemoradiotherapy is used
▶ Sorafenib appears to have minimal activity in this disease and may be
tried in an attempt to control systemic disease but should not be used
as initial treatment
▶ ATC is not RAI avid, thus patients are not candidates for RAI treatment
▶ Radiofrequency ablation of primary or metastatic lesions is considered
experimental and should not be used if more established frontline
therapy is possible

Key Takeaways
▶ Targeted therapy has transformed the treatment of metastatic
thyroid cancer
▶ Sorafenib and lenvatinib approved for
RAI-refractory DTC
▶ Vandetanib and cabozantinib approved for MTC
▶ Thyroid cancer is an active area of investigation and treatment
options should multiply in coming years

Audience Q&As

References
Agrawal N, Akbani R, Askoy BA, et al (2014). Integrated genomic characterization of papillary thyroid carcinoma. Cell, 159(3);676-690.
DOI:10.1016/j.cell.2015.09.050
Alexander EK, Kennedy GV, Baloch ZW, et al (2012). Preoperative diagnosis of benign thyroid nodules with indeterminate cytology. New Engl J
Med, 367:705-715. DOI:10.1056/NEJMoa1203208
Avram AM, Esfandiari NH & Wong KK (2015). Preablation 131-I scands with SPECT/CT contribute to thyroid cancer risk stratification and 131-I
therapy planning. J Clin Endocrinol Metab, 100(5):1895-1902. DOI:10.1210/jc.2014-4043
Brose MS, Cabanillas ME, Cohen EE, et al (2016). Vemurafenib in patients with BRAF(V600E)-positive metastatic or unresectable papillary
thyroid cancer refractory to radioactive iodine: a non-randomised, multicentre, open-label, phase 2 trial. Lancet Oncol, (9):1272-1282.
DOI:10.1016/S1470-2045(16)30166-8
Brose MS, Nutting CM, Jarzab B, et al (2014). Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid
cancer: a randomised, double-blind, phase 3 trial. Lancet, 384(9940):319-328. DOI:10.1016/S0140-6736(14)60421-9
Cantwell-Dorris ER, O’Leary JJ & Sheils OM (2011). BRAFV600E: implications for carcinogenesis and molecular therapy. Mol Cancer Ther,
10(3):385-394. DOI:10.1158/1535-7163.MCT-10-0799
Clinicaltrials.gov (2016). Ponatinib for medullary thyroid cancer. Available at: https://clinicaltrials.gov/ct2/show/NCT01838642. NLM Identifier:
NCT01838642.
Clinicaltrials.gov (2017a). A study using regorafenib as second or third line therapy in metastatic medullary thyroid cancer. Available at:
https://clinicaltrials.gov/ct2/show/NCT02657551. NLM Identifier: NCT02657551.
Clinicaltrials.gov (2017b). A phase II study of MLN0128 in metastatic anaplastic thyroid cancer. Available at:
https://clinicaltrials.gov/ct2/show/NCT02244463. NLM Identifier: NCT02244463.
Cohen SJ, Punt CJ, Iannotti N, et al (2008). Relationship of circulating tumor cells to tumor response, progression-free survival, and overall
survival in patients with metastatic colorectal cancer. J Clin Oncol, 26(19):3213-3221. DOI:10.1200/JCO.2007.15.8923
Cohen EE, Rosen LS, Vokes EE, et al (2008). Axitinib is an active treatment for all histologic subtypes of advanced thyroid cancer: results from
a phase II study. J Clin Oncol. 2008;26:4708-4713.
Cooper DS, Doherty GM, Haugen BR, et al (2006). Management guidelines for patients with thyroid nodules and differentiated thyroid cancer.
Thyroid, 16(2):109-142.
De Crevoisier R, Baudin E, Bachelot A, et al (2004). Combined treatment of anaplastic thyroid carcinoma with surgery, chemotherapy, and
hyperfractionated accelerated external radiotherapy. Int J Radiat Oncol Biol Phys, 60(4):1137-1143.
Edge S, Byrd DR, Compton CC, et al (2010). AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer.

References
Elisei R, Schlumberger MJ, Müller SP, et al (2013). Cabozantinib in progressive medullary thyroid cancer. J Clin Oncol, 31(29):3639-3646.
DOI:10.1200/JCO.2012.48.4659
Haugen BR, Alexander EK, Bible KC, et al (2016). 2015 American Thyroid Association management guidelines for adult patients with thyroid
nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated
thyroid cancer. Thyroid, 26(1):1-133. DOI:10.1089/thy.2015.0020
Ho AL, Grewal RK, Leboeuf R, et al (2013). Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer. N Engl J Med, 368(7):623-
632. DOI:10.1056/NEJMoa1209288
Hundahl SA, Fleming ID, Fremgen AM, et al (1998). A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the
U.S., 1985-1995. Cancer, 83(12):2638-48
Kebebew E, Greenspan FS, Clark OH, et al (2005). Anaplastic thyroid carcinoma. Treatment outcome and prognostic factors. Cancer,
103(7):1330-1335. DOI: 10.1002/cncr.20936
Kunstman JW, Juhlin CC, Goh G, et al (2015). Characterization of the mutational landscape of anaplastic thyroid cancer via whole-exome
sequencing. Hum Mol Genet, 24(8):2318-2329. DOI:10.1093/hmg/ddu749
Lim H, Devesa SS, Sosa JA, et al (2017). Trends in thyroid cancer incidence and mortality in the United States, 1974-2013. JAMA,
317(13):1338-1348. DOI:10.1001/jama.2017.2719
Lloyd RV, Beuhler D & Khanafshar E (2011). Papillary thyroid carcinoma variants. Head Neck Pathol, 5(1):51-56. DOI:10.1007/s12105-010-
0236-9
Lorch JN, Busaidy N, Ruan DT, et al (2013). A phase II study of everolimus in patients with aggressive RAI refractory (RAIR) thyroid cancer
(TC). J Clin Oncol, 31(15_suppl):6023. DOI:10.1200/jco.2013.31.15_suppl.6023
Lorch JH, Chau N, Hanna G, et al (2016). A multi-center phase II study of everolimus in patients with aggressive thyroid cancer and genetic
analysis. 86th Annual Meeting of the American Thyroid Association. Poster 33.
Mehnert JM, Varga A. Brose M, et al (2016). Pembrolizumab for advanced papillary or follicular thyroid cancer: preliminary results from the
phase 1b KEYNOTE-028 study. J Clin Oncol, 34(15_suppl):6091. DOI:10.1200/JCO.2016.34.15_suppl.6091
Nagaiah G, Fu P, Wasman JK, et al (2009). Phase II trial of sorafenib (bay 43-9006) in patients with advanced anaplastic carcinoma of the
thyroid (ATC). J Clin Oncol, 27(suppl_15):A6058. DOI:10.1200/jco.2009.27.15s.6058
Nascimento C, Borget I, Al Ghuzian A, et al (2015). Postoperative fluourine-18-fluorodeoxyglucose positron emission tomography/computed
tomography: an important imaging modality in patients with aggressive histology of differentiated thyroid cancer. Thyroid, 25(4):437-
444. DOI:10.1089/thy.2014.0320

References
Omry-Orbach G (2016). Risk stratification in differentiated thyroid cancer: an ongoing process. Rambam Maimonides Med, 7(1):e0003.
DOI:10.5041/RMMJ.10230
Ricarte-Filho JC, Ryder M, Chitale DA, et al (2009). Mutational profile of advanced primary and metastatic radioactive iodine-refractory thyroid
cancers reveals distinct pathogenetic roles for BRAF, PIK3CA, and AKT1. Cancer Res, 69(11):4885-4893. DOI:10.1158/0008-
5472.CAN-09-0727
Schlumberger M, Tahara M, Wirth LJ, et al (2015). Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med,
372(7):621-630. DOI:10.1056/NEJMoa1406470
Schöffski P, Elisei R, Müller S, et al (2012). An international, double-blind, randomized, placebo-controlled phase III trial (EXAM) of cabozantinib
(XL184) in medullary thyroid carcinoma (MTC) patients (pts) with documented RECIST progression at baseline. J Clin Oncol,
30(15_suppl):5508. DOI:10.1200/jco.2012.30.15_suppl.5508
Sherman SI, Clary DO, Elisei R, et al (2016). Correlative analyses of RET and RAS mutations in a phase 3 trial of cabozantinib in patients with
progressive, metastatic medullary thyroid cancer. Cancer, 122(24):3856-3864. DOI:10.1002/cncr.30252
Sosa JA, Elisei R, Jarzab B, et al (2011). A randomized phase II/III trial of a tumor vascular disrupting agent fosbretabulin tromethamine (CA4P)
with carboplatin (C) and paclitaxel (P) in anaplastic thyroid cancer (ATC): final survival analysis for the FACT trial. J Clin Oncol,
29(suppl). Abstract 5502.
Sosa JA, Elisei R, Jarzab B, et al (2014). Randomized safety and efficacy study of fosbretabulin with paclitaxel/carboplatin against anaplastic
thyroid carcinoma. Thyroid, 24(2):232-240. DOI:10.1089/thy.2013.0078.
Stjlepovic N & Capdevila J (2014). Multikinase inhibitors in the treatment of thyroid cancer: specific role of lenvatinib. Biologics, 8:129-139.
DOI:10.2147/BBT.S39381
Takahashi S, Tahara M, Kiyota N, et al (2014). Phase II study of lenvatinib (len), a multi-targeted tyrosine kinase inhibitor, in patients (pts) with
all histologic subtypes of advanced thyroid cancer (differentiated, medullary and anaplastic). Ann Oncol, 25(suppl 4):iv340-iv356.
DOI:10.1093/annonc.mdu240.10
Takei N, Furukawa K, Hanyu O, et al (2014). A possible link between BDNF and mTOR in control of food intake. Front Psychol, 5:1093.
DOI:10.3389/fpsyg.2014.01093
Wagle N, Grabiner BC, Van Allen EM, et al (2014). Response and acquired resistance to everolimus in anaplastic thyroid cancer. N Engl J Med,
371(15):1426-1433. DOI:10.1056/NEJMoa1403352
Wells SA Jr, Robinson BG, Gagel RF, et al (2012). Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: a
randomized, double-blind phase III trial. J Clin Oncol, 30(2):134-141. DOI:10.1200/JCO.2011.35.5040

References
Xing M, Alzahrani AS, Carson KA, et al (2013). Association between BRAF V600E mutation and mortality in patients with papillary thyroid
cancer. JAMA, 309(14):1493-1501. DOI:10.1001/jama.2013.3190
Yassa L, Cibas ES, Benson CB, et al (2007). Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation.
Cancer, 111(6):508-516. DOI: 10.1002/cnr.23116
Yeh MW, Bauer AJ, Bernet VA, et al (2015). American Thyroid Association statement on preoperative imaging for thyroid cancer surgery.
Thyroid, 25(1):3-14. DOI:10.1089/thy.2014.0096
Zbuk KM & Eng C (2007). Cancer phenomics: RET and PTEN as illustrative models. Nat Rev Cancer, 7(1):35-45. DOI: 10.1038/nrc2037