Embed Size (px)
Citation preview

University of Groningen
Medullary Thyroid CarcinomaVerbeek, Hans
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2015
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Verbeek, H. (2015). Medullary Thyroid Carcinoma: from diagnosis to treatment. [S.l.]: [S.n.].
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 17-07-2020

Medullary Thyroid Carcinoma
From diagnosis to treatment
Hans Verbeek

Medullary Thyroid Carcinoma
From diagnosis to treatment
Verbeek, H.H.G.
Cover: Wouter van de Gronde, www.woutr.nl
Printed by: Ipskamp Drukkers
ISBN: 978-90-367-7392-8 (print)
978-90-367-7391-1 (eBook)
Copyright © 2014 H.H.G. Verbeek, The Netherlands
All rights reserved. No part of this thesis may be reproduced, stored in a retrieval
system, or transmitted in any form or by any means, without prior written
permission of the author.
Financial support for printing of this thesis was kindly provided by: The Endocrinology Fund, as part
of the Ubbo Emmius Fund, University Medical Center Groningen and University of Groningen.

Medullary Thyroid Carcinoma
From diagnosis to treatment
Proefschrift
ter verkrijging van de graad van doctor aan de
Rijksuniversiteit Groningen
op gezag van de
rector magnificus prof. dr. E. Sterken
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
woensdag 7 januari 2015 om 16.15 uur
door
Hans Hendrik Gijsbert Verbeek
geboren op 1 september 1985
te Emmen

Promotores
Prof. dr. T.P. Links
Prof. dr. J.T.M. Plukker
Prof. dr. R.M.W. Hofstra
Beoordelingscommissie
Prof. dr. W.J.G. Oyen
Prof. dr. I.H.M. Borel Rinkes
Prof. dr. E.G.E. de Vries

Contents
Chapter 1 General introduction and aims of the thesis 7
Chapter 2 Medullary thyroid cancer, a tumour with many appearances 17
Chapter 3 Calcitonin testing for detection of medullary thyroid cancer 27
in patients with thyroid nodules
Chapter 4 Fewer cancer reoperations for medullary thyroid cancer 57
after initial surgery according to ATA guidelines
Chapter 5 PET imaging in thyroid carcinoma 73
Chapter 6 Clinical relevance of 18F-FDG PET and 18F-DOPA PET in 91
recurrent medullary thyroid carcinoma
Chapter 7 The effects of four different tyrosine kinase inhibitors on 109
medullary and papillary thyroid cancer cells
Chapter 8 Summary, discussion and future perspectives 125
Nederlandse samenvatting 139
Dankwoord 147
Curriculum vitae 151
Appendices 153

Paranimfen:
B. Kok
C.H. Verbeek

Chapter 1
General introduction and aims of the thesis

Chapter 1
8
General introduction
The thyroid
One of the largest endocrine organs of the human body is the thyroid. This butterfly-shaped
organ is located in the neck, in front of the trachea, directly below the larynx (Figure 1A). The
thyroid is composed of follicles, surrounded by follicular and parafollicular cells (C-cells)
(Figure 1B). Endocrine organs, such as the thyroid, produce hormones; biochemical active
messengers which are released in the blood and regulate body functions. The thyroid produces
thyroxine (T4), tri-iodotyronine (T3) (thyroid hormones) and calcitonin. The thyroid
hormones are involved in the metabolic rate throughout the body, while calcitonin exerts an
effect on calcium levels.
A. B.
Figure 1 Schematic representation of the thyroid gland (A) and (B) a histological section of thyroid tissue
showing the different thyroid cells.
Thyroid hormone production is a complex process and involves selective uptake of iodine
which is bound to thyroglobulin, a large protein synthesized in the follicular thyroid cells to
form eventually thyroxine and tri-iodotyronine. To release these hormones in the
bloodstream, they are cleaved from the thyroglobulin which takes place intracellular. In the
circulation, thyroid hormones are bound for 99% to the thyroxine binding globulin, and only
1% is free available for uptake by tissue cells.
C- cells
Follicular cells
Follicle

General introduction and aims of the thesis
9
Thyroid hormones act throughout the whole body and increase metabolism by activating
transcription of many genes. Although thyroxine is much more present in the circulation, tri-
iodotyronine is the active form of thyroid hormone and therefore almost all thyroxine is
diodinated in order to have an effect on gene transcription.
Calcitonin is the other hormone of the thyroid produced in the parafollicular C-cells, which
account for about 0.1% of all thyroid cells. These cells have another embryological origin
than the follicular thyroid cells. Calcitonin is a 32-amino acid peptide. The main effect of
calcitonin is decreasing serum calcium levels, mainly by inhibiting bone resorption.1,2
However, in comparison to the parathyroid hormone (PTH) secreted by the parathyroids, the
effect of calcitonin on calcium metabolism is limited.
Thyroid nodules
Thyroid nodules are common in the general population; they are detected in up to 7% of
patients with neck palpation and on ultrasound even up to 70%.3-6 Functional imaging
methods such as PET imaging also frequently reveal thyroid nodules.7 Thyroid nodules are
more present in women than in men and the incidence of thyroid nodules also increases with
age.3,8,9 Benign nodules can be caused by clonal expansion of follicular cells (hyperplasia),
increase of the colloid follicles (colloid nodules), formation of cysts (cystic nodules) or
inflammation (thyroiditis).10,11 Most nodules are benign; only 5% to 10% of patients with
palpable thyroid nodules have thyroid cancer.
Thyroid cancer
Five major histological types of thyroid cancer are recognized; papillary, follicular,
medullary, poorly differentiated and undifferentiated (anaplastic) cancer. Papillary and
follicular cancer (also known as differentiated thyroid cancer) arise from the follicular
epithelium and account for 80-90% of all thyroid cancers. Medullary thyroid cancer arises
from the parafollicular C-cells and accounts for approximately 5%-10% (Figure 2). Poorly
differentiated thyroid carcinoma also arises from the follicular epithelium but exhibits a more
aggressive growth pattern compared to differentiated thyroid carcinoma, although less
aggressive than undifferentiated thyroid carcinoma. In undifferentiated thyroid carcinoma
undifferentiated cells exhibit features indicative of epithelial differentiation and
immunohistochemical staining is generally negative for thyroglobulin and calcitonin.
Undifferentiated thyroid carcinoma covers the last 5%-10% of the cases.11

Chapter 1
10
Medullary thyroid cancer
MTC was first described in a patient 1906 as a “malignant goiter with amyloid” by Jaquet.12
In 1959, Hazard defined a case of thyroid carcinoma with a solid non follicular structure with
amyloid in the stroma as a MTC.13 MTC can occur sporadically (75%) or as part of a familial
syndrome called Multiple Endocrine Neoplasia type 2 (MEN 2). This syndrome is caused by
a mutation in the ‘REarranged during Transfection’ (RET) gene and a MEN2A and MEN2B
variant are discerned. Other manifestations of the MEN2 syndromes are a pheochromocytoma
and hyperparathyroidism (MEN2A) or neurofibromatosis (MEN2B) (Table 1).
Figure 2 Histological section of medullary thyroid carcinoma
Table 1 Clinical expression of familial MTC-associated syndromes14
FMTC MEN 2A MEN2B
MTC 100% 100% 100%
Pheochromocytoma 0% 10-60% 50%
Hyperparathyroidism 0% 10-25% 0%
Marfanoid habitus 0% 0% 100%
Intestinal ganlioneuromatosis 0% 0% 60-90%
Mucosal neuromas 0% 0% 70-100%
Clinical presentation and diagnosis
Most MTC patients present with an asymptomatic palpable solitary thyroid nodule or lymph
node. Some patients have symptoms such as dyspnea, dysphagia, coughing or hoarseness.
Due to excessive calcitonin production diarrhea or flushing may occur.15,16 In very rare cases
ectopic ACTH production of the neuroendocrine cells can cause Cushing syndrome.17 At

General introduction and aims of the thesis
11
presentation, about 50% of the MTC patients have lymph node metastases and distant
metastasis are diagnosed in around 15% of patients.18,19 Fine needle aspiration cytology is
generally the first diagnostic procedure for thyroid nodules. However, the sensitivity of this
procedure, without the use of additional immunohistochemical analysis, for detecting MTC is
limited.20 Since MTC originates from the calcitonin producing C-cells, this hormone can be
used as a sensitive tumour marker. Another tumour marker used in MTC is carcinoembryonic
antigen (CEA), however this marker is less sensitive. Serum calcitonin levels are not only
determined in patients suspected of MTC, but are also used as screening tool for detection of
MTC in patients with thyroid nodules. Although calcitonin testing in patients with thyroid
nodules can detect MTC in an early stage, it also increases the risk of unnecessary surgery as
a proportionate number of patients with thyroid nodules have an elevated basal calcitonin
based on other causes than MTC (e.g. thyroiditis, idiopathic, sepsis and chronic renal
failure).21-24
Treatment
According to the current American Thyroid Association (ATA) guidelines, treatment for
sporadic MTC consists of complete surgical removal of the thyroid (total thyroidectomy) and
the adjacent lymph nodes in the central compartment (central compartment dissection). If the
disease has spread to lateral lymph nodes of the neck, a lateral lymph node dissection is also
indicated.25 However a proportionate number of MTC patients cannot be cured due to the
extensiveness of the disease at presentation.26,27 In contrast to papillary and follicular thyroid
cancer, MTC patients do not benefit from adjuvant radioactive iodine treatment as the C-cells
do not have uptake of iodine.28 Therefore adequate surgery is of crucial importance in MTC,
including meticulous nodal dissection in the central and/or lateral neck. Although current
ATA guidelines provide clear recommendations for the surgical approach, the effect of
adherence to these recommendations on the outcome of MTC patients remains unclear.
Follow-up
Despite extensive surgery, a large proportion of MTC patients cannot be cured.29 Although
many patients with residual disease have a good life expectancy, some will develop
progressive disease.30 Therefore follow-up is important including regular determinations of
calcitonin and CEA. If these tumour markers are elevated or increasing, further diagnostic
work-up is needed using morphological (US/MRI/CT) and functional imaging (positron

Chapter 1
12
emission tomography (PET)). Although calcitonin and CEA doubling times are currently the
most reliable markers for progression, time consuming serial measurements are required for
accurate determination. Early detection of progressive disease is important because
appropriate therapeutic interventions, such as local surgical treatment, may delay
symptomatic deterioration. Therapeutic strategies are based on the outcome of the imaging
procedure and the doubling time of the tumour markers, and covers a wait and see policy with
close monitoring, a surgical intervention or systemic (targeted) therapy, if possible in a
clinical trial.
Systemic treatment
Traditional chemotherapeutic regimens have not been proven to be effective in the palliative
treatment of MTC. Recently developed tyrosine kinase inhibitors have shown improvement of
progression free survival in MTC patients.31,32 However, most studies have used one
particular TK inhibitor without analysis of the mutations present in the tumour. This makes it
difficult to compare these compounds for different patient groups. Most tyrosine kinase
inhibitors target multiple intracellular pathways, which can cause next to the intended effect
also side-effects, including cardiac toxicity and hand-foot syndrome.33,34 Therefore careful
consideration must be given when applying these new therapies.
Aims and outlines of the thesis
This thesis covers problems encountered in the diagnosis and treatment of primary and
recurrent MTC. The aims of the studies in this thesis were to:
1. Address the value of calcitonin testing for detection of MTC in patients with thyroid
nodules.
2. Evaluate the recommendations regarding surgical treatment by the current ATA
guidelines for MTC patients.
3. Detect MTC patients with progressive recurrent disease in an early stage.
4. Optimize treatment with targeted therapy (tyrosine kinase inhibitors) for MTC patients
with RET mutations/translocations with recurrent disease.
Chapter 2 encompasses an introduction to MTC and the difficulties in diagnosis. To illustrate
the different clinical presentation and behaviour of MTC, three patients with different stages

General introduction and aims of the thesis
13
of disease are presented. A brief overview of currently used methods for diagnosis, treatment
options and follow-up is provided.
MTC patients detected in an early stage of the disease have a better prognosis. As almost all
MTCs secrete calcitonin, systematic determination of calcitonin might detect these tumours in
patients presenting with a thyroid nodule. However, the role of routine calcitonin testing
remains unclear, and no consensus exists between different guidelines. Chapter 3 focuses on
the value of routine calcitonin testing for detection of MTC in patients with thyroid nodules.
A formal systematic meta-analysis was performed to determine the diagnostic accuracy of the
calcitonin test. Sixteen studies were eventually included in which 72368 patients with nodular
thyroid disease underwent basal calcitonin testing and 187 MTC patients were identified.
Summary estimates of sensitivity and specificity for different cut-off values and subgroups
were determined.
Surgery is the most important therapeutic option for curative treatment of MTC. For MTC
patients presenting with a palpable thyroid nodule without suspected lymph node
involvement, treatment consists of a total thyroidectomy and central compartment dissection.
In many institutes this approach is followed by an unilateral elective nodal dissection of the
lateral neck. When suspected nodal involvement is present, a therapeutic lateral lymph node
dissection, according to the American Thyroid Association (ATA) 2009 guidelines is
performed. As the effect of adherence to these recommendations on the outcome of MTC
patients is unclear, we retrospectively evaluated these guidelines with respect to locoregional
control and clinical outcome. In Chapter 4 we reviewed the surgical and pathology reports of
86 patients treated between 1980 and 2010 in two major tertiary referral centres. We
compared the clinical outcome (reoperations, biochemical cure, survival and complications)
of the patients treated adequately according to ATA guidelines versus patients treated
inadequately. Furthermore, we examined to which extent clinical outcome of patients was
influenced by one-step versus a two-step intended curative surgical procedure, institute of
initial curative surgery (experienced centre versus non-centre hospital). Finally, influence of
patient and tumour characteristics on clinical outcome were evaluated.
After surgery, follow-up is important in patients with MTC, as a large proportion of patients
with biochemical residual disease will develop clinical recurrent disease. Although prognosis
is good in most patients with recurrent disease, some patients develop progressive disease.

Chapter 1
14
Regular determinations of calcitonin and CEA are useful in the early identification of these
patients, because therapeutic interventions, such as surgery for local tumour control, can be of
value in these patients. If tumour markers increase, further diagnostic work-up with
anatomical and/or functional imaging is required. In Chapter 5 we aimed to provide an
overview of the available PET imaging methods used for MTC and other types of thyroid
cancer. In Chapter 6 we investigated the potential of 18F-deoxyglucose (FDG-PET) and 18F-
diphenylalanine (DOPA-PET) to identify progression in MTC patients. PET positivity was
compared with biochemical parameters (calcitonin and CEA serum levels and doubling times)
in 47 patients. In a subgroup of 21 patients whole body metabolic burden (WBMTB) was
assessed with standardized uptake value and the number of lesions, and compared with
biochemical parameters. Furthermore, survival was compared with 18F-DOPA PET or 18F-
FDG PET positivity.
In MTC, but also PTC patients with progressive disease, systemic targeted therapy with
tyrosine kinase inhibitors is currently considered. As activating mutations or rearrangements
in the RET gene can cause MTC and PTC, tyrosine kinase inhibitors that target the RET
receptor might be promising. In Chapter 7 we aimed to determine which inhibitor is the most
effective and if there is rationale for mutation based therapy. We cultured and treated three
cell lines expressing a MEN2A (MTC-TT), a MEN2B (MZ-CRC-1) mutation, and a
RET/PTC (TPC-1) rearrangement. We compared four tyrosine kinase inhibitors (axitinib,
sunitinib, vandetanib and cabozantinib) in vitro. We evaluated the effects on cell proliferation,
RET expression, RET autophosphorylation and on RET downstream pathways (Extracellular
Signal-regulated Kinase (ERK)).
In Chapter 8 a general discussion is provided and future perspectives are addressed. In
Chapter 9 a summary of this thesis in Dutch is given.

General introduction and aims of the thesis
15
References
1. Chambers TJ, Moore A. The sensitivity of isolated osteoclasts to morphological transformation by
calcitonin. J Clin Endocrinol Metab 1983;57:819-824.
2. Karsdal MA, Henriksen K, Arnold M, Christiansen C. Calcitonin: a drug of the past or for the future?
Physiologic inhibition of bone resorption while sustaining osteoclast numbers improves bone quality.
BioDrugs 2008;22:137-144.
3. Vander JB, Gaston EA, Dawber TR. The significance of nontoxic thyroid nodules. Final report of a 15-
year study of the incidence of thyroid malignancy. Ann Intern Med 1968;69:537-540.
4. Rallison ML, Dobyns BM, Meikle AW, Bishop M, Lyon JL, Stevens W. Natural history of thyroid
abnormalities: prevalence, incidence, and regression of thyroid diseases in adolescents and young
adults. Am J Med 1991;91:363-370.
5. Wiest PW, Hartshorne MF, Inskip PD, et al. Thyroid palpation versus high-resolution thyroid
ultrasonography in the detection of nodules. J Ultrasound Med 1998;17:487-496.
6. Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules
discovered incidentally on thyroid imaging. Ann Intern Med 1997;126:226-231.
7. Soelberg KK, Bonnema SJ, Brix TH, Hegedus L. Risk of malignancy in thyroid incidentalomas detected
by 18F-fluorodeoxyglucose positron emission tomography: a systematic review. Thyroid 2012;22:918-
925.
8. Vanderpump MP, Tunbridge WM, French JM, et al. The incidence of thyroid disorders in the
community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol (Oxf) 1995;43:55-68.
9. Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med 1993;328:553-559.
10. Salabe GB. Pathogenesis of thyroid nodules: histological classification? Biomed Pharmacother
2001;55:39-53.
11. Schmid KW. Molecular pathology of thyroid tumors. Pathologe 2010;31 Suppl 2:229-233.
12. Jaquet AJ. Ein fall von metastasierenden amyloidtumoren (lymphosarcoma). Virchows Archiv
1906:251-267.
13. HAZARD JB, HAWK WA, CRILE G,Jr. Medullary (solid) carcinoma of the thyroid; a clinicopathologic
entity. J Clin Endocrinol Metab 1959;19:152-161.
14. de Groot JW, Links TP, Plukker JT, Lips CJ, Hofstra RM. RET as a diagnostic and therapeutic target in
sporadic and hereditary endocrine tumors. Endocr Rev 2006;27:535-560.
15. Beressi N, Campos JM, Beressi JP, et al. Sporadic medullary microcarcinoma of the thyroid: a
retrospective analysis of eighty cases. Thyroid 1998;8:1039-1044.
16. Mure A, Gicquel C, Abdelmoumene N, et al. Cushing's syndrome in medullary thyroid carcinoma. J
Endocrinol Invest 1995;18:180-185.
17. Hijazi YM, Nieman LK, Medeiros LJ. Medullary carcinoma of the thyroid as a cause of Cushing's
syndrome: a case with ectopic adrenocorticotropin secretion characterized by double enzyme
immunostaining. Hum Pathol 1992;23:592-596.
18. Kebebew E, Ituarte PH, Siperstein AE, Duh QY, Clark OH. Medullary thyroid carcinoma: clinical
characteristics, treatment, prognostic factors, and a comparison of staging systems. Cancer
2000;88:1139-1148.
19. Modigliani E, Cohen R, Campos JM, et al. Prognostic factors for survival and for biochemical cure in
medullary thyroid carcinoma: results in 899 patients. The GETC Study Group. Groupe d'etude des
tumeurs a calcitonine. Clin Endocrinol (Oxf) 1998;48:265-273.
20. Bugalho MJ, Santos JR, Sobrinho L. Preoperative diagnosis of medullary thyroid carcinoma: fine needle
aspiration cytology as compared with serum calcitonin measurement. J Surg Oncol 2005;91:56-60.
21. Lips CJ, Landsvater RM, Hoppener JW, et al. Clinical screening as compared with DNA analysis in
families with multiple endocrine neoplasia type 2A. N Engl J Med 1994;331:828-835.
22. Landsvater RM, Rombouts AG, te Meerman GJ, et al. The clinical implications of a positive calcitonin
test for C-cell hyperplasia in genetically unaffected members of an MEN2A kindred. Am J Hum Genet
1993;52:335-342.
23. Machens A, Haedecke J, Holzhausen HJ, Thomusch O, Schneyer U, Dralle H. Differential diagnosis of
calcitonin-secreting neuroendocrine carcinoma of the foregut by pentagastrin stimulation.
Langenbecks Arch Surg 2000;385:398-401.

Chapter 1
16
24. Niccoli P, Brunet P, Roubicek C, et al. Abnormal calcitonin basal levels and pentagastrin response in
patients with chronic renal failure on maintenance hemodialysis. Eur J Endocrinol 1995;132:75-81.
25. Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer: management guidelines of the American
Thyroid Association. Thyroid 2009;19:565-612.
26. Machens A, Gimm O, Ukkat J, Hinze R, Schneyer U, Dralle H. Improved prediction of calcitonin
normalization in medullary thyroid carcinoma patients by quantitative lymph node analysis. Cancer
2000;88:1909-1915.
27. Scollo C, Baudin E, Travagli JP, et al. Rationale for central and bilateral lymph node dissection in
sporadic and hereditary medullary thyroid cancer. J Clin Endocrinol Metab 2003;88:2070-2075.
28. Meijer JA, Bakker L, Valk GD, et al. Radioactive Iodine in the treatment of Medullary Thyroid
Carcinoma: a controlled multicenter study. Eur J Endocrinol 2013.
29. Machens A, Schneyer U, Holzhausen HJ, Dralle H. Prospects of remission in medullary thyroid
carcinoma according to basal calcitonin level. J Clin Endocrinol Metab 2005;90:2029-2034.
30. Rendl G, Manzl M, Hitzl W, Sungler P, Pirich C. Long-term prognosis of medullary thyroid carcinoma.
Clin Endocrinol (Oxf) 2008;69:497-505.
31. Wells SA,Jr, Robinson BG, Gagel RF, et al. Vandetanib in patients with locally advanced or metastatic
medullary thyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol 2012;30:134-141.
32. Elisei R, Schlumberger MJ, Muller SP, et al. Cabozantinib in progressive medullary thyroid cancer. J Clin
Oncol 2013;31:3639-3646.
33. Ye L, Santarpia L, Gagel RF. The evolving field of tyrosine kinase inhibitors in the treatment of
endocrine tumors. Endocr Rev 2010;31:578-599.
34. Kapiteijn E, Schneider TC, Morreau H, Gelderblom H, Nortier JW, Smit JW. New treatment modalities
in advanced thyroid cancer. Ann Oncol 2012;23:10-18.

Chapter 2
Medullary thyroid cancer, a tumour
with many appearances
Hans H.G. Verbeek, Jan Willem B. de Groot, John T.M. Plukker, Robert M.W. Hofstra
Adrienne H. Brouwers, Michiel N. Kerstens, Thera P. Links
Ned Tijdschr Geneesk 2010; 154: A1818 (translated from Dutch)

Chapter 2
18
Abstract
Medullary thyroid cancer (MTC) has a variable clinical presentation. We present 3 patients
with this endocrine tumour. The first patient, a 41-year-old woman complaining of diarrhoea,
a painful abdomen, weight loss and sensibility disorders in both legs, had metastases of MTC
in the spine, with little progression during 2 years of follow-up. The second patient, a 64-year-
old woman suffering from a painful nodule in the neck and a painful shoulder, was diagnosed
with MTC and liver, lung and bone metastases. She died after 14 months due to progressive
disease. The third patient, an 81-year-old woman with hyperparathyroidism, was
coincidentally diagnosed with MTC after goitre surgery at the age of 67. When she was
evaluated for rising calcitonin levels, a pheochromocytoma was found. RET mutation analysis
confirmed a MEN2A syndrome. Current diagnostic procedures of MTC may include positron
emission tomography with 18F-deoxyglucose (18F-FDG PET) and 18F-diphenylalanine (18F-
DOPA PET). MTC is usually treated surgically. Tyrosine kinase inhibitors also appear to
offer potential new therapeutic possibilities.

MTC, a tumour with many appearances
19
Introduction
Medullary thyroid carcinoma (MTC) is a rare endocrine tumour which originates from the
calcitonin producing C-cells in the thyroid. The serum level of calcitonin has therefore a great
diagnostic value as tumour marker. Also the serum level of carcinoembryonic antigen (CEA)
is often elevated, but is less specific for MTC. In the Netherlands, 20-30 MTC patients are
diagnosed yearly. MTC can occur sporadically (75% of cases) or familiarly as part of the
multiple endocrine neoplasia type 2 syndrome (MEN2). Of this syndrome, caused by a
mutation in the ‘REarranged during Transfection (RET)’ gene, a MEN2A and MEN2B variant
are known (Table 1).1 Here we illustrate the broad spectrum of presentation and the clinical
course of MTC with 3 patients. Furthermore the current diagnostic modalities and treatment
options are discussed.
Patient A, a 41 year old woman, presented with a multinodular goitre. Repeated fine needle
aspiration cytology (FNAC) of the thyroid did not reveal malignancy. Four years later she
presented with diarrhoea, a painful lower abdomen and a weight loss of 13 kg. Additional
investigation, which included gastroduodenoscopy, colonoscopy, abdominal and transvaginal
ultrasound (US), did not lead to a diagnosis. She then developed an abnormal walking pattern
with sensibility dysfunction of both legs. Magnetic resonance imaging (MRI) showed a
tumour in the sixth thoracic vertebrae with compression of the myelum. Surgical debulking
took place and the pathologist diagnosed a metastasis of a MTC. The calcitonin and CEA
were highly elevated (respectively 143,150 ng/l (ref 0.3-12 ng/l) and 1400 ug/l (ref 0.5-5
ug/l)). The serum calcium was normal and there were no hints of pheochromocytoma.
Additional RET-mutation analysis did not show a mutation. Further investigations for staging
with fluor-18-deoxyglucose (18F-FDG) positron emission tomography (PET) and fluor 18-
dihydroxyphenylalanine (18F-DOPA) PET showed the primary process in the thyroid with
extensive bone metastasis (Figure 1). A total thyreoidectomy with lymph node dissection of
the central compartment was performed. In this procedure all lymph nodes and fat tissue
between both carotids was removed, from the os hyoideum cranially to the v. brachiocheplica
caudally. After surgery a single dose with 150 mCurie I131 MIBG was given for persisting
diarrhoea, with a subjectively good response. At this moment four years after MIBG therapy
there is slowly progressive disease, which is too slow for inclusion in a clinical trial with a
tyrosine kinase inhibitor.

Chapter 2
20
Table 1 Clinical characteristics of patients with familial medullary thyroid carcinoma,
multiple endocrine neoplasia (MEN) 2A and MEN2B.
Clinical characteristic Prevalence (%)
Familial MTC* MEN2A MEN2B
Medullary thyroid carcinoma 100 100 100
C-cell hyperplasia 100 100 100
Pheochromocytoma 0 10-60 50
Hyperparathyroidism 0 10-25 0
Neurofibromatosis 0 0 60-90
Marfanoid habitus 0 0 100
* Families are described in which only MTC occurs without other endocrine neoplasia’s.
Patient B, a 64–year old female presented with a painful nodule in the neck and a painful
right shoulder in another hospital. FNAC of the nodule showed a MTC. Ultrasound of the
liver, CT-imaging of the abdomen and bone scintigraphy showed metastasis in the liver and
skeleton, upon which referral to our centre was made. Additional imaging with 18F-FDG PET
showed besides liver metastasis also neck and lung metastasis. Calcitonin serum levels were
strongly elevated (650 ng/l); CEA was not determined and no biochemical clues existed for a
pheochromocytoma or hyperparathyroidism. RET-mutation analysis was not performed
because the patient was above 50 years and there was no clinical suspicion of a MEN2
syndrome. For local control of the primary tumour, a total thyroidectomy with a central and
lateral lymph node dissection was performed. External radiotherapy was given
postoperatively in the neck and mediastinum (70 Gy in 35 fractions). There was, however,
biochemical progression and progression on 18F-FDG and 18F-DOPA PET, especially of the
bone metastasis, for which palliative radiotherapy was given. Because of her poor clinical
condition, no systemic therapy was started. The patient deceased fourteen months after initial
presentation.
Patient C, an 81 year old woman, had at the age of 67 undergone in another hospital a
subtotal thyroidectomy and parathyroidectomy for a primary hyperparathyroidism and goitre.
Histopathological investigation revealed a hyperplasia of the parathyroids and a coincidental
MTC; no information on tumour size was available. An additional total thyroidectomy
without lymph node dissection was performed.

MTC, a tumour with many appearances
21
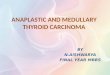
Figure 1 Positron emission tomography with 18
F-DOPA PET (left) and 18
F-FDG PET (right) of patient A. The 18
F-
DOPA PET shows clear uptake in the primary tumour in the neck. Extensive bone metastasis in the skull, spine,
skull and both femora is present. There is physiological uptake of 18
F-DOPA in the putamen, the caudate
nucleus, kidneys and bladder. The 18
F-FDG PET shows also clear uptake in the primary tumour and focal uptake
in the pelvis and right femur. There is faint uptake in the area of the 6th
thoracic vertebra, because of surgical
debulking 6 weeks before the scan. There is physiological uptake in the brain, kidneys, bladder and colon.
The patient was referred to our centre for further analysis of rising serum calcitonin levels; the
CEA concentration was not elevated. For a period of four years she had paroxysmal occurring
heat sensations without other symptoms. Blood pressure was 170/74 mm Hg, and further
physical examinations revealed no abnormalities. Biochemical investigation showed, besides
a raised serum calcitonin concentration, also increased metanephrines in plasma and urine,
suggestive of a pheochromocytoma. Imaging revealed enlarged lymph nodes in the neck and
an adrenal tumour on the left.
A laparoscopic adrenalectomy was performed with removal of a pheochromocytoma. DNA
analysis was performed because of the clinical presentation, despite the high age. The patient
was carrier of a Cys618Phe mutation of the RET-gene, a single base substitution in codon
618, in exon 10, resulting in the amino acid substitution of cysteine by phenylalanine. This

Chapter 2
22
confirmed the clinical diagnosis MEN2A. Because of the high age of the patient and the lack
of clinical symptoms a ‘wait and see’ policy for the MTC was adopted. In the family of the
patient genetic analysis was performed over four generations. Of the 40 family members
investigated, 19 carried the Cys618Phe mutation.
These patients show the varied clinical course of MTC. The presentation of patients A and B
is characteristic for a sporadic MTC, in which at the time of diagnosis extensive metastasis is
already present. It’s likely that a MTC was already present when patient A presented with
goitre. This shows that patients with metastasized disease can survive for many years. The
progressive and fatal nature of MTC is illustrated by the clinical course of patient B. The
clinical course of patient C shows the sometimes mild course of MTC with a RET-mutation.
Most RET-mutations result in an aggressive biological behaviour, but in some patients the
clinical course is more favourable. The mutation of our patient had great implications for her
family, because carriers of the mutation are candidates for prophylactic thyroidectomy, with
or without central compartment dissection and lifelong follow-up for possible occurrence of a
pheochromocytoma and primary hyperparathyroidism.
Clinical presentation
Patients with MTC most often present with a palpable tumour in the neck. More than 50% of
patients already have lymph node metastases at the time of diagnosis and 15% have distant
metastasis.2 Patient A presented with diarrhoea, a symptom that can occur due to
hypersecretion of calcitonin.1 In patients with long term unexplained diarrhoea, MTC can be
considered in differential diagnosis. Retrospectively, patient C presented with at that time
unrecognised manifestations of MEN2A. Failure to recognise this syndrome can lead to
inadequate diagnosis and therapy. The patient did have a pheochromocytoma and had
therefore an increased risk of a potentially fatal hypertensive crisis.3
Diagnosis
According to current guidelines, an ultrasound guided FNAC in a solitary thyroid nodule is
preferred.4 In 63%-89% of MTC patients this gives the correct diagnosis, and 91%-100% of
MTC patients are operated based on FNAC results.1 When FNAC is inconclusive,
determination of serum calcitonin and CEA can be helpful. Calcitonin is a sensitive tumour
marker (sensitivity 98%), but there is still discussion about the cost-effectiveness because

MTC, a tumour with many appearances
23
thyroid nodules are common, MTC is relatively rare and false-positive findings occur
frequently.1,5
Morphological imaging with CT or MRI can be used for staging. Before starting treatment
it’s important to know if and where MTC metastases are present. To determine this,
functional imaging with 18F-FDG PET and 18F-DOPA PET can be used, because
morphological imaging is less sensitive. Fluor-18-DOPA is a relatively new tracer for
imaging of neuroendocrine tumours. DOPA is a precursor in the catecholamine synthesis,
which specifically occurs in many of these tumours. 18F-DOPA PET has the highest
sensitivity while 18F-FDG PET is more often positive in patients with a progressive tumour.6
Because of the risk of MEN2, which inherits autosomal dominantly, every patient with
MTC under the age of 50 is a candidate for genetic screening. Pre-operative determination of
serum calcium and metanephrines is indicated in all patients with MTC to rule out
hyperparathyroidism or pheochromocytoma. Manifestations of a MEN2 can then be
diagnosed and treated at an early stage.
When a RET-mutation is established in a patient, genetic screening of family members is
necessary to offer carriers – including children – a prophylactic thyroidectomy.7 The age of
children undergoing such a procedure varies between one and ten year and depends on the
mutation. Early recognition and adequate treatment of MTC in this way can prevent severe
morbidity and mortality.
Treatment
Primary tumour
The treatment of MTC is primary surgical and consists of a total thyroidectomy and possible
additional lymph node dissection.8 The extent of the lymph node dissection depends on the
expansion of the primary tumour and the presence of lymph node or distant metastasis.
Recurrence
The treatment of locoregional recurrent disease is also surgical. If there is curative intent an
extensive systematic central and lateral lymph node dissection is performed. If there are
distant metastases, the procedure is less extensive and more focussed on locoregional control,
and locoregional radiotherapy can be given.9 Iodine-131 can be given if there is proven uptake
of this tracer.1 Another option for therapy is radioactive labelled octreotide.10 However both

Chapter 2
24
therapies have modest results. Currently no effective systemic treatment is available and only
treatment in a clinical trial is advised.2
Follow-up
Measurement of serum calcitonin and CEA levels are important in the follow-up of patients
with MTC. A raised or raising tumour marker indicates local recurrent disease or metastasis.
Additional morphological and functional imaging can determine localisation, after which
possible treatment can be given.
Prognosis
The 10 year survival rate of MTC is around 75%.1 The most important prognostic factors are
the extent of the primary tumour at the time of diagnosis and the presence of lymph node or
distant metastasis. Despite the wide spectrum of available diagnostic modalities, MTC is often
diagnosed in a late stadium and survival has barely increased during the last decades.1
New therapeutic options
A large proportion of sporadic MTC patients has persistent disease activity with locoregional
recurrent disease and distant metastasis. Tyrosine kinase inhibitors might give these patients
new perspectives. These drugs target tyrosine kinase mediated signal transduction in
malignant C-cells. The RET receptor is a tyrosine kinase which is active in a large proportion
of the MTC patients, causing uninhibited proliferation of C-cells.1,7 The RET-receptor might
therefore be a good target for this antiproliferative therapy.
Multikinase inhibitors
Multikinase inhibitors like vandetanib and XL-184, which not only target the RET-receptor
but also other receptors like the vascular endothelial growth receptor (VEGFR) and the
mesenchymal-epithelial-transitionfactor (MET)-receptor are promising, with reported tumour
responses in 20%-33% of patients and stable disease in 25%-53%.11,12 However, in a
proportion of patients no effects have been seen. Therefore development of new drugs or
combination therapy is necessary.1,7

MTC, a tumour with many appearances
25
Conclusion
MTC is a rare tumour with different presentations. Because an apparent sporadic MTC can be
the first manifestation of a MEN2 syndrome, pheochromocytoma and hyperparathyroidism
have to be ruled out preoperatively through biochemical analysis. Furthermore RET-mutation
analysis is recommended, at least in patients under the age of 50 and in patients with a clinical
suspicion. In this case, family members can also be screened and prophylacticly treated if a
mutation is found. MTC patients are preferably treated in a multidisciplinary centre with
extensive experience in thyroid surgery, endocrinology, genetics and nuclear medicine.

Chapter 2
26
References
1. Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer: management guidelines of the American
Thyroid Association. Thyroid 2009;19:565-612.
2. Kebebew E, Ituarte PH, Siperstein AE, Duh QY, Clark OH. Medullary thyroid carcinoma: clinical
characteristics, treatment, prognostic factors, and a comparison of staging systems. Cancer
2000;88:1139-1148.
3. Milos IN, Frank-Raue K, Wohllk N, et al. Age-related neoplastic risk profiles and penetrance
estimations in multiple endocrine neoplasia type 2A caused by germ line RET Cys634Trp (TGC>TGG)
mutation. Endocr Relat Cancer 2008;15:1035-1041.
4. Links TP, Huysmans DA, Smit JW, et al. Guideline 'Differentiated thyroid carcinoma', including
diagnosis of thyroid nodules. Ned Tijdschr Geneeskd 2007;151:1777-1782.
5. Costante G, Durante C, Francis Z, Schlumberger M, Filetti S. Determination of calcitonin levels in C-cell
disease: clinical interest and potential pitfalls. Nat Clin Pract Endocrinol Metab 2009;5:35-44.
6. Koopmans KP, de Groot JW, Plukker JT, et al. 18F-dihydroxyphenylalanine PET in patients with
biochemical evidence of medullary thyroid cancer: relation to tumor differentiation. J Nucl Med
2008;49:524-531.
7. de Groot JW, Links TP, Plukker JT, Lips CJ, Hofstra RM. RET as a diagnostic and therapeutic target in
sporadic and hereditary endocrine tumors. Endocr Rev 2006;27:535-560.
8. de Groot JW, Links TP, Sluiter WJ, Wolffenbuttel BH, Wiggers T, Plukker JT. Locoregional control in
patients with palpable medullary thyroid cancer: results of standardized compartment-oriented
surgery. Head Neck 2007;29:857-863.
9. Kebebew E, Kikuchi S, Duh QY, Clark OH. Long-term results of reoperation and localizing studies in
patients with persistent or recurrent medullary thyroid cancer. Arch Surg 2000;135:895-901.
10. Kwekkeboom DJ, de Herder WW, Kam BL, et al. Treatment with the radiolabeled somatostatin analog
[177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol 2008;26:2124-2130.
11. Wells SA,Jr, Gosnell JE, Gagel RF, et al. Vandetanib for the treatment of patients with locally advanced
or metastatic hereditary medullary thyroid cancer. J Clin Oncol 2010;28:767-772.
12. Kurzrock R, Sherman S, Hong D, et al. A phase 1 study of XL184, a MET, VEGFR2, and RET kinase
inhibitor, administered orally to patients (pts) with advanced malignancies, including a subgroup of pts
with medullary thryoid cancer (MTC). EORTC 2008:119.

Chapter 3
Calcitonin testing for detection of medullary thyroid
cancer in patients with thyroid nodules
Hans H.G. Verbeek, Jan Willem B. de Groot, Wim J. Sluiter, Anneke C. Muller Kobold
Edwin R. van den Heuvel, John T.M. Plukker, Thera P. Links
Protocol published in: Cochrane Database of Systematic Reviews 2012, Issue 10
Review submitted

Chapter 3
28
Abstract
Background Thyroid nodules are very common. Calcitonin is a sensitive tumour marker for
the detection of medullary thyroid carcinoma (MTC). Although the European Thyroid
Association's guideline advocates calcitonin determination in patients with thyroid nodules,
the role of routine calcitonin testing in patients with thyroid nodules is still debatable.
Objectives The objective of this review was to determine the diagnostic accuracy of
calcitonin testing in the detection of MTC in patients with thyroid nodules.
Search methods We searched The Cochrane Library, MEDLINE, EMBASE and Web of
Science from inception to March 2013.
Selection criteria We included all retrospective and prospective cohort studies in which all
patients with thyroid nodules had undergone determination of basal calcitonin levels (and
stimulated calcitonin, if performed).
Data collection and analysis Two review authors independently scanned all retrieved records.
Data was extracted by using a standard data extraction form. We assessed risk of bias and
applicability using the QUADAS-2 (quality assessment of diagnostic accuracy studies) tool.
We obtained summary estimates of the expected operating points (sensitivity and specificity)
for each threshold using the HSROC model.
Main results In 16 studies, 73052 patients with nodular thyroid disease were identified.
Prevalence of MTC was 0.26% (n=187). Summary estimates of sensitivity and specificity for
basal calcitonin testing were 99.2% (95% CI 96.4%-100%) and 98.7% (95% CI 97.5%-100%)
respectively. For stimulated calcitonin testing sensitivity was slightly lower (98.5%; 95% CI
93.9%-100%) while specificity was higher (99.9%; 95% CI 99.7%-100%). The positive
predictive value (PPV) of basal calcitonin testing was 7.5% and for stimulated calcitonin
testing 72%.
Authors' conclusions Both basal and stimulated calcitonin testing have a high sensitivity and
specificity. The value of routine testing in patients with thyroid nodules remains questionable,
due to the low PPV of basal calcitonin testing. Whether routine calcitonin testing improves
prognosis in MTC patients remains unclear.

Calcitonin for detection of MTC
29
Background
Thyroid nodules are very common in the general population, and they can be found in 2.3% to
6.9% of all adults.1-3 Ultrasound detects an even higher frequency of thyroid nodules (17% to
69%).4 Thyroid nodules are more prevalent in women than in men (1.5% to 2% vs. 6.4% to
10%) and the incidence increases with age.1,5,6 Of all patients with thyroid nodules who
undergo fine needle aspiration (FNA), approximately 7.7% to 12% have thyroid cancer and in
3.3% to 3.7% of these patients medullary thyroid cancer (MTC) will be diagnosed.7-11
MTC is a neuro-endocrine tumour originating from the parafollicular C-cells. These C-
cells secrete calcitonin, a 32-amino acid peptide, which can be used as a sensitive tumour
marker. The 10-year survival for MTC is about 75%, but the prognosis depends on the extent
of the primary tumour, the presence of nodal disease and distant metastases.12 The primary
treatment for MTC is surgery, consisting of a total thyroidectomy with central compartment
dissection and even more extensive lymph node dissection depending on the extent of the
disease. Some patients develop recurrent disease, which limits the therapeutic options.
Patients with progressive disease may benefit from newly developed targeted therapies,
although early diagnosis of MTC and adequate surgical treatment remain crucial for a
favourable prognosis.13
Calcitonin is elevated in virtually all MTC patients and therefore a very sensitive tumour
marker, although MTC does not always produce calcitonin.14,15 On the other hand
hypercalcitoninaemia can also be caused by other conditions such as thyroiditis, sepsis,
hypercalcaemia, hypergastrinaemia, other neuroendocrine tumours, chronic renal failure,
chronic pulmonary disease, acute trauma, inhalation injury and pseudohypoparathyroidism.16-
19
In the recent guidelines of the American Thyroid Association (ATA) the diagnostic work-
up of a thyroid nodule consists, after history, physical examination and TSH determination, of
a diagnostic ultrasound and FNA when a nodule is seen on ultrasound. The role of calcitonin
testing in the work-up of thyroid nodules is unclear and there is no clinical consensus on
calcitonin testing. While the ATA's revised evidence-based guidelines for thyroid cancer do
not recommend for or against calcitonin determination, the European Thyroid Association's
consensus-based guideline advocates calcitonin determination in all patients with thyroid
nodules.20-22 Based on these guidelines and several studies, routine calcitonin testing is
practiced in multiple centres, while the use remains disputed.

Chapter 3
30
Despite the high sensitivity and specificity, only a small number of patients with elevated
calcitonin levels have MTC. This is due to the low prevalence of MTC. Accordingly, the
positive predictive value (PPV) in most studies is low, although some studies do report PPVs
of up to 100%.23 Furthermore, the cut-off level of calcitonin has not yet been established and
there are indications that different subgroups of patients need specific cut-off points, since
there are gender specific cut-off levels.24 Perhaps only a subset of patients should undergo
calcitonin testing. It is also unclear whether calcitonin testing can contribute to longer overall
survival or will increase the quality of life of MTC patients. Finally, to determine its role in
the evaluation of thyroid nodules the cost-effectiveness of calcitonin testing is also
important.25,26
Role of calcitonin testing
There are several potential roles for calcitonin testing in the diagnostic work-up of thyroid
nodules (Figure 1). First it can be used as a screening tool. Screening, however, implies that
the entire healthy population will undergo determination of calcitonin, which is currently not
effective or clinically relevant. Therefore we focus only on calcitonin testing in patients with
thyroid nodules, detected through palpation or ultrasound. It can be performed in all patients
with thyroid nodules at an early stage and before FNA (Figure1: I). In this case the supposed
sensitivity is very high but a great number of patients will have false positive results which
might lead to unnecessary surgery (resulting in life-long thyroid hormone supplementation
and risk of recurrent nerve damage and hypoparathyroidism). As FNA is also commonly used
for diagnosing other types of thyroid cancer which do not secrete calcitonin, calcitonin testing
as a replacement for FNA is irrational and clinically not relevant.
Calcitonin testing can be used as an add-on test after FNA in patients with suspicious or
indeterminate cytology (Figure 1: II). In this case the number of false positives will be lower,
but some MTC patients might be missed (when cytology is benign) with the risk that MTC in
these patients will be diagnosed at a later stage or not at all. Calcitonin testing can also be
used as a preoperative test in all patients who will undergo thyroid surgery (Figure 1: III). In
that case not all MTC patients will be detected but the risk of patients who undergo an
operation receiving too restricted surgery decreases. This form of calcitonin testing will not be
included in this review as it is more focused on preoperative assessment of tumour type than
on screening.

Calcitonin for detection of MTC
31
This review will address the value of calcitonin testing for diagnosing MTC in patients
with thyroid nodules for the triage and add-on roles of the calcitonin test. We want to give
more insight into the different sensitivities and specificities for these different roles. By
providing data on the diagnostic accuracy of the calcitonin test in light of the low prevalence
of MTC in thyroid nodules we want to contribute to the discussion on the role of the
calcitonin test in patients with thyroid nodules.
Figure 1 Possible roles of calcitonin testing

Chapter 3
32
Index tests
The available test for diagnosing MTC in thyroid nodules is the calcitonin assay. The former
radioimmunoassays for calcitonin measurement recognised the monomeric and the dimeric
form of calcitonin, as well as its precursors leading to false-positive results. The more recent
and most commonly used immunometric assays mainly recognise the mature, monomeric
form of calcitonin. They rely on a 'sandwich' formation by two monoclonal or polyclonal
antibodies recognising different epitopes on calcitonin.27 However, limitations still exist in the
calcitonin assays. If a one-step assay is applied, in case of an extremely high calcitonin
concentration, all the antibodies including the signal antibodies are saturated with the antigen,
preventing a sandwich formation. Then, the antigen concentration measured may be falsely
low (also known as the ‘high dose hook’).28 Furthermore, also mainly in one-step assays, the
presence of heterophilic antibodies may give erroneously high results of calcitonin by cross-
linking the antibodies in the absence of calcitonin.29,30 Very rarely ‘blocking’ heterophilic
antibodies are also able to produce false-negative results.31 Alternative methods for
quantification, such as mass spectrometry may circumvent this problem, as was also shown
for thyroglobulin.32 Furthermore, despite the World Health Organization international
reference preparation for human calcitonin, differences exist between the same type of assays
of different manufacturers, making it even more difficult to compare results from different
studies and to establish an optimal cut-off value.27,33,34
To improve the specificity of the calcitonin assay, calcitonin stimulation tests with
pentagastrin or calcium are used.35 These stimulation tests can distinguish calcitonin secreted
by MTC from other sources of calcitonin but there are some limitations.36 Stimulation with
pentagastrin can induce unpleasant side effects, such as nausea, vomiting or skin rash.37
Furthermore, pentagastrin is not available in several countries. Calcium stimulation tests are
better tolerated but are not routinely used although an increasing number of small studies have
advocated the use of calcium.38-40 We planned to perform a heterogeneity analysis on whether
basal calcitonin, stimulated calcitonin, or both, were determined and also the type of
stimulation test used.
Alternative tests
The alternative test for diagnosing MTC in patients with thyroid nodules is fine needle
aspiration cytology (FNAC) with eventually immunohistochemical examination in suspicious
lesions. FNAC is an accurate and cost-effective method for evaluation of thyroid nodules, but

Calcitonin for detection of MTC
33
the sensitivity for diagnosis of MTC is not optimal, ranging from 63% to 89%.41-43 The
outcome of the FNAC in these studies resulted in surgery in 91% to 100% of patients.
Although a large proportion of the patients received surgery despite incorrect FNAC results,
this might be an inadequate test as MTC requires a different surgical approach than
differentiated thyroid cancer. Other techniques, such as measuring calcitonin levels in
washout fluids of fine needle aspirates may improve accuracy but few studies have reported
on this in limited numbers of patients.44-46
Rationale
A number of studies and reviews on this topic advocate calcitonin testing for detection of
MTC. These studies are hard to compare, however, since they have different inclusion criteria
and different cut-off points for calcitonin levels. Moreover, there is no consensus between the
American and European guidelines on thyroid nodules. Calcitonin testing in patients with
thyroid nodules is associated with a high rate of false-positive results and a low PPV. It has
not been established that calcitonin testing reduces MTC-related mortality in these patients.
Cheung et al. stated that calcitonin testing in the US is cost-effective at the same level as
mammography screening and advocates calcitonin testing in subgroups of patients such as
young men with larger thyroid nodules, but this also remains a matter for debate.26
Objectives
The objective of this review was to determine the diagnostic accuracy of calcitonin testing in
the detection of MTC in patients with thyroid nodules.
Investigation of sources of heterogeneity
We planned to investigate several potential sources of heterogeneity, including differences in
cut-off values, assay types and different verification methods. Possible factors that were
evaluated as source for heterogeneity were;
• Age.
• Gender.
• Nodules detected by palpation or ultrasound.
• Nodule size.
• Number of nodules.
• Sonographic morphology of thyroid nodules.

Chapter 3
34
• FNA procedures performed through ultrasound guidance versus palpation.
• Basal versus stimulated calcitonin testing.
Methods
Criteria for considering studies for this review
Types of studies
We included all retrospective and prospective cohort studies in which all patients with thyroid
nodules had undergone determination of basal calcitonin levels (and stimulated calcitonin, if
performed).
Participants
We included patients with nodular thyroid disease (defined as solitary thyroid disease
(toxic/non-toxic), multinodular thyroid disease (toxic/non-toxic), autonomously functioning
thyroid nodule) found by palpation or on ultrasound in whom calcitonin testing was
performed. We distinguished between studies in which calcitonin testing was performed as a
triage (before FNAC) or as an add-on test (after FNAC). We included patients with coexisting
non-nodular disease such as autoimmune thyroid disease (Graves' disease or Hashimoto's
thyroiditis) and subacute thyroiditis. We excluded patients with only non-nodular thyroid
disease. If studies included both patients with nodular and non-nodular disease, we included
them only if it was possible to separate the calcitonin levels and surgical outcomes of these
patient groups or if fewer than 10% of patients had non-nodular disease. We excluded patients
with known sporadic or familiar MTC (MEN2A/B, FMTC) prior to calcitonin screening. We
also excluded studies that included these patients and did not describe them separately.
Index tests
The index tests for this review included all serum tests used to determine basal and stimulated
serum calcitonin levels.
Target conditions
The target condition was MTC.

Calcitonin for detection of MTC
35
Reference standards
The optimal clinical reference standard for diagnosis of MTC was considered
histopathological examination of the thyroid after surgery of all patients, even patients
without elevated calcitonin levels. In all of the studies, however, the problem of differential
verification was encountered and only patients with (markedly) elevated calcitonin levels or
patients with suspicious cytology had histological verification (although some patients did
undergo surgery for other reasons e.g. mechanical complaints due to a multinodular goitre).
We planned therefore to make use of other reference standards such as clinical follow-up. A
follow-up of at least three years was considered adequate as most clinically relevant MTCs
will be identified at that time, while longer follow-up carries the risk that MTC patients are
diagnosed while not having the disease at the time of calcitonin testing. To determine whether
standard of verification significantly influences accuracy, we planned to include method of
verification in the heterogeneity analysis.
Search methods for identification of studies
Electronic searches
We used the following sources for the identification of trials.
• The Cochrane Library.
• MEDLINE.
• EMBASE.
• Web of Science.
For detailed search strategies please see Appendix 1. The Editorial Base of the Cochrane
Metabolic and Endocrine Disorders Group provided support for generating the optimal search
strategy. We used PubMed's 'My NCBI' (National Centre for Biotechnology Information)
email alert service for the identification of newly published studies using a basic search
strategy (see Appendix 1). We included studies published in English language.
Searching other resources
We examined the references lists of relevant publications for additional studies. We searched
in Pubmed for related articles of relevant studies.

Chapter 3
36
Data collection and analysis
Selection of studies
To determine the studies to be assessed further, two review authors (HHGV, JWBG)
independently scanned the abstract, title or both sections of every record retrieved. All
potentially relevant articles were investigated as full text. Any disagreements were resolved
by a third reviewer (TPL). A PRISMA (preferred reporting items for systematic reviews and
meta-analyses) flow-chart of study selection was made.47
Data extraction and management
We extracted data on study design and study population using a standard data extraction form
(Appendix 2), in which we included the following items:
• Study design.
• Included number of patients.
• Inclusion and exclusion criteria.
• General patient characteristics.
• Type of calcitonin assay and cut-off values.
• Number of patients with nodular thyroid disease.
• Number of patients with palpable nodules and/or nodules on ultrasound.
• Number of patients who had undergone calcitonin testing and number of positive
patients.
• Number of patients operated and reason for operation.
• Number of patients with known follow-up and outcome of follow-up.
• Histological outcome of patients operated.
• Number of patients with MTC.
Assessment of methodological quality
We assessed risk of bias and applicability using the QUADAS-2 (quality assessment of
diagnostic accuracy studies) tool. We rated each of the four key domains (patient selection,
index test, reference standard, flow and timing) using the signalling questions as developed by
the QUADAS-2 group.48 The criteria for each signalling question are provided in Appendix 3.
We scored all items in the QUADAS-2 tool as ‘yes’, ‘no’ or ‘unclear', and used graphs to
present overall scores of risk of bias and applicability for each domain.

Calcitonin for detection of MTC
37
Statistical analysis and data synthesis
We incorporated true positives, false positives, true negatives and false negatives of each
study in a 2x2 table and calculated test sensitivity and specificity with corresponding 95%
confidence intervals. For extraction of data, we used pre-specified cut-offs based on previous
literature with different cut-offs for basal and stimulated calcitonin levels. These cut-off
values were 10,15, 20, 30, 50 and 100 pg/ml for basal calcitonin levels and 100 pg/ml and 200
pg/ml for stimulated calcitonin levels. We entered the data into RevMan 5.2.3, to graphically
present coupled forest plots, showing the pairs of sensitivity and specificity of each study, for
each threshold.
Investigations of heterogeneity
We used SAS software for meta-analysis. We obtained summary estimates of the expected
operating points (sensitivity and specificity) for each threshold using the HSROC model.49
Depending on the number of included studies and available data, covariates were added in this
model, for investigation of possible sources of heterogeneity.
Sensitivity analyses
We performed sensitivity analyses on the different domains scored on the QUADAS-2 tool, in
order to explore the influence of the quality of the included studies.
Results
Results of the search
A total of 2947 unique records were identified by our search in January 2012 and updated
searches in June 2012 and March 2013. An additional two records were identified by
examining references list of relevant publications. One other relevant publication was also
included. Screening of all records resulted in 35 publications that were eligible for further
evaluation. After assessment 19 articles were excluded. Eventually 16 studies were included
in this review (Figure 2).

Chapter 3
38
Included studies
Characteristics of the 16 included studies are shown in the table Characteristics of included
studies (Appendix 4).50-65 A total of 73052 patients with nodular thyroid disease were
included in these studies, of which 72368 underwent basal calcitonin testing with or without
stimulated calcitonin testing as shown in Table 1. A total of 187 MTC patients were
identified. Three studies performed only basal calcitonin testing, whereas in thirteen studies
both basal and stimulated calcitonin testing was performed.
Figure 2 Study flow diagram.
Calcitonin assays
Two studies used an radio immunometric assay (RIA) for determination of calcitonin,
including one study which during the study period switched from a RIA assay to an
immunoradiometric assay (IRMA).50,51 Five other studies used also an IRMA assay.52,54,56,60,61

Calcitonin for detection of MTC
39
Ta
ble
1 O
verv
iew
of
stu
dy
po
pu
lati
on
s
Stu
dy
ID
[n
] w
ith
no
du
lar
thy
roid
dis
ea
se
[n]
wit
h
calc
ito
nin
test
ing
[n]
wit
h
po
siti
ve
ba
sal
calc
ito
nin
test
ing
[n]
wit
h
stim
ula
ted
calc
ito
nin
test
ing
[n]
wit
h
po
siti
ve
stim
ula
ted
calc
ito
nin
test
ing
[n]
op
era
ted
[n
] w
ith
foll
ow
-up
[n]
wit
h M
TC
M
TC
pre
va
len
ce
Rie
u 1
99
5
46
9
46
9
4
4
4
15
N
R
4
0.8
5
Ozg
en
19
99
7
73
7
73
4
n
p
- 1
75
3
4
0
.52
Ha
hm
20
01
1
44
8
14
48
5
6
39
1
2
19
4
NR
1
0
0.6
9
Ha
tzl-
Gri
ese
nh
ofe
r 2
00
2
38
99
3
89
9
23
0
15
7
30
3
9
43
1
2
0.3
1
Eli
sei
20
04
1
08
64
1
08
64
4
7
45
4
4
44
4
4
44
0
.41
Ka
ran
ika
s 2
00
4
19
5
19
5
13
1
3
2
1
1
1
0.5
1
Vie
rha
pp
er
20
05
1
02
92
1
01
57
5
07
4
81
1
03
7
6
32
3
6
0.3
5
Pa
pi
20
06
1
47
4
14
25
2
3
19
6
3
15
N
R
9
0.6
3
Sch
eu
tz 2
00
6
10
5
10
5
5
5
0
0
NR
0
0
Co
sta
nte
20
07
5
81
7
58
17
2
82
5
8
17
7
47
2
12
1
5
0.2
6
Rin
k 2
00
9
21
92
8
21
92
8
88
5
21
8
62
1
57
2
14
2
8
0.1
3
Ha
sse
lgre
n 2
01
0
95
9
70
2
39
n
p
- 2
46
7
02
*
6
0.8
5
He
rma
nn
20
10
1
00
7
10
07
1
7
16
4
5
1
2
2
0.2
0
Sch
ne
ide
r 2
01
2
11
27
0
11
27
0
32
1
4
12
1
8
10
1
2
0.1
1
Gio
va
ne
lla
20
12
1
47
9
12
36
1
4
14
4
7
7
2
0
.16
Gra
ni
20
12
1
07
3
10
73
4
1
np
-
3
NR
2
0
.19
To
tal
73
05
2
72
36
8
21
99
1
08
3
30
0
20
42
1
28
0
18
7
0.2
6
"-"
de
no
tes
no
t re
po
rte
d.
* C
ross
lin
kag
e w
ith
Da
nis
h T
hyr
oid
Ca
nce
r D
ata
ba
se.
Ab
bre
via
tio
ns:
MT
C:
me
du
llary
th
yro
id c
an
cer,
np
: N
ot
pe
rfo
rme
d

Chapter 3
40
Two of these five studies switched during the study period to a chemiluminescence assay
(ICMA).56,61 The remaining nine studies used an ICMA assay.53,55,57-59,62-65 In conclusion,
thirteen studies used only one calcitonin assay during their study period, while three studies
used two assays. One of these three studies, that switched from an IRMA to an ICMA assay,
used the ICMA assay only in 14 out of 702 patients, and was therefore in further analyses
regarded as using an IRMA assay.61 The other two studies that switched from calcitonin assay
were not included in the covariate analysis regarding assay type.
In total, calcitonin assays of nine different manufacturers were used (Appendix 4;
Characteristics of included studies). Especially in the seven studies using a RIA or IRMA
assay a large heterogeneity in manufacturers was present (n=7); some studies used during the
study period assays from 2 different producers. Within the nine studies using a ICMA assay,
one study did not report the manufacturer,65 while in the other studies an assay was used from
one of two producers.
Verification method
Differential verification was present in all studies; all patients with a (highly) elevated basal
and/or stimulated calcitonin underwent surgery, while only a subset of patients with negative
calcitonin tests had surgery. We considered clinical follow-up of calcitonin negative patients
as an appropriate alternative for detection of missed MTC patients. However, none of the
included studies did report on clinical follow-up of all of their calcitonin negative patients.
Only in the study of Hasselgren follow-up was performed that consisted of cross linkage with
a national thyroid cancer database.61
Calcitonin as triage or add-on test
None of the studies included, provided explicit information on the role of calcitonin testing in
the diagnostic pathway of thyroid nodules. In nine studies FNA was described in the materials
and methods section as part of the diagnostic protocol. Most of these studies stated that
surgery was indicated if basal or stimulated calcitonin was clearly elevated (e.g. >100 pg/ml)
regardless of the results of FNA. In these studies the role of calcitonin testing can be
considered as a triage test in which calcitonin positive patients are subjected to surgery, while
calcitonin negative patients require more diagnostic work-up in the form of FNA. In all
studies in which FNA was not described in the diagnostic protocol, calcitonin testing was
performed in all included patients, independent of another diagnostic procedure, and if

Calcitonin for detection of MTC
41
markedly elevated an indication to perform surgery. Therefore in these studies calcitonin
testing was also regarded as a triage test.
Patient and study characteristics
Average and/or median age was described in twelve studies, but only one study reported the
results of calcitonin testing specified in different age groups.58 Information on gender of the
included patients was provided in 15 studies, although only in seven studies detailed
information on outcome was given for both sexes. In nine studies information was available
on whether thyroid nodules in the included patients were detected through palpation or US;
four studies included patients with thyroid nodules found by US and five studies included
patients with thyroid nodules detected through US or palpation. With regard to nodule size
only one study provided information on summary measures of size for the included patients,
although no detailed information was provided for patients with elevated calcitonin levels. No
study presented information on number of nodules or US morphology of all patients. In four
studies information was given on whether FNA procedures were performed through palpation
or US; in one study both techniques were performed, in the three others US-guided FNA was
performed.
Excluded studies
In the table Characteristics of excluded studies (Appendix 5) reasons for exclusion for the 19
excluded studies are shown. Of six studies only a meeting abstract was available and no full
text article was published.66-71 Four articles were written in non-English language.72-75 Two
studies used a study population that was also described in a later publication.76,77 Three
studies did not specify the numbers of patients with thyroid nodules.78-80 Three studies
reported on calcitonin testing in pre-operative patients, which is not the topic of this review.81-
83 One study reported on calcitonin testing in isthmic thyroid nodules; because this patient
group evaluated only nodules in a specific part of the thyroid, we excluded this study.84
Methodological quality of included studies
In Figure 3 the overall quality of the 16 included studies is shown, with regard to the risk of
bias and concerns about applicability scored according to the QUADAS 2 domains. In the
domain Patient selection, one study scored high on the risk of bias as patients were included
who showed evidence of growth during follow-up examinations.53 This might have increased

Chapter 3
42
the rate of included patients with a malignancy. In all studies the risk of bias by the
conduction or interpretation of the calcitonin test was scored low. The risk of bias with the
conduct or interpretation of the reference standard was unclear in all studies, for the reference
standard in calcitonin negative patients, was not described. Due to this lack of reference
standard, resulting in a verification bias, the risk of bias with regard to flow and timing was in
all studies expect one regarded as high. In the only study using a cross linkage with a national
thyroid cancer database the risk was scored as unclear.61 No concerns of applicability existed
in all studies. In Figure 4 the individual quality assessment of all studies can be found.
Figure 3 Risk of bias and applicability concerns graph: review authors' judgements about each domain
presented as percentages across included studies
Findings
The sensitivity of the reported basal calcitonin testing cut-off in the included studies ranged
from 83% to 100%, while the specificity ranged from 94% to 100% (Figure 5 and Figure 6).
In the study of Schuetz et al. no MTC patients with nodular thyroid disease were identified so
sensitivity could not be calculated.57 The summary estimates of sensitivity and specificity
were 99.2% and 98.7% respectively (95% Confidence intervals (CI) 96.4%-100% and 97.5%-
100% respectively).
Effect of cut-off value
We extracted data for several cut-off values from the included studies, ranging from 10 pg/ml
to 100 pg/ml. With the cut-off value of 10 pg/ml the sensitivity of the individual studies
ranged from 92% to 100% while specificity ranged from 95% to 99%; summary estimates
were 99.9% (95% CI: 99.1-100%) for sensitivity and 96.8% (95% CI: 95.5%-98.1%) for
specificity (Table 2). With the highest cut-off value of 100 pg/ml sensitivities ranged from
42%-100% and specificity from 95%-100%. Summary estimates of sensitivity and specificity

Calcitonin for detection of MTC
43
for the different cut-off values of basal calcitonin >10 pg/ml could not be calculated due to
limited number of studies.
Figure 4 Risk of bias and applicability concerns summary: review authors'
judgements about each domain for each included study
Effect of stimulated calcitonin
Thirteen studies were included in the analysis of stimulated calcitonin. Sensitivity of
individual studies ranged between 82% and 100%. Specificity ranged from 99% to 100%
(Figure 7). Summary estimates were 98.5% (95% CI 93.9%-100%) for sensitivity and 99.9%
(95% CI: 99.7%-100%) for specificity, respectively (Summary of findings Table 1, Figure 8).

Chapter 3
44
Due to limited numbers of studies no summary estimates could be calculated for different cut-
off values.
Table 1 Summary of findings
Summary points (95% CI) No. of patients (studies)
Basal calcitonin
Reported cut-off value Sensitivity 99.2% (96.4%-100%)
Specificity 98.7% (97.5%-99.9%)
72369 (16)
10 pg/ml Sensitivity 99.9% (99.1%-100%)
Specificity 96.8% (95.5%-98.1%)
44393 (10)
Basal and stimulated reported calcitonin
Reported cut-off value Sensitivity 98.5% (93.9%-100%)
Specificity 99.9% (99.7%-100%)
69702 (13)
Subgroup analysis
Gender
Female
Male
Sensitivity 95.9% (83.1%-100%)
Specificity 99.0% (97.6%-100%)
Sensitivity 100% (NA-NA*)
Specificity 98.2% (95.9%-100%)
14858 (6)
4339 (6)
Figure 5 Forest plot of basal reported cut-off values.

Calcitonin for detection of MTC
45
Figure 6 Summary ROC Plot of basal reported cut-off values.
Effect of gender
In Summary of findings Table 1 summary estimates for basal reported calcitonin for
subgroups of females and males are reported. For females the sensitivity ranged between 96%
and 100% and the specificity ranged between 96% and 100%. For males the sensitivity ranged
between 82% and 100% and the specificity ranged and between 90% and 100% (Figure 9).
Summary estimates for females were 95.9 % (95% CI 83.1%-100%) for sensitivity and 99.0%
(95% CI: 97.6%-100%) for specificity. Summary estimates for males were 100% (95% CI
NA) and 98.2% (95% CI: 95.9%-100%) for sensitivity and specificity respectively. Only one
study used gender specific basal calcitonin cut-off values for all included patients.53 Another
study which used two assays during the study period also had a gender specific cut-off for the
second assay, but this concerned only 14 patients.61 The study of Rink et al. used gender
specific stimulated calcitonin cut-off values.60 Due to limited number of studies no summary
estimates could be calculated for different cut-off values.

Chapter 3
46
Figure 7 Forest plot of basal and stimulated reported cut-off values.
Effect of assay type, detection method of thyroid nodules and FNA method
Due to limited number of studies no summary estimates could be calculated for subgroups
with respect to assay type or manufacturer, detection method of thyroid nodules and method
of FNA.
Figure 8 Summary ROC Plot of basal and stimulated reported cut-off values.

Calcitonin for detection of MTC
47
Sensitivity analysis
We planned to perform a sensitivity analysis with regard to quality items scored with the
QUADAS 2 tool. However, no large differences were seen between studies regarding quality
items. Only two studies had aberrant scores with regard to the risk of bias on the domains of
patient selection and flow and timing (Figure 4).
Figure 9 Forest plot of basal calcitonin reported cut-off values for females and males.

Chapter 3
48
Discussion
Summary of main results
In this review we included 16 studies for determination of the diagnostic accuracy of
calcitonin testing in patients with thyroid nodules. We found high summary estimates of
sensitivity and specificity for the reported basal calcitonin cut-off value of all studies. For
reported basal and stimulated calcitonin sensitivity was slightly lower and specificity slightly
increased. In subgroup analysis, sensitivity in females was lower, while specificity was higher
compared to males.
Strengths and weaknesses of the review
We evaluated the diagnostic accuracy of calcitonin testing for detection of medullary thyroid
cancer in patients with thyroid nodules with a comprehensive search of literature, and
performing a formal diagnostic meta-analysis.
One of the major limitations of this review is the lack of adequate reference standards for
calcitonin negative patients in nearly all included studies. This increases the risk that false
negative patients are missed and the reported sensitivities are overestimated. In two of the
included studies false negative MTC patients were identified, although in the study of
Vierhapper et al. two of the three false negative patients were not operated and a histological
diagnosis was not obtained.56 In studies performing preoperative calcitonin testing, the rate of
false negative MTC patients ranged between 4.3%- 12.5% of all MTC patients identified.18,83
Because the prevalence of MTC is low in patients with thyroid nodules, even a small number
of false negative patients can markedly affect sensitivity. The clinical relevance of these false
negative MTC can be discussed as in most calcitonin testing studies this are patients with a
micro MTC without nodal metastasis. However, reports also exist on MTC patients with more
aggressive disease and undetectable calcitonin levels.85
Another limitation of this study is the small number of studies that could be included in
final analyses. Due to this small number only for a few subgroups summary estimates could
be calculated. Furthermore, no optimal cut point could be assessed due to the heterogeneity of
the used cut-off levels in the different studies. This was further complicated by the large
heterogeneity in assay types and manufacturers.

Calcitonin for detection of MTC
49
Other reports
Other reviews have been published on the value of calcitonin testing in the detection of
medullary thyroid carcinoma, although no systematic reviews were performed. Daniels
provided an overview of 15 studies but included also patients with preoperative calcitonin
testing and multiple studies of one study group. The author concluded that due to the large
reservoir of undetected of medullary thyroid micro carcinoma's of uncertain malignant
potential, and the unavailability of pentagastrin in the US, calcitonin testing is not indicated in
the United States and Canada.86 Costante et al. evaluated 11 studies in their review and
concluded that the question whether to routinely measure calcitonin remained unsolved
because no evidence exists whether testing actually reduces MTC-related mortality.87
Applicability of findings to the review question
This review provides summary estimates of sensitivity and specificity for basal and stimulated
calcitonin. The role of calcitonin testing in the diagnostic evaluation in thyroid nodules
remains unclear. The final purpose of calcitonin testing is to detect MTC patients in an early
stage, in which the chance of biochemical cure improves and the prognosis of patients. The
findings of this review indicate that calcitonin testing is a very sensitive and specific test, but
this has to be interpreted bearing in mind the low prevalence of MTC. The positive predictive
value of calcitonin testing is therefore low, especially with lower cut-off values. Although
several conditions are known to cause increased calcitonin levels, still in a fairly large
proportion of patients with elevated calcitonin levels MTC cannot be excluded. Repeated
calcitonin testing and follow up in these patients is therefore warranted. A number of these
patients will be operated without histological evidence of a MTC. Some patients will have C-
Cell hyperplasia, but the clinical relevance of this finding and its malignant potential remain
unclear.
Cost effectiveness in health care becomes more and more important. In this review no
formal cost effectiveness analysis is performed, so no validated statements can be made.
However, Cheung et al performed in 2008 a cost effectiveness analysis in which calcitonin
testing was concluded to be cost effective similar to colonoscopy and mammography
screening.26 In their hypothetical model, several parameters had an important influence on
cost-effectiveness, such as specificity of the calcitonin test and prevalence of MTC. Cheung et
al. used a cut-off value of 50 pg/ml with a specificity of 98 % in the base line model, almost
similar to the 98.7% specificity we found of the basal calcitonin test. However, the MTC

Chapter 3
50
prevalence established in our review was 0.26%; one third of the prevalence used by Cheung
et al. With a three times lower prevalence, costs will also increase almost three times. In a
review of autopsy studies the prevalence of occult MTC was estimated to be 0.14%.88
Although it is not known if all MTC's detected at autopsy are clinically irrelevant and will be
detected through calcitonin screening, a proportion of these tumours will be, further lowering
the prevalence of clinically relevant MTC's. Our findings with regard to sensitivity, specificity
and MTC prevalence, applied to the cost-effectiveness model of Cheung et al. imply that
basal calcitonin testing does not seem to be cost effective. The effects on cost-effectiveness of
a combined basal and stimulated calcitonin on cost effectiveness is more difficult to estimate.
In their model Cheung et al. give a sensitivity and specificity for this combined approach of
80% and 98% respectively while our summary estimates show both a higher sensitivity and
specificity. However, it is likely that also this model is influenced by the prevalence of MTC,
decreasing cost-effectiveness with lower prevalence.
Implications for practice
Calcitonin testing can be a sensitive and specific instrument for detecting MTC in thyroid
nodules. However, due to the low prevalence of MTC its role as a screening tool remains
unclear. If we apply our findings from a basal calcitonin test with a cut-off of 10 pg/ml to a
population of 10000 patients with a MTC prevalence of 0.26% (mean prevalence of the
included studies), 26 patients will have MTC. All these 26 patients will have an elevated basal
calcitonin test, while 319 patients without MTC also will have an elevated basal calcitonin.
The positive predictive value of the calcitonin test in this situation is 7.5%. Surely not all
patients with an elevated basal calcitonin will be operated, but even if a cause of elevated
calcitonin can be found in 90% of the false positive patients, more than 50% (n=32) of the
patients will be operated unnecessary. Increasing cut-off values results in a higher positive
predictive value but at the cost of missed MTC patients. An optimal cut-off value for is
therefore difficult to generate. Also the variation between assays used in different studies
makes it hard to establish a common cut-off value. Adding a stimulated calcitonin test
increases specificity with a very little effect on sensitivity. Still all 26 patients with MTC will
be detected and only 10 patients will have a false positive stimulated calcitonin test. In this
scenario, the positive predictive value increases almost 10 times to 72%. However, the most
commonly used stimulative, pentagastrin, is not available in several countries.
The major reason to perform calcitonin testing is to ultimately improve prognosis of MTC
patients. The supposed value of calcitonin testing is the detection of MTC patients in an

Calcitonin for detection of MTC
51
earlier stage in which biochemical cure is still possible. However, to assess this, one has to
know which of the MTC patients would not have been detected trough regular examinations
(US/FNA/optional calcitonin), and which of these detected patients by calcitonin testing have
or will develop a clinically relevant MTC. Some studies demonstrate that survival was
significantly improved after introduction of routine calcitonin testing in patients with thyroid
nodules.54,89,90 However, these studies have made their comparison with a historical group,
and other factors might also have contributed to improved survival. These factors include, for
instance, improved surgical treatment strategies and use of ultrasound. Furthermore, it is also
interesting to note that MTC was supposedly detected at an earlier stage in these studies, but
the age of the screened MTC patients was not lower compared to the patients that were not
screened.54,89 As MTC is considered to be a slow growing tumour which takes several years to
become clinically evident, the fact that MTC patients in the screened groups are of equal or
even higher age, might indicate that additional MTC patients have been detected who would
have otherwise had an indolent course of their disease. Another indication that otherwise
undetected and possibly indolent MTC patients are identified is the increased number of MTC
patients detected in shorter periods in the calcitonin tested patients compared to the historical
cohorts.54,90
Implications for research
This review shows that the diagnostic accuracy of calcitonin testing in MTC is high.
However, this conclusion is based on studies in which the MTC prevalence in calcitonin
negative patients might have been underestimated. Future studies should therefore report
more accurately on the follow-up of calcitonin negative patients, to ensure that no MTC
patients are missed, and also to provide more information on the clinical behaviour of these
tumours. Furthermore accurate reporting of assay type and manufacturer is crucial for
establishing optimal cut-off points for diagnosis of MTC. Also the role of the calcitonin test,
being a triage or add-on test next to FNA (with or without measurement of calcitonin in
washout fluids) should be further evaluated. Furthermore reporting results for subgroups may
also identify subgroups with a higher MTC prevalence in which calcitonin testing can be
more cost effective.

Chapter 3
52
References
1. Vander JB, Gaston EA, Dawber TR. The significance of nontoxic thyroid nodules. Final report of a 15-
year study of the incidence of thyroid malignancy. Ann Intern Med 1968;69:537-540.
2. Rallison ML, Dobyns BM, Meikle AW, Bishop M, Lyon JL, Stevens W. Natural history of thyroid
abnormalities: prevalence, incidence, and regression of thyroid diseases in adolescents and young
adults. Am J Med 1991;91:363-370.
3. Wiest PW, Hartshorne MF, Inskip PD, et al. Thyroid palpation versus high-resolution thyroid
ultrasonography in the detection of nodules. J Ultrasound Med 1998;17:487-496.
4. Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules
discovered incidentally on thyroid imaging. Ann Intern Med 1997;126:226-231.
5. Vanderpump MP, Tunbridge WM, French JM, et al. The incidence of thyroid disorders in the
community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol (Oxf) 1995;43:55-68.
6. Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med 1993;328:553-559.
7. Gilliland FD, Hunt WC, Morris DM, Key CR. Prognostic factors for thyroid carcinoma. A population-
based study of 15,698 cases from the Surveillance, Epidemiology and End Results (SEER) program
1973-1991. Cancer 1997;79:564-573.
8. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. A National Cancer Data Base report on 53,856 cases
of thyroid carcinoma treated in the U.S., 1985-1995 [see commetns]. Cancer 1998;83:2638-2648.
9. Marqusee E, Benson CB, Frates MC, et al. Usefulness of ultrasonography in the management of
nodular thyroid disease. Ann Intern Med 2000;133:696-700.
10. Nam-Goong IS, Kim HY, Gong G, et al. Ultrasonography-guided fine-needle aspiration of thyroid
incidentaloma: correlation with pathological findings. Clin Endocrinol (Oxf) 2004;60:21-28.
11. Papini E, Guglielmi R, Bianchini A, et al. Risk of malignancy in nonpalpable thyroid nodules: predictive
value of ultrasound and color-Doppler features. J Clin Endocrinol Metab 2002;87:1941-1946.
12. de Groot JW, Plukker JT, Wolffenbuttel BH, Wiggers T, Sluiter WJ, Links TP. Determinants of life
expectancy in medullary thyroid cancer: age does not matter. Clin Endocrinol (Oxf) 2006;65:729-736.
13. Tan A, Xia N, Gao F, Mo Z, Cao Y. Angiogenesis-inhibitors for metastatic thyroid cancer. Cochrane
Database Syst Rev 2010;(3):CD007958. doi:CD007958.
14. Redding AH, Levine SN, Fowler MR. Normal preoperative calcitonin levels do not always exclude
medullary thyroid carcinoma in patients with large palpable thyroid masses. Thyroid 2000;10:919-922.
15. Wang TS, Ocal IT, Sosa JA, Cox H, Roman S. Medullary thyroid carcinoma without marked elevation of
calcitonin: a diagnostic and surveillance dilemma. Thyroid 2008;18:889-894.
16. Baudin E, Bidart JM, Rougier P, et al. Screening for multiple endocrine neoplasia type 1 and hormonal
production in apparently sporadic neuroendocrine tumors. J Clin Endocrinol Metab 1999;84:69-75.
17. Machens A, Haedecke J, Holzhausen HJ, Thomusch O, Schneyer U, Dralle H. Differential diagnosis of
calcitonin-secreting neuroendocrine carcinoma of the foregut by pentagastrin stimulation.
Langenbecks Arch Surg 2000;385:398-401.
18. Niccoli P, Brunet P, Roubicek C, et al. Abnormal calcitonin basal levels and pentagastrin response in
patients with chronic renal failure on maintenance hemodialysis. Eur J Endocrinol 1995;132:75-81.
19. Vlaeminck-Guillem V, D'herbomez M, Pigny P, et al. Pseudohypoparathyroidism Ia and
hypercalcitoninemia. J Clin Endocrinol Metab 2001;86:3091-3096.
20. Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management
guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009;19:1167-
1214.
21. Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer: management guidelines of the American
Thyroid Association. Thyroid 2009;19:565-612.
22. Pacini F, Schlumberger M, Dralle H, et al. European consensus for the management of patients with
differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol 2006;154:787-803.
23. Costante G, Durante C, Francis Z, Schlumberger M, Filetti S. Determination of calcitonin levels in C-cell
disease: clinical interest and potential pitfalls. Nat Clin Pract Endocrinol Metab 2009;5:35-44.
24. Machens A, Hoffmann F, Sekulla C, Dralle H. Importance of gender-specific calcitonin thresholds in
screening for occult sporadic medullary thyroid cancer. Endocr Relat Cancer 2009;16:1291-1298.
25. Borget I, De Pouvourville G, Schlumberger M. Editorial: Calcitonin determination in patients with
nodular thyroid disease. J Clin Endocrinol Metab 2007;92:425-427.

Calcitonin for detection of MTC
53
26. Cheung K, Roman SA, Wang TS, Walker HD, Sosa JA. Calcitonin measurement in the evaluation of
thyroid nodules in the United States: a cost-effectiveness and decision analysis. J Clin Endocrinol
Metab 2008;93:2173-2180.
27. d'Herbomez M, Caron P, Bauters C, et al. Reference range of serum calcitonin levels in humans:
influence of calcitonin assays, sex, age, and cigarette smoking. Eur J Endocrinol 2007;157:749-755.
28. Leboeuf R, Langlois MF, Martin M, Ahnadi CE, Fink GD. "Hook effect" in calcitonin immunoradiometric
assay in patients with metastatic medullary thyroid carcinoma: case report and review of the
literature. J Clin Endocrinol Metab 2006;91:361-364.
29. Bieglmayer C, Niederle B, Vierhapper H. Interference causes false high calcitonin levels with a
commercial assay. J Endocrinol Invest 2002;25:197.
30. Tommasi M, Brocchi A, Cappellini A, Raspanti S, Mannelli M. False serum calcitonin high levels using a
non-competitive two-site IRMA. J Endocrinol Invest 2001;24:356-360.
31. Preissner CM, Dodge LA, O'Kane DJ, Singh RJ, Grebe SK. Prevalence of heterophilic antibody
interference in eight automated tumor marker immunoassays. Clin Chem 2005;51:208-210.
32. Netzel BC, Grebe SK, Algeciras-Schimnich A. Usefulness of a thyroglobulin liquid chromatography-
tandem mass spectrometry assay for evaluation of suspected heterophile interference. Clin Chem
2014;60:1016-1018.
33. Zanelli JM, Gaines-Das RE, Corran P. Establishment of the second international standards for porcine
and human calcitonins: report of the international collaborative study. Acta Endocrinol (Copenh)
1993;128:443-450.
34. Kratzsch J, Petzold A, Raue F, et al. Basal and stimulated calcitonin and procalcitonin by various assays
in patients with and without medullary thyroid cancer. Clin Chem 2011;57:467-474.
35. Wells SA, J., Baylin SB, Linehan WM, Farrell RE, Cox EB, Cooper CW. Provocative agents and the
diagnosis of medullary carcinoma of the thyroid gland. 1978;188:139-141.
36. Samaan NA, Castillo S, Schultz PN, Khalil KG, Johnston DA. Serum calcitonin after pentagastrin
stimulation in patients with bronchogenic and breast cancer compared to that in patients with
medullary thyroid carcinoma. 1980;51:237-241.
37. Ewers HR, Brouwers HP, Merguet P, Hengstebeck W. Side effects after stimulation of gastric secretion
with pentagastrin (author's transl). Med Klin 1976;71:19-23.
38. Colombo C, Verga U, Mian C, et al. Comparison of calcium and pentagastrin tests for the diagnosis and
follow-up of medullary thyroid cancer. J Clin Endocrinol Metab 2012;97:905-913.
39. Doyle P, Duren C, Nerlich K, et al. Potency and Tolerance of Calcitonin Stimulation with High-Dose
Calcium Versus Pentagastrin in Normal Adults. 2009;94:2970-2974.
40. Kudo T, Miyauchi A, Ito Y, et al. Serum calcitonin levels with calcium loading tests before and after
total thyroidectomy in patients with thyroid diseases other than medullary thyroid carcinoma.
2011;58:217-221.
41. Bugalho MJ, Santos JR, Sobrinho L. Preoperative diagnosis of medullary thyroid carcinoma: fine needle
aspiration cytology as compared with serum calcitonin measurement. J Surg Oncol 2005;91:56-60.
42. Chang TC, Wu SL, Hsiao YL. Medullary thyroid carcinoma: pitfalls in diagnosis by fine needle aspiration
cytology and relationship of cytomorphology to RET proto-oncogene mutations. Acta Cytol
2005;49:477-482.
43. Papaparaskeva K, Nagel H, Droese M. Cytologic diagnosis of medullary carcinoma of the thyroid gland.
Diagn Cytopathol 2000;22:351-358.
44. Abraham D, Gault PM, Hunt J, Bentz J. Calcitonin estimation in neck lymph node fine-needle aspirate
fluid prevents misinterpretation of cytology in patients with metastatic medullary thyroid cancer.
Thyroid 2009;19:1015-1016.
45. Boi F, Maurelli I, Pinna G, et al. Calcitonin measurement in wash-out fluid from fine needle aspiration
of neck masses in patients with primary and metastatic medullary thyroid carcinoma. J Clin Endocrinol
Metab 2007;92:2115-2118.
46. Kudo T, Miyauchi A, Ito Y, Takamura Y, Amino N, Hirokawa M. Diagnosis of medullary thyroid
carcinoma by calcitonin measurement in fine-needle aspiration biopsy specimens. Thyroid
2007;17:635-638.
47. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and
meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS
Med 2009;6:e1000100.
48. Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of
diagnostic accuracy studies. Ann Intern Med 2011;155:529-536.

Chapter 3
54
49. Macaskill P. Empirical Bayes estimates generated in a hierarchical summary ROC analysis agreed
closely with those of a full Bayesian analysis. J Clin Epidemiol 2004;57:925-932.
50. Rieu M, Lame MC, Richard A, et al. Prevalence of sporadic medullary thyroid carcinoma: the
importance of routine measurement of serum calcitonin in the diagnostic evaluation of thyroid
nodules. Clin Endocrinol (Oxf) 1995;42:453-460.
51. Ozgen AG, Hamulu F, Bayraktar F, et al. Evaluation of routine basal serum calcitonin measurement for
early diagnosis of medullary thyroid carcinoma in seven hundred seventy-three patients with nodular
goiter. Thyroid 1999;9:579-582.
52. Hahm JR, Lee MS, Min YK, et al. Routine measurement of serum calcitonin is useful for early detection
of medullary thyroid carcinoma in patients with nodular thyroid diseases. Thyroid 2001;11:73-80.
53. Hatzl-Griesenhofer M, Pichler R, Bogner S, et al. Results of calcitonin screening in a Central Upper
Austrian Region. J Endocr Genet 2002;3:75-85.
54. Elisei R, Bottici V, Luchetti F, et al. Impact of routine measurement of serum calcitonin on the
diagnosis and outcome of medullary thyroid cancer: experience in 10,864 patients with nodular
thyroid disorders. J Clin Endocrinol Metab 2004;89:163-168.
55. Karanikas G, Moameni A, Poetzi C, et al. Frequency and relevance of elevated calcitonin levels in
patients with neoplastic and nonneoplastic thyroid disease and in healthy subjects. J Clin Endocrinol
Metab 2004;89:515-519.
56. Vierhapper H, Niederle B, Bieglmayer C, Kaserer K, Baumgartner-Parzer S. Early diagnosis and curative
therapy of medullary thyroid carcinoma by routine measurement of serum calcitonin in patients with
thyroid disorders. Thyroid 2005;15:1267-1272.
57. Schuetz M, Beheshti M, Oezer S, et al. Calcitonin measurements for early detection of medullary
thyroid carcinoma or its premalignant conditions in Hashimoto's thyroiditis. Anticancer Res
2006;26:723-727.
58. Papi G, Corsello SM, Cioni K, et al. Value of routine measurement of serum calcitonin concentrations in
patients with nodular thyroid disease: A multicenter study. J Endocrinol Invest 2006;29:427-437.
59. Costante G, Meringolo D, Durante C, et al. Predictive value of serum calcitonin levels for preoperative
diagnosis of medullary thyroid carcinoma in a cohort of 5817 consecutive patients with thyroid
nodules. J Clin Endocrinol Metab 2007;92:450-455.
60. Rink T, Truong PN, Schroth HJ, Diener J, Zimny M, Grunwald F. Calculation and validation of a plasma
calcitonin limit for early detection of medullary thyroid carcinoma in nodular thyroid disease. Thyroid
2009;19:327-332.
61. Hasselgren M, Hegedus L, Godballe C, Bonnema SJ. Benefit of measuring basal serum calcitonin to
detect medullary thyroid carcinoma in a Danish population with a high prevalence of thyroid nodules.
Head Neck 2010;32:612-618.
62. Herrmann BL, Schmid KW, Goerges R, Kemen M, Mann K. Calcitonin screening and pentagastrin
testing: predictive value for the diagnosis of medullary carcinoma in nodular thyroid disease. Eur J
Endocrinol 2010;162:1141-1145.
63. Giovanella L, Verburg FA, Imperiali M, Valabrega S, Trimboli P, Ceriani L. Comparison of serum
calcitonin and procalcitonin in detecting medullary thyroid carcinoma among patients with thyroid
nodules. Clin Chem Lab Med 2012:1-5.
64. Schneider C, Kobe C, Schmidt M, et al. Calcitonin screening in patients with thyroid nodules. Diagnostic
value. Nuklearmedizin 2012;51:228-233.
65. Grani G, Nesca A, Del Sordo M, et al. Interpretation of serum calcitonin in patients with chronic
autoimmune thyroiditis. Endocr Relat Cancer 2012;19:345-349.
66. Lepage M, Bounaud MP, Breton I, et al. Calcitonin Determination in Assessment of Cold Thyroid-
Nodules - Prospective-Study on 195 Patients. Revue De Medecine Interne 1992;13:S364-S364.
67. Mariss P, Kammeier A, Thermann M, Emrich D, Raute-Kreinsen U. Calcitonine screening in patients
with nodular goiter for detection of medullary thyroid cancer. Eur J Nucl Med 2001;28:1043-1043.
68. Mariss P, Kammeier A, Thermann M, Emrich D, Raute-Kreinsen U. Untersuchungen des
serumcalcitonin zur diagnostik medullärer schilddrüsenkarzinome bei patienten mit struma nodosa.
Nuklearmedizin 2001;40:A60-A60.
69. Lipp RW, Grohs S, Mader J, Obermaier-Pitsch B, Pieber T, Piswanger-Soelkner J. Routine calcitonin
screening for medullary thyroid cancer detection in an Austrian population. Eur J Nucl Med Mol
Imaging 2011;38:S100.

Calcitonin for detection of MTC
55
70. Zaplatnikov K, Soukhov V. Nuclear Medicine methods and prognostic significance of calcitonin and
pentagastrin test at diagnosis of sporadic MTC. European Journal of Nuclear Medicine and Molecular
Imaging 2012;39:S594-S594.
71. Marui S, Danilovic DS, Camargo RY, Lando VS, Knobel M, Batista MC. The utility of serum calcitonin
measurement in thyroid nodule evaluation: Experience of a single university hospital in Sao Paulo,
Brazil. Endocr Rev 2012;33.
72. Henry JF, Denizot A, Niccoli P, Gramatica L, Conte-Devolx B, De Micco C. Preoperative diagnosis of
sporadic medullary thyroid carcinoma. Interest of routine measurement of serum calcitonin. Lyon Chir
1995;91:467-472.
73. Henry JF, Denizot A, Puccini M, Niccoli P, Conte-Devolx B, Fie Micco C. Early diagnosis of sporadic
medullary cancer of the thyroid: Contribution of routine calcitonin assay. Presse Med 1996;25:1583-
1588.
74. Lopez-Guzman A, Escola CA, Andia VM, Arranz A, Garcia B, Del Campo AG. Routine calcitonin
measurement in nodular thyroid disease. Endocrinol Nutr 2002;49:222-226.
75. Shong YK, Choi CS, Park HY, Cho BY. Clinical Significance of Routine Measurement of Serum Calcitonin
in Korean Patients with Thyroid Nodules as a Screening test of Sporadic Thyroid Medullary Carcinoma.
Journal of Korean Society of Endocrinology 1996;11:11-17.
76. Pacini F, Fontanelli M, Fugazzola L, et al. Routine measurement of serum calcitonin in nodular thyroid
diseases allows the preoperative diagnosis of unsuspected sporadic medullary thyroid carcinoma. J
Clin Endocrinol Metab 1994;78:826-829.
77. Vierhapper H, Raber W, Bieglmayer C, Kaserer K, Weinhausl A, Niederle B. Routine measurement of
plasma calcitonin in nodular thyroid diseases. J Clin Endocrinol Metab 1997;82:1589-1593.
78. Kaserer K, Scheuba C, Neuhold N, et al. C-cell hyperplasia and medullary thyroid carcinoma in patients
routinely screened for serum calcitonin. Am J Surg Pathol 1998;22:722-728.
79. Iacobone M, Niccoli-Sire P, Sebag F, De Micco C, Henry JF. Can sporadic medullary thyroid carcinoma
be biochemically predicted? Prospective analysis of 66 operated patients with elevated serum
calcitonin levels. World J Surg 2002;26:886-890.
80. Mirallie E, Iacobone M, Sebag F, Henry JF. Results of surgical treatment of sporadic medullary thyroid
carcinoma following routine measurement of serum calcitonin. Eur J Surg Oncol 2004;30:790-795.
81. Niccoli P, Wion-Barbot N, Caron P, et al. Interest of routine measurement of serum calcitonin: study in
a large series of thyroidectomized patients. The French Medullary Study Group. J Clin Endocrinol
Metab 1997;82:338-341.
82. Gibelin H, Essique D, Jones C, Levillain P, Marechaud R, Kraimps JL. Increased calcitonin level in thyroid
nodules without medullary carcinoma. Br J Surg 2005;92:574-578.
83. Chambon G, Alovisetti C, Idoux-Louche C, et al. The use of preoperative routine measurement of basal
serum thyrocalcitonin in candidates for thyroidectomy due to nodular thyroid disorders: results from
2733 consecutive patients. J Clin Endocrinol Metab 2011;96:75-81.
84. Papi G, Rossi G, Corsello SM, et al. Nodular disease and parafollicular C-cell distribution: results from a
prospective and retrospective clinico-pathological study on the thyroid isthmus. 2010;162:137-143.
85. Frank-Raue K, Machens A, Leidig-Bruckner G, et al. Prevalence and clinical spectrum of nonsecretory
medullary thyroid carcinoma in a series of 839 patients with sporadic medullary thyroid carcinoma.
Thyroid 2013;23:294-300.
86. Daniels GH. Screening for medullary thyroid carcinoma with serum calcitonin measurements in
patients with thyroid nodules in the United States and Canada. Thyroid 2011;21:1199-1207.
87. Costante G, Durante C, Francis Z, Schlumberger M, Filetti S. Determination of calcitonin levels in C-cell
disease: clinical interest and potential pitfalls. Nat Clin Pract Endocrinol Metab 2009;5:35-44.
88. Valle LA, Kloos RT. The prevalence of occult medullary thyroid carcinoma at autopsy. J Clin Endocrinol
Metab 2011;96:E109-E113.
89. Karga H, Giagourta I, Papaioannou G, et al. Changes in risk factors and Tumor Node Metastasis stage
of sporadic medullary thyroid carcinoma over 41 years, before and after the routine measurements of
serum calcitonin. Metabolism 2010.
90. Alevizaki M, Saltiki K, Rentziou G, et al. Medullary thyroid carcinoma: the influence of policy changing
in clinical characteristics and disease progression. Eur J Endocrinol 2012;167:799-808.

56

Chapter 4
Fewer cancer reoperations for medullary thyroid
cancer after initial surgery according to ATA guidelines
Hans H.G. Verbeek, Johannes A.A. Meijer, Wouter T. Zandee, Kelvin H. Kramp
Wim J. Sluiter, Johannes W. Smit, Job Kievit, Thera P. Links, John T.M. Plukker
Annals of Surgical Oncology 2014 [Epub ahead of print]

Chapter 4
58
Abstract
Introduction Surgery is still the only curative treatment for medullary thyroid cancer (MTC).
We evaluated clinical outcome in patients with locoregional MTC with regard to adequacy of
treatment following ATA guidelines and number of sessions to first intended curative surgery
in different hospitals.
Methods We reviewed all records of MTC patients (n=184) treated between 1980 and 2010
in two tertiary referral centres in the Netherlands. Symptomatic MTC (palpable tumour or
suspicious lymphadenopathy) patients without distant metastasis were included (n=86).
Patients were compared with regard to adequacy of surgery according to ATA
recommendations, tumour characteristics, number of local cancer reoperations, biochemical
cure, clinical disease free survival (DFS), overall survival (OS) and complications.
Results Adherence to ATA guidelines resulted in fewer cancer-related reoperations (0.24 vs.
0.60; p=0.027) and more biochemical cure (40.9% vs. 20%; p=0.038). Surgery according to
ATA-guidelines on patients treated in referral centres was significantly more often adequate.
(59.2% vs. 26.7%; p=0.026). Tumour size and LN+ were the most important predictors for
clinical recurrence (relative risk: RR 4.1 (size >40 mm); 4.1 (LN+) and death (RR 4.2 (size
>40 mm); 8.1 (LN+).
Conclusions ATA-compliant surgery resulted in fewer local reoperations and more
biochemical cure. Patients in referral centres more often underwent adequate surgery
according to ATA-guidelines. Size and LN+ were the most important predictors for DFS and
OS.

Fewer reoperations after ATA compliant surgery
59
Introduction
At present, surgery offers the only possibility of cure for medullary thyroid carcinoma (MTC).
The American Thyroid Association (ATA) guidelines recommend total thyroidectomy and
bilateral lymph node dissection (LND) of the central compartment (level VI) as initial
treatment.1 In case of regional node involvement, lateral compartment LND (level II–V)
should be performed. Consensus with regard to indication, timing and extent (ipsi- or
bilateral) of the lateral LND is lacking.2-4 Adherence to ATA guidelines may improve disease
specific survival (DSS) in patients with locoregional disease.5 However, other studies reported
that extent of cervical lymphadenectomy, although important for staging and locoregional
control, did not increase biochemical cure or survival.6,7
Besides LND extent, both surgeons’ experience and the volume of the centre are important
factors, as they are associated with complication rates and length of hospital stay.8 However,
many MTC patients are still treated primarily in low-volume hospitals, and are at risk of
receiving inadequate initial surgical management.9,10
Patients initially treated in an inadequate manner are usually considered candidates for
completion surgery. One third of these patients may benefit from meticulous surgical
eradication resulting in long-term disease free survival (DFS).11 However, reoperations are
technically challenging with potentially increased morbidity, including hypoparathyroidism
and recurrent nerve damage.11-13
The first aim of this retrospective cohort study was to evaluate ATA recommendations for
primary surgical treatment by comparing clinical outcomes (i.e. number of reoperations,
biochemical cure, survival and complications) after the first curative intended surgical
resection in patients treated with ATA-compliant surgery versus patients treated with non-
ATA compliant surgery (A). Secondly, we investigated whether clinical outcome was
influenced by a one-step (versus two step) intended curative surgical procedure (B) or by the
location of initial curative surgery (experienced centre versus hospital) (C). Finally, we
evaluated the influence of patient and tumour characteristics on clinical outcome.

Chapter 4
60
Materials and methods
Patients and tumour characteristics
The records of all 184 MTC patients treated between 1980 and 2010 in two major tertiary
referral centres in the Netherlands, the University Medical Centre in Groningen (UMCG) and
the Leiden University Medical Centre (LUMC), were reviewed retrospectively. Inclusion
criteria were: histologically proven symptomatic MTC at presentation (palpable tumour
and/or suspicious lymph nodes), available required data, treatment with curative intent and
clinical absence of distant metastases upon diagnosis and within 6 months after initial
intended curative surgery. Sixty-six patients did not meet the above criteria and were
excluded, as were 32 patients with hereditary MTC who had a preventive thyroidectomy
based only on mutation analysis or increased calcitonin levels. Eventually 86 patients were
included for final analyses (Table 1).
Table 1 Patient and tumour related characteristics
Characteristic N (%)
Sex
Female
Male
41 (47.7)
45 (52.3)
Type
Sporadic
Hereditary
60 (69.8)
26 (30.2)
Age (y)
Median
Range
46.6
9 - 84
Tumour size (cm)
<2
2-4
>4
Unknown
37 (43.0)
29 (33.7)
18 (20.9)
2 (2.3)
Lymph node involvement
N0
N1a
N1b
N1x*
26 (30.2)
13 (15.1)
46 (53.5)
1 (1.2)
Stage (TNM 7)
Stage I
Stage II
Stage III
Stage IVa
Unknown
11 (12.8)
13 (15.1)
15 (17.4)
45 (52.3)
2 (2.4)
Number of patients (N) with percentages in parentheses (%)
unless otherwise indicated. *Not known if N1a or N1b.

Fewer reoperations after ATA compliant surgery
61
Patients were categorized as; (A) those in whom initial intended curative surgery was
performed in adherence to current ATA guidelines with adequate (group A1) or inadequate
surgery (group A2); (B) those in whom intended curative surgery was performed in a one-
step (group B1) or two-step (group B2) procedure and (C) those whose surgery was
performed in a centre (UMCG/LUMC; group C1/C3) or a non-centre (low-volume) hospital
(group C2) (Figure 1).
Figure 1 Distribution of patients (total 86) with adequate and inadequate surgery (group A) in surgery with
curative intent in one or two sessions (group B) and surgery in a centre or non-centre hospital (group C).
*According to American Thyroid Association guidelines.
Review of surgery and pathology reports
All surgical and pathology reports were independently reviewed and scored by at least three
of four reviewers. Differences in scoring outcome were solved by consensus. First the type of
thyroidectomy (diagnostic or therapeutic) was scored and whether it was a hemi-, subtotal or
total thyroidectomy. Secondly, the types of LND were categorized as lymphadenectomy in
the central (level VI) or lateral region (levels II-VI), and in a unilateral or bilateral neck

Chapter 4
62
dissection. The LND was scored as complete or partial(including lymph -node picking), using
anatomical structures and borders defined by the American Head and Neck Society and
American Academy of Otolaryngology-Head and Neck Surgery.14,15 We evaluated mean and
total numbers of resected nodal categories and tumour positive lymph nodes (LN+). In all
patients the time and location (centre vs. non-centre hospital) of first surgery with curative
intent was documented, and whether it was performed in one or two sessions.
Using ATA guidelines, the first intended curative surgery was scored as being carried out
adequately or inadequately. Adequate surgery consisted of total thyroidectomy with complete
central compartment dissection (level VI) combined with a uni- or bilateral LND, levels II–V,
when there was a preoperative suspicion of metastatic lateral lymph nodes during clinical or
radiological examination.1
Evaluation of putative selection bias
To exclude putative selection bias of non-referred patients we compared data of one referral
centre (UMCG) with data from the national cancer registry (data available during last
decade). This registry reported 50 MTC patients, which was equal to the number treated in the
centre; this indicated that in a non-centre hospital there was no significant number of MTC
patients treated successfully, without later referral to the tertiary centre.
Follow-up and outcome
Follow-up consisted of regular calcitonin and carcinoembryonic antigen (CEA)
measurements, and when these were markedly elevated further evaluation was carried out
with morphological imaging (US, CT, or MRI), functional imaging (PET) or US guided fine
needle aspiration biopsy (FNAB). Biochemical cure was defined as normalization of
calcitonin and CEA levels after the first surgical procedure with curative intent, and before
any further intervention. Recurrence was defined as any lesion with positive cytology or
suspected lesion upon imaging with significantly increased tumour markers. Indeterminate
lesions appearing in imaging without confirmation by other imaging methods or acquired
cytology and/or histology during follow-up, were considered tumour negative. The time
between the first curative intended surgery and clinical recurrence or death was used to define
disease free survival (DFS), disease specific survival (DSS) and overall survival (OS). All
cancer reoperations and complications after first surgery with curative intent were
documented. Recurrent laryngeal nerve palsy diagnosed by indirect laryngoscopy was

Fewer reoperations after ATA compliant surgery
63
considered permanent if persisting >6 months. Hypoparathyroidism was considered
permanent if calcium supplementation was necessary >6 months.
Statistical analysis
For statistical analysis we used IBM SPSS statistics 20. For comparison of continuous
normally distributed variables we used Student’s t test or One way ANOVA and for
continuous variables not normally distributed we used the Mann-Whitney U test or Kruskall
Wallis test. The Chi-square test or Fisher exact test was applied for categorical data. For
survival analysis we used a standardized survival model as described earlier.16 The
significance level was p <0.05, 2-sided.
Results
Distribution of patients and tumour characteristics between different groups
An overview of all 86 included patients according to adequacy of first curative intended
surgery (A), number of required sessions (B) and institute (C) is given in Figure 1. Correlated
patient and tumour characteristics are shown in Table 2.
Analysis A: Adequacy of surgery according to ATA guidelines
Surgical procedures according to ATA guidelines were initially adequate in 46 patients
(Figure 1: group A1) and inadequate in 40 patients (Figure 1; group A2; Supplementary Table
1). Adequately treated patients had significant more LN’s examined (24.7 vs. 13.7; p=0.016),
but the number of tumour positive LN’s was almost equal (9.6 vs. 7.9; Table 2).
Analysis B: Number of performed sessions to obtain intended curative surgery
Intended curative surgery was obtained in one session in 66 patients (Figure 1; group B1),
while in 20 patients a two-step procedure was necessary to obtain intended curative surgery
(Figure 1; group B2). Supplementary Table 2 lists the initial procedures in patients requiring
two-step surgery. Patients treated in one-step had significantly more LN involvement (77.3%
vs. 45%, p=0.006) and stage IVa disease (60% vs. 31.6%, p=0.003) (Table 2).

Chapter 4
64
Analysis C: Institute of first intended curative surgery
Sixty-four patients received all surgical procedures in a tertiary referral centre (Figure 1;
group C1). Fifteen of the other 22 patients were treated with curative intent in a non-centre
hospital (group C2). Seven patients received complementary intended curative surgery in a
centre after undergoing a diagnostic hemithyroidectomy in a non-centre hospital (group C3).
Adequate surgery was more often performed in centres (59.2%; 42/71), as compared with
non-centre hospitals (4/15) (relative risk, RR=2.22; p=0.026). Two-step surgery was
significantly more often needed for patients treated initially in non-centre hospitals (54.5%;
12/22) as compared to patients treated in a centre (8/64; p<0.001) (Table 2).
Clinical outcome with regard to ATA-compliant or ATA-non-compliant surgery
(Group A)
Cancer reoperations
After surgery with curative intent, 32 patients underwent a cancer reoperation; 29 of the latter
had histological confirmed MTC. Local cancer reoperations (n=34) were performed on 25
patients. Three patients had four distant reoperations and one patient had a local and two
distant reoperations. The median interval between initial curative surgery and cancer
reoperation was 33 (range 4–331) months. The mean number of local reoperations was
significantly lower in adequately versus inadequately treated patients (total re-operations 11
vs. 24; average 0.24 vs. 0.60, p=0.027; Table 2).
Biochemical cure
Biochemical cure after first intended curative surgery occurred in 31 patients (36%). At the
last follow-up 26 patients (30.9%) had biochemical cure and in adequately treated patients it
was significantly higher (40.9% vs. 20 %, p=0.038; Table 2).
Clinical recurrent disease and survival
During follow-up, 38 patients developed clinical recurrent disease (16 only local recurrences,
7 only distant metastasis and 15 both local and distant). Adequacy of intended curative
surgery did not predict clinical DFS, OS or DSS (Table 3).

Fewer reoperations after ATA compliant surgery
65
Ta
ble
2 P
ati
en
t ch
ara
cte
rist
ics,
tu
mo
ur
cha
ract
eri
stic
s, m
ea
n n
um
be
r o
f in
vest
iga
ted
an
d p
osi
tive
lym
ph
no
de
s† a
nd
clin
ica
l
ou
tco
me
in d
iffe
ren
t p
ati
en
t g
rou
ps
G
rou
p A
Gro
up
B
G
rou
p C
A
de
qu
ate
#
Ina
de
qu
ate
#
P
O
ne
se
ssio
n
Tw
o s
ess
ion
s P
Ce
ntr
e‡
No
n-c
en
tre
P
Pa
tie
nt
cha
ract
eri
stic
s
F
em
ale
4
5.7
%
50
.0%
0
.68
7
4
3.9
%
60
%
0.2
08
40
.8%
8
0.0
%
0.0
06
S
po
rad
ic M
TC
6
9.6
%
70
.0%
0
.96
5
6
5.2
%
85
.0%
0
.09
0
6
4.8
%
93
.3%
0
.03
2
A
ge
(y
rs,
me
an
) 4
9.0
4
5.0
0
.27
8
4
6.6
4
8.9
0
.59
2
4
7.3
4
6.7
0
.90
6
Tu
mo
ur
cha
ract
eri
stic
s
T
um
ou
r si
ze >
40
mm
2
0 %
2
3.1
%
0.7
32
18
.8 %
3
0%
0
.35
1
1
8.8
%
33
.3%
0
.29
6
LN
in
vo
lve
me
nt
69
.5%
7
0%
0
.96
5
7
7.3
%
45
%
0.0
06
73
.2%
5
3.3
%
0.2
14
T
NM
sta
ge
4a
5
5.6
%
51
.3%
0
.69
5
6
0%
3
1.6
%
0.0
29
57
.9%
3
3.3
%
0.0
83
Nu
mb
er
of
lym
ph
no
de
s LN
n
LN
n
LN
n
LN
n
LN
n
LN
n
In
ve
stig
ate
d (
me
an
(n
))
24
.7 (
35
) 1
3.7
(2
9)
0.0
16
20
.7 (
50
) 1
6.3
(1
4)
0.4
36
21
.4 (
53
) 1
1.6
(1
1)
0.1
08
P
osi
tiv
e (
me
an
(n
))
9.6
(3
1)
7.9
(2
6)
0.5
52
9.4
(4
8)
6 (
9)
0.3
84
9 (
49
) 8
.1 (
8)
0.8
38
Cli
nic
al
ou
tco
me
R
eo
pe
rati
on
s (m
ea
n)
0.2
4
0.6
0
0.0
27
0.3
6
0.5
5
0.4
57
0.3
4
0.7
3
0.2
18
B
ioch
em
ica
l cu
re (
%)
40
.9%
2
0%
0
.03
8
2
8.1
%
40
%
0.3
16
29
%
40
%
0.4
03
† In
pts
(n
) w
ith
an
y fo
rm o
f ly
mp
h n
od
e d
isse
ctio
n (
incl
ud
ing
lym
ph
no
de
pic
kin
g).
#A
cco
rdin
g t
o A
me
rica
n T
hyr
oid
Ass
oci
ati
on
gu
ide
line
s. ‡
Incl
ud
ing
all
pa
tie
nts
wh
o h
ad
th
eir
cu
rati
ve in
ten
de
d s
urg
ery
in a
ce
ntr
e (
gro
up
C1
an
d C
3).

Chapter 4
66
Complications
Postoperative hypoparathyroidism (n=31: 36%), was not significant different between patients
treated adequately or inadequately (41.3% vs. 30%). Also, the postoperative recurrent nerve
palsy rate (n=10: 12.2%) was not significant different between the two groups (9.1% vs.
15.8%).
Table 3 Evaluation of risk factors for clinical disease free (DFS) and overall survival (OS)
Clinical DFS OS
Univariate Bivariate* Univariate Bivariate*
RR
(95% CI) P
RR
(95% CI) P
RR
(95% CI) P
RR
(95% CI) P
Surgery according to
ATA guidelines (yes)
1.06
(0.56 – 2.02)
0.84
0.65
(0.28 – 1.48)
0.30
Centre curative surgery
(non-centre)
1.18
(0.52 – 2.67)
0.69
0.45
(0.11 – 1.84)
0.26
Curative surgery in
one/two sessions (two)
0.82
(0.36 - 1.85)
0.63
0.57
(0.19 - 1.65)
0.30
Sex (female) 0.55
(0.29 – 1.05)
0.07
0.61
(0.32 – 1.17)
0.13
0.24
(0.09 – 0.65)
0.005
0.36
(0.12 – 1.03)
0.06
Type MTC (hereditary) 0.51
(0.25 – 1.04)
0.06
0.65
(0.32 – 1.33)
0.24
0.18
(0.03 – 1.05)
0.06
0.36
(0.05 – 2.43)
0.29
Tumour size (>40 mm) 4.1
(2.23 – 7.65)
7. 10-6
4.20
(1.87 – 9.44)
5. 10-4
LN involvement 4.1
(1.73 – 9.75)
0.001
3.18
(1.30 – 7.74)
0.01
8.08
(1.50 – 43.47)
0.015
4.39
(0.70 – 27.55)
0.11
TNM stage (4a) 2.9
(1.48 – 5.49)
0.002
2.41
(1.24 – 4.69)
0.01
6.80
(1.94 – 23.87)
0.003
4.75
(1.26 – 17.82)
0.02
*Corrected for tumour size. DFS: disease free survival. OS: overall survival. RR: relative risk. ATA: American
Thyroid Association. MTC: medullary thyroid carcinoma. LN: lymph node.
Clinical outcome with respect to number of sessions (Group B)
No difference was found in cancer reoperations (average 0.36 vs. 0.55), biochemical cure at
last follow-up (28.1% vs. 40.0%) and survival between patients treated by one-step versus
two-step intended curative surgery (Table 2 and 3) After a two-step surgery patients had
significantly less postoperative hypoparathyroidism (15 % vs. 42.4%, p=0.025), also after
correction for LN+ and TNM stage. No significant difference existed in recurrent nerve palsy
(15.9% vs. 0%).

Fewer reoperations after ATA compliant surgery
67
Clinical outcome with respect to centre of first curative intended surgery (Group C)
Between patients treated in a centre as opposed to a non-centre, the clinical outcome did not
differ. There were no differences in cancer reoperations (mean 0.34 vs. 0.73) and biochemical
cure at last follow-up (29.0% vs. 40.0 %; Table 2), nor on clinical DFS, DSS and OS (Table
3). Hypoparathyroidism and recurrent nerve palsy occurred in 35.2% vs. 40% (p=NS) and
10.5% vs. 20% (p=NS).
Clinical outcome with respect to patient and tumour characteristics
Patient and tumour characteristics did not affect the number of reoperations. Biochemical cure
at last follow-up was significantly lower in patients with LN involvement and stage IVa
disease (19.0% vs. 57.7%, p<0.001 and 16.2% vs. 48.7%, p=0.001). Most tumour-related
factors were significant predictors for clinical recurrence (Table 3). After correction for
tumour size as the most significant predictor, LN involvement and TNM stage IVa remained
significant risk factors for clinically recurrent disease
Favourable significant predictors for OS and DSS were female gender, small tumour size
(<40 mm), no LN involvement and TNM stage I-III. With correction for tumour size, only the
TNM stage remained a significant predictor. After correction for TNM stage, tumour size was
the most significant factor for survival, with a RR of 3.92 (p=0.002).
Patients with familial MTC more often had postoperative hypoparathyroidism (53.8% vs.
28.3%, p=0.024) while recurrent nerve palsy more frequently occurred in sporadic MTC
(17.9% vs 0% in familial MTC, p=0.026) and stage IVa disease (19.5% vs 2.6% in stage III
disease, p=0.029).

Chapter 4
68
Discussion
In this study, we emphasize the importance of adequate initial surgery to optimize cure and
locoregional control of MTC. Patients treated adequately according to current ATA guidelines
had significantly fewer local cancer reoperations and more frequent biochemical cure during
follow-up after primary surgery with curative intent. Despite significantly more advanced
disease in patients treated with one-step surgery with curative intent, no difference was
observed in the number of local cancer reoperations or biochemical cure in these patients as
compared to patients requiring a two-step surgery. Tumour characteristics were the most
important predictors for biochemical cure, clinical DFS, DSS and OS.
Important issues in the surgical treatment of MTC patients are the indication and extent of
lateral LND. Because of lack of evidence, leading experts and guidelines advocate different
surgical approaches.1-4,17 For symptomatic MTC patients with limited local disease the ATA
recommends lateral LND if there is suspicion of lateral LN involvement, while the BTA
guidelines advocate bilateral selective LND in pT2-4 tumours or palpable lymph nodes in
central or lateral compartment.1,17 Although systematic LND has improved biochemical cure,
it is still difficult to obtain cure in patients with extensive lymph node involvement.18-22
Indeed, not the extent of operation but rather the baseline tumour characteristics such as
preoperative calcitonin and TNM stage are independent predictors for biochemical cure.7,21
The survival benefits of extensive LND remains contradictory.18,23 Although we did not
specifically evaluate the extent of LND’s, a significant survival benefit with respect to ATA-
compliant surgery was not observed, whereas the latter resulted more often in biochemical
cure. Panigrahi et al. recorded a significantly shorter DSS in patients with regional nodal
disease not treated according to ATA recommendations, which is in contrast to the results of
our study.5 However, the authors included a relative large proportion of patients (16%) with a
subtotal or no thyroidectomy. Moreover, they categorized patients receiving an incomplete
LND as having been treated according to the guidelines. Although our study is more
representative for current practice because of our strict definition of adequate surgery,
comparison between both studies remains difficult.
While results on cure and survival remain contradictory, extensive LND is advocated for
preventing locoregional recurrences, reoperations and future complications.18,23,24 We found
fewer cancer reoperations and more biochemical cure in patients adequately treated according
to current ATA guidelines, a fact which is beneficial for MTC patients. We showed a higher

Fewer reoperations after ATA compliant surgery
69
rate of ATA-compliant surgery in referral centres, underscoring earlier data dealing with high
volume hospitals and surgery for thyroid cancer.10
Preoperative work-up by experienced surgeons is advocated, as preoperative diagnosis is
still difficult to establish. An illustration in this study was the performance of a diagnostic
hemithyroidectomy in a substantial number of patients. Despite less advanced disease in these
patients the number of cancer reoperations was relatively high (after second completion
surgery) and biochemical cure was not more frequent. The avoidance of a diagnostic
hemithyroidectomy might have resulted in a more radical initial procedure, and probably with
fewer reoperations. Therefore an adequate diagnosis before initial surgery is crucial in order
to reach locoregional control.25-27
Based on the retrospective character of this study there is a possibility of selection bias.
Other limitations include the relatively low number of patients and possible understaging, due
to limited sensitivity of imaging techniques in the early study period and in patients
inadequately treated.
Conclusion
This study shows the importance of adequate surgery according to ATA guidelines in order to
obtain biochemical cure and regional disease control, leading to fewer cancer reoperations.
This was achieved even in the presence of advanced disease in which size and LN+
commonly predict outcome. Our results indicate a higher rate of adequate surgery in tertiary
referral centres, and support centralized treatment for all patients with confirmed or suspected
MTC.

Chapter 4
70
References
1. Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer: management guidelines of the American
Thyroid Association. Thyroid 2009;19:565-612.
2. Leboulleux S, Baudin E, Travagli JP, Schlumberger M. Medullary thyroid carcinoma. Clin Endocrinol
(Oxf) 2004;61:299-310.
3. Machens A, Dralle H. Biomarker-based risk stratification for previously untreated medullary thyroid
cancer. J Clin Endocrinol Metab 2010;95:2655-2663.
4. Moley JF. Medullary thyroid carcinoma: management of lymph node metastases. J Natl Compr Canc
Netw 2010;8:549-556.
5. Panigrahi B, Roman SA, Sosa JA. Medullary thyroid cancer: are practice patterns in the United States
discordant from American Thyroid Association guidelines? Ann Surg Oncol 2010;17:1490-1498.
6. Kandil E, Gilson MM, Alabbas HH, Tufaro AP, Dackiw A, Tufano RP. Survival implications of cervical
lymphadenectomy in patients with medullary thyroid cancer. Ann Surg Oncol 2011;18:1028-1034.
7. Yip DT, Hassan M, Pazaitou-Panayiotou K, et al. Preoperative basal calcitonin and tumor stage
correlate with postoperative calcitonin normalization in patients undergoing initial surgical
management of medullary thyroid carcinoma. Surgery 2011;150:1168-1177.
8. Sosa JA, Bowman HM, Tielsch JM, Powe NR, Gordon TA, Udelsman R. The importance of surgeon
experience for clinical and economic outcomes from thyroidectomy. Ann Surg 1998;228:320-330.
9. Kebebew E, Greenspan FS, Clark OH, Woeber KA, Grunwell J. Extent of disease and practice patterns
for medullary thyroid cancer. J Am Coll Surg 2005;200:890-896.
10. Lifante JC, Duclos A, Couray-Targe S, Colin C, Peix JL, Schott AM. Hospital volume influences the choice
of operation for thyroid cancer. Br J Surg 2009;96:1284-1288.
11. Fialkowski E, DeBenedetti M, Moley J. Long-term outcome of reoperations for medullary thyroid
carcinoma. World J Surg 2008;32:754-765.
12. Gimm O, Ukkat J, Dralle H. Determinative factors of biochemical cure after primary and reoperative
surgery for sporadic medullary thyroid carcinoma. World J Surg 1998;22:562-7; discussion 567-8.
13. Dralle H, Sekulla C, Haerting J, et al. Risk factors of paralysis and functional outcome after recurrent
laryngeal nerve monitoring in thyroid surgery. Surgery 2004;136:1310-1322.
14. Robbins KT, Clayman G, Levine PA, et al. Neck dissection classification update: revisions proposed by
the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck
Surgery. Arch Otolaryngol Head Neck Surg 2002;128:751-758.
15. Robbins KT, Shaha AR, Medina JE, et al. Consensus statement on the classification and terminology of
neck dissection. Arch Otolaryngol Head Neck Surg 2008;134:536-538.
16. de Groot JW, Plukker JT, Wolffenbuttel BH, Wiggers T, Sluiter WJ, Links TP. Determinants of life
expectancy in medullary thyroid cancer: age does not matter. Clin Endocrinol (Oxf) 2006;65:729-736.
17. British Thyroid Association, Royal College of Physicians. Guidelines for the management of thyroid
cancer. Report of the Thyroid Cancer Guidelines Update Group. London: Royal College of Physicians;
2007.
18. Dralle H, Damm I, Scheumann GF, et al. Compartment-oriented microdissection of regional lymph
nodes in medullary thyroid carcinoma. Surg Today 1994;24:112-121.
19. Modigliani E, Cohen R, Campos JM, et al. Prognostic factors for survival and for biochemical cure in
medullary thyroid carcinoma: results in 899 patients. The GETC Study Group. Groupe d'etude des
tumeurs a calcitonine. Clin Endocrinol (Oxf) 1998;48:265-273.
20. Kebebew E, Ituarte PH, Siperstein AE, Duh QY, Clark OH. Medullary thyroid carcinoma: clinical
characteristics, treatment, prognostic factors, and a comparison of staging systems. Cancer
2000;88:1139-1148.
21. Machens A, Gimm O, Ukkat J, Hinze R, Schneyer U, Dralle H. Improved prediction of calcitonin
normalization in medullary thyroid carcinoma patients by quantitative lymph node analysis. Cancer
2000;88:1909-1915.
22. Scollo C, Baudin E, Travagli JP, et al. Rationale for central and bilateral lymph node dissection in
sporadic and hereditary medullary thyroid cancer. J Clin Endocrinol Metab 2003;88:2070-2075.
23. Pelizzo MR, Boschin IM, Bernante P, et al. Natural history, diagnosis, treatment and outcome of
medullary thyroid cancer: 37 years experience on 157 patients. Eur J Surg Oncol 2007;33:493-497.

Fewer reoperations after ATA compliant surgery
71
24. Moley JF, Dilley WG, DeBenedetti MK. Improved results of cervical reoperation for medullary thyroid
carcinoma. Ann Surg 1997;225:734-40; discussion 740-3.
25. Niccoli P, Wion-Barbot N, Caron P, et al. Interest of routine measurement of serum calcitonin: study in
a large series of thyroidectomized patients. The French Medullary Study Group. J Clin Endocrinol
Metab 1997;82:338-341.
26. Elisei R. Routine serum calcitonin measurement in the evaluation of thyroid nodules. Best Pract Res
Clin Endocrinol Metab 2008;22:941-953.
27. Chambon G, Alovisetti C, Idoux-Louche C, et al. The use of preoperative routine measurement of basal
serum thyrocalcitonin in candidates for thyroidectomy due to nodular thyroid disorders: results from
2733 consecutive patients. J Clin Endocrinol Metab 2011;96:75-81.

Chapter 4
72
Supplementary data
Supplementary Table 1 First intended curative surgical procedure in
inadequately* treated patients (group A2, N = 40)
Type of treatment N
Incomplete thyroidectomy and no CCD 1
No CCD 8
Incomplete CCD
(only node picking or unilateral CCD) 22
Incomplete CCD and LND
(only node picking or unilateral CCD and incomplete
neck dissection not including all levels II-V)
5
Incomplete LND
(incomplete neck dissection not including all levels
II-V)
4
*According to ATA guidelines. CCD: Central compartment (level VI) dissection,
LND: Lymph node dissection.
Supplementary Table 2 First surgical procedure in pts requiring two sessions
(group B2, N = 20)
Type of surgery N
(Diagnostic) hemithyroidectomy 15
Hemithyroidectomy with unilateral LND 2
Total thyroidectomy 1
Total thyroidectomy with bilateral node picking 1
Total thyroidectomy with unilateral LND 1
LND: Lymph node dissection

Chapter 5
PET Imaging in thyroid carcinoma
Hans H.G. Verbeek, Ha T.H. Phan, Adrienne H. Brouwers
Klaas P. Koopmans, Thera P. Links
Methods of Cancer Diagnosis, Therapy and Prognosis. Vol. 7. Editor: M.A. Hayat. Springer
Sience + Business Media BV 2010.

Chapter 5
74
Introduction
Thyroid cancer is the most common endocrine malignancy. It is divided in several types with
papillary, folliculary, and Hürthecell cancer (also called differentiated thyroid cancer)
originating from the follicular epithelial cells as the most common types (>90%). Other types
are medullary thyroid carcinoma (a neuroendocrine tumour originating from the calcitonin
producing C-cells) (3%-10%) and anaplastic carcinoma (often a dedifferentiated form of the
other types) (2%-10%).1
There is a different treatment for each of these types of thyroid cancer. In differentiated
thyroid cancer the initial therapy is total thyroidectomy with or without lymph node
dissection, followed by adjuvant radioactive iodine therapy. Radioactive iodine therapy with 131I can be used successfully due to the active uptake of iodine in tumour cells of thyroid
origin. However, this property can be lost during dedifferentiation, which limits the use of this
therapy in anaplastic carcinoma. Medullary thyroid tumour cells show no iodine uptake at all
and curative options are therefore mainly limited to surgical resection of primary tumour and
metastases.2
The prognosis for differentiated thyroid cancer is good, with an average 10-years survival
between 80% and 95%. However, these tumours can dedifferentiate, which results in limited
therapeutic options, leading to a much poorer prognosis with a 5-years survival of 30%.
Medullary thyroid carcinoma has a 10-years survival of 20%-70%, and for anaplastic thyroid
carcinoma the median survival is 2-6 months.3-5
Imaging is especially important in determining the right therapeutic approach for patients
with differentiated and medullary thyroid carcinoma. Different imaging techniques are
available such as computed tomography (CT), magnetic resonance imaging (MRI),
conventional nuclear scintigraphy, positron emission tomography (PET), etc.. While MRI and
CT are imaging techniques which show morphologic structures, PET imaging depicts
pathophysiological processes and is described as functional imaging. The value of PET
imaging is emerging mainly in the follow-up of thyroid cancer. Several PET imaging
techniques are available for different types of thyroid cancer and these techniques and their
applications are discussed in this chapter.

PET imaging in thyroid carcinoma
75
Positron Emission Tomography
Positron emission tomography imaging is a technique used in nuclear medicine which is
based on the use of positron emitting isotopes in specific molecules which are relevant for
specific metabolic pathways. The PET technique yields a high resolution and the capability to
quantify the amount of radioactivity measured in a specific region. Positrons, emitted by an unstable atom nucleus, are the antiparticles of electrons and have
the same mass, but an opposite charge. Positrons are not detected by a PET camera, but
photons, which are formed when a positron fuses with an electron, are detected. This means
that the positron binds with an electron to form a positronium which annihilates. In this
annihilation process all the mass is converted into energy by which two photons are formed.
These photons, always carrying an energy of 511 keV, are emitted in opposite directions
under an angle of 180º and are detected by the PET camera.6
Radioisotopes used in PET imaging usually have a short half live, such as carbon-11(11C;
half-life (T½) 20 min), nitrogen-13 (13N; T½ 10 min), oxygen-15(15O; T½ 2 min) and fluorin-
18(18F; T½ 110 min). Positron emitting radionuclides are in most cases produced by
bombarding the target material with highly accelerated particles (deuterons or protons) using
a cyclotron and inducing a nuclear reaction. Centres which use isotopes with a very short half-
life, such as 15O, 13N, and 11C, need to have an on-site cyclotron. Other longer living isotopes
can be made elsewhere and then transported to the PET imaging facility.7
A cyclotron is a type of particle accelerator which accelerates charged particles using a
high-frequency, alternating voltage. A perpendicular magnetic field causes the particles to
assume a circular orbit so that they reencounter the accelerating voltage many times. When
the particles are accelerated fast enough they are bombarded on to specific atoms and
radionuclides are formed. These radionuclides are trapped and transported to the laboratory
where they can be processed for clinical use. The resulting end-products are called
radiotracers. The most commonly used tracers are precursors for metabolic pathways,
although many other tracer types exist. After preparation and careful quality monitoring,
tracers can be injected.
The imaging device used is the PET camera. Most PET cameras consist of a ring of special
detectors which are well suited for the detection of 511 keV gamma rays. Software registers
only simultaneously entering photonpairs on different detectors. This is called coincidence
detection. Coincidence detection removes the need for a lead collimator such that the

Chapter 5
76
sensitivity of the PET imaging system is much higher than for the conventional Anger camera
that is used in planar nuclear imaging or single photon emission computed tomography
(SPECT). Both the specific block detector structure and the absence of a collimator contribute
to a higher resolution as compared with SPECT. Another advantage of PET is that the amount
of radioactivity injected in the body can be quantitatively determined. PET is a non-invasive,
sensitive imaging tool for depicting of molecular and biochemical processes without changing
its physical properties.6
In contrast to radiologic imaging which shows the morphologic structures, nuclear
medicine techniques depict pathophysiological processes and are also described as functional
imaging methods. The imaging with PET is considered to be an useful diagnostic tool for the
detection of cancer, brain diseases, and coronary artery diseases.
Combined PET/CT
The combination of PET and CT scanning is a new promising imaging technique. The
integrated PET/CT scanner allows acquisition of CT and PET images in one session. The
combination of morphologic and functional imaging leads to more precise anatomical
localization of tumour lesions. The localization of tumour foci is important for initiating the
appropriate treatment such as surgery. Especially in patients with a negative radioiodine scan
where surgery is the only therapeutic option, the integrated PET/CT scan can be helpful in
guiding therapeutic management.
18Fluorine-fluorodeoxyglucose (
18F-FDG) PET
Mechanism
Fluorodeoxyglucose (FDG) is a glucose analogue and is used as a precursor for glucose
metabolism. In both benign and malignant tissue it enters the cell by the same glucose
transporters. However, the need for glucose in malignant cells is strongly increased because
these cells have a considerably less efficient energy metabolism.8 For example, the energy
production per molecule of glucose in malignant cells is decreased because anaerobic
glycolysis is strongly increased instead of the much more efficient energy production from the
citric acid cycle. This inefficient use of glucose is the basis for the preferential uptake of
glucose or an offered glucose analogue as FDG in malignant cells.

PET imaging in thyroid carcinoma
77
In the cell FDG is phosphorylated by a hexokinase enzyme into FDG-6 phosphate which,
in contrast to glucose-6-phospate, cannot be further metabolized. Therefore, the FDG-6-
phosphate does not leave the cell and becomes trapped intracellulary. The final quantity of
FDG-6-phosphate is proportional to the glycolytic rate of the cell. Besides the increased
glycolysis, it has been demonstrated that in malignant cells levels of transmembrane glucose
transporters (e.g., the GLUT-1 transporter) and possibly some hexokinase isoenzymes are also
increased, also resulting in increased FDG uptake.9
However, in all metabolically active tissues, such as brain cells, active muscles, and
activated macrophages, increased glucose metabolism leads to an increased FDG uptake. 18F-
FDG PET is, therefore, a marker for glucose metabolism in general. In most normal tissues
(e.g., liver, kidney, intestine, muscle and some tumour cells) the level of phosphate activity is
variable; nevertheless, FDG-6-phospate accumulation is lower than in malignant tissues. In
addition, some benign tissues require more glucose.10,11 So, the uptake mechanism of FDG
with irreversible trapping in malignant tissue is ideal for PET imaging and has been applied
widely in oncology. However, it is important to make a correct interpretation of these PET
images, for non-malignant tissue also has FDG uptake.
Scan method
Uptake of 18F-FDG occurs rapidly after administration and the amount taken up increases
with time. The most applied imaging moment is 60-90 min after tracer administration. The
reason is that the excretion of 18F-FDG via the kidneys reduces 18F-FDG in the blood, which
causes clearance of ‘background’ uptake and the decay of fluorin-18 (T½ 110 min). Generally
the patient preparation consists of an 18F-FDG injection in a fasting condition and after oral
prehydration. The injected dose varies between 2-8 MBq/kg.
Clinical application
Thyroid nodules
The value of 18F-FDG PET in the distinction between malignant and benign thyroid nodules
before surgery is unclear. Several studies reported that 18F-FDG PET is useful in the
preoperative evaluation of cytologicaly inconclusive nodules with a high negative predictive
value.12-14 De Geus-Oei et al. observed that the probability for thyroid cancer increased from
14% (pre-PET) to 32% (post-PET) in case the nodule was positive on 18F-FDG PET.12 In this
study 18F-FDG PET could reduce the number of futile hemithyroidectomies by 66%.

Chapter 5
78
A. 18F-FDG PET
B. CT-lung C. 18F-FDG PET/CT
Figure 1 These are the images of a 68-year old male known with follicular thyroid cancer. This patient showed
increased serum Tg level (14 ng/ml) suspected for recurrent or metastatic disease. Blind treatment with 131
I
was given followed by a post-treatment whole body scan (WBS) after 10 days which was negative. 18
F-FDG PET
(A) showed a focal lesion in the lower lobe of the left lung (arrow), confirmed by CT (B, arrow). Picture C
showed the fusion image of 18
F-FDG PET and CT for the lesion in the left lung (arrow).
However, recent studies by Kim et al. and Bogsrud et al., demonstrated that 18F-FDG PET is
not helpful in differentiating between malignant and benign nodules, and therefore has only
limited value in preoperative evaluation of indeterminate thyroid nodules.15,16
So, conflicting results are reported on the usefulness of 18F-FDG PET in the prediction of
malignancy in thyroid nodules in case of inconclusive cytology, and therefore further research
is needed. Meanwhile histopathological examination remains the gold standard.
Differentiated thyroid cancer (DTC): follow-up
More information is available regarding the value of 18F-FDG PET in the follow-up of thyroid
cancer such as the detection of recurrences or metastases, especially in patients with a
negative radioiodine scan or in patients who has lost the ability to accumulate iodine. A

PET imaging in thyroid carcinoma
79
complementary uptake of 18F-FDG and radioiodine can be present, which is known as the
‘flip-flop’ phenomenon and was first described by Joensuu and Ahonen.17 This phenomenon
might be explained by the degree of tissue differentiation. Well differentiated thyroid tissue
has the capability to take up iodine but is metabolically inactive while less differentiated
thyroid cancer tissue loses its capability to trap iodine and becomes metabolically more
active. This makes 18F-FDG PET scanning the method of choice for the detection of 131I
negative metastases of differentiated thyroid carcinoma.18
Performance of 18F-FDG PET during thyrotropin (TSH) stimulation improves the results in
comparison to the scanning during the euthyroid state (during thyroxin treatment) as was
shown by van Tol et al..19 In vitro studies have shown a stimulating effect of TSH on Glut 1
expression and glucose transport.20,21 This increase in glucose carriers results in a higher
uptake of glucose and also 18F-FDG in thyroid cancer cells, which improves the result of the
PET-scan. Stimulation with exogenous TSH (recombinant human(rh) TSH) also increases 18F-FDG uptake by differentiated thyroid cancer, and therefore more lesions can be detected
and tumour/background contrast is enhanced.22,23 The influence of rhTSH on the background
is not well-known, but there is evidence that rhTSH increases 18F-FDG uptake in the tumour
lesion itself.
Several studies have been performed to assess the value of 18F-FDG PET imaging in the
follow up of thyroid cancer. Hooft et al. performed a meta-analysis of studies that investigated
the role of 18F-FDG PET in patients with thyroid cancer after negative radioiodine
scintigraphy and elevated serum thyroglobulin.24 The diagnostic accuracy of these studies was
assessed. Observed sensitivity and specificity in these studies were ranging from 70%-95%
and 77%-100%, respectively. Furthermore, they observed that there are methodological
problems in these studies such as small sample size, validity of reference tests, and short
follow-up. Nonetheless, 18F-FDG PET is now considered a valuable diagnostic imaging tool
in the follow-up of 131I-negative patients for the detection of recurrences or metastases.
However, it is not known whether PET is superior to bone scintigraphy in the detection of
bone metastases in thyroid cancer. Comparative studies of bone scans and 18F-FDG PET are
lacking. In a retrospective study, 24 patients had undergone both 18F-FDG PET and bone
scans within six months because of suspected bone metastases.25 This study shows that bone
scintigraphy is still valuable in differentiated thyroid cancer, as it was found that 38% of bone
metastases could be missed on 18F-FDG PET. Further prospective studies in a higher number
of patients are required to define the exact role of bone scan and 18F-FDG PET in the
detection of bone metastases in patients with differentiated thyroid cancer (DTC).

Chapter 5
80
Combined or integrated 18F-FDG PET/CT in patients with negative 131I scans and elevated
thyroglobulin (Tg) showed that the diagnostic accuracy can be improved compared to 18F-
FDG PET or CT alone. The combination of these imaging techniques has also led to a change
in patient management and therapy, e.g., extension of surgery by providing precise anatomical
localization of the recurrent or metastatic disease.26
Medullary thyroid cancer (MTC)
The detection of recurrence or metastases in MTC is difficult and there is no single method
sensitive enough to reveal all MTC recurrences or metastases. In comparison with the
calcitonin tumour marker nearly all imaging modalities (Ultrasonography, CT, MRI, and
scintigraphy) have limited sensitivities. The clinical role of 18F-FDG PET in the diagnosis and
staging of recurrent and metastatic MTC seems promising.27
The sensitivity and specificity of 18F-FDG PET ranges between 73%-88% and 76%-80%,
respectively. In a study by de Groot et al., 18F-FDG PET was performed in patients with
elevated serum tumour markers after total thyroidectomy.28 Compared with 111In-octreotide
imaging(lesion based sensitivity: 41%), 99mTc(V)DMSA scintigraphy (57%) and
morphological imaging (87%), 18F-FDG PET (96%) was superior. However, morphological
imaging will always be needed because 18F-FDG PET only yields functional data and no
morphological information, which is necessary to assess resectability.
The combination of 18F-FDG PET/CT can have a useful role in medullary thyroid cancer.
Because surgery only can cure the disease, precise anatomical localization and the extent of
the recurrent or metastatic disease is mandatory. However, little data and case reports have
shown an increased diagnostic accuracy so further studies are needed.27
18Fluorine-dihydroxyphenylalanine (
18F-DOPA)
Mechanism
The mechanism responsible for uptake of 18Fluorine-dihydroxyphenylalanine (18F-DOPA) in
medullary thyroid carcinoma is probably the strongly upregulated transmembrane transport of
amino acids via the large amino acid transporters in medullary thyroid carcinoma cells. It is
not yet clear whether the increased uptake of 18F-DOPA PET is the result of the increased
transporter capabilities or the increased metabolic activity of the catecholamine pathway.

PET imaging in thyroid carcinoma
81
After transmembrane transport, 18F-DOPA is intracytoplasmatically converted into
dopamine by the enzyme aromatic acid decarboxylase (AADC). The formed 18F-dopamine is
transported into secretory vesicles via the vesicular mono aminoacid transporters (VMAT) in
which it can be further metabolized to 18F-noradrenalin and 18F-adrenalin.29 Although the 18F
atom influences the metabolism of 18F-DOPA there is no or little effect on the transport into
the intracellular environment. In the kidneys, 18F-DOPA is rapidly converted into 18F-dopamine
which is than excreted actively in urine. This conversion can be inhibited by oral
administration of carbidopa prior to tracer administration.30
Carbidopa also lowers the physiological uptake of 18F-DOPA in the pancreas, but it is yet
unknown which mechanism is responsible for this decrease in pancreatic uptake. The
reduction in renal and urinary activity leads to a better image quality in the surroundings of
the urinary system. Also, the reduced uptake in the pancreas makes the identification of
lesions in the pancreatic region easier. It can be speculated that by reducing the excretion of 18F-DOPA, more 18F-DOPA is available for neuroendocrine tumour lesions; thereby,
increasing the tumour to background ratio, leading to a better discrimination of
neuroendocrine lesions.
Scan method
In most centres, patients are prepared with oral administration of carbidopa, either in a fixed
dose or in a dose calibrated to body weight. Patients are scanned in a fasting condition for 4-6
h. In most centres a whole body study will be performed ranging from the skull to the upper
femora. The average injected dose is 200 MBq, the radiation burden ~ 4 mSv.30 Attenuation
correction is applied, either by using a CT in a PET-CT machine or by using camera-specific
attenuation protocols.
Clinical application
Medullary thyroid cancer
Although 18F-DOPA PET is not yet in widespread use, it is a promising new functional
imaging procedure for imaging neuroendocrine tumours. More and more centres gain access
to this tracer either via on-site production or production elsewhere. Hoegerle et al. were the
first to describe the use of 18F-DOPA PET in medullary thyroid cancer.31 In this study 18F-
DOPA PET was compared with 18F-FDG PET, SRS, and CT/MRI. A high precision of 18F-
DOPA PET was observed in the diagnosis of lymph node metastases (sensitivity 88%), while

Chapter 5
82
organ metastases were better detected with conventional imaging (sensitivity 13%). In the
recently published study by Koopmans et al. diagnostic accuracy was assessed for 18F-DOPA
PET in patients with carcinoid tumours which are, like medullary thyroid carcinoma,
neuroendocrine tumors.32 Compared to conventional somotostatine receptor scintigraphy
(SRS) they showed improved sensitivity of 18F-DOPA PET in staging and identify carcinoid
tumours.
A. 18F-FDG PET B. 18F-DOPA PET
Figure 2 These are the images of a patient known with medullary thyroid cancer. In this patient 18
F-FDG PET
(A) and 18
F-DOPA PET (B) were performed. The 18
F-DOPA PET (B) showed multiple lesions in the liver and
several lesions in the spinal column(arrows) while the 18
F-FDG PET showed hardly any lesions.
The value of 18F-DOPA PET for the detection of recurrent or residual disease in 21 patients
with postsurgically elevated calcitonin or CEA was assessed by Koopmans et al..33 They
compared 18F-DOPA PET with 18F-FDG PET, 99mT(V)DMSA, and CT/MRI. 18F-DOPA PET
was superior to conventional imaging for the detection of MTC on patient (sensitivity 87%)
and regional (89%) level. On lesional level 18F-DOPA PET (sensitivity 71%) was equal to
morphological imaging (64%) but superior to 18F-FDG PET (30%) and 99mT(V)DMSA (19%).
In the recent study by Beuthien-Baumann et al., 18F-DOPA-PET also seems to be more
specific than 18F-FDG PET for the detection of metastases of MTC.34 Thus, compared with 18F-FDG PET and conventional imaging techniques, 18F-DOPA PET provides better results in
the imaging of medullary thyroid cancer. However, it is still unclear if this improved imaging
results in different therapeutic approaches, and so further research is needed.

PET imaging in thyroid carcinoma
83
11C-Methionine (MET) PET
Mechanism
Proteins play an important role in virtually all biological processes. Proteins are built from a
set of 20 amino acids. Amino acid transport across the cell membranes into the cells occurs
primarily via carrier-mediated processes. Amino acid transport is generally increased in
malignant transformation.35-37 This increased protein metabolism in cancer cells is important
for metabolic tumour imaging, for which radiolabeled amino acids can be applied. These
amino acid tracers could help in imaging areas where 18F-FDG is limited such as the
interference of high (physiologic) 18F-FDG uptake in the brain. Another reason is that amino
acid imaging is less influenced by inflammatory disease. The most frequently used
radiolabeled amino acid is L-[methyl-11C]-methionine. Normal biodistribution of radiolabeled
methionine occurs in the pancreas, liver, spleen, kidney, and salivary glands.
Scan method
11C-MET PET scanning can be performed 10 to 20 min after intravenous injection of a fixed
dose or a dose calibrated on body weight (suggested range is 70 MBq to 1100 MBq), in a
fasting condition for 2-6 h. Images are corrected, either by using a CT in a PET/CT machine
or by using camera-specific attenuation protocols.
Clinical application
Differentiated thyroid cancer
The need for new tracers and improvement of diagnostic tools in thyroid cancer is growing.
So far, no data on the application of methionine (MET) PET in thyroid cancer are available.
The general feasibility of amino acid imaging in many tumour types has been sufficiently
shown.37
It is imaginable that thyroid cancer could sufficiently concentrate amino acids due to its
metabolically inert nature and high protein synthesis (e.g., thyroglobulin). In a feasibility
study by Phan et al., 11C-MET PET has been compared with 18F-FDG PET in the detection of
recurrent or metastatic disease in 20 patients with negative 131I scans and elevated Tg.38 Six of
the 20 patients showed uptake on both PET scans, but the abnormalities were more 18F-FDG-
avid and more extensive on the 18F-FDG PET in 3 patients. In four of the 20 patients uptake

Chapter 5
84
was only observed on the 11C-MET PET; however, no anatomical localization could be
confirmed. Presently, the significance of the MET uptake in these four patients is unclear, so
the clinical value of 11C-MET PET in the detection of recurrent DTC disease still has to be
proven in the (long-term) follow-up.
A. 11C-MET PET B. 18F-FDG PET
Figure 3 These are the images of a 68-y old female known with papillary thyroid cancer. This patient had
unreliable Tg due to the presence of Tg antibodies (which were increasing in the course of the follow-up). The
post-treatment 131
I whole body scan (WBS) was negative. Due to suspicion of dedifferentiated, metastatic
disease 11
C-MET PET (A) and 18
F-FDG PET (B) were performed. 11
C-MET PET (A) showed lesions in the
mediastinum with slightly to moderate 11
C-MET uptake. 18
F-FDG PET (B) also showed multiple lesions in the
mediastinum, but the lesions showed clearly higher 18
F-FDG uptake and the abnormalities were more
extensive.
124Iodine-PET
Mechanism
Iodine-124 is a positron emitting isotope, which is suitable for PET imaging, with a half-life
of 4.2 days.39 This isotope has been used for dosimetric purposes or thyroid volume
measurements.40 While the radioisotopes 123I and especially 131I are used on a wide scale in
diagnosis and treatment of many thyroid disorders, 124I has received little attention.
Chemically identical to nonradioactive iodine, this radioisotope allows thyroid cancer imaging
with the high resolution PET technique.39,40

PET imaging in thyroid carcinoma
85
Scan method
The 124I -PET scan can be obtained 24 h to 6 days after administration of 74-100 MBq of 124I.
A whole body PET scan (from the upper thigh up until the top of the skull) can be performed
in 2D or 3D mode, using standard energy window setting of 350-650 keV (or energy window
setting 425-650 keV or 460-562 keV in case of the presence of high amounts of 131I.41
Clinical application
Differentiated thyroid cancer
Accumulation of iodine is a highly specific characteristic for differentiated thyroid cancer
(DTC) cells. In patients with increasing or recurrent detectable Tg a blind treatment (meaning
after a negative diagnostic 131I scan) with high dose 131I followed by a post-treatment 131I scan
is used as a diagnostic tool. However, this strategy with (unnecessary) high radiation exposure
must be taken into account in patients without 131I uptake in their metastases. Besides the high
radiation exposure, there is a high TSH level which potentially stimulates thyroid cancer cell
growth.
Based on the higher spatial resolution, 124I-PET is potentially able to detect recurrent
disease in DTC with a higher sensitivity than (diagnostic) 131I scans. With this higher
sensitivity and the possibility to combine the 124I-PET scan with morphologic imaging, such
as CT data, an appropriate therapeutic decision in terms of surgery and/or additional high dose 131I can be made. 124I-PET imaging might, therefore, become the diagnostic tool of choice in
the follow-up of DTC. In the study by Freudenberg et al., 124I-PET (/CT) modalities were
compared with the high dose 131I-WBS in 12 patients with DTC.42 They showed an overall
lesion detectability of 87 %, 83%, and 100% for 124I, 131I-WBS and combined 124I-PET/CT
respectively. So, these 124I-PET (/CT) modalities are promising diagnostic tools and are
suitable alternative to the high dose 131I-WBS in the follow-up of DTC patients.
In a prospective, feasibility study by Phan et al., 20 patients with advanced DTC (T4,
extranodal tumour growth, distant metastasis) underwent a low-dose diagnostic 131I scan, a 124I PET scan, and a high-dose (posttreatment) 131I scan.43 The 131I images were compared to
the 124I-PET images. 124I-PET proved to be a superior diagnostic tool as compared to low dose
diagnostic 131I scans, and showed comparable findings with the post-treatment 131I-WBS
which was in agreement with the study by Freudenberg et al. and Abdul Fatah et al..42,44
Therefore, 124I-PET could be used as a diagnostic tool in the follow-up of patients with DTC
for the favourable radiation exposure burden compared to the high dose diagnostic 131I-WBS

Chapter 5
86
and the superior diagnostic accuracy compared to low dose diagnostic 131I-WBS and the
fusion possibility with CT which improves clinical decision making.
A. Post-treatment 131I-WBS B. 124I-PET
C. 18F-FDG PET
Figure 4 These are the images of a 68-year old male known with follicular thyroid cancer. This patient showed
increased serum Tg level (14 ng/ml) suspected for recurrent or metastatic disease. Blind treatment with 131
I
was given followed by a post-treatment whole body scan (WBS) after 10 days (A), which was negative. The 124
I-
PET (B) was also negative, besides physiological uptake in the salivary glands, oesophagus, gastro-intestinal
tract, kidney and bladder. 18
F-FDG PET (C) showed a focal lesion in the lower lobe of the left lung (arrow),
confirmed by CT. This complementary uptake of radioiodine and 18
F-FDG is known as the flip-flop phenomenon.
Conclusion
This chapter on PET imaging in thyroid cancer gives an overview of the different PET
techniques available in thyroid cancer. PET imaging is based on two principles: the ability of
unstable atom nucleus to emit positrons and the labelling of organic molecules, which are
used in specific metabolic pathways.

PET imaging in thyroid carcinoma
87
For differentiated thyroid cancer the most frequently used PET technique is 18F-FDG PET
imaging, which is based on the use of a glucose analogue. Although its application in the
preoperative assessment of thyroid nodules is still unclear, it is considered an useful tool in
the follow up of differentiated thyroid cancer. The use of PET/CT scanning which combines
functional imaging with morphological imaging is promising, providing more accurate
localization of tumour sites, which is important for further treatment.
Other PET radiotracers have been developed: the clinical value of amino acid tumour
imaging with 11C-MET PET is unclear and still has to be proven in the follow-up of
differentiated thyroid cancer. Another relative new PET imaging technique is the iodine
isotope 124I. Compared with the high dose diagnostic 131I whole body scan, 124I-PET showed
similar findings and can therefore be used as a diagnostic tool in the follow-up of
differentiated thyroid cancer.
For the follow-up of medullary thyroid cancer 18F-FDG PET is also the most employed
imaging technique. However, 18F-DOPA PET, which is based on a precursor of dopamine,
seems to be superior compared to 18F-FDG PET in the follow up of medullary thyroid cancer.
A potential new tracer is 11C-5-HTP, which is based on a precursor of serotonin and already
has been applied in neuroendocrine tumours. The value of this technique has to be further
assessed in medullary thyroid cancer.
The need for new tracers and advanced PET imaging to improve the diagnostic
sensitivities and accuracy in detection, staging, and follow-up of thyroid cancer patients is
growing. Knowledge of the pathogenesis, the molecular characteristics and the behaviour of
the tumour cell is crucial for developing of specific tracers and techniques, e.g., radiolabeled
Tg, (rh) TSH. Although new tracers are developed and applied in patients, little data are
available on the changes in therapeutic management these new PET-techniques give. While
PET-imaging is still in development, more research is needed to assess the effects on therapy
of these new developments. In conclusion, PET imaging is a useful diagnostic tool in thyroid
cancer and new promising techniques are developed which could further improve the
diagnostic accuracy and therapeutic approaches.

Chapter 5
88
References
1. Schlumberger M, Pacini F. Epidemiology. In: Anonymous Thyroid Tumours. Paris: Editions nucleon;
2003. p 51-60.
2. Sherman SI, Angelos P, Ball DW, et al. Thyroid carcinoma. J Natl Compr Canc Netw 2005;3:404-457.
3. Modigliani E, Cohen R, Campos JM, et al. Prognostic factors for survival and for biochemical cure in
medullary thyroid carcinoma: results in 899 patients. The GETC Study Group. Groupe d'etude des
tumeurs a calcitonine. Clin Endocrinol (Oxf) 1998;48:265-273.
4. Tubiana M, Haddad E, Schlumberger M, Hill C, Rougier P, Sarrazin D. External radiotherapy in thyroid
cancers. Cancer 1985;55:2062-2071.
5. Venkatesh YS, Ordonez NG, Schultz PN, Hickey RC, Goepfert H, Samaan NA. Anaplastic carcinoma of
the thyroid. A clinicopathologic study of 121 cases. Cancer 1990;66:321-330.
6. Bailey DL, Karp JS, Surti S. Physics and instrumentation in PET. In: PE Valk, DL Bailey, DW Townsend,
MN Maisey, editors. Positron Emission Tomography; Basic Sience and Clinical Practice. London:
Springer; 2003.
7. Mason NS, Mathis CA. Radiohalogens for PET imaging. In: PE Valk, DL Bailey, DW Townsend, MN
Maisey, editors. Positron emission tomography basic science and clinical practice. London: Springer;
2003.
8. Warburg OH, Dickens F, Kaiser Wilhelm If. The Metabolism of Tumours: Investigations from the Kaiser
Wilhelm Institute for Biology, Berlin-Dahlem. : Richard R. Smith; 1931.
9. Brown RS, Goodman TM, Zasadny KR, Greenson JK, Wahl RL. Expression of hexokinase II and Glut-1 in
untreated human breast cancer. Nucl Med Biol 2002;29:443-453.
10. Kubota R, Yamada S, Kubota K, Ishiwata K, Tamahashi N, Ido T. Intratumoral distribution of fluorine-
18-fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation tissues studied by
microautoradiography. J Nucl Med 1992;33:1972-1980.
11. Strauss LG. Fluorine-18 deoxyglucose and false-positive results: a major problem in the diagnostics of
oncological patients. Eur J Nucl Med 1996;23:1409-1415.
12. de Geus-Oei LF, Pieters GF, Bonenkamp JJ, et al. 18F-FDG PET reduces unnecessary
hemithyroidectomies for thyroid nodules with inconclusive cytologic results. J Nucl Med 2006;47:770-
775.
13. Mitchell JC, Grant F, Evenson AR, Parker JA, Hasselgren PO, Parangi S. Preoperative evaluation of
thyroid nodules with 18FDG-PET/CT. Surgery 2005;138:1166-74; discussion 1174-5.
14. Kresnik E, Gallowitsch HJ, Mikosch P, et al. Fluorine-18-fluorodeoxyglucose positron emission
tomography in the preoperative assessment of thyroid nodules in an endemic goiter area. Surgery
2003;133:294-299.
15. Kim JM, Ryu JS, Kim TY, et al. 18F-fluorodeoxyglucose positron emission tomography does not predict
malignancy in thyroid nodules cytologically diagnosed as follicular neoplasm. J Clin Endocrinol Metab
2007;92:1630-1634.
16. Bogsrud TV, Karantanis D, Nathan MA, et al. The value of quantifying 18F-FDG uptake in thyroid
nodules found incidentally on whole-body PET-CT. Nucl Med Commun 2007;28:373-381.
17. Joensuu H, Ahonen A. Imaging of metastases of thyroid carcinoma with fluorine-18
fluorodeoxyglucose. J Nucl Med 1987;28:910-914.
18. Schluter B, Bohuslavizki KH, Beyer W, Plotkin M, Buchert R, Clausen M. Impact of FDG PET on patients
with differentiated thyroid cancer who present with elevated thyroglobulin and negative 131I scan. J
Nucl Med 2001;42:71-76.
19. van Tol KM, Jager PL, Piers DA, et al. Better yield of (18)fluorodeoxyglucose-positron emission
tomography in patients with metastatic differentiated thyroid carcinoma during thyrotropin
stimulation. Thyroid 2002;12:381-387.
20. Filetti S, Damante G, Foti D. Thyrotropin stimulates glucose transport in cultured rat thyroid cells.
Endocrinology 1987;120:2576-2581.
21. Hosaka Y, Tawata M, Kurihara A, Ohtaka M, Endo T, Onaya T. The regulation of two distinct glucose
transporter (GLUT1 and GLUT4) gene expressions in cultured rat thyroid cells by thyrotropin.
Endocrinology 1992;131:159-165.
22. Petrich T, Borner AR, Otto D, Hofmann M, Knapp WH. Influence of rhTSH on [(18)F]fluorodeoxyglucose
uptake by differentiated thyroid carcinoma. Eur J Nucl Med Mol Imaging 2002;29:641-647.

PET imaging in thyroid carcinoma
89
23. Chin BB, Patel P, Cohade C, Ewertz M, Wahl R, Ladenson P. Recombinant human thyrotropin
stimulation of fluoro-D-glucose positron emission tomography uptake in well-differentiated thyroid
carcinoma. J Clin Endocrinol Metab 2004;89:91-95.
24. Hooft L, Hoekstra OS, Deville W, et al. Diagnostic accuracy of 18F-fluorodeoxyglucose positron
emission tomography in the follow-up of papillary or follicular thyroid cancer. J Clin Endocrinol Metab
2001;86:3779-3786.
25. Phan HT, Jager PL, Plukker JT, Wolffenbuttel BH, Dierckx RA, Links TP. Detection of bone metastases in
thyroid cancer patients: bone scintigraphy or 18F-FDG PET? Nucl Med Commun 2007;28:597-602.
26. Shammas A, Degirmenci B, Mountz JM, et al. 18F-FDG PET/CT in patients with suspected recurrent or
metastatic well-differentiated thyroid cancer. J Nucl Med 2007;48:221-226.
27. Nanni C, Rubello D, Fanti S, et al. Role of 18F-FDG-PET and PET/CT imaging in thyroid cancer. Biomed
Pharmacother 2006;60:409-413.
28. de Groot JW, Links TP, Jager PL, Kahraman T, Plukker JT. Impact of 18F-fluoro-2-deoxy-D-glucose
positron emission tomography (FDG-PET) in patients with biochemical evidence of recurrent or
residual medullary thyroid cancer. Ann Surg Oncol 2004;11:786-794.
29. Pearse AG. The APUD cell concept and its implications in pathology. Pathol Annu 1974;9:27-41.
30. Brown WD, Oakes TR, DeJesus OT, et al. Fluorine-18-fluoro-L-DOPA dosimetry with carbidopa
pretreatment. J Nucl Med 1998;39:1884-1891.
31. Hoegerle S, Altehoefer C, Ghanem N, Brink I, Moser E, Nitzsche E. 18F-DOPA positron emission
tomography for tumour detection in patients with medullary thyroid carcinoma and elevated
calcitonin levels. Eur J Nucl Med 2001;28:64-71.
32. Koopmans KP, de Vries EG, Kema IP, et al. Staging of carcinoid tumours with 18F-DOPA PET: a
prospective, diagnostic accuracy study. Lancet Oncol 2006;7:728-734.
33. Koopmans KP, de Groot JW, Plukker JT, et al. 18F-dihydroxyphenylalanine PET in patients with
biochemical evidence of medullary thyroid cancer: relation to tumor differentiation. J Nucl Med
2008;49:524-531.
34. Beuthien-Baumann B, Strumpf A, Zessin J, Bredow J, Kotzerke J. Diagnostic impact of PET with 18F-
FDG, 18F-DOPA and 3-O-methyl-6-[18F]fluoro-DOPA in recurrent or metastatic medullary thyroid
carcinoma. Eur J Nucl Med Mol Imaging 2007;34:1604-1609.
35. BUSCH H, DAVIS JR, HONIG GR, ANDERSON DC, NAIR PV, NYHAN WL. The uptake of a variety of amino
acids into nuclear proteins of tumors and other tissues. Cancer Res 1959;19:1030-1039.
36. Isselbacher KJ. Sugar and amino acid transport by cells in culture--differences between normal and
malignant cells. N Engl J Med 1972;286:929-933.
37. Jager PL, Vaalburg W, Pruim J, de Vries EG, Langen KJ, Piers DA. Radiolabeled amino acids: basic
aspects and clinical applications in oncology. J Nucl Med 2001;42:432-445.
38. Phan HT, Jager PL, Plukker JT, Wolffenbuttel BH, Dierckx RA, Links TP. Comparison of 11C-methionine
PET and 18F-fluorodeoxyglucose PET in differentiated thyroid cancer. Nucl Med Commun
2008;29:711-716.
39. Pentlow KS, Graham MC, Lambrecht RM, et al. Quantitative imaging of iodine-124 with PET. J Nucl
Med 1996;37:1557-1562.
40. Eschmann SM, Reischl G, Bilger K, et al. Evaluation of dosimetry of radioiodine therapy in benign and
malignant thyroid disorders by means of iodine-124 and PET. Eur J Nucl Med Mol Imaging
2002;29:760-767.
41. Lubberink M, van Schie A, de Jong HW, van Dongen GA, Teule GJ. Acquisition settings for PET of 124I
administered simultaneously with therapeutic amounts of 131I. J Nucl Med 2006;47:1375-1381.
42. Freudenberg LS, Antoch G, Jentzen W, et al. Value of (124)I-PET/CT in staging of patients with
differentiated thyroid cancer. Eur Radiol 2004;14:2092-2098.
43. Phan HT, Jager PL, Paans AM, et al. The diagnostic value of 124I-PET in patients with differentiated
thyroid cancer. Eur J Nucl Med Mol Imaging 2008;35:958-965.
44. Abdul Fatah S, Brans B, Huijberts M, Sels J, Nieuwenhuijzen Kruseman A, Teule G. Impact of I-124 PET-
CT in the loco-regional staging of differentiated thyroid carcinoma. J NUCL MED MEETING ABSTRACTS
2007;48:127P-c.

90

Chapter 6
Clinical relevance of 18
F-FDG PET and 18
F-DOPA PET in
recurrent medullary thyroid carcinoma
Hans H.G. Verbeek, John T.M. Plukker, Klaas P. Koopmans, Jan Willem B. de Groot
Robert M.W. Hofstra, Anneke C. Muller-Kobold, Anouk N.A. van der Horst-Schrivers
Adrienne H. Brouwers, Thera P. Links
J Nucl Med. 2012; 53: 1863-71

Chapter 6
92
Abstract
Introduction The transition from stable to progressive disease is unpredictable in patients
with biochemical evidence of medullary thyroid carcinoma (MTC). Calcitonin and
carcinoembryonic antigen (CEA) doubling times are currently the most reliable markers for
progression, but for accurate determination serial measurements are required which need time.
We compared 18F-fluoro-2-deoxy-D-glucose (18F-FDG) positron emission tomography (PET)
and 18F-dihydroxyphenylanaline (18F-DOPA) PET with biochemical parameters and survival
to assess whether these imaging modalities could be of value in detecting progressive disease.
Methods We evaluated outcome of 18F-FDG PET and/or 18F-DOPA PET with calcitonin and
CEA doubling times in 47 MTC patients. A subgroup of patients was included in whole
metabolic burden (WBMTB) analysis, with determination of standardized uptake values
(SUV) and number of lesions. WBMTB of 18F-DOPA PET and 18F-FDG PET was compared
with biochemical parameters. Furthermore survival was compared with 18F-DOPA PET
and/or 18F-FDG PET positivity.
Results In 38 out of 40 patients with 18F-FDG PET doubling times were available. There was
a significant correlation with 18F-FDG PET positivity. Doubling times were <24 months in
77% (n=10/13) of 18F-FDG PET positive patients, while 88% (n=22/25) of 18F-FDG PET
negative patients had doubling times >24 months (p<0.001). Between doubling times and 18F-
DOPA PET positivity no significant correlation existed. 18F-DOPA PET detected significantly
more lesions (75%, 56 of 75) compared to 18F-FDG PET (47%, 35 of 75) in the 21 patients
included in WBMTB analysis (p=0.009). Calcitonin and CEA levels correlated significantly
with WBMTB on 18F-DOPA PET but doubling times did not. 18F-FDG PET positivity was a
more important indicator for poor survival in patients with both scans performed.
Conclusion 18F-FDG PET is superior in detecting patients with biochemical progressive
disease and identifying patients with a poor survival. Although 18F-DOPA PET has less
prognostic value it can more accurately assess the extent of the disease in patients with
residual MTC. Hence, both scans are informative regarding tumour localization and
behaviour. Based on these results we designed a clinical flow diagram for the general practice
in detecting recurrent MTC.

18F-FDG PET and
18F-DOPA PET in MTC
93
Introduction
Medullary thyroid carcinoma (MTC) accounts for about 4% of all thyroid cancers. The
overall 10 year survival ranges between 40% and 80% and has not increased substantially in
the past few decades.1-3 Unfortunately, even in MTC that is clinically confined to the neck,
many patients already have metastatic disease and are beyond cure even by surgery.
Furthermore, though the overall survival in patients with only biochemical evidence of
residual MTC is good, a number of patients will develop progressive and symptomatic
disease.4 Early identification of these patients is clinically relevant because appropriate
therapeutic interventions may delay symptomatic deterioration. However, the transition from
a stable status to a progressive disease course is unpredictable and it is hard to identify
patients who may benefit from early intervention.
Calcitonin is a specific tumour marker for MTC, carcinoembryonic antigen (CEA) is less
specific, but can also be useful.5 Currently, short calcitonin and CEA doubling times are
considered the best available indicators to assess progressive disease, MTC recurrence and
cancer mortality.6,7 Calcitonin and CEA levels can fluctuate, however, and determination of
the doubling times needs serial measurement for 12-24 months and is therefore time-
consuming.
Most imaging techniques have a moderate sensitivity in detecting MTC.8 Positron emission
tomography (PET) using the radioactive tracers 18F-fluoro-2-deoxy-D-glucose (18F-FDG) and
more recently 18F-dihydroxyphenylanaline (18F-DOPA) are available for the staging and
follow-up of MTC.9-15 Some studies have suggested that 18F-FDG PET might be more
sensitive in patients with a short calcitonin doubling time.16,17 Furthermore, a higher
metabolic activity, expressed as the maximum standardized uptake value (SUV), on 18F-FDG
PET compared with the maximum SUV on 18F-DOPA PET, might be related to a more
aggressive tumour type.18 PET also enables determination of the total tumour load expressed
as the whole-body metabolic burden (WBMTB), reflecting metabolic tumour activity, as was
shown in a recent study of 18F-DOPA PET in carcinoid patients.19
In this retrospective study of patients with biochemical evidence of MTC, our aim was to
assess the ability of 18F-FDG PET and 18F-DOPA PET to discriminate between patients with
progressive disease and patients with stable disease.

Chapter 6
94
Materials and methods
Patients
We analysed all patients with histologically proven MTC seen at the Department of
Endocrinology for follow-up and who had undergone 18F-FDG PET and/or 18F-DOPA PET
for detection of residual or metastatic MTC between 2002 and 2010. We excluded patients
with undetectable calcitonin levels, patients with concurrent systemic treatment at the time of 18F-FDG PET or 18F-DOPA PET, and patients with less than 2 calcitonin or CEA values at
the time of 18F-FDG PET or 18F-DOPA PET imaging. For WBMTB analysis, we excluded
patients with more than 6 months between 18F-FDG PET and 18F-DOPA PET imaging.
Several patients (n=21) were also described in a previous study assessing the value of 18F-
DOPA PET in patients with MTC.16 That study was approved by the local medical ethics
committee, and the patients gave written informed consent to participate in it. After
completion of that study PET was performed as part of standard patient care; therefore in
concordance with national law no further Institutional Board Review approval was required.
We initially analysed 47 MTC patients (Figure 1). In group A, composed of 40 patients, 18F-FDG PET was performed and we compared outcome with doubling times (n=38) and
survival (n=37). For the 38 patients composing group B, 18F-DOPA PET was performed, and
we compared outcome with biochemical parameters (n=36) and survival (n=34).Thirty one
patients had undergone both scans and in 24 patients these scans were performed within 6
months of each other. We performed WBMTB and survival analysis in respectively, 21 and
22 patients (group C), of which 14 and 15 patients respectively, were also included in the
previous study.16 The number of patients participating in each analysis and reasons for
exclusion are shown in Figure 1. Patient characteristics of the different groups are shown in
Table 1.
18
F-DOPA PET, 18
F-FDG PET and image analysis
18F-FDG and 18F-DOPA were locally produced as described previously.20 All patients were
studied after a 6-h fasting period, were allowed to continue all medication, and were
encouraged to drink water. For 18F-FDG PET, data acquisition started after 60 or 90 min after
injection of 18F-FDG intravenously(5 MBq/kg; range 250-824 MBq). For 18F-DOPA PET,
whole body 2-dimensional-PET images were acquired 60 min after the intravenous
administration of a standard dose of 18F-DOPA (range 70-220 MBq). To reduce tracer

18F-FDG PET and
18F-DOPA PET in MTC
95
decarboxylation and subsequent renal clearance and thereby increase tracer uptake in tumour
cells, patients received carbidopa (2 mg/kg; maximum 150 mg) orally as pre-treatment 1 h
before the 18F-DOPA injection.
Figure 1 Flow diagram for inclusion and analysis of MTC patients.*Insufficient biochemical data for calculation
of doubling times. †Insufficient follow-up data.
‡n = 1 without suitable scan for WBMTB analysis due to
technical problems. pts = patients.
18F-FDG PET and 18F-DOPA PET images were interpreted by two dedicated nuclear
medicine specialists as part of routine patient care and were subsequently independently
reviewed. We calculated the WBMTB, defined as the sum of the metabolic burden of each
tumour lesion in the PET image, for both PET methods. We defined metabolic burden as
mean SUV × volume of tumour lesion obtained from the PET image using a volume of
interest that was enclosed by a 40 % isodensity contour (Figure 2).21,22 We categorized
patients according to differences in WBMTB uptake on paired 18F-FDG and 18F-DOPA PET
scans; more than 10% WBMTB on 18F-FDG PET, more than 10% WBMTB on 18F-DOPA
PET, equal uptake (less than 10% difference) or no uptake on both scans.

Chapter 6
96
Biochemical analysis
Calcitonin was determined using an enzyme-linked immunosorbent assay (Biomerica, Irvine,
Califorina, USA) with a reference value of 0.3-12 ng/L. CEA levels were measured using a
chemiluminescent microparticle immunoassay (Abbott Laboratories, North Chicago, Illinois,
USA) with a reference value of 0.5-5.0 µg/L.
Table 1 Patient characteristics
18
F-FDG PET
analysis
(group A; n = 38)
18F-DOPA PET
analysis
(group B; n = 36)
WBMTB
analysis
(Group C; n = 21)
Sex
Male
Female
19
19
17
19
10
11
Age (y)
Mean
Range
53.2
19-79
52.4
19-79
56.7
19-79
Type
Sporadic
Familial
18
20
18
18
12
9
Calcitonin (ng/L)
Median
Range
346.2
1.8-161,275
825
17.8-240,325
817
17.8-161,275
CEA (µg/L)
Median
Range
10.2
0.5-2620
12.3
0.5-2620
9.7
0.5-2620
Calcitonin doubling time
<24 mo
>24 mo
13 (34%)
25 (66%)
13 (36%)
23 (64%)
9 (43%)
12 (57%)
CEA doubling time
<24 mo
>24 mo
6 (19%)
32 (81%)
5 (14%)
30* (86%)
3 (14%)
18 (86%)
Calcitonin and CEA doubling time
Calcitonin or CEA <24 mo
Calcitonin and CEA >24 mo
13 (34%)
25 (66%)
14 (39%)
22 (61%)
9 (43%)
12 (57%)
PET
Positive
Negative
13 (34%)
25 (66%)
16 (44%)
20 (56%)
10 (48%)
11 (52%)
*Of one patient CEA doubling time could not be calculated. mo = months.

18F-FDG PET and
18F-DOPA PET in MTC
97
Calcitonin and CEA serum levels and doubling times
For calculating the calcitonin and CEA doubling time, we used in principle 4 values (with a
minimum of 2), obtained within a median period of 11 months (range 2-47 months) around 18F-FDG PET and 18F-DOPA PET imaging. We used the average of these values for further
analysis. We calculated exponential growth curves aB, using standard linear regression of the
serum levels on time and doubling times as ln(2)/B. To identify progressive patients we
defined biochemical progressive disease as a calcitonin or CEA doubling time of less than 24
months in concordance with the study of Giraudet et al..6
Figure 2 Determination of volume of interest (VOI) and standardized uptake value (SUV) for calculation of the
whole metabolic burden. On this 18
F-FDG PET scan four lesions (respectively subcarinal, in the lateral
hemithorax, and in the liver region) are enclosed by a 40% iso-contour, after manual designation, with
automatic calculation of SUVmean, SUVmax and lesion volume.
Follow-up
Follow-up was performed according to current guidelines, consisting of regular determination
of calcitonin and CEA.23 If there was an elevation in one of these tumour markers, further
evaluation was performed with morphological or functional imaging. Depending on the
outcome of imaging, the therapeutic strategy was determined.
Statistical analysis
For statistical analysis we used PASW statistics 18 (SPSS Ltd.). We performed a χ2 test for
comparison of PET outcome and doubling times. Correlation between WBMTB of 18F-FDG

Chapter 6
98
PET and 18F-DOPA PET and calcitonin or CEA levels and doubling times was calculated
with Spearman’s r test. To determine the optimal calcitonin cut-off level for 18F-FDG PET
and 18F-DOPA PET, we calculated the maximum value of sensitivity multiplied by specificity,
as derived from ROC curve analysis. We performed a χ2 test for comparison of uptake and
WBMTB category with doubling times or a Fisher exact test when the frequency of cells with
an expected value of 5 was higher than 20%. For comparison of the number of detected
lesions between 18F-FDG PET and 18F-DOPA PET, a McNemar test was used. For survival
analysis we used the Kaplan Meier method, and the log-rank test for comparison. The
significance level was 0.05, 2-sided.
Results
Patients
18F-FDG PET and biochemical parameters (Group A)
We analysed 38 patients for outcome of 18F-FDG PET and calcitonin or CEA levels and
doubling times. 18F-FDG PET was positive in 13 patients (34%) (Table 2). In 18F-FDG PET-
positive patients, levels of calcitonin and CEA were significantly higher and more patients
had calcitonin and CEA doubling times less than 24 months. Positive and negative predictive
values for biochemical progressive disease were 77% and 88% respectively in 18F-FDG PET-
positive and -negative patients. In ROC curve analysis, we found an optimal calcitonin cut-off
of 874 ng/L for PET positivity, with a sensitivity of 69% and a specificity of 70% for the
detection of tumour lesions.
18
F-DOPA PET and biochemical parameters (Group B)
Of the 36 patients analysed for the outcome of 18F-DOPA PET and biochemical parameters, 18F-DOPA PET was positive in 16 (44%) (Table 3). Calcitonin and CEA levels differed
significantly between 18F-DOPA PET positive and -negative patients, but there was no
significant difference in doubling times. The positive and negative predictive values for
progressive disease were 56% and 75%, respectively, in 18F-DOPA PET-positive and -
negative patients. In ROC curve analysis, we found a calcitonin cut-off of 825 ng/l to be
optimal for PET positivity, with a sensitivity and specificity of 88% and 80%, respectively,
for detection of tumour lesions.

18F-FDG PET and
18F-DOPA PET in MTC
99
Table 2 Biochemical parameters of patients with 18FDG PET (Group A)
18
F-FDG PET
Positive (n = 13)
18F-FDG PET
Negative (n = 25)
P
Calcitonin (ng/L)
Median
Range
2320
(60.4 – 161,275)
246
(1.8 – 18565)
0.040
CEA (ug/L)
Median
Range
32.4
(0.8 -2620)
6.5
(0.5-187)
0.006
Calcitonin doubling time
< 24 mo
> 24 mo
10 (77%)
3 (23%)
3 (14%)
22 (86%)
< 0.001
CEA doubling time
< 24 mo
> 24 mo
6 (46%)
7 (54%)
0
25 (100%)
0.001
Calcitonin and CEA doubling time
Calcitonin or CEA < 24 mo
Calcitonin and CEA > 24 mo
10 (77%)
3 (23%)
3 (14%)
22 (86%)
< 0.001
Mo = months.
Table 3 Biochemical parameters of patients with 18F-DOPA PET (Group B)
*Of 1 pt CEA level was not available. †Of 1 pt CEA dt could not be calculated. mo = months.
WMBTB results of 18
F-FDG PET and 18
F-DOPA PET (Group C)
For the 21 patients with both 18F-FDG PET and 18F-DOPA PET who were included in
WBMTB analysis, the results for both scans were negative in 11 patients. Of the remaining 10
patients, 4 had higher WBMTB on 18F-FDG PET, another 4 had higher WBMTB on 18F-
DOPA PET, and 2 had equal WBMTBs (Table 4). The total number of lesions found was 75,
and 18F-DOPA PET detected significantly more lesions than 18F-FDG PET (56 vs. 35)
18
F-DOPA PET
Positive (n = 16)
18F-DOPA PET
Negative (n =20)
P
Calcitonin (ng/L)
Median
Range
3626
(88 – 240,325)
287
(17.8 – 2320)
< 0.001
CEA (ug/L)
Median
Range
36.6
(1.2 – 2620)
6.6
(0.5 – 72)
<0.001
Calcitonin doubling time
< 24 mo
> 24 mo
8 (50%)
8 (50%)
5 (25%)
15 (75%)
NS
CEA doubling time
< 24 mo
> 24 mo
4 (27%)
11 (73%)
1 (5%)
19 (95%)
NS
Calcitonin and CEA doubling time
Calcitonin or CEA < 24 mo
Calcitonin and CEA > 24 mo
9 (56%)
7 (44%)
5 (25%)
15 (75%)
NS

Chapter 6
100
(p=0.009). In PET-positive patients, WBMTB on 18F-DOPA PET was significantly correlated
with calcitonin levels (r=0.82) (p=0.013) and CEA levels (r=0.88) (p=0.004) but not with
doubling times. There was no significant correlation between WBMTB of 18F-FDG PET and
calcitonin and CEA levels or doubling times. Between the different WBMTB categories and
calcitonin and CEA doubling times, no significant relation was found.
Table 4 Biochemical parameters and WBMTB in different WBMTB categories (Group C)
WBMTB Category
18F-DOPA >
18F-
FDG (n= 4)
18F-FDG >
18
F-DOPA (n = 4)
18F-DOPA =
18F-FDG (n = 2)
Negative P
Calcitonin (ng/L)
Median
Range
13052
832-161,275
650
89-1,066
14958
6,679-22,236
246
18-1,030
0.015
CEA (µg/L)
Median
Range
727
22-2620
14.2
0.8-29.3
1088
32.4 -2144
3.1
0.5-28.1
0.002
Calcitonin and CEA doubling time
Calcitonin or CEA < 24 mo
Calcitonin and CEA > 24 mo
1
3
3
1
2
0
3
8
NS
No. of lesions 18
F-FDG
Mean
Total 18
F-DOPA
Mean
Total
1.3
5
9.5
38
5.3
21
2.5
10
4.5
9
4
8
-
-
WBMTB (cm3)
18F-FDG
Median
Range 18
F-DOPA
Median
Range
55.4
0 – 121
271.6
15.3 – 983
83.3
18.8 - 920
6.1
0 - 465
275
11.5 – 538
271
12.5 - 530
-
-
Treatment based on PET
Eight patients underwent reoperation because of recurrent disease. In 5 patients, PET showed
local disease and contributed to the decision for surgery. 18F-FDG PET was performed in 4
and positive in 2. 18F-DOPA PET was performed in 4 patients and positive in 3. All PET
lesions were confirmed on histological examination. In the other 3 patients, PET was negative
and surgery was performed because of positive conventional imaging or palpable
abnormalities. All patients who underwent reoperation had no clinical progression during
follow-up (range 6.6–106 months). Seven patients received targeted treatment with tyrosine
kinase inhibitors. 18F-FDG PET imaging was performed in 6 patients and all showed

18F-FDG PET and
18F-DOPA PET in MTC
101
metastatic disease, 18F-DOPA PET was performed in 5 and showed metastatic disease in 4.
Three patients developed stable disease. The other 27 patients did not receive surgical or
systemic treatment during follow-up.
Survival and PET outcome
In the 42 patients of whom follow-up data were available, median follow-up was 63.8 months
(range 2.3-114 months). During follow-up 11 patients died: 7 because of progressive MTC, 3
because of other causes (prostate cancer, oesophageal cancer and sepsis due to perforated
appendicitis) and in 1 patient for whom the reason of death was unknown. In 37 patients with 18F-FDG PET imaging and sufficient follow-up, survival was significantly lower in 18F-FDG
PET positive patients than in 18F-FDG PET negative patients (p<0.001) (Figure 3A). The
same was true for 18F-DOPA PET positive compared with -negative patients (n=34)
(p=0.019) (Figure 3B). However, in univariate analysis of patients who had undergone both 18F-FDG PET and 18F-DOPA PET (n=22), the survival in patients with a positive 18F-FDG
PET was lower and independent of 18F-DOPA PET outcome, whereas survival in 18F-DOPA
PET positive patients was dependent of 18F-FDG PET outcome (p=0.018) (Figure 3C). Figure
4 shows a patient with biochemical progressive disease and uptake on both scans.
Figure 3 Kaplan Meier curve of survival (in years) after 18
F-FDG PET (A), 18
F-DOPA PET (B) and both 18
F-FDG
PET and 18
F-DOPA PET(C).

Chapter 6
102
Figure 4 MTC patient with uptake on both 18
F-DOPA PET (left) and 18
F-FDG PET (right). On 18
F-DOPA-PET
lesions are seen in the right supraclavicular region, the right hemithorax and there is slight uptake subcarinal. In
the abdomen there are several lesions with faint uptake. Also on 18
F-FDG-PET uptake is seen in the right
supraclavicular region, right hemithorax and intensive uptake subcarinal. Furthermore several lesions are seen
in the liver region. Calcitonin and CEA levels were highly elevated (23236 ng/L (ref 0.3-12 ng/L) and 2144 ug/L
(ref 0.5-5.0 μg/L)) and calcitonin and CEA doubling times were short; 13 months and 12 months respectively.
The patient died 29 months after scans were performed due to progressive disease.
Discussion
In this study, 18F-FDG PET was superior to 18F-DOPA PET in identifying patients with
progressive disease. Unlike 18F-DOPA PET positivity, 18F-FDG PET positivity correlated
significantly with biochemical progressive disease. Furthermore, we showed that 18F-FDG
PET- and 18F-DOPA PET positive patients, had a significantly decreased survival. However,
univariate analysis in patients for whom both scans were performed showed that 18F-FDG
PET positivity had the most influence on survival. WBMTB analysis showed that metabolic
activity on 18F-DOPA PET correlated significantly with calcitonin and CEA levels.
Differences (>10%) in WBMTB on 18F-FDG PET and 18F-DOPA PET could not distinguish
stable from progressive disease.
In a previous study of our institute focusing on detecting residual disease with both 18F-
FDG PET and 18F-DOPA PET, we already described the superiority of 18F-FDG PET in 2

18F-FDG PET and
18F-DOPA PET in MTC
103
patients with progressive disease.16 This outcome is probably based on the fact that aggressive
(dedifferentiated) disease has a higher glucose metabolism and consequently higher 18F-FDG
uptake. This observation was also made by others but the described series are rather
small.14,15,17,18 Bogsrud et al. showed a higher mortality in 18F-FDG PET positive patients than
in 18F-FDG PET negative patients.24 However, survival data in patients with 18F-DOPA PET
have not been described before. This study shows that progressive patients can be identified
with both PET techniques, taking into account biochemical parameters and survival.
For 18F-FDG PET of patients with progressive MTC, not only have higher sensitivities
been described but also increased tracer intensity. Marzola et al. included only patients with
short doubling times (6-9 months) and showed significantly higher maximum SUV on 18F-
FDG PET versus 18F-DOPA PET, although patient- and lesion-based sensitivity of 18F-DOPA
PET was higher.18 In our WBMTB analysis, we did not find a significant difference in
doubling times between patients with a higher uptake on 18F-FDG PET and patients with a
higher uptake on 18F-DOPA PET. This lack of significance could have been caused by the
small number of patients with positive scan results in WBMTB analysis (n=11) or the
different doubling time cut-offs used for defining progressive disease.
Although the doubling times of calcitonin and CEA have thus far been the most reliable
indicators of recurrence and progressive disease in MTC, cut-off values are still a matter of
discussion. Meijer et al. showed a higher hazard ratio for recurrence for a calcitonin doubling
time cut-off of 12 months (hazard ratio, 5.33) than 24 months (hazard ratio, 2.93), but warned
about interpreting these cut-off values with caution.7 Moreover that study focuses on disease
recurrence and not progression in general. We based our 24 months cut-off for doubling times
on the results of the study by Giraudet et al., who compared doubling times with progression
according to the Response Evaluation Criteria in Solid Tumours (RECIST). They found
progressive disease in 94% of patients with doubling times less than 25 months while 86%
had stable disease when doubling times were more than 24 months.6
Our results show a significant correlation between WBMTB on 18F-DOPA PET and
calcitonin and CEA levels, demonstrating that 18F-DOPA PET might be a good indicator of
tumour load. Although 18F-FDG PET is better in distinguishing progressive disease, 18F-
DOPA PET seems to be more important in assessing the extent of residual disease. In our
WBMTB analysis, 18F-DOPA PET also detected more tumour lesions than did 18F-FDG PET.
On the whole, 18F-DOPA PET is superior to 18F-FDG PET with a higher patient-based
sensitivity (64% vs. 48%, respectively [range, 38%-83% vs. 17%-64%, respectively]) and
lesion-based sensitivity (72% vs 52%, respectively [range 52%-94% vs. 28%-62%]) (Table

Chapter 6
104
5).12-15,17,18 However, in line with the study of Kauhanen et al. and a recent review by Wong et
al., combining both modalities increases sensitivity and is complementary.14,25
Nevertheless, many patients with biochemical recurrent disease do not show lesions on
currently available imaging modalities. Most of these patients have moderately elevated
tumour markers and long doubling times, probably because of the nature of calcitonin-
producing metastases (sclerotic, necrotic or calcified) and their small size.26 A previous study
of our centre showed that MTC lesions are best detected on 18F -DOPA PET above >500 ng/L
and ROC curve analysis in the current study found a cut-off value of 825 ng/l to be optimal in
distinguishing 18F -DOPA PET-positive from -negative patients.16 This cut-off value is also
dependent on the resolution of the PET camera system, which with new developments
becomes increasingly sensitive. Also, the combination of PET with CT increases the yield of
these scans and lowers the threshold for localization of tumour lesions.27
The negative predictive value for biochemical progressive disease in our study was 88%
for 18F-FDG PET and 75% for 18F-DOPA PET. However, there are still patients - both in our
study (n=3) and in other series – who have rapidly increasing tumour markers but do not have
positive functional imaging results.18 In these patients, there is still need for other modalities
for the detection of occult MTC. Yet, the first results of new tracers like 68Ga-somatostatin
analogues or 11C-Methionine are not convincing.15,28,29
Table 5 Patient and lesion based sensitivity of 18F-FDG PET and 18F-DOPA PET. PET patient based sensitivity % (n) PET lesion based sensitivity % (n)
N 18
F-FDG 18
F-DOPA Combined Total no. of
lesions
18F-FDG
18F-DOPA
Hoegerle et al. 2001 11 64% (7) 64% (7) 73% (8) 27 44% (12) 63% (17)
Beuthien-Baumann et
al. 2007 15 47% (7) 47% (7) 60% (9) NA NA NA
Beheshti et al. 2009 26 58% (15) 81% (21) 85% (22) 53 62% (33) 94% (50)
Marzola et al. 2010 18 61% (11) 83% (15) 89% (16) 111 58% (64) 76% (84)
Kauhanen et al. 2011 19 53% (10) 58% (11) 63% (12) 118 47% (55) 52% (61)
Treglia et al. 2012 18 17% (3) 72% (13) 72% (13) 72 28% (20) 85% (61)
This study 21‡ 38% (8) 38% (8) 48% (10) 75 47% (35) 75% (56)
Total 128 48% (61) 64% (82) 70% (90) 456 48% (219) 72% (329)
*Average calcitonin, median not available. †Only 19 pts with data available.
‡Only patients included in WBMTB
analysis.

18F-FDG PET and
18F-DOPA PET in MTC
105
On the basis of the results of this and previous studies, we recommend a combined approach
for patients with recurrent MTC and increasing tumour markers (Figure 5). Conventional
imaging of the neck (ultrasound, MRI or CT) to detect localized disease can be followed by 18F-FDG PET or PET/CT to identify progressive disease. In the case of a negative 18F-FDG
PET result or the presence of only localized resectable disease (head and neck region), an 18F-
DOPA PET or PET/CT scan is recommended, to exclude distant metastasis and support the
decision for local surgery.
Figure 5 Flow-diagram for combined approach of 18
F-FDG PET and 18
F-DOPA PET in patients with recurrent
MTC and increasing tumour markers. If 18
F-FDG PET or 18
F-DOPA PET shows distant metastatic disease, targeted
therapy can be considered. If there is resectable localized disease on 18
F-FDG PET or 18
F-DOPA PET, with an
anatomical substrate, surgery could be considered. If both 18
F-FDG PET and 18
F-DOPA PET are negative, follow-
up would be appropriate.

Chapter 6
106
This study is limited by its retrospective character and the differences in 18F-FDG PET uptake
time, which can result in differences in the mean SUV. Most of our patients who were
included in the WBMTB analysis had an uptake time of 60 min (n=16). Because the WBMTB
for determination of tumour load depends not only on the mean SUV but also on tumour
volume and number of lesions we concluded that a slight difference in mean SUV does not
significantly influence our results. Furthermore, there could be a selection bias in patients
undergoing only 1 type of scan, or both scans. However, no significant difference existed in
patient characteristics (including doubling times) between these 2 groups (data not shown).
Other limitations are the small study size, which is often the case with rare tumours, and the
fact that not all PET lesions were histologically confirmed.
Conclusion
In MTC patients, 18F-FDG PET positivity seems to be associated with biochemical
progressive disease and significantly affects survival. 18F-DOPA PET has a higher sensitivity
than 18F-FDG PET, and WBMTB on 18F-DOPA PET can be related to the tumour load.
Therefore, 18F-DOPA PET seems to be more important in assessing the extent of the disease
in patients with residual disease whereas 18F-FDG PET can more accurately identify patients
with progressive disease. Both scans may be used to guide therapeutic strategies in patients
with recurrent MTC.

18F-FDG PET and
18F-DOPA PET in MTC
107
References
1. de Groot JW, Plukker JT, Wolffenbuttel BH, Wiggers T, Sluiter WJ, Links TP. Determinants of life
expectancy in medullary thyroid cancer: age does not matter. Clin Endocrinol (Oxf) 2006;65:729-736.
2. Kebebew E, Greenspan FS, Clark OH, Woeber KA, Grunwell J. Extent of disease and practice patterns
for medullary thyroid cancer. J Am Coll Surg 2005;200:890-896.
3. Roman S, Lin R, Sosa JA. Prognosis of medullary thyroid carcinoma: demographic, clinical, and
pathologic predictors of survival in 1252 cases. Cancer 2006;107:2134-2142.
4. Rendl G, Manzl M, Hitzl W, Sungler P, Pirich C. Long-term prognosis of medullary thyroid carcinoma.
Clin Endocrinol (Oxf) 2008;69:497-505.
5. Kebebew E, Ituarte PH, Siperstein AE, Duh QY, Clark OH. Medullary thyroid carcinoma: clinical
characteristics, treatment, prognostic factors, and a comparison of staging systems. Cancer
2000;88:1139-1148.
6. Giraudet AL, Al Ghulzan A, Auperin A, et al. Progression of medullary thyroid carcinoma: assessment
with calcitonin and carcinoembryonic antigen doubling times. Eur J Endocrinol 2008;158:239-246.
7. Meijer JA, le Cessie S, van den Hout WB, et al. Calcitonin and carcinoembryonic antigen doubling times
as prognostic factors in medullary thyroid carcinoma: a structured meta-analysis. Clin Endocrinol (Oxf)
2010;72:534-542.
8. Koopmans KP, Neels ON, Kema IP, et al. Molecular imaging in neuroendocrine tumors: molecular
uptake mechanisms and clinical results. Crit Rev Oncol Hematol 2009;71:199-213.
9. de Groot JW, Links TP, Jager PL, Kahraman T, Plukker JT. Impact of 18F-fluoro-2-deoxy-D-glucose
positron emission tomography (FDG-PET) in patients with biochemical evidence of recurrent or
residual medullary thyroid cancer. Ann Surg Oncol 2004;11:786-794.
10. Iagaru A, Masamed R, Singer PA, Conti PS. Detection of occult medullary thyroid cancer recurrence
with 2-deoxy-2-[F-18]fluoro-D-glucose-PET and PET/CT. Mol Imaging Biol 2007;9:72-77.
11. Rubello D, Rampin L, Nanni C, et al. The role of 18F-FDG PET/CT in detecting metastatic deposits of
recurrent medullary thyroid carcinoma: a prospective study. Eur J Surg Oncol 2008;34:581-586.
12. Hoegerle S, Altehoefer C, Ghanem N, Brink I, Moser E, Nitzsche E. 18F-DOPA positron emission
tomography for tumour detection in patients with medullary thyroid carcinoma and elevated
calcitonin levels. Eur J Nucl Med 2001;28:64-71.
13. Beuthien-Baumann B, Strumpf A, Zessin J, Bredow J, Kotzerke J. Diagnostic impact of PET with 18F-
FDG, 18F-DOPA and 3-O-methyl-6-[18F]fluoro-DOPA in recurrent or metastatic medullary thyroid
carcinoma. Eur J Nucl Med Mol Imaging 2007;34:1604-1609.
14. Kauhanen S, Schalin-Jantti C, Seppanen M, et al. Complementary Roles of 18F-DOPA PET/CT and 18F-
FDG PET/CT in Medullary Thyroid Cancer. J Nucl Med 2011;52:1855-1863.
15. Treglia G, Castaldi P, Villani MF, et al. Comparison of (18)F-DOPA, (18)F-FDG and (68)Ga-somatostatin
analogue PET/CT in patients with recurrent medullary thyroid carcinoma. Eur J Nucl Med Mol Imaging
2012:569-580.
16. Koopmans KP, de Groot JW, Plukker JT, et al. 18F-dihydroxyphenylalanine PET in patients with
biochemical evidence of medullary thyroid cancer: relation to tumor differentiation. J Nucl Med
2008;49:524-531.
17. Beheshti M, Pocher S, Vali R, et al. The value of 18F-DOPA PET-CT in patients with medullary thyroid
carcinoma: comparison with 18F-FDG PET-CT. Eur Radiol 2009;19:1425-1434.
18. Marzola MC, Pelizzo MR, Ferdeghini M, et al. Dual PET/CT with (18)F-DOPA and (18)F-FDG in
metastatic medullary thyroid carcinoma and rapidly increasing calcitonin levels: Comparison with
conventional imaging. Eur J Surg Oncol 2010;36:414-421.
19. Fiebrich HB, de Jong JR, Kema IP, et al. Total (18)F-dopa PET tumour uptake reflects metabolic
endocrine tumour activity in patients with a carcinoid tumour. Eur J Nucl Med Mol Imaging
2011;38:1854-1861.
20. de Vries EFJ, Luurtsema G, Brüssermann M, Elsinga PH, Vaalburg W. Fully automated synthesis module
for the high yield one-pot preparation of 6-[18F]fluoro--DOPA. Applied Radiation and Isotopes
1999;51:389-394.
21. Jentzen W, Freudenberg L, Eising EG, Heinze M, Brandau W, Bockisch A. Segmentation of PET volumes
by iterative image thresholding. J Nucl Med 2007;48:108-114.

Chapter 6
108
22. Erdi YE, Mawlawi O, Larson SM, et al. Segmentation of lung lesion volume by adaptive positron
emission tomography image thresholding. Cancer 1997;80:2505-2509.
23. Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer: management guidelines of the American
Thyroid Association. Thyroid 2009;19:565-612.
24. Bogsrud TV, Karantanis D, Nathan MA, et al. The prognostic value of 2-deoxy-2-[18F]fluoro-D-glucose
positron emission tomography in patients with suspected residual or recurrent medullary thyroid
carcinoma. Mol Imaging Biol 2010;12:547-553.
25. Wong KK, Laird AM, Moubayed A, et al. How has the management of medullary thyroid carcinoma
changed with the advent of 18F-FDG and non-18F-FDG PET radiopharmaceuticals. Nucl Med Commun
2012.
26. Giraudet AL, Vanel D, Leboulleux S, et al. Imaging medullary thyroid carcinoma with persistent
elevated calcitonin levels. J Clin Endocrinol Metab 2007;92:4185-4190.
27. Luster M, Karges W, Zeich K, et al. Clinical value of 18-fluorine-fluorodihydroxyphenylalanine positron
emission tomography/computed tomography in the follow-up of medullary thyroid carcinoma.
Thyroid 2010;20:527-533.
28. Jang HW, Choi JY, Lee JI, et al. Localization of medullary thyroid carcinoma after surgery using (11)C-
methionine PET/CT: comparison with (18)F-FDG PET/CT. Endocr J 2010;57:1045-1054.
29. Conry BG, Papathanasiou ND, Prakash V, et al. Comparison of (68)Ga-DOTATATE and (18)F-
fluorodeoxyglucose PET/CT in the detection of recurrent medullary thyroid carcinoma. Eur J Nucl Med
Mol Imaging 2010;37:49-57.

Chapter 7
The effects of four different tyrosine kinase inhibitors
on medullary and papillary thyroid cancer cells
Hans H. G. Verbeek*, Maria M. Alves*, Jan Willem B. de Groot, Jan Osinga
John T. M. Plukker, Thera P. Links, Robert M. W. Hofstra
*The first two authors contributed equally to this study
J Clin Endocrinol Metab. 2011; 96: E991-5

Chapter 7
110
Abstract
Context Medullary and papillary thyroid carcinoma (MTC and PTC) are two types of thyroid
cancer that can originate from activating mutations or rearrangements in the RET gene.
Therapeutic options are limited in recurrent disease, but because RET is a tyrosine kinase
(TK) receptor involved in cellular growth and proliferation, treatment with a TK inhibitor
might be promising. Several TK inhibitors have been tested in clinical trials, but it is unknown
which inhibitor is most effective and whether there is any specificity for particular RET
mutations.
Objective We aimed to compare the effect of four TK inhibitors (axitinib, sunitinib,
vandetanib, and XL184 (cabozantinib)) on cell proliferation, RET expression and
autophosphorylation, and ERK activation in cell lines expressing a MEN2A (MTC-TT), a
MEN2B (MZ-CRC-1) mutation, and a RET/PTC (TPC-1) rearrangement.
Design The three cell lines were cultured and treated with the four TK inhibitors. Effects on
cell proliferation and RET and ERK expression and activation were determined.
Results XL184 and vandetanib most effectively inhibited cell proliferation, RET
autophosphorylation in combination with a reduction of RET expression, and ERK
phosphorylation in MTC-TT and MZ-CRC-1, respectively. TPC-1 cells showed a decrease in
RET autophosphorylation after treatment with XL184, but no effect was observed on ERK
activation.
Conclusion There is indeed specificity for different RET mutations, with XL184 being the
most potent inhibitor in MEN2A and PTC and vandetanib the most effective in MEN2B in
vitro. No TK inhibitor was superior for all the cell lines tested, indicating that mutation-
specific therapies could be beneficial in treating MTC and PTC.

Effects of TK inhibitors on MTC and PTC cells
111
Introduction
Medullary thyroid carcinoma (MTC) and papillary thyroid carcinoma (PTC) can be caused by
activating mutations or rearrangements of the rearranged during transfection (RET) gene.
MTC originates from the calcitonin-producing C cells of the thyroid and can occur
sporadically (75%) or as part of a familial cancer syndrome (25%). The latter occurs as
multiple endocrine neoplasia (MEN) type 2 syndrome (MEN2A and MEN2B) or as familial
MTC.1-3 PTC is the most common thyroid cancer (80% of all thyroid cancers) and originates
from the follicular epithelial cells of the thyroid. In 2.5%–40% of PTC, a RET rearrangement
is found, although this percentage is higher in patients exposed to radiation.1
Total thyroidectomy and extensive lymph node dissection is the curative treatment for
MTC and PTC, followed by radioiodine ablation in PTC. However, recurrent disease is often
seen in sporadic MTC, and until recently, reoperation was the only therapeutic option. In
iodine-refractory PTC, no effective adjuvant therapy is available as well.4,5 New systemic
therapies are therefore needed for both recurrent MTC and PTC.
With RET being the gene involved in a subset of MTC and PTC, it is logical to consider
the encoded receptor as an important target for systemic therapy. RET is expressed in all
tumour cells and continuous autophosphorylation on its tyrosine kinase (TK) residues caused
by mutations (MEN2) or rearrangements (PTC) on RET results in a constant activation of
downstream signalling pathways that ultimately lead to tumour growth.1 Therefore, inhibition
of RET phosphorylation and its downstream pathways could be of great value.
Small-molecule inhibitors that selectively inhibit TK have been proven to be effective in
the treatment of several neoplastic diseases.6-8 A number of these clinically useful inhibitors
target TK receptors that belong to the same family group of proteins as RET.9 Several TK
inhibitors have already been tested in vitro and evaluated in phase II clinical trials (Table 1).
In a large number of patients (25%–81%), a stable disease state can be established, and some
patients even show a partial response (2%–33%).10-19
Because most studies have focused on one particular TK inhibitor and have not looked for
mutation specificity, it is hard to compare these compounds for the different patient groups.
We therefore set out to compare the efficiency of four recently developed TK inhibitors,
XL184 (cabozantinib), vandetanib, sunitinib, and axitinib, using three cell lines: MTC-TT
reported to be derived from a sporadic MTC expressing a C634W RET mutation, MZ-CRC-1

Chapter 7
112
derived from a patient with metastatic sporadic MTC expressing an M918T RET mutation,
and TPC-1 derived from a patient with PTC expressing a RET/PTC-1 rearrangement.
Table 1 Molecular targets and clinical trials performed with tyrosine kinase inhibitors in
medullary thyroid carcinoma (MTC) patients.
Molecular targets No. of
patients
Tumor response
% (n)
Stable disease
% (n)
Ref.
Imatinib
Bcr-Abl, PDGFR α
and β, c-Fms, c-Kit,
RET
24 0 38 (9) 10,11
Sorafenib
RAF, VEGFR2 and 3,
PDGFR, RET
21 10 (2) 86 (18) 12
Motesanib VEGFR 1, 2, and 3,
PDGFR, c-Kit, RET
91 2 (2) 81 (74)
13
Gefitinib* EGFR 4 0 0 14
Vandetanib
VEGFR, EGFR, RET 30
19
20 (6)
16 (3)
53 (16)
53 (10)
15
16
Axitinib
VEGFR 1, 2, and 3, 11 18 (2) 27 (3) 17
Sunitinib*
RET, VEGFR, PDGFR
6 0 83 (5) 18
XL184#
MET, VEGFR-2, RET 37 (35 with
measurable disease)
29 (10) 41 (15) 19
* Clinical trial performed in advanced thyroid cancer patients, not only MTC patients;
# Phase 1 trial.
Materials and Methods
Cell culture
MZ-CRC-1, MTC-TT, TPC-1, and HEK293 (human embryonic kidney cells) cell lines were
cultured as described in Supplemental Materials and Methods.
Tyrosine kinase inhibitors
XL184 (Exelixis, San Francisco, CA), vandetanib (AstraZeneca, Zoetermeer, The
Netherlands), and sunitinib and axitinib (Pfizer, Capelle a/d IJssel, The Netherlands) were
made up as a stock solution of 10 mM in dimethylsulfoxide (DMSO).
Cell proliferation assays
MTC-TT and MZ-CRC-1cells were plated in 200 µl medium at concentrations of 4 × 104 cells
per well. TPC-1 and HEK293 cells were plated at a density of 2 × 103 cells per well. After
overnight incubation, increasing concentrations of TK inhibitor solutions (0, 0.005, 0.05, 0.1,

Effects of TK inhibitors on MTC and PTC cells
113
0.5, and 5 µM) were added. A concentration of 0.1% DMSO was used in all experiments.
Control cells were grown without DMSO or TK inhibitor. Proliferation was measured at 1, 4,
and 7 d using a cell proliferation kit (MTT assay; Roche, Almere, The Netherlands) according
to the manufacturer’s instructions. The concentration that led to 50% growth inhibition (IC50)
was determined using linear interpolation at r=0.5 (Supplemental Table 1). If IC50
concentrations were between 0.5 and 5 µM, additional cell proliferation assays were
performed (Supplemental Figure 1, A–D). All experiments were performed in triplicate.
Cell lysates and Western blot analysis
MZ-CRC-1, MTC-TT, and TPC-1 cells were treated with 0, IC50, and maximal
concentrations of the different TK inhibitors for 0, 2, and 5 d. Cell lysates were prepared as
described in Supplemental Materials and Methods, and supernatants were stored at -80C
before they were further processed for SDS-PAGE followed by Western blot analysis. The
antibodies used are described in Supplemental Materials and Methods. All experiments were
performed in duplicate.
RNA extraction and RT-PCR
MTC-TT and MZ-CRC-1 cells, treated with 0, IC50, and maximal concentrations
(Supplemental Table 1) of XL184 and vandetanib, respectively, were collected after 0, 2, and
5 d. RNA extraction and RT-PCR procedures are described in the Supplemental Materials and
Methods.
Statistical analysis
The statistical analysis was performed using the software program SPSS version 16.0.
Results
Effect of different TK inhibitors on cell proliferation
A dose-dependent decrease in cell proliferations was seen for all four inhibitors (Figure 1, A–
C, and Supplemental Figure 1, A–D). In contrast, HEK293 cells, who do not endogenously
express RET, showed only minor effects on proliferation at concentrations lower than 0.5 µM
(Supplemental Figure 2A). Based on the IC50 values (Supplemental Figure 2B and

Chapter 7
114
Supplemental Table 1), we observed that XL184 was the most effective inhibitor of MTC-TT
(IC50=0.04 µM) and TPC-1 (IC50=0.06 µM) proliferation, whereas for MZ-CRC-1,
vandetanib inhibited cell proliferation at the lowest concentration (IC50=0.26 µM). DMSO
did not seem to have a significant negative effect on cell growth of any of the cell lines tested
(Supplemental Table 2).
Effect of XL184 and vandetanib on RET autophosphorylation
Inhibition of RET autophosphorylation on tyrosine 1062 was observed for the three cell lines
tested after 2 d of treatment with XL184 (MTC-TT and TPC-1) and vandetanib (MZ-CRC-1).
However, only vandetanib was able to induce this effect with IC50 levels (Figure 1D). For
MTC-TT and TPC-1, 5 d exposure to IC50 concentrations of XL184 were necessary to reduce
RET autophosphorylation levels (Figure 1, E and F). To investigate whether the decrease in
RET autophosphorylation was due to reduced levels of RET expression, the membranes were
stripped and probed for RET. MTC-TT and MZ-CRC-1 cells showed a dose-dependent
response after 5 d incubation with XL184 and vandetanib, respectively. At IC50 values, a
marked decreased in RET expression was observed, and at maximal concentrations, RET was
no longer detectable (Figure 1, D and F). To determine whether this effect was due to
inhibition of RET transcription, RET expression levels were determined. For MTC-TT, no
effect on RET transcription levels was observed. However, for MZ-CRC-1, 5 d exposure to
maximal concentrations of vandetanib led to a decrease in RET expression (Supplemental
Figure 3, A–C). For TPC-1 cells, the total amount of RET remained relatively unchanged
even after 5 d exposure to maximal concentrations of XL184 (Figure 1F).
Effect of XL184 and vandetanib on RET downstream signalling pathways
RET is involved in the activation of several signalling pathways, including the MAPK
pathway.20 Therefore, we evaluated the effect of XL184 and vandetanib in ERK activation.
For MTC-TT and MZ-CRC-1, ERK phosphorylation was markedly reduced with IC50 levels
of XL184 and vandetanib, respectively, and was totally inhibited when maximal
concentrations were used (Figure 1, D and E). However, XL184 was able to exert this effect
after only 2 d exposure. Interestingly, this reduction of ERK activation was related to a
decrease in ERK expression (Figure 1, D and E). For TPC-1, no effect on ERK expression
and activation was observed, even when maximal concentrations of XL184 were used (Figure
1F).

Effects of TK inhibitors on MTC and PTC cells
115
Figure 1 Effect of XL184, vandetanib, sunitinib, and axitinib on cell proliferation. A–C, Dose-response curves
of MZ-CRC-1 (A), MTC-TT (B), and TPC-1 (C) cell lines incubated with different concentrations of XL184,
vandetanib, sunitinib, and axitinib; D–F, effect of XL184 and vandetanib on RET expression, RET
autophosphorylation, ERK expression, and ERK phosphorylation: MZ-CRC-1 cells treated with IC50
concentration and 5 μM vandetanib for 2 and 5 d (D), MTC-TT (E), and TPC-1 (F) cells treated with IC50
concentration and 5 μM XL184 for 2 and 5 d. Error bars shown correspond to SD.
Discussion
We compared the effects of four TK inhibitors, XL184, vandetanib, sunitinib, and axitinib, on
cell proliferation and RET inhibition and looked for mutation specificity using cell lines
harbouring a MEN2A mutation (MTC-TT), a MEN2B mutation (MZ-CRC-1), and a
RET/PTC rearrangement (TPC-1). Our results showed that all four TK inhibitors are capable
of reducing cell proliferation to some extent. However, XL184 was found to be the most
efficient inhibitor for MEN2A and PTC-derived cell lines, whereas vandetanib proved to be
the most potent inhibitor for MEN2B.

Chapter 7
116
We also showed that XL184 and vandetanib were able to decrease RET
autophosphorylation and expression levels in MTC-TT and MZ-CRC-1 cells, respectively.
However, only vandetanib exerted this effect by inhibiting RET transcription. It is possible
that for XL184, lysosomal or proteasomal degradation is involved, as was described for other
inhibitors.20 For TPC-1 a marked decrease in RET phosphorylation levels was detected, but
surprisingly, RET/PTC expression levels increased after exposure to XL184. This dual effect
might be the result of a negative feedback mechanism to compensate a reduction in RET
activation. Furthermore, it shows that XL184 exerts its effect in PTC by direct inhibition of
RET autophosphorylation and that lysosomal or proteasomal degradation may not be effective
due to the presence of the fusion protein.
Finally, we explored the effect of these drugs in a downstream signalling pathway directly
activated by RET, the MAPK pathway. For MTC-TT and MZ-CRC-1, exposure to XL184
and vandetanib, respectively, induced a marked decrease in ERK phosphorylation.
Interestingly, a reduction on ERK expression was also observed for these cell lines,
suggesting a possible effect of XL184 and vandetanib on ERK transcription. For the TPC-1
PTC model system, no change in ERK phosphorylation was detected after exposure to
XL184. ERK phosphorylation through other TK receptors and TK effector molecules, e.g.
BRAF, are likely to exert a stronger effect in ERK phosphorylation than RET. It is possible
that for PTC, a combination of different inhibitors targeting RET and, e.g. BRAF
(serine/threonine-protein kinase B-Raf), could circumvent this problem and thus result in an
even more effective treatment for this type of cancer.
Because no TK inhibitor was superior for the cell lines tested, our in vitro results suggest
that mutation-specific therapies could be beneficial for the treatment of MTC and PTC.
However, because only three different mutations were analysed, additional mutational studies
are necessary to confirm this specificity.
To date, no distinction has been made between the different RET-related mutational
subtypes (MEN2A/MEN2B/PTC) in clinical trials, and it is known that aspecific targeting of
TK inhibitors can also contribute to antitumor effects. However, the risk of severe side effects
for the patients in combination with the development of resistance to the TK inhibitors
incorrectly used reinforces the need of mutation specific therapies. Furthermore, the combined
use of different TK inhibitors for multiple targeting will also benefit from this knowledge,
because only then optimal combinations of inhibitors can be chosen.
In conclusion, our results are in general agreement with the outcome of the clinical trials,
supporting the idea that XL184 and vandetanib are two potent inhibitors for tumour response

Effects of TK inhibitors on MTC and PTC cells
117
in MTC. We also showed that there is specificity of these inhibitors for the treatment of
different RET mutations, which suggest that mutation-specific therapies will likely improve
the outcome of ongoing studies. Thus, reanalysis of already performed trials based on
mutation status is more than worthwhile.
Acknowledgments
We thank Exelixis, AstraZeneca, and Pfizer for providing the TK inhibitors for investigation
and Jackie Senior for editing the manuscript.

Chapter 7
118
References
1. de Groot JW, Links TP, Plukker JT, Lips CJ, Hofstra RM. RET as a diagnostic and therapeutic target in
sporadic and hereditary endocrine tumors. Endocr Rev 2006;27:535-560.
2. Hofstra RM, Landsvater RM, Ceccherini I, et al. A mutation in the RET proto-oncogene associated with
multiple endocrine neoplasia type 2B and sporadic medullary thyroid carcinoma. Nature
1994;367:375-376.
3. Eng C, Mulligan LM. Mutations of the RET proto-oncogene in the multiple endocrine neoplasia type 2
syndromes, related sporadic tumours, and hirschsprung disease. Hum Mutat 1997;9:97-109.
4. Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer: management guidelines of the American
Thyroid Association. Thyroid 2009;19:565-612.
5. Cooper DS, Doherty GM, Haugen BR, et al. Management guidelines for patients with thyroid nodules
and differentiated thyroid cancer. Thyroid 2006;16:109-142.
6. Druker BJ, Talpaz M, Resta DJ, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine
kinase in chronic myeloid leukemia. N Engl J Med 2001;344:1031-1037.
7. Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced
gastrointestinal stromal tumors. N Engl J Med 2002;347:472-480.
8. McArthur GA, Demetri GD, van Oosterom A, et al. Molecular and clinical analysis of locally advanced
dermatofibrosarcoma protuberans treated with imatinib: Imatinib Target Exploration Consortium
Study B2225. J Clin Oncol 2005;23:866-873.
9. Ye L, Santarpia L, Gagel RF. The evolving field of tyrosine kinase inhibitors in the treatment of
endocrine tumors. Endocr Rev 2010;31:578-599.
10. de Groot JW, Zonnenberg BA, van Ufford-Mannesse PQ, et al. A phase II trial of imatinib therapy for
metastatic medullary thyroid carcinoma. J Clin Endocrinol Metab 2007;92:3466-3469.
11. Frank-Raue K, Fabel M, Delorme S, Haberkorn U, Raue F. Efficacy of imatinib mesylate in advanced
medullary thyroid carcinoma. Eur J Endocrinol 2007;157:215-220.
12. Lam ET, Ringel MD, Kloos RT, et al. Phase II clinical trial of sorafenib in metastatic medullary thyroid
cancer. J Clin Oncol 2010;28:2323-2330.
13. Schlumberger MJ, Elisei R, Bastholt L, et al. Phase II study of safety and efficacy of motesanib in
patients with progressive or symptomatic, advanced or metastatic medullary thyroid cancer. J Clin
Oncol 2009;27:3794-3801.
14. Pennell NA, Daniels GH, Haddad RI, et al. A phase II study of gefitinib in patients with advanced thyroid
cancer. Thyroid 2008;18:317-323.
15. Wells SA,Jr, Gosnell JE, Gagel RF, et al. Vandetanib for the treatment of patients with locally advanced
or metastatic hereditary medullary thyroid cancer. J Clin Oncol 2010;28:767-772.
16. Robinson BG, Paz-Ares L, Krebs A, Vasselli J, Haddad R. Vandetanib (100 mg) in patients with locally
advanced or metastatic hereditary medullary thyroid cancer. J Clin Endocrinol Metab 2010;95:2664-
2671.
17. Cohen EE, Rosen LS, Vokes EE, et al. Axitinib is an active treatment for all histologic subtypes of
advanced thyroid cancer: results from a phase II study. J Clin Oncol 2008;26:4708-4713.
18. Cohen EE, Needles BM, Cullen KJ, et al. Phase 2 study of sunitinib in refractory thyroid cancer. Journal
of Clinical Oncology 2008;26.
19. Kurzrock R, Sherman S, Hong D, et al. A phase 1 study of XL184, a MET, VEGFR2, and RET kinase
inhibitor, administered orally to patients (pts) with advanced malignancies, including a subgroup of pts
with medullary thryoid cancer (MTC). EORTC 2008:119.
20. Plaza-Menacho I, Mologni L, Sala E, et al. Sorafenib functions to potently suppress RET tyrosine kinase
activity by direct enzymatic inhibition and promoting RET lysosomal degradation independent of
proteasomal targeting. J Biol Chem 2007;282:29230-29240.

Effects of TK inhibitors on MTC and PTC cells
119
Supplementary data
Materials and Methods
Cell culture
MTC-TT and TPC-1 cell lines were cultured in RPMI medium (Gibco, Breda, The
Netherlands) supplemented with 15% or 10% (for TPC-1) fetal bovine serum (FBS,
BioWhittaker, Lonza,Verviers, Belgium), 1% L-glutamine (Gibco) and 1% penicillin/strepto-
mycin (Gibco). MZ-CRC-1 and HEK293 cell lines were cultured in DMEM high medium
containing 4.5 g/L of glucose, L-glutamine and pyruvate (Gibco), supplemented with 15% or
10% (for HEK293) FBS and 1% penicillin/streptomycin. All cells were maintained at 37°C
and 5% CO2 atmosphere.
Cell lysates and Western blot analysis
Cells were washed with ice-cold PBS and incubated with lysis buffer (m-PER, Thermo Fisher
Scientific, Rockford, IL, USA) containing protease (Thermo Fisher Scientific) and
phosphatase (Thermo Fisher Scientific) inhibitors, for 30 min on ice. Cell lysates were
collected by scraping and cleared by centrifugation at 14,000 rpm for 10 min in a pre-cooled
(4°C) centrifuge.
The following antibodies were used for Western blot: RET (H-300), RET (C-19), p-RET
(Y1062) (Santa Cruz Biotechnology, Heidelberg, Germany); ERK, p-ERK (Cell Signaling,
Danvers, MA, USA) and actin (C4, MP Biomedicals, Illkirch, France). Secondary antibodies
used were goat anti-rabbit IgG-HRP (Bio-Rad, Veenendaal, The Netherlands) and goat anti-
mouse IgG-HRP (Bio-Rad). All the experiments were performed in duplicates.
RNA extraction and RT-PCR
Cells were washed with PBS (Gibco) and RNA extraction was performed using the RNeasy
mini kit© (Qiagen, Venlo, The Netherlands). First strand cDNA was originated using the
Ready-To-Go You-Prime First-Strand Beads© kit (GE Healthcare, Zeist, The Netherlands)
according to the manufacturer’s instructions. The following primers were used: RET forward
(5’-CCGTGAAGATGCTGAAAGAG-3’); RET reverse (5’-
AGAGGCCGTCGTCATAAATC-3’); GAPDH forward (5’-

Chapter 7
120
TGAAGGTCGGAGTCAACGGATTTGGT-3’); GAPDH reverse (5’-
GCAGAGATGATGACCCTTTTGGCTC -3’).

Effects of TK inhibitors on MTC and PTC cells
121
Supplementary Tables
Supplementary Table 1 IC50 concentrations of the different TK inhibitors
in different cell lines
Cell-line
Compound MTC-TT MZ-CRC TPC-1
Sunitinib
0.78 + 0.19 μM 0.71 + 0.15 μM 0.37 + 0.03 μM
Vandetanib
0.47 + 0.33 μM 0.26 + 0.07 μM 0.41 + 0.09 μM
Axitinib
1.56 + 0.04 μM > 5 μM 1.14 + 0.03 μM
XL184
0.04 + 0.03 μM > 5 μM 0.06 + 0.02 μM
MTC-TT cells express a MEN2A mutation, MZ-CRC-1 cells express a MEN2B mutation,
and TPC-1 cells express a RET/PTC rearrangement.
Supplementary Table 2 Effect of DMSO on cell proliferation of MZ-CRC-1, MTC-TT and TPC-1
Cell proliferation
Sign. Control (SD) 0 concentration (SD)
MZ-CRC-1 104.7% (10.2%) 100% (7.0%) 0.35 (NS)
MTC-TT 94.2% (18.4%) 100% (14.5%) 0.11 (NS)
TPC-1 100.3% (10.4%) 100% (12.1%) 0.93 (NS)
Control cells were grown without DMSO or inhibitors, cells in the “0”condition were grown without inhibitors
but in the presence of 0.1% DMSO.

Chapter 7
122
Supplementary Figures
Supplementary Figure 1 Additional dose response curves for (A) MTC-TT cells treated with sunitinib, (B)
MTC-TT cells treated with axitinib, (C) MZ-CRC-1 cells treated with sunitinib and (D) TPC-1 cells treated with
axitinb.

Effects of TK inhibitors on MTC and PTC cells
123
Supplementary Figure 2 (A) Dose response curves for HEK293 cell line incubated with different
concentrations of XL184, vandetanib, sunitinib and axitinib. (B) Overview of the IC50 values (the concentration
that lead to 50% cell death) of the four tyrosine kinase inhibitors for MTC-TT, MZ-CRC-1 and TPC-1 cell lines.
Error bars shown correspond to standard deviation. * Concentrations are above 5 µM.

Chapter 7
124
Supplementary Figure 3 Effects of XL184 and vandetanib on RET mRNA levels. (A) MTC-TT cells treated
with IC50 concentration and 5 µM of XL184 showed no effect on RET transcription levels. (B) MZ-CRC-1 cells
treated with IC50 concentration and 5 µM of vandetanib showed a decrease in RET transcription levels after
prolonged exposure (5 days) to 5 µM of this inhibitor. (C) Graphical representation of RET bands’ intensity after
correction for GAPDH levels confirmed a reduction of RET mRNA levels for MZ-CRC-1 cells after prolonged
exposure to 5 µM of vandetanib. MTC-TT cells express a MEN2A mutation (RET C634R) and MZ-CRC-1 cells
express a MEN2B mutation (RET M918T). IC50 = concentration that leads to 50% cell death. GAPDH was used
as an internal control.

Chapter 8
Summary, discussion and future perspectives

Chapter 8
126
Summary
Medullary thyroid carcinoma (MTC) arises from the parafollicular C-cells and accounts for
approximately 5% of all thyroid cancers.1 MTC occurs sporadically (75%) or in a familial
form as part of one of the inherited syndromes known as familial MTC (FMTC) and Multiple
Endocrine Neoplasia type 2 (MEN 2). A MEN2A and MEN2B variant of the syndrome are
discerned and mutations in the ‘REarranged during Transfection’ (RET) gene are responsible
for these syndromes. Other manifestations of the MEN2 syndromes include
pheochromocytoma (MEN 2A and 2B) and hyperparathyroidism (MEN2A) or
neurofibromatosis (MEN2B).2
At presentation most MTC patients have an asymptomatic palpable solitary thyroid nodule
or palpable lymph node(s). Fifty percent of the patients have lymph node metastasis and 10%
will have distant metastasis at the time of diagnosis.3,4 Usually, the first diagnostic procedure
for thyroid nodules is fine needle aspiration cytology (FNAC) with ultrasound guidance.
However, without the use of specific immunohistochemical analyses, the sensitivity of this
procedure for detecting MTC is limited.5 As MTC originates from the calcitonin producing C-
cells, this hormone may also be used as a screening tool in patients with thyroid nodules to
detect MTC in an early stage of the disease. This application is a matter of discussion as a
proportionate number of patients has an elevated calcitonin caused by other conditions than
MTC.6,7
The initial treatment of patients with sporadic MTC without identified metastases consists
of a total thyroidectomy with an elective lymphadenectomy of regional lymph nodes in the
central compartment (level VI) (central compartment dissection (CCD)), according to the
current American Thyroid Association (ATA) guidelines. If the disease has already spread to
the lateral lymph nodes of the neck, a modified radical uni- or bilateral dissection of the
lateral lymph nodes (levels II-V) (lateral node dissection (LND)) is also indicated.8 As
surgery offers the only chance on cure, some surgeons not only perform an elective CCD, but
also an elective LND because of a relative risk of nodal (micro) metastases. A considerable
number of MTC patients (>50%) are beyond cure, because the disease has been so broadly
metastasized, even when MTC presented as a locoregional disease.9,10 Unlike other types of
thyroid cancer, MTC patients will not benefit from adjuvant radioactive iodine treatment.11
Therefore, adequate surgery in MTC is of crucial importance for optimal locoregional control
and potential cure.

Summary, discussion and future perspectives
127
Although more than 50% of MTC patients cannot be cured despite extensive surgery, many
patients with minimal residual disease have a good life expectancy.12,13 To monitor disease
progression, careful follow-up, consisting of regular determinations of the tumour markers
calcitonin and carcinoembryonic antigen (CEA) is important.14 If these tumour markers are
increasing, diagnostic work-up with morphological and functional imaging (including
Positron Emission Tomography (PET)) is advocated. Calcitonin and CEA doubling times are
currently the most reliable markers for progression, but accurate determination requires serial
measurements which are time consuming. Early detection of progression may be important,
because appropriate therapeutic interventions may delay symptomatic deterioration.
Depending on the extent of the disease, based on imaging and the rate of elevation of tumour
markers, several therapeutic strategies can be considered; a ‘wait and see’ approach with close
monitoring, surgical intervention (for locoregional control) or treatment with systemic
(targeted) therapy.
Chemotherapy has not yet been proven to be effective in the palliative treatment of MTC.
Recent preclinical and clinical research involving tyrosine kinase (TK) inhibitors, have shown
an improvement of the progression free survival in MTC patients.15,16 However, it is unknown
whether the effectiveness of these inhibitors is dependent on the somatic or germ line RET
mutation of the tumour or patient. Different RET mutations give rise to different
configurationally changes of the RET protein.17 For instance, the mostly found mutation
found in sporadic MTC, the ’MEN2B mutation’, changes the ATP pocket of the RET protein,
to which these inhibitors bind. We therefore speculate that selecting patients based on specific
RET mutations may increase the effectiveness of targeted therapy. Furthermore, most TK
inhibitors have several targets activating multiple pathways, which can cause, next to tumour
regression, also side-effects such as cardiac toxicity or hand-foot syndrome.18,19 Therefore,
careful selection of patients is important in which mutation specific therapy can be of value.
This thesis covers several important clinical issues in the diagnosis and treatment of primary
and recurrent (inherited) MTC. The aim of this thesis was to evaluate and to improve both
diagnostic and therapeutic modalities in the treatment of patients with MTC by: (1)
Addressing the value of calcitonin testing for detection of MTC in patients with thyroid
nodules; (2) Evaluating the recommendations regarding surgical treatment by the current
ATA guidelines for MTC patients; (3) Investigating the value of 18F-FDG PET and 18F-
DOPA PET for detection progressive recurrent MTC and (4) Evaluating different tyrosine
kinase inhibitors for treatment of MTC.

Chapter 8
128
In Chapter 1 a general introduction and the aims and outlines of this thesis are presented.
In Chapter 2 three patients with different stages of disease were presented to illustrate the
variety in clinical presentation and behaviour of MTC. Based on these patients a short
overview of the presentation, diagnosis, treatment and follow-up of MTC was provided.
In Chapter 3 the diagnostic accuracy of the calcitonin test for detection of MTC in patients
with thyroid nodules was evaluated. MTC patients detected in an early stage of the disease
have a better prognosis, so early detection of MTC in patients with thyroid nodules can be
beneficial. As almost all MTC’s secrete calcitonin, standard determination of calcitonin may
detect these tumours in patients with thyroid nodules. However, no consensus exists whether
or not to perform routine calcitonin testing in patients with thyroid nodules. A meta-analysis
was performed to evaluate the diagnostic accuracy of the calcitonin test. Sixteen studies were
eventually included. Summary estimates for different cut-off values were determined.
Sensitivity was high for lower basal cut-off values and combined basal and stimulated
calcitonin testing. Specificity did slightly increase with higher cut-off values and stimulated
testing. Overall, the diagnostic accuracy of calcitonin testing was high. However, for the
interpretation of this accuracy, the low prevalence of MTC has also to be taken into account.
The rarity of MTC decreases the positive predictive value and thereby the clinical
applicability of routine calcitonin testing for the detection of MTC. The low positive
predictive value carries the risk of patients being operated unnecessary. Moreover, the cost-
effectiveness of calcitonin screening for the early detection of MTC is still a matter of
discussion following the overall low prevalence of MTC.
In Chapter 4 we investigated, whether the current American Thyroid Association (ATA)
recommendations are of clinical benefit for MTC patients with respect to the surgical
treatment. No evidence exists for the optimal surgical treatment, especially with regard to the
extent of the lateral lymph node dissection (LND). Therefore, different surgical strategies are
advocated by experts and guidelines. The ATA guidelines recommend total thyroidectomy
and LND of the central compartment (level VI) as the initial treatment.8 In case of regional
node involvement, systematic LND of the lateral compartments (level II – V) should be
performed. Retrospectively, we reviewed the surgical and pathology reports of 86 patients and
compared the clinical outcome (reoperations, biochemical cure, survival and complications)
of the patients treated by ATA-compliant surgery versus the patients treated by ATA-non-

Summary, discussion and future perspectives
129
compliant surgery. Furthermore we examined to which extent clinical outcome of patients
was influenced by (1) one-step versus a two-step intended curative, (2) the location of the
initial curative surgery (experienced referral centre versus non-centre hospital), and (3) patient
and tumour characteristics. Our results indicated that patients treated adequately according to
ATA guidelines had significantly fewer reoperations compared to the inadequately operated
patients. Moreover, these patients remained significantly more often biochemically cured. We
could not demonstrate a significant effect on the clinical outcome of the patients treated in an
experienced referral centre hospital, but these patients received significantly more often
adequate surgery. Tumour size and lymph node involvement showed to be the most important
predictors for clinical disease free (DFS) and overall survival (OS).
In Chapter 5 we discussed the role of Positron Emission Tomography (PET) imaging using
different radiotracers in the staging and follow-up of papillary thyroid cancer (PTC) and
MTC. PET imaging is based on the use of positron emitting isotopes. For the detection of
thyroid cancers, several radiotracers are available. 18Fluorine-Fluorodeoxyglucose (18F-FDG),
a glucose analogue, is frequently used. While its use for discriminating between benign and
malignant thyroid nodules is contradictory, 18F-FDG can be of value in the follow-up of
differentiated thyroid cancer (DTC). Especially in patients with a negative radioiodine scan
but a detectable tumour marker thyroglobulin 18F-FDG can localize disease activity. Other
available tracers for the use during follow-up of DTC are 11C-Methionine PET (11C-MET-
PET) and 124Iodine-PET (124I-PET). While the value of 11C-MET-PET seems limited, 124I-PET
may be a superior diagnostic tool in comparison to the 131Iodine whole body scintigraphy
(WBS). In MTC patients, 18F-FDG also has been used, but 18Flurorine-
dihydroxyphenylalanine (18F-FDOPA) seems to be more sensitive. This radiotracer makes use
of a strongly upregulated transmembrane transport of amino acids via the large amino acid
transporters. In conclusion, PET imaging is a useful diagnostic tool in thyroid cancer although
the optimal radiotracer depends on the type of cancer and the intent of imaging
(staging/follow-up).
In Chapter 6 we evaluated the outcome of both 18F-FDG PET and 18F-DOPA PET with
calcitonin and carcinoembryonic (CEA) doubling times in 47 MTC patients. Early
identification of MTC patients with progressive residual disease is relevant because
appropriate therapeutic interventions may delay symptomatic deterioration. Calcitonin
doubling time is the most reliable marker for progression, but for accurate calculation, serial

Chapter 8
130
measurements over a considerable period are needed. Most morphological imaging techniques
like CT or MRI have moderate sensitivities for detecting recurrent MTC, but in the last
decade 18F-FDG PET and 18F-DOPA PET have become available for staging and follow-up of
MTC. We assessed the ability of 18F-FDG PET and 18F-DOPA PET to discriminate patients
with progressive disease and patients with stable disease. PET positivity was compared with
biochemical parameters (calcitonin and CEA serum levels and doubling times) and survival.
In a subgroup of patients whole body metabolic burden (WBMTB) was assessed with
standardized uptake value and the number of lesions. The WMBTB was compared with
biochemical parameters.
We observed that 18F-FDG-PET positivity was significantly correlated with both calcitonin
and CEA levels and their doubling times. Although 18F-DOPA PET positivity was
significantly correlated with the calcitonin and CEA levels, no significant correlation existed
with doubling times. 18F-DOPA PET detected significantly more lesions compared to 18F-
FDG PET in the 21 patients included in WBMTB analysis. However, 18F-FDG PET positive
was a more important indicator for poor survival. Both scans are therefore important in the
follow-up of patients; while 18F-DOPA PET is better in assessing the extent of the disease, 18F-FDG PET can more accurately identify patients with progressive disease.
In Chapter 7 we described the effects of four different tyrosine kinase inhibitors on MTC and
PTC cell lines. MTC and PTC can be caused by activating or rearrangements in the RE-
arranged during Transfection (RET) gene. This gene encodes for the RET tyrosine kinase
(TK) receptor which is involved in cellular growth and proliferation. Several TK inhibitors
have been tested in clinical trials, but it is unknown if there is specificity for particular RET
mutations and which inhibitor is the most effective. We cultured three cell-lines expressing a
MEN2A (MTC-TT), a MEN2B (MZ-CRC-1) mutation, and a RET/PTC (TPC-1)
rearrangement. We treated these cell lines with four different tyrosine kinase inhibitors
(axitinib, sunitinib, vandetanib and cabozantinib (XL184)) and compared the effect on cell
proliferation, RET expression and autophosphorylation, and RET downstream pathways
(Mitogen-Activated Protein Kinase (MAPK) pathway; involved in cell differentiation,
proliferation and survival).
A dose-dependent decrease in cell proliferation was found in all four tested tyrosine kinase
inhibitors. Cabozantinib was the most effective inhibitor of the MEN2A and RET/PTC cell
line, whereas vandetanib was the most effective inhibitor for the MEN2B cell line. Both
cabozantinib and vandetanib were able to decrease RET autophosphorylation and RET

Summary, discussion and future perspectives
131
expression levels in MEN2A and MEN2B cells. However, only vandetanib exerted this effect
by inhibiting RET transcription. A marked decrease in RET phosphorylation was detected for
RET/PTC cells, but RET/PTC expression was increased after exposure to cabozantinib. With
regard to downstream targets of RET, the MAPK pathway, and more specifically
Extracellular Signal-regulated Kinase (ERK) phosphorylation and expression, was markedly
decreased in MEN2A and MEN2B cells after exposure to cabozantinib and vandetanib
respectively. In RET/PTC cells no change in ERK phosphorylation and expression was
observed. Our results show that both vandetanib and cabozantinib are potent inhibitors for
tumour progression in MTC. We also found a specificity of the TK inhibitors for different
RET-mutations, suggesting mutation-specific therapies might be of benefit for MTC and PTC
patients.
Discussion and future perspectives
Although several new diagnostic and therapeutic technologies have been developed, the
prognosis of patients with medullary thyroid cancer has not improved in the last decades. The
current diagnostic and therapeutic approaches will be discussed and future perspectives are
provided.
Calcitonin as a routine test in patients with thyroid nodules
Whether or not to perform routine calcitonin testing is still a matter of debate. Although a
clearly elevated calcitonin level is highly suggestive for MTC, moderately elevated levels are
seen in a large number of non-MTC patients. While the European Thyroid Association (ETA)
guidelines recommend routine determination of calcitonin, the ATA guidelines do not
recommend either for or against routine measurement.8,20 Based on current literature, routine
testing is performed in several centres. In our systematic meta-analysis we showed that the
calcitonin test had a high diagnostic accuracy in terms of sensitivity and specificity. However,
the high diagnostic accuracy itself does not advocate routine calcitonin testing. Due to the low
prevalence of MTC in patients with thyroid nodules (range 0.11%-0.85%), the positive
predictive value of the calcitonin test is low.21-24 This is especially true if a low basal
calcitonin cut-off value is used and no additional stimulation tests are performed. With a cut-
off value of 10 pg/ml, only 7.5% of patients with an elevated calcitonin level will have a
histological proven MTC. Another important problem for evaluation of the routine use of the

Chapter 8
132
calcitonin test is the variation between assays, which make comparison between different
study groups difficult.25 Although not all patients with elevated calcitonin levels will be
operated on, a considerable proportion of these patients will be operated unnecessary, if the
supposed diagnosis MTC was not confirmed with immunohistochemical (IHC) based
cytological examination.
Cheung et al. performed a formal cost-effectiveness model on the routine calcitonin test in
thyroid nodules and concluded that calcitonin testing had a comparable cost-effectiveness to
mammography.26 However, if we apply our findings in this model, routine calcitonin testing
is not cost-effective, especially due to the lower prevalence we established in the evaluated
studies. Cost-effectiveness can be improved in several ways, such as applying the calcitonin
test only in subgroups of patients with a higher prevalence of MTC. Further studies should
focus on identification of such subgroups (e.g. young male patients, or patients with large
thyroid nodules). Based on current literature there seems no role for routine calcitonin testing
in all patients with thyroid nodules.
Instead of using the calcitonin test as a triage test next to or before FNA, calcitonin testing
can also be used as an add-on test after FNA. Determining calcitonin levels in patients with
inconclusive FNAC (Bethesda 3) results might be a more cost-effective approach in
comparison to routine calcitonin testing in all thyroid nodule patients. Measuring calcitonin in
FNA aspirates can increase the sensitivity of FNAC for diagnosis of MTC. Recently the use
of FNA-calcitonin measurement has been advocated in addition to routine calcitonin testing
as a possible alternative to stimulated calcitonin testing.27 The (cost-)effectiveness of this
approach is unclear as it still requires routine calcitonin testing and needs further evaluation.
Another application of the calcitonin test may be as a routine pre-operative test. The
reported sensitivity of routine pre-operative testing is lower compared to routine calcitonin
testing in all patients. This lower sensitivity is likely the result from a verification bias; studies
including only pre-operative patients have histological verification in all calcitonin-negative
patients while studies including all patients have only histological confirmation in a limited
number of calcitonin-negative patients (e.g. operated for other causes).28,29 The sensitivity of
pre-operative calcitonin testing is for detection of MTC is higher than FNAC and can increase
the rate of correct pre-operative diagnoses. This can result in more adequate initial surgical
procedures which is of crucial importance in MTC patients. Few studies have reported on the
value of pre-operative calcitonin testing and more research is needed whether this approach
can be cost-effective.

Summary, discussion and future perspectives
133
Optimal surgical treatment for MTC patients
Although the current ATA guidelines provide specific recommendations for the surgical
approach, the effect of adherence to these recommendations on the outcome of MTC patients
is unclear. We demonstrated that patients who were not treated adequately according to
guidelines had more locoregional reoperations and less biochemical cure at follow-up. We
also observed that patients treated in a non-centre institute had less often adequate surgery
compared to patients treated in a centre. Our findings underscore the importance to organize
the treatment of MTC patients in specialized tertiary referral centres, with maximal surgical
experience but also a multidisciplinary approach including endocrinologists, surgeons,
radiologists, nuclear physicians and pathologists. One of the main problems in the treatment
of MTC is to determine accurately the extent of the disease. Even with state of the art
diagnostic methods it is difficult to determine locally advanced disease and in particular
optimal nodal staging. On the other hand, although accurate imaging is crucial for optimal
locoregional surgery, it remains unclear when the point of cure is passed due to undetectable
distant metastases even with extended (elective) surgical dissections.30
Although total thyroidectomy and central compartment lymph node dissection are accepted
as standard procedure in common practice, it still remains unclear whether or not to perform a
(bi)lateral lymph node dissection of level II-V in MTC patients, especially in the elective
treatment of patients without apparent lymph node metastases in the lateral compartments. A
number of authors recommend an elective lateral lymph node dissection whenever lymph
node metastases are present in the central lymph node compartment (level VI).31 Other
authors suggest a (uni)lateral lymph node dissection when calcitonin levels are elevated >20
pg/ml and a bilateral lymph node dissection with calcitonin >200 pg/ml. Using such a cut-off
level for calcitonin minimizes the risk that MTC patients receive inadequate surgery.
However, as a consequence there is a risk of over treating patients as nearly 90% of MTC
patients with calcitonin between 20-200 pg/ml have no lateral lymph node metastases.32
Long-term results on cure and survival of the different proposed strategies are lacking in
patients without apparent lateral lymph node metastasis, and the current ATA guidelines are
indeterminate. In absence of such data, careful follow-up of treated patients is crucial. Either
way, comprehensive pre-operative evaluation is important and functional imaging techniques
can play an important role pre-operative staging. These techniques can also identify patients
who may not benefit from surgical treatment. The optimal surgical treatment for MTC
patients thus remains difficult; another reason to advocate treatment in an experienced centre.

Chapter 8
134
Functional imaging in the follow-up of MTC
We showed that 18F-FDG PET was superior in detecting patients with progressive disease,
while 18F-DOPA PET was better in assessing the extent of residual disease. We therefore
proposed a flow diagram with a combined approach of 18F-FDG PET and 18F-FDOPA PET in
patients with increasing tumour markers. Using this flow diagram, progressive MTC patients
who do not benefit from (local) surgical treatment but are candidates for systemic treatment
can be identified. A proportion of patients with progressive disease - indicated by rapidly
increasing tumour markers - still have false negative imaging results.33 Other imaging
modalities in these patients are necessary for detection of recurrent tumour lesions to assess
the optimal (therapeutic) approach. However, first results for new tracers such as 68Ga-
somatostatin analogues or 11C-methionine are not convincing. Compared with 18F-FDG PET
and 18F-FDOPA PET, 68Ga-somatostatin analogue did not identify additional lesions or led to
a change in TNM status.34,35 Although 11C-MET PET had a higher sensitivity for detecting
cervical metastasis compared to 18F-FDG PET, it was not superior compared to ultrasound.36
Further applications of nuclear imaging may be valuable in the early evaluation of
therapeutic response of targeted therapy, thereby identifying patients who may benefit from
this treatment. A preclinical study with vandetanib showed for instance that 18F-FDG PET
was able to assess metabolic changes after three days of treatment. A down-regulation of key
genes in the glycolysis pathway was observed resulting in a reduction of uptake of
deoxyglucose both in vitro and in vivo.37 Other improvements in the future may focus on
developing radiotracers which are able to selectively image mutated receptors, as was shown
for a mutant form of EGFR in lung carcinoma.38 As somatic mutations exist in the RET
receptor in a fair proportion of sporadic MTC patients, using selective radiotracers may better
identify these lesions and also serve as a new treatment modality.
New treatment modalities
In the last years, new systemic therapeutic options have become available for the treatment of
MTC patients. We showed in a comparison of four different TK inhibitors targeting RET that
vandetanib and cabozantinib were the most effective TK inhibitors. This was also confirmed
in two phase III clinical trials evaluating these TK inhibitors with a significant effect on
progression free survival (PFS).39,40 Although these TK inhibitors show promising results,
only effects on PFS have been reported, while no benefits on overall survival (OS) have been
demonstrated yet. With vandetanib an estimated PFS of 30.5 months was reported versus 19.3

Summary, discussion and future perspectives
135
months in the placebo group. For cabozantinib a PFS of 11.2 months was observed versus 4
months in the control group, but this study included only progressive patients (i.e. showing
progression compared to imaging obtained within the prior 14 months). Targeted therapies are
generally better tolerated in comparison to cytotoxic chemotherapeutic regimens, although a
large proportion of patients develop serious side-effects which may have a great impact on the
quality of life. Furthermore, timing for initiation of these therapies has to be made with
consideration of the natural course of disease progression, as a large proportion of patients
have stable or slowly progressive disease. However, in patients presenting with progressive
disease there may be a role for (neo) adjuvant systemic therapy.
Besides the RET activated pathway, also other receptors and pathways can be potential
therapeutic targets in MTC. Indeed, over-expression of VEGF, VEGFR and MET have been
described in MTC.41-43 It also has been shown that inhibition of RET can lead to over
activation of signalling trough EGFR.44 Inhibiting multiple kinases can therefore be beneficial
to suppress such escape mechanisms. Most inhibitors currently in use are already multikinase
inhibitors, thus exerting their effects on multiple kinases. However, the optimal combination
of inhibition with regard to tumour regression and side effects may advocate the use of
multiple inhibitors. Combinations of TK inhibitors with classic chemotherapeutic agents may
also be beneficial as was reported in an in vivo study showing an additional effect of cisplatin
to sunitinib.45
In the meanwhile new TK inhibitors are being developed and tested. Ponatinib was shown
to be a potent inhibitor of RET kinases in a pre-clinical study.46 A phase II study with this
new drug is currently recruiting for patients with advanced MTC (clinicaltrails.gov). Other
TK inhibitors evaluated for MTC are lenvatinib and AZD1480.47,48 Not only tyrosine kinases
can be therapeutic targets for medullary thyroid carcinoma. A recent in vitro study showed
promising results with an agent targeting mitochondria in MTC tumour cells.49
In conclusion, the treatment options for patients with advanced metastatic MTC are being
extended. However, although results of clinical trials look promising, no definite
improvement of survival has been established. Further studies are needed to identify more
effective TK inhibitors, possible in combination with other TK inhibitors or with agents
blocking other potential targets. Careful consideration must be given to outweigh the benefits
of possible disease control versus side effects of these new therapies. Therefore treatment of
this rare neuroendocrine tumour should be performed in an experienced centre to further
enhance diagnostic and therapeutic strategies to ultimately improve the outcome of MTC
patients.

Chapter 8
136
References
1. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. A National Cancer Data Base report on 53,856 cases
of thyroid carcinoma treated in the U.S., 1985-1995 [see commetns]. Cancer 1998;83:2638-2648.
2. de Groot JW, Links TP, Plukker JT, Lips CJ, Hofstra RM. RET as a diagnostic and therapeutic target in
sporadic and hereditary endocrine tumors. Endocr Rev 2006;27:535-560.
3. Kebebew E, Ituarte PH, Siperstein AE, Duh QY, Clark OH. Medullary thyroid carcinoma: clinical
characteristics, treatment, prognostic factors, and a comparison of staging systems. Cancer
2000;88:1139-1148.
4. Modigliani E, Cohen R, Campos JM, et al. Prognostic factors for survival and for biochemical cure in
medullary thyroid carcinoma: results in 899 patients. The GETC Study Group. Groupe d'etude des
tumeurs a calcitonine. Clin Endocrinol (Oxf) 1998;48:265-273.
5. Bugalho MJ, Santos JR, Sobrinho L. Preoperative diagnosis of medullary thyroid carcinoma: fine needle
aspiration cytology as compared with serum calcitonin measurement. J Surg Oncol 2005;91:56-60.
6. Landsvater RM, Rombouts AG, te Meerman GJ, et al. The clinical implications of a positive calcitonin
test for C-cell hyperplasia in genetically unaffected members of an MEN2A kindred. Am J Hum Genet
1993;52:335-342.
7. Machens A, Haedecke J, Holzhausen HJ, Thomusch O, Schneyer U, Dralle H. Differential diagnosis of
calcitonin-secreting neuroendocrine carcinoma of the foregut by pentagastrin stimulation.
Langenbecks Arch Surg 2000;385:398-401.
8. Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer: management guidelines of the American
Thyroid Association. Thyroid 2009;19:565-612.
9. Machens A, Gimm O, Ukkat J, Hinze R, Schneyer U, Dralle H. Improved prediction of calcitonin
normalization in medullary thyroid carcinoma patients by quantitative lymph node analysis. Cancer
2000;88:1909-1915.
10. Scollo C, Baudin E, Travagli JP, et al. Rationale for central and bilateral lymph node dissection in
sporadic and hereditary medullary thyroid cancer. J Clin Endocrinol Metab 2003;88:2070-2075.
11. Meijer JA, Bakker L, Valk GD, et al. Radioactive Iodine in the treatment of Medullary Thyroid
Carcinoma: a controlled multicenter study. Eur J Endocrinol 2013.
12. Machens A, Schneyer U, Holzhausen HJ, Dralle H. Prospects of remission in medullary thyroid
carcinoma according to basal calcitonin level. J Clin Endocrinol Metab 2005;90:2029-2034.
13. de Groot JW, Plukker JT, Wolffenbuttel BH, Wiggers T, Sluiter WJ, Links TP. Determinants of life
expectancy in medullary thyroid cancer: age does not matter. Clin Endocrinol (Oxf) 2006;65:729-736.
14. Rendl G, Manzl M, Hitzl W, Sungler P, Pirich C. Long-term prognosis of medullary thyroid carcinoma.
Clin Endocrinol (Oxf) 2008;69:497-505.
15. Wells SA,Jr, Robinson BG, Gagel RF, et al. Vandetanib in patients with locally advanced or metastatic
medullary thyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol 2012;30:134-141.
16. Elisei R, Schlumberger MJ, Muller SP, et al. Cabozantinib in progressive medullary thyroid cancer. J Clin
Oncol 2013;31:3639-3646.
17. Plaza-Menacho I, Mologni L, McDonald NQ. Mechanisms of RET signaling in cancer: current and future
implications for targeted therapy. Cell Signal 2014;26:1743-1752.
18. Kapiteijn E, Schneider TC, Morreau H, Gelderblom H, Nortier JW, Smit JW. New treatment modalities
in advanced thyroid cancer. Ann Oncol 2012;23:10-18.
19. Ye L, Santarpia L, Gagel RF. The evolving field of tyrosine kinase inhibitors in the treatment of
endocrine tumors. Endocr Rev 2010;31:578-599.
20. Pacini F, Schlumberger M, Dralle H, et al. European consensus for the management of patients with
differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol 2006;154:787-803.
21. Rieu M, Lame MC, Richard A, et al. Prevalence of sporadic medullary thyroid carcinoma: the
importance of routine measurement of serum calcitonin in the diagnostic evaluation of thyroid
nodules. Clin Endocrinol (Oxf) 1995;42:453-460.
22. Vierhapper H, Niederle B, Bieglmayer C, Kaserer K, Baumgartner-Parzer S. Early diagnosis and curative
therapy of medullary thyroid carcinoma by routine measurement of serum calcitonin in patients with
thyroid disorders. Thyroid 2005;15:1267-1272.

Summary, discussion and future perspectives
137
23. Elisei R, Bottici V, Luchetti F, et al. Impact of routine measurement of serum calcitonin on the
diagnosis and outcome of medullary thyroid cancer: experience in 10,864 patients with nodular
thyroid disorders. J Clin Endocrinol Metab 2004;89:163-168.
24. Schneider C, Kobe C, Schmidt M, et al. Calcitonin screening in patients with thyroid nodules. Diagnostic
value. Nuklearmedizin 2012;51:228-233.
25. d'Herbomez M, Caron P, Bauters C, et al. Reference range of serum calcitonin levels in humans:
influence of calcitonin assays, sex, age, and cigarette smoking. Eur J Endocrinol 2007;157:749-755.
26. Cheung K, Roman SA, Wang TS, Walker HD, Sosa JA. Calcitonin measurement in the evaluation of
thyroid nodules in the United States: a cost-effectiveness and decision analysis. J Clin Endocrinol
Metab 2008;93:2173-2180.
27. Trimboli P, Guidobaldi L, Crescenzi A, Bongiovanni M, Giovanella L. The essential use of FNA-calcitonin
for detecting medullary thyroid cancer. Endocrine 2014.
28. Niccoli P, Wion-Barbot N, Caron P, et al. Interest of routine measurement of serum calcitonin: study in
a large series of thyroidectomized patients. The French Medullary Study Group. J Clin Endocrinol
Metab 1997;82:338-341.
29. Chambon G, Alovisetti C, Idoux-Louche C, et al. The use of preoperative routine measurement of basal
serum thyrocalcitonin in candidates for thyroidectomy due to nodular thyroid disorders: results from
2733 consecutive patients. J Clin Endocrinol Metab 2011;96:75-81.
30. Kebebew E, Kikuchi S, Duh QY, Clark OH. Long-term results of reoperation and localizing studies in
patients with persistent or recurrent medullary thyroid cancer. Arch Surg 2000;135:895-901.
31. Moley JF. Medullary thyroid carcinoma: management of lymph node metastases. J Natl Compr Canc
Netw 2010;8:549-556.
32. Machens A, Dralle H. Biomarker-based risk stratification for previously untreated medullary thyroid
cancer. J Clin Endocrinol Metab 2010;95:2655-2663.
33. Marzola MC, Pelizzo MR, Ferdeghini M, et al. Dual PET/CT with (18)F-DOPA and (18)F-FDG in
metastatic medullary thyroid carcinoma and rapidly increasing calcitonin levels: Comparison with
conventional imaging. Eur J Surg Oncol 2010;36:414-421.
34. Conry BG, Papathanasiou ND, Prakash V, et al. Comparison of (68)Ga-DOTATATE and (18)F-
fluorodeoxyglucose PET/CT in the detection of recurrent medullary thyroid carcinoma. Eur J Nucl Med
Mol Imaging 2010;37:49-57.
35. Treglia G, Castaldi P, Villani MF, et al. Comparison of (18)F-DOPA, (18)F-FDG and (68)Ga-somatostatin
analogue PET/CT in patients with recurrent medullary thyroid carcinoma. Eur J Nucl Med Mol Imaging
2012:569-580.
36. Jang HW, Choi JY, Lee JI, et al. Localization of medullary thyroid carcinoma after surgery using (11)C-
methionine PET/CT: comparison with (18)F-FDG PET/CT. Endocr J 2010;57:1045-1054.
37. Walter MA, Benz MR, Hildebrandt IJ, et al. Metabolic imaging allows early prediction of response to
vandetanib. J Nucl Med 2011;52:231-240.
38. Yeh HH, Ogawa K, Balatoni J, et al. Molecular imaging of active mutant L858R EGF receptor (EGFR)
kinase-expressing nonsmall cell lung carcinomas using PET/CT. Proc Natl Acad Sci U S A
2011;108:1603-1608.
39. Wells SA,Jr, Robinson BG, Gagel RF, et al. Vandetanib in patients with locally advanced or metastatic
medullary thyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol 2012;30:134-141.
40. Elisei R, Schlumberger MJ, Muller SP, et al. Cabozantinib in progressive medullary thyroid cancer. J Clin
Oncol 2013;31:3639-3646.
41. Rodriguez-Antona C, Pallares J, Montero-Conde C, et al. Overexpression and activation of EGFR and
VEGFR2 in medullary thyroid carcinomas is related to metastasis. Endocr Relat Cancer 2010;17:7-16.
42. Capp C, Wajner SM, Siqueira DR, Brasil BA, Meurer L, Maia AL. Increased expression of vascular
endothelial growth factor and its receptors, VEGFR-1 and VEGFR-2, in medullary thyroid carcinoma.
Thyroid 2010;20:863-871.
43. Papotti M, Olivero M, Volante M, et al. Expression of Hepatocyte Growth Factor (HGF) and its
Receptor (MET) in Medullary Carcinoma of the Thyroid. Endocr Pathol 2000;11:19-30.
44. Vitagliano D, De Falco V, Tamburrino A, et al. The tyrosine kinase inhibitor ZD6474 blocks proliferation
of RET mutant medullary thyroid carcinoma cells. Endocr Relat Cancer 2010;18:1-11.
45. Lopergolo A, Nicolini V, Favini E, et al. Synergistic cooperation between sunitinib and cisplatin
promotes apoptotic cell death in human medullary thyroid cancer. J Clin Endocrinol Metab
2014;99:498-509.

Chapter 8
138
46. De Falco V, Buonocore P, Muthu M, et al. Ponatinib (AP24534) Is a Novel Potent Inhibitor of Oncogenic
RET Mutants Associated With Thyroid Cancer. J Clin Endocrinol Metab 2013;98:E811-9.
47. Schlumberger M, Jarzab B, Cabanillas ME, et al. A phase II trial of the multitargeted kinase inhibitor
lenvatinib (E7080) in advanced medullary thyroid cancer (MTC). J Clin Oncol 2012;30.
48. Couto JP, Almeida A, Daly L, Sobrinho-Simoes M, Bromberg JF, Soares P. AZD1480 blocks growth and
tumorigenesis of RET- activated thyroid cancer cell lines. PLoS One 2012;7:e46869.
49. Starenki D, Park JI. Mitochondria-Targeted Nitroxide, Mito-CP, Suppresses Medullary Thyroid
Carcinoma Cell Survival In Vitro and In Vivo. J Clin Endocrinol Metab 2013;98:1529-1540.

Nederlandse samenvatting

Nederlandse samenvatting
140
Nederlandse samenvatting
Medullair schildkliercarcinoom (medullair thyroïd carcinoom, MTC) gaat uit van de
calcitonine producerende C-cellen in de schildklier en is verantwoordelijk voor ongeveer 5%
van alle soorten schildklierkanker. MTC komt sporadisch voor (75%) of als onderdeel van
één van de erfelijke tumorsyndromen; familiair MTC (FMTC) en multipele-endocriene-
neoplasie-type 2 (MEN2). Bij het MEN2 syndroom worden een MEN2A en een MEN2B
variant onderscheiden, waarbij mutaties in het ‘REarranged during Transfection’ (RET) gen
ten grondslag liggen aan deze syndromen. Andere uitingen van het MEN2 syndroom zijn
bijniertumoren (feochromocytoom; MEN2A en 2B), hyperparathyreoïdie (MEN2A) of
neurofibromatose (MEN2B).
De meeste patiënten met MTC presenteren zich met een asymptomatische palpabele nodus
in de schildklier of in één of meerdere lymfeklieren. Als de diagnose wordt gesteld heeft 50%
van de patiënten uitzaaiingen in de lymfeklieren en 10% uitzaaiingen elders in het lichaam.
Om de diagnose MTC te stellen is een echogeleide dunne naald biopsie de eerste stap. Hierbij
kan immunohistochemische analyse de sensitiviteit voor het opsporen van MTC verhogen.
Omdat MTC uitgaat van de calcitonine producerende C-cellen, kan de bepaling van
calcitonine in het bloed ook worden gebruikt als een screenings instrument bij patiënten met
een schildkliernodus om MTC in een vroeg stadium op te sporen. Deze screening staat echter
nog ter discussie, omdat een aanzienlijk aantal patiënten een verhoogd calcitonine heeft op
basis van andere oorzaken dan een MTC.
Volgens de huidige richtlijn van de Amerikaanse Schildklier Associatie (American
Thyroid Association; ATA) bestaat de initiële behandeling van patiënten met een sporadisch
MTC zonder bekende metastasen bij diagnose uit een totale thyreoïdectomie met een
electieve lymfadenectomie van regionale lymfeklieren in het centrale compartiment (level VI)
(centrale compartiments dissectie (CCD)). Wanneer er sprake is van ziekte uitbreiding naar de
laterale lymfeklieren van de hals is er ook een indicatie voor een gemodificeerde radicale uni-
of bi- laterale dissectie (LND). Omdat chirurgische behandeling de enige kans biedt op curatie
en/of locoregionale controle, voeren sommige chirurgen naast een electieve CCD ook een
electieve LND uit. De keuze hiervoor wordt mede bepaald door het risico op micrometastasen
wanneer een ziekte zich locoregionaal presentereert. Bij meer dan 50% van de patiënten is de
ziekte zodanig uitgebreid dat geen curatie bereikt kan worden. In tegenstelling tot andere
vormen van schildkliercarcinoom hebben MTC patiënten geen baat bij adjuvante therapie met

Nederlandse samenvatting
141
radioactief jodium. Daarom is adequate chirurgie in MTC van cruciaal belang voor optimale
locoregionale controle en curatie.
Hoewel meer dan 50% van de patiënten ondanks uitgebreide chirurgie niet kan worden
genezen, is de levensverwachting van het merendeel van de patiënten met een beperkte
tumorrest goed. Zorgvuldige follow-up is van belang om tijdig ziekte progressie vast te
stellen, en bestaat uit regelmatige bepalingen van de tumormarkers calcitonine en
carcinoembryonic antigeen (CEA); een tweede tumormarker voor MTC. Wanneer deze
tumormarkers stijgen is verdere diagnostiek met anatomische en functionele beeldvorming
geïndiceerd. De verdubbelingstijden van de calcitonine en CEA waarden zijn vooralsnog de
meest betrouwbare markers voor ziekteprogressie. Om ziekteprogressie vast te stellen zijn
echter meerdere metingen nodig over een langere periode. Het vroegtijdig vaststellen van
ziekteprogressie kan van belang zijn, omdat eventuele therapeutische interventies verdere
ziekteprogressie kunnen vertragen. Afhankelijk van de uitgebreidheid van de ziekte en de
snelheid waarmee tumormarkers stijgen, kunnen verschillende therapeutische strategieën
worden overwogen; een ‘wait and see’ beleid met een zorgvuldig vervolg van de patiënt, een
chirurgische interventie (voor locoregionale controle) of behandeling met gerichte
systemische (targeted) therapie.
In de palliatieve behandeling van MTC is conventionele chemotherapie niet effectief
gebleken. Recent onderzoek met gerichte tyrosine kinase (TK) remmers bij MTC patiënten
heeft een langere progressie vrije overleving laten zien. Het is echter onbekend of het effect
van deze tyrosine kinase remmers afhankelijk is van de aanwezigheid van een (somatische of
kiembaan) RET mutatie in de tumor of patiënt. Verschillende RET mutaties zijn
verantwoordelijk voor specifieke configurationele veranderingen van het RET eiwit. De meest
voorkomende mutatie in sporadische MTC patiënten bijvoorbeeld, ‘de MEN2B mutatie’,
verandert het ATP pocket van het RET eiwit. Sommige TK remmers kunnen hier minder goed
aan binden. De effectiviteit van gerichte therapie kan daarom mogelijk verbeterd worden door
de TK remmer te selecteren aan de hand van de specifieke RET mutatie. Daarnaast hebben de
meeste TK remmers verschillende aangrijpingspunten die meerdere intracellulaire
signaalroutes kunnen activeren. Naast het effect op de tumor kunnen ook bijwerkingen
optreden, zoals cardiale toxiciteit of het hand-voet syndroom. Zorgvuldige selectie van
patiënten is belangrijk, en in de toekomst kan mogelijk mutatie specifieke therapie ontwikkeld
worden.

Nederlandse samenvatting
142
Dit proefschrift onderzoekt verschillende belangrijke klinische vraagstukken over de diagnose
en behandeling van patiënten met een primair en recidief MTC. Het doel was om de
diagnostische en therapeutische modaliteiten in de behandeling van MTC te evalueren en te
verbeteren door middel van: (1) het evalueren van de waarde van de calcitonine test voor het
opsporen van MTC in patiënten met een schildkliernodus; (2) het beoordelen van de huidige
ATA richtlijn ten aanzien van de chirurgische behandeling van MTC patiënten; (3) het
bepalen van de waarde van 18F-FDG PET en 18F-DOPA PET in de detectie van progressief en
recidiverend MTC en (4) het onderzoeken van de effectiviteit van verschillende tyrosine
kinase remmers bij de behandeling van MTC.
In Hoofdstuk 1 wordt een algemene introductie gegeven over MTC en worden het doel en de
achtergronden van dit proefschrift besproken.
In Hoofdstuk 2 presenteren we drie patiënten met verschillende ziektestadia om de variatie in
klinische presentatie en biologisch gedrag van het MTC te illustreren. Aan de hand van deze
patiënten wordt een korte beschrijving gegeven van de presentatie, diagnose, behandeling en
follow-up van MTC.
Omdat MTC patiënten bij wie de ziekte in een vroeg stadium wordt vastgesteld een betere
prognose hebben, zou vroege opsporing van waarde kunnen zijn. Deze tumoren zouden met
een calcitonine bepaling kunnen worden gedetecteerd omdat vrijwel alle MTC’s calcitonine
produceren. Er bestaat echter geen consensus over het routinematig bepalen van calcitonine in
bepaalde patiëntengroepen, bijvoorbeeld bij patiënten die zich presenteren met een
schildkliernodus. Om de diagnostische accuratesse van de calcitonine test te evalueren voor
het opsporen van MTC bij patiënten met een schildkliernodus is in Hoofdstuk 3 een meta-
analyse verricht. Zestien studies werden geïncludeerd, waarbij schattingen werden gemaakt
van de sensitiviteit en specificiteit voor verschillende cut-off waarden met en zonder
stimulatie. Bij een lage basale calcitonine cut-off waarde (10 pg/ml) werd een hoge
sensitiviteit gevonden. De gecombineerde basale en gestimuleerde calcitonine bepalingen
resulteerden ook in een hoge sensitiviteit. Wanneer gekozen werd voor een hogere cut-off
waarde of een gestimuleerde calcitonine waarde nam de specificiteit iets toe. Gezien de hoge
sensitiviteit en specificiteit is de totale diagnostische accuratesse van de calcitonine bepaling
hoog. Door de lage prevalentie van MTC is de calcitonine bepaling echter niet meteen
geschikt als screeningsinstrument. Omdat MTC een zeldzame ziekte is, is de positief

Nederlandse samenvatting
143
voorspellende waarde (PPV) laag. Daarmee is ook de klinische toepasbaarheid van de
routinematige calcitoninebepaling voor het opsporen van MTC beperkt in patiënten met een
schildkliernodus. De lage PPV maakt het risico op een het onnodig opereren van patiënten
groter. Ook blijft de kosteneffectiviteit van de calcitoninescreening, gezien deze lage
prevalentie, nog onduidelijk.
In Hoofdstuk 4 is geëvalueerd of de chirurgische behandeling van MTC zoals beschreven in
de richtlijn van de American Thyroid Association (ATA) patiënten een klinisch voordeel
oplevert. Voor de optimale chirurgische behandeling bestaat geen eenduidig bewijs, met name
niet ten aanzien van de uitgebreidheid van de laterale lymfeklier dissectie. Daarom worden
door verschillende experts en richtlijnen verschillende chirurgische strategieën voorgesteld.
De ATA richtlijn adviseert een totale thyreoïdectomie en lymfeklierdissectie van het centrale
compartiment (level VI) als initiële behandeling. Bij positieve regionale lymfeklieren is ook
een systematische lymfeklierdissectie van de laterale compartimenten (level II-V)
geïndiceerd. In een retrospectieve studie werd de klinische uitkomst van patiënten behandeld
volgens de ATA richtlijn vergeleken met patiënten niet behandeld volgens deze richtlijn.
Deze klinische uitkomst was gedefinieerd als aantal re-operaties, biochemische curatie,
overleving en complicaties. Daarnaast werd onderzocht in welke mate de klinische uitkomst
werd beïnvloed door (1) een operatie met curatieve intentie in één of twee sessies, (2) de
locatie van de initiële curatieve operatie (tertiair verwijzingscentrum versus niet-centrum
ziekenhuis) en (3) patiënt en tumorkarakteristieken. De resultaten van deze studie laten zien
dat patiënten die volgens de richtlijn adequaat zijn behandeld significant minder re-operaties
hadden vergeleken met de inadequaat geopereerde patiënten. Daarnaast hadden adequaat
geopereerde patiënten significant meer biochemische curatie. Er werd geen significant effect
aangetoond op de klinische uitkomst van patiënten geopereerd in een tertiair
verwijzingscentrum, maar deze patiënten ondergingen wel significant vaker een adequate
operatie. Tumorgrootte en lymfeklierbetrokkenheid waren de belangrijkste voorspellers van
ziektevrije en totale overleving.
In Hoofdstuk 5 wordt de rol besproken van beeldvorming met verschillende radioactieve
tracers met behulp van de positron emissie tomografie (PET) voor de stagering en follow-up
van patiënten met een papillair, folliculair en medullair schildkliercarcinoom. PET is
gebaseerd op het gebruik van isotopen die positronen uitzenden. Voor de detectie van
schildkliercarcinoom zijn meerdere radioactieve tracers beschikbaar. 18Fluorine-

Nederlandse samenvatting
144
Fluorodeoxyglucose (18F-FDG) is een glucose analoog, die van waarde is in de follow-up van
patiënten met een papillair en folliculair schildkliercarcinoom. Met name bij patiënten met
een negatieve 131Jodium scintigrafie maar een detecteerbare tumormarker (thyreoglobuline),
kan 18F-FDG ziekte activiteit lokaliseren. Andere beschikbare tracers voor gebruik in de
follow-up van het papillair en folliculair schildkliercarcinoom zijn 11C-Methionine PET (11C-
MET PET) en 124Iodine-PET (124I-PET). Hoewel de waarde van 11C-MET PET beperkt lijkt,
heeft 124I-PET mogelijk wel een toegevoegde waarde vergeleken met de standaard 131Jodium
scintigrafie, de huidige plaatsbepaling is echter nog onduidelijk.
Bij patiënten met MTC wordt 18F-FDG ook gebruikt, maar lijkt 18Flurorinedihydroxyphenylalanine (18F-DOPA) meer sensitief. Deze radiotracer maakt
gebruik van een sterk verhoogd transport van aminozuren via de ‘large amino acid
transporters’. Beeldvorming met behulp van PET is een belangrijk diagnostisch instrument bij
patiënten met een schildkliercarcinoom. De optimale radioactieve tracer is afhankelijk van het
type carcinoom en het doel van de beeldvorming (stageren/follow-up).
In Hoofdstuk 6 wordt een studie bij 47 patiënten met MTC beschreven, waarin de opname op
de 18F-FDG PET als 18F-DOPA PET wordt vergeleken met verdubbelingstijden van
calcitonine en carcinoembryonic antigeen (CEA). Vroege opsporing van progressieve ziekte
bij MTC patiënten kan belangrijk zijn, omdat behandeling verdere achteruitgang kan
vertragen. De calcitonine verdubbelingstijd is de belangrijkste biochemische marker voor
progressieve ziekte, maar hiervoor zijn meerdere metingen over een langere tijdsperiode
noodzakelijk. Positiviteit op de 18F-FDG PET en 18F-DOPA PET scan werd vergeleken met
de absolute calcitonine en CEA serum waarden, de verdubbelingstijden van deze
tumormarkers en overleving van de patiënt. Tevens werd in een subgroep aan de hand van een
gestandaardiseerde opname waarde van de tracers (standardized uptake value; SUV) en het
aantal laesies de zogenaamde ‘whole body metabolic burden (WBMTB)’ bepaald. Deze
WBMTB werd vergeleken met de bovengenoemde biochemische parameters. 18F-FDG PET positiviteit was significant gecorreleerd met zowel de absolute calcitonine
en CEA waarden als met de verdubbelingstijden van beide tumormarkers. 18F-DOPA PET
positiviteit was significant gecorreleerd met de absolute calcitonine en CEA waarden, maar er
was geen correlatie met verdubbelingstijden. Met de 18F-DOPA PET werden significant meer
laesies gedetecteerd dan met de 18F-FDG PET. Positiviteit op de 18F-FDG PET was een
belangrijke indicator voor een kortere overleving, in vergelijking met patiënten met een
negatieve 18F-FDG PET scan. Geconcludeerd kan worden dat beide scans van waarde zijn bij

Nederlandse samenvatting
145
de follow-up van patiënten met MTC; 18F-DOPA PET vooral om de uitgebreidheid van de
ziekte vast te stellen, 18F-FDG PET om de patiënten met progressieve ziekte beter te
identificeren.
In Hoofdstuk 7 wordt een studie beschreven waarin de effecten van vier verschillende
tyrosine kinase remmers in MTC en papillair schildklier carcinoom (PTC) cellijnen wordt
geëvalueerd. MTC en PTC kunnen worden veroorzaakt door een activatie of
herrangschikking in het ‘RE-arranged during Transfection’ (RET) gen. Dit gen codeert voor
de RET tyrosine kinase receptor, die betrokken is bij celgroei en proliferatie. Verschillende
tyrosine kinase remmers zijn getest in klinische trials, maar het is onbekend of er ook
specificiteit bestaat voor een bepaalde RET mutatie en welke tyrosine kinase remmer dan het
meest effectief is. Cellijnen met een MEN2A (MTC-TT) mutatie, een MEN2B (MZ-CRC-1)
mutatie en een RET/PTC (TPC-1) herrangschikking werden behandeld met vier verschillende
tyrosine kinase remmers (axitinib, sunitinib, vandetanib en cabozantinib (XL184)). Het effect
op celproliferatie, RET expressie en autofosforylatie werd bepaald. Ook werd het effect op
Mitogen-activated protein kinase (MAPK) signaalroute onderzocht (meer specifiek het effect
op ‘Extracellular Signal-regulated Kinase’ (ERK)); een onderliggende RET signaalroute
betrokken bij celdifferentiatie, proliferatie en overleving.
Alle vier onderzochte tyrosine kinase remmers lieten een dosisafhankelijke afname in
celproliferatie zien. Cabozantinib was de meest effectieve remmer in de MEN2A en
RET/PTC cellijn, terwijl vandetanib de meest effectieve remmer voor de MEN2B cellijn was.
Zowel cabozantinib als vandetanib waren in staat om de RET autofosforylatie en RET
expressie te verminderen in de MEN2A en MEN2B cellijn. Echter, alleen bij vandetanib
gebeurde dit door het remmen van de RET transcriptie. Bij behandeling met cabozantinib
werd een duidelijke afname in RET fosforylatie gezien in de RET/PTC cellijn, maar de
RET/PTC expressie was toegenomen. ERK fosforylatie en expressie waren zowel in MEN2A
als MEN2B cellijnen afgenomen na behandeling met cabozantinib of vandetanib. In
RET/PTC cellijnen werd geen verandering in ERK fosforylatie en expressie gezien. Deze
studie laat zien dat vandetanib en cabozantinib potente remmers zijn van tumorproliferatie in
MTC cellijnen. Daarnaast werd ook een specificiteit van de tyrosine kinase remmers
gevonden voor cellijnen met verschillende RET mutaties. Dit suggereert dat mutatie
specifieke therapie van waarde kan zijn in MTC en PTC patiënten.

146

147
Dankwoord
Het medullaire schildkliercarcinoom is een zeldzame tumor waarvoor de behandeling de inzet
vraagt van een ervaren en gemotiveerd behandelteam, met expertise vanuit verschillende
disciplines. Tijdens mijn onderzoek heb ik met veel mensen samengewerkt vanuit deze
verschillende vakgebieden. Dit proefschrift zou dan ook niet mogelijk zijn geweest zonder
hun hulp.
Prof. dr. T.P. Links, beste Thera, het was een voorrecht om onder jouw begeleiding dit
proefschrift te mogen schrijven. Zonder jouw enorme gedrevenheid zou dit project niet zijn
geslaagd. Je optimisme heeft me op de moeilijke momenten altijd weer kunnen motiveren.
Niet alleen op wetenschappelijk gebied heb ik enorm veel van je geleerd, maar ook op
persoonlijk vlak heb ik me onder jouw begeleiding verder ontwikkeld. Ik hoop dat we in de
toekomst nog veel kunnen samenwerken.

Dankwoord
148
Prof. dr. J.Th.M. Plukker, beste John, toen ik met mijn onderzoeksproject begon was ik erg
onder de indruk van jouw verschijning. Ik heb je gelukkig naast een enorm kundig chirurg,
ook leren kennen als een erg toegankelijke en vriendelijke begeleider. De chirurgische
precisie waarmee je mijn stukken las heeft me menigmaal doen zuchten, maar leidde
uiteindelijk altijd tot een beter eindresultaat. Tijdens onze discussies over mijn onderzoek heb
ik geleerd dat ondanks een totaal verschillende benadering, chirurgen en internisten heel goed
tot een gezamenlijke oplossing kunnen komen.
Prof. dr. R.M.W. Hofstra, beste Robert, bij jou begon dit wetenschappelijke avontuur. Mijn
proefproject bij jou op het lab heeft uiteindelijk geleid tot dit mooie resultaat. Jouw
enthousiasme en relativerende houding hebben me door het eerste deel van mijn promotie
geleid. De werkbesprekingen met jouw vrolijke noot en aanstekelijke lach waren altijd
motiverend, ook als er weer eens een experiment was mislukt. Daarnaast heb ik veel kunnen
leren van je kritische blik en inhoudelijk scherp commentaar.
Mijn dank gaat tevens uit naar de leden van de beoordelingscommissie, Prof. dr. E.G.E. de
Vries, Prof. dr. I.H.M. Borrel Rineks en Prof. dr. W.J.G. Oyen, voor de tijd en energie die zij
hebben gestoken in het lezen en beoordelen van mijn proefschrift.
Ook wil ik alle co-auteurs bedanken voor hun bijdrage; in het bijzonder bedank ik dr. J.W.B.
de Groot, dr. M.M. Alves, drs. J.A.A. Meijer en dr. W.J. Sluiter. Beste Jan Willem, als mijn
voorganger als onderzoeker naar het medullair schildkliercarcinoom, heb je vaak als mijn
voorbeeld gediend. Ik ben dankbaar voor de mogelijkheid om jouw werk op dit onderwerp uit
te breiden en verder te brengen. Dear Maria, without your help on the lab, a large part of my
preclinical work would not have been possible. It was great to work with you and thank you
for all your help. Beste Ton, menigmaal hebben we ‘s avonds uren aan de telefoon gezeten
om alle chirurgie- en pathologieverslagen te beoordelen. Ondanks de afstand en je drukke
agenda hebben we denk ik uiteindelijk een mooi eindresultaat behaald. Dank voor je kritische
inbreng en succes met het afronden van je eigen promotie. Beste Wim, regelmatig heb ik je
opgezocht voor statistische adviezen. Net als velen zat ik naast je op de stoel, waarbij je uitleg
altijd heel logisch leek, maar eenmaal weer terug op m’n eigen plek de toepassing hiervan
toch een stuk lastiger was.

Dankwoord
149
Tevens wil ik de volgende co-auteurs bedanken; Prof. dr. J. Kievit, Prof. dr. J.W. Smit, Prof.
E. van den Heuvel, dr. A.H. Brouwer, dr. A.C. Muller-Kobold. Beste Job, Jan, Adrienne,
Anneke en Edwin, dank voor jullie constructieve commentaar, adviezen en uitleg.
Al mijn collega’s en mede-onderzoekers van de verschillende afdelingen wil ik ook bedanken.
Speciaal wil ik Jan Osinga bedanken, die mij wegwijs heeft gemaakt in het laboratorium en
me de basistechnieken heeft bijgebracht. Daarnaast dank aan Wouter Zandee en Kelvin
Kramp voor het analyseren en beoordelen van de vele operatie- en pathologieverslagen.
Daarnaast ook dank aan mijn kamergenoten op de afdeling Endocrinologie voor de
gezelligheid en afwisseling naast de vele uren achter het computerscherm.
Daarnaast wil ik graag mijn vrienden bedanken voor de nodige ontspanning naast dit
promotietraject. De mooie ploma’s, borrels, feestjes, weekendjes weg en vakanties met de
SaBOOTeurs en Concept 3 waren een fantastische afleiding, die ik zeker niet had willen
missen!
Ook wil ik graag mijn broer en zussen bedanken. Lieve Carolien, Anton, Ingrid en Harriët;
het is geweldig om als jongste broer met jullie in een gezin op te groeien. Ondanks dat we
elkaar misschien minder vaak zien en spreken als we zouden willen, ben ik dankbaar voor de
fijne band die we met elkaar hebben!
Lieve Pap en Mam, dank voor jullie onvoorwaardelijke liefde, steun en interesse! Zonder alle
dingen die ik van jullie heb meegekregen en geleerd zou mijn leven er een stuk anders uit
zien. Ik ben jullie heel erg dankbaar!
Liefste Martine; met jou ben ik al vijf jaar heel gelukkig! Jij bent er voor mij altijd. Ik kijk uit
naar de toekomst om samen met jou te genieten van al het moois wat nog gaat komen!

150

151
Curriculum Vitae
Hans Verbeek werd op 1 september 1985 geboren te Emmen. In 2003 behaalde hij zijn VWO
diploma aan het Katholiek Drenths College te Emmen. Vervolgens begon hij zijn studie
Geneeskunde aan de Rijksuniversiteit Groningen. In 2005 haalde hij tevens zijn propedeuse
Natuurkunde. In aansluiting op een proefproject dat de effecten van tyrosine kinase remmers
op medullair schildkliercarcinoom cellijnen onderzocht begon Hans in 2008 aan een MD-PhD
traject. Dit MD-PhD traject, onder begeleiding van prof. dr. T.P. Links, prof. dr. J.T.M.
Plukker en prof. dr. R.M.W. Hofstra, onderzocht de diagnose en behandeling van primair en
recidiverend medullair schildkliercarcinoom. In januari 2013 rondde Hans zijn studie
Geneeskunde af. In juni 2013 startte hij als arts in opleiding tot internist in het Deventer
Ziekenhuis (opleider dr. C.G. Vermeij) waar hij op dit moment nog steeds werkzaam is.

152

Appendices

Appendices
154
Appendix 1
Search strategy
Search terms
Unless otherwise stated, search terms are free text terms.
Abbreviations:
'$': stands for any character; '?': substitutes one or no character; adj: adjacent (i.e. number of words
within range of search term); exp: exploded MeSH; MeSH: medical subject heading (MEDLINE
medical index term); pt: publication type; sh: MeSH; tw: text word.
The Cochrane Library
#1 MeSH descriptor Thyroid Neoplasms explode all trees
#2 MeSH descriptor Goiter, Nodular explode all trees
#3 ( (thyroid* in All Text near/6 neoplas* in All Text) or (thyroid* in All Text near/6 cancer in All Text)
or (thyroid* in All Text near/6 carcinoma* in All Text) or (thyroid* in All Text near/6
macrocarcinoma* in All Text) or (thyroid* in All Text near/6 microcarcinoma* in All Text) )
#4 ( (thyreoid* in All Text near/6 neoplas* in All Text) or (thyreoid* in All Text near/6 cancer in All
Text) or (thyreoid* in All Text near/6 carcinoma* in All Text) or (thyreoid* in All Text near/6
macrocarcinoma* in All Text) or (thyreoid* in All Text near/6 microcarcinoma* in All Text) )
#5 ( (thyroid* in All Text near/6 tumor* in All Text) or (thyroid* in All Text near/6 tumour* in All Text)
or (thyreoid* in All Text near/6 tumor* in All Text) or (thyreoid* in All Text near/6 tumour* in All
Text) )
#6 ( (thyroid* in All Text near/6 nodul* in All Text) or (thyroid* in All Text near/6 multinodul* in All
Text) or (thyreoid* in All Text near/6 nodul* in All Text) or (thyreoid* in All Text near/6 multinodul*
in All Text) )
#7 MTC in All Text
#8 MeSH descriptor Carcinoma, Medullary explode all trees
#9 (carcinoma* in All Text near/6 medull* in All Text)
#10 (#8 or #9)
#11 (thyroid* in All Text or thyreoid* in All Text)
#12 (#10 and #11)
#13 (#1 or #2 or #3 or #4 or #5 or #6 or #7 or #12)
#14 MeSH descriptor Calcitonin explode all trees
#15 (calcitrin* in All Text or calcitonin* in All Text or thyrocalcitonin* in All Text)
#16 (#14 or #15)
#17 (#13 and #16)
#18 MeSH descriptor Diagnostic Tests, Routine explode all trees
#19 MeSH descriptor Biopsy, Fine-Needle explode all trees
#20 MeSH descriptor Diagnostic techniques, endocrine explode all trees
#21 MeSH descriptor Magnetic resonance imaging explode all trees
#22 MeSH descriptor Ultrasonography explode all trees
#23 MeSH descriptor Biological markers explode all trees
#24 MeSH descriptor Carcinoembryonic antigen explode all trees
#25 MeSH descriptor Diagnostic imaging explode all trees
#26 MeSH descriptor Immunoassay explode all trees
#27 MeSH descriptor Chemiluminescent measurements explode all trees

Appendices
155
#28 diagnos* in All Text
#29 ( (tumor in All Text near/6 marker* in All Text) or (biological in All Text near/6 marker* in All
Text) or (tumour in All Text near/6 marker* in All Text) )
#30 ( (calcitonin* in All Text and test* in All Text) or (pentgastrin* in All Text and test* in All Text) )
#31 (PET-CT in All Text or RET in All Text or MRI in All Text)
#32 (fine in All Text and (needle in All Text near/6 biops* in All Text) )
#33 (MRI in All Text or FNAC in All Text or FNAB in All Text)
#34 CEA in All Text
#35 (cytology in All Text or immunohistochem* in All Text or ultrasonograph* in All Text or
echograph* in All Text)
#36 (imaging in All Text and technique* in All Text)
#37 (RIA in All Text or IRMA in All Text or ILMA in All Text)
#38 (#18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30 or #31
or #32 or #33 or #34 or #35 or #36 or #37)
#39 (#17 and #38)
MEDLINE
1 exp Thyroid Neoplasms/
2 exp Goiter nodular/
3 ((thyroid* or thyreoid*) adj6 (neoplas* or cancer or carcinoma* or macrocarcinoma* or
microcarcinoma* or tumo?r*)).tw,ot.
4 (nodul* adj3 (thyroid* or thyreoid* or goiter)).tw,ot.
5 ((thyroid* or thyreoid*) adj3 (multinodul* or multi nodul*)).tw,ot.
6 MTC*.ab.
7 or/1-6
8 exp Carcinoma, medullary/
9 (medullary adj6 (thyroid* or thyreoid*)).tw,ot.
10 8 or 9
11 (thyroid* or thyreoid*).tw,ot.
12 10 and 11
13 7 or 12
14 exp Calcitonin/
15 (Calcitrin* or calcitonin*).tw,ot.
16 thyrocalcitonin*.tw,ot.
17 9007-12-9.rn.
18 or/14-17
19 (screen* or detect*).tw,ot.
20 exp Diagnostic Tests, Routine/
21 exp Biopsy, Fine-Needle/
22 exp Diagnostic Techniques, Endocrine/
23 exp Magnetic Resonance Imaging/
24 exp Ultrasonography/
25 exp Biological markers/
26 exp Carcinoembryonic antigen/
27 exp diagnostic imaging/
28 exp Pentagastrin/du [Diagnostic Use]
29 exp Immunoassay/
30 Carcinoma, medullary/di [diagnosis]
31 chemiluminescent.mp.
32 ((tumo?r or biological) adj6 marker*).tw,ot.
33 diagnos*.tw,ot.

Appendices
156
34 (RIA or IRMA or ILMA).tw,ot.
35 calcitonin* test*.tw,ot.
36 PET-CT.mp.
37 RET.mp.
38 fine needle aspiration*.tw,ot.
39 pentagastrin-test*.tw,ot.
40 MRI.tw,ot.
41 (MRI or FNAC or FNAB).tw,ot.
42 (cytology or immunohistochem* or ultrasonograph* or echograph*).tw,ot.
43 CEA.tw,ot.
44 imaging technique*.tw,ot.
45 or/19-44
46 13 and 18 and 45
47 (animals not (animals and humans)).sh.
48 46 not 47
EMBASE
1 thyroid tumor/
2 exp thyroid cancer/
3 exp thyroid nodule/
4 exp thyroid medullary carcinoma/
5 exp nodular goiter/
6 ((thyroid* or thyreoid*) adj6 (neoplas* or cancer or carcinoma* or macrocarcinoma* or
microcarcinoma* or tumo?r)).tw,ot.
7 ((thyroid* or thyreoid*) adj6 medullary carcinoma*).tw,ot.
8 (nodul* adj3 (thyroid* or thyreoid*)).tw,ot.
9 ((thyroid* or thyreoid*) adj3 (multinodul* or multi nodul*)).tw,ot.
10 MTC*.tw,ot.
11 or/1-10
12 exp calcitonin/
13 (calcitrin* or calcitonin* or thyrocalcitonin*).tw,ot.
14 9007-12-9.rn.
15 or/12-14
16 11 and 15
17 exp diagnostic test/
18 exp needle biopsy/
19 exp endocrine system examination/
20 exp nuclear magnetic resonance imaging/
21 exp echography/
22 exp biological marker/
23 exp carcinoembryonic antigen/
24 exp diagnostic imaging/
25 exp immunoassay/
26 exp chemiluminescent/
27 pentagastrin test.mp.
28 exp medullary carcinoma/di [Diagnosis]
29 ((tumo?r or biological) adj6 marker*).tw,ot.
30 diagnos*.tw,ot.
31 (RIA or IRMA or ILMA).tw,ot.
32 ((calcitonin* or pentagastrin*) adj6 test*).tw,ot.
33 (screen* or detect*).tw,ot.

Appendices
157
34 PET-CT.mp.
35 RET.mp.
36 needle biop*.tw,ot.
37 (MRI or FNAC or FNAB).tw,ot.
38 (cytology or immunhistochem* or ultrasonograph* or echograph*).tw,ot.
39 CEA.tw,ot.
40 imaging technique*.tw,ot.
41 or/17-40
42 16 and 41
43 limit 42 to human
Web of Science
# 1 Topic=(thyroid* tumor*) OR Topic=(thyroid* cancer) OR Topic=(thyroid* neoplas*) OR
Topic=(thyroid* carcinoma*) OR Topic=(thyroid* microcarcinoma*) OR Topic=(thyroid*
macrocarcinoma) OR Topic=(thyroid* medullary carcinoma*) OR Topic=(thyroid* nodul*) OR
Topic=(thyroid* multinodul*) OR Topic=(nodul* goiter*)
# 2 Topic=(thyreoid* tumor*) OR Topic=(thyreoid* cancer) OR Topic=(thyreoid* neoplas*) OR
Topic=(thyreoid* carcinoma*) OR Topic=(thyreoid* microcarcinoma*) OR Topic=(thyreoid*
macrocarcinoma) OR Topic=(thyreoid* medullary carcinoma*) OR Topic=(thyreoid* nodul*) OR
Topic=(thyreoid* multinodul*) OR Topic=(nodul* goiter*) OR Topic=(MTC)
# 3 Topic=(calcitonin*) OR Topic=(calcitrin*) OR Topic=(thyrocalcitonin*)
# 4 #1 OR #2
# 5 #3 AND #4
# 6 Topic=(diagnostic test*) OR Topic=(needle biopsy) OR Topic=(endocrine examination*) OR
Topic=(echograph*) OR Topic=(ultrasonograph*) OR Topic=(magnetic resonance imaging) OR
Topic=(MRI) OR Topic=(biological marker*) OR Topic=(diagnostic imaging) OR Topic=(immunoassay)
OR Topic=(chemiluminescent*) OR Topic=(tumor marker*)
# 7 Topic=(carcioembryonic antigen) OR Topic=(CEA) OR Topic=(pentagastrin test*) OR
Topic=(diagnos*) OR Topic=(calcitonin* test*) OR Topic=(screen*) OR Topic=(detect*) OR Topic=(RIA)
OR Topic=(IRMA) OR Topic=(ILMA) OR Topic=(PET-CT) OR Topic=(RET)
# 8 Topic=(FNAC) OR Author=(FNAB) OR Publication Name=(cytology) OR Topic=(immunhistochem*)
OR Topic=(imaging technique*)
# 9 #6 OR #7 OR #8
# 10 #5 AND #9
# 11 Topic=(animal*)
# 12 #10 NOT #11
'My NCBI' alert service
("thyroid nodule"[MeSH Terms] OR ("thyroid"[All Fields] AND "nodule"[All Fields]) OR "thyroid
nodule"[All Fields]) AND ("calcitonin"[MeSH Terms] OR "calcitonin"[All Fields])

Appendices
158
Appendix 2
Additional Table 2 Data extraction form
Design
Design:
Inclusion criteria:
Exclusion criteria:
Patient characteristics
and setting
Number of participants:
Number with NTD:
Number with NTD and calcitonin testing:
Sex (female%):
Age (mean/SD): range:
MTC:
Type of thyroid nodules:
Thyroid nodules detected by palpation or US:
Nodule size:
Number of nodules:
Sonographic morphology of thyroid nodules:
FNA procedures performed through ultrasound guidance or palpation:
Setting:
Country:
Index test
Index test:
Calcitonin as a triage or add-on test:
Used calcitonin assay:
Stimulated calcitonin performed:
Indication stimulated calcitonin:
Stimulative:
Dose:
Time:
Reported and extracted cut-off values
Basal:
Stimulated:
Reference standard
Target condition:
Reference standards:
Indication surgical treatment:
Type of surgical treatment:
Calcitonin negative (n)
Number FNA:
Number operated:
Calcitonin positive (n)
Number FNA:
Number operated:
Flow and timing
Follow-up calcitonin negative:
Type:
Duration:
Follow-up calcitonin positive:
Type:
Duration:

Appendices
159
Appendix 3
QU
AD
AS
-2 S
ign
all
ing
qu
est
ion
s fo
r b
ias
Do
ma
in
Sig
na
llin
g q
ue
stio
n
Cri
tera
Ye
s U
ncl
ea
r N
o
Pa
tie
nt
sele
ctio
n
1.
Co
nse
cuti
ve
or
ran
do
m s
am
ple
en
roll
ed
?
A c
on
secu
tive
or
ran
do
m s
am
ple
of
pa
tie
nts
we
re e
nro
lle
d in
th
e
stu
dy.
It is
un
cle
ar
wh
eth
er
a
con
secu
tive
or
ran
do
m s
am
ple
of
pa
tie
nts
wa
s e
nro
lled
in t
he
stu
dy.
Th
ere
wa
s n
o c
on
secu
tive
or
ran
do
m s
am
ple
incl
ud
ed
in
the
stu
dy
(e.g
. o
nly
pa
tie
nts
alr
ea
dy
in s
usp
icio
n o
f
(me
du
llary
) th
yro
id
ma
lign
an
cy a
nd
pa
tie
nts
wit
h
hig
h r
isk
for
(fa
mili
al)
MT
C.
2.
Ca
se c
on
tro
l d
esi
gn
av
oid
ed
?
Th
ere
wa
s n
o c
ase
co
ntr
ol d
esi
gn
. It
is u
ncl
ea
r if
th
ere
wa
s a
ca
se
con
tro
l de
sig
n
Th
ere
wa
s a
ca
se c
on
tro
l
de
sig
n
3.
Ina
pp
rop
ria
te
ex
clu
sio
ns
av
oid
ed
?
Th
ere
are
no
pa
tie
nts
ina
pp
rop
ria
te e
xclu
de
d (
e.g
.
pa
tie
nts
wit
h s
usp
icio
us
US,
wh
o
will
alr
ea
dy
be
op
era
ted
on
)
It is
un
cle
ar
if t
he
re w
as
avo
ida
nce
of
ina
pp
rop
ria
te
exc
lusi
on
s
Th
ere
is
ina
pp
rop
ria
te
exc
lusi
on
of
pa
tie
nts
(e
.g.
exc
lusi
on
of
pa
tie
nts
wit
h
hig
h r
isk
of
ma
lign
an
cy)
Ind
ex
te
st
1.
Ind
ex
te
st r
esu
lts
inte
rpre
ted
wit
ho
ut
kn
ow
led
ge
re
sult
s
refe
ren
ce s
tan
da
rd?
Th
is it
em
will
be
om
itte
d a
s o
nly
stu
die
s a
re in
clu
de
d in
wh
ich
th
e r
efe
ren
ce s
tan
da
rd
(his
top
ath
olo
gic
al e
xam
ina
tio
n)
is p
erf
orm
ed
aft
er
calc
ito
nin
te
stin
g.
Furt
he
rmo
re c
alc
ito
nin
te
stin
g i
s
a o
bje
ctiv
e t
est
(a
lth
ou
gh
inte
rpre
tati
on
de
pe
nd
s o
n t
he
th
resh
old
, b
ut
this
will
be
ass
ess
ed
in t
he
ne
xt it
em
)
2.
Pre
-sp
eci
fie
d
thre
sho
ld?
Th
ere
wa
s a
pre
-sp
eci
fie
d
calc
ito
nin
cu
t-o
ff l
eve
l.
It is
un
cle
ar
if t
he
re w
as
a p
re-
spe
cifi
ed
cu
t-o
ff l
eve
l
Th
ere
wa
s n
o p
re-s
pe
cifi
ed
calc
ito
nin
cu
t-ff
le
vel.

Appendices
160
Q
UA
DA
S-2
Sig
na
llin
g q
ue
stio
ns
for
bia
s
Do
ma
in
Sig
na
llin
g q
ue
stio
n
Cri
tera
Ye
s U
ncl
ea
r N
o
Re
fere
nce
sta
nd
ard
1.
Re
fere
nce
sta
nd
ard
lik
ely
to
co
rre
ctly
cla
ssif
y
targ
et
con
dit
ion
?
In p
ati
en
s re
ceiv
ing
su
rge
ry
the
re is
ad
eq
ua
te
his
top
ath
olo
gic
al e
xam
ina
tio
n
of
thyr
oid
tis
sue
.
In p
ati
en
ts r
ece
ivin
g f
oll
ow
-up
,
the
re is
at
lea
st t
hre
e y
ea
rs
follo
w-u
p y
ea
rs in
clu
din
g a
t
lea
st o
ne
US
exa
min
ati
on
an
d if
ind
ica
ted
FN
AC
.
In p
ati
en
ts r
ece
ivin
g s
urg
ery
it's
un
cle
ar
ho
w h
isto
pa
tho
log
ica
l
exa
min
ati
on
is p
erf
orm
ed
.
In p
ati
en
ts r
ece
ivin
g f
oll
ow
-up
the
tim
e a
nd
pro
toco
l fo
r
follo
w-u
p is
un
cle
ar
In p
ati
en
ts r
ece
ivin
g s
urg
ery
his
top
ath
olo
gic
al e
xam
ina
tio
n
is n
ot
ad
eq
ua
te.
In p
ati
en
ts w
ith
ou
t su
rge
ry,
follo
w-u
p is
to
sh
ort
or
do
es
no
t
incl
ud
e a
t le
ast
on
e U
S
exa
min
ati
on
an
d F
NA
C.
2.
Re
fere
nce
sta
nd
ard
resu
lts
inte
rpre
ted
wit
ho
ut
kn
ow
led
ge
resu
lts
ind
ex
te
st?
Th
e o
utc
om
e a
sse
sso
r o
f
his
top
ath
olo
gic
al a
nd
fo
llow
-up
resu
lts
wa
s n
ot
aw
are
of
calc
ito
nin
te
stin
g r
esu
lts
It is
no
t cl
ea
r if
th
e o
utc
om
e
ass
ess
or
of
his
top
ath
olo
gic
al
an
d f
ollo
w-u
p r
esu
lts
wa
s
aw
are
of
calc
ito
nin
te
stin
g
resu
lts
Th
e o
utc
om
e a
sse
sso
r o
f
his
top
ath
olo
gic
al a
nd
fo
llow
-up
resu
lts
wa
s a
wa
re o
f ca
lcit
on
in
test
ing
re
sult
s
Flo
w a
nd
tim
ing
1.
Ap
pro
pri
ate
in
terv
al
be
twe
en
in
de
x t
est
an
d
refe
ren
ce s
tan
da
rd?
Tim
e b
etw
ee
n c
alc
ito
nin
te
stin
g
an
d h
isto
pa
tho
log
ica
l
exa
min
ati
on
is <
3 m
on
ths
It is
un
cle
ar
wh
at
the
tim
e
pe
rio
d b
etw
ee
n r
efe
ren
ce
sta
nd
ard
an
d in
de
x te
st is
.
Tim
e b
etw
ee
n c
alc
ito
nin
te
stin
g
an
d h
isto
pa
tho
log
ica
l exc
ee
ds
3
mo
nth
s.
2.
All
pa
tie
nts
re
ceiv
ed
refe
ren
ce s
tan
da
rd?
All
pa
tie
nts
re
ceiv
ed
su
rge
ry,
an
d p
ati
en
ts w
ho
did
no
t
rece
ive
su
rge
ry h
ave
clin
ica
l
follo
w-u
p o
f a
t le
ast
th
ree
yea
rs.
It is
no
t cl
ea
r if
th
e w
ho
le
sam
ple
did
re
ceiv
e s
urg
ery
or
follo
w-u
p.
On
ly a
se
lect
ed
su
bse
t o
f th
e
pa
tie
nts
re
ceiv
ed
or
surg
ery
or
no
t a
ll p
ati
en
ts h
ave
clin
ica
l
follo
w-u
p.
3.
Pa
tie
nts
re
ceiv
ed
sam
e r
efe
ren
ce
sta
nd
ard
?
All
pa
tie
nts
we
re o
pe
rate
d a
nd
his
top
ath
olo
gic
al e
xam
ina
tio
n
of
the
th
yro
id w
as
pe
rfo
rme
d.
It is
no
t cl
ea
r if
all
pa
tie
nts
we
re
op
era
ted
an
d r
ece
ive
d
his
top
ath
olo
gic
al e
xam
ina
tio
n.
No
t a
ll p
ati
en
ts w
ere
op
era
ted
or
his
top
ath
olo
gic
al
exa
min
ati
on
wa
s n
ot
pe
rfo
rme
d in
all
pa
tie
nts
.
4.
All
pa
tie
nts
in
clu
de
d i
n
the
an
aly
sis?
All
pa
tie
nts
en
roll
ed
we
re
incl
ud
ed
in t
he
an
aly
sis
It is
no
t cl
ea
r if
all
pa
tie
nts
we
re
incl
ud
ed
in t
he
an
aly
sis.
No
t a
ll p
ati
en
ts e
nro
lled
we
re
incl
ud
ed
in t
he
an
aly
sis
(e.g
.
pa
tie
nts
lost
to
fo
llow
-up
)

Appendices
161
Appendix 4
Characteristics of included studies
Rieu 1995 Patient Selection
A. Risk of Bias
Patient Sampling Design: Prospective cohort study.
Inclusion criteria: Pts with thyroid nodules detected by clinical examination or with
abnormal TSH levels or both.
Exclusion criteria: Not reported.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 657 patients.
Number with NTD: 469 patients.
Number with NTD and calcitonin testing: 469 patients.
Sex (female%): 88,1% (579/657); only reported of whole study population.
Age (mean/SD): 45, SD: Not reported range: 15-87 years; only reported of whole study
population.
MTC: 4 patients.
Type of thyroid nodules: non toxic uninodular goitre (n = 136), autonomously functioning
thyroid nodule (n = 14), non toxic multinodular goitre (n = 224), toxic multinodular goitre (n =
15), nodular Hashimoto thyroiditis (n = 53), nodular Graves' disease (n = 25), nodular
formation related to subacute thyroiditis in a hyperthyroid phase (n = 2).
Thyroid nodules detected by palpation or US: both, number not specified.
Nodule size: not reported.
Number of nodules: Uninodular (n = 150), multinodular (n = 239), not reported (n = 80).
Sonographic morphology of thyroid nodules: A localized thyroid area was considered
nodular when it had a distinctive rim at two different incidences. When this rim was absent, a
thyroid area with round or oval patterns, and also echogenicity different from that of the
surrounding normal tissue, was classified as nodular.
FNA procedures performed through ultrasound guidance or palpation: Not
reported.
Setting: Not reported.
Country: France
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal and stimulated calcitonin.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay:
01-1989 – 12-1989, RIA (Mallinckrodt Medical SA, Evry, France).
01-1990 – 12- 1993: IRMA (CIS-Oris International, Saint Quentin en Yvelins, France.
Stimulated calcitonin: Yes.
Indication: Patients with basal serum CT above normal range.
Stimulative: Pentagastrin.
Dose: 0.5 ug/kg.

Appendices
162
Time: 0, 3, 5, 15 and 30 min after injection.
Reported and extracted cut-off values
Basal: reported: RIA: 35 ng/l, IRMA 10 ng/l; extracted 50 ng/l; 100 ng/l.
Stimulated: reported: 100 ng/l; extracted 100 ng/l.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNA in patients whose nodular formation was accessible to such a
procedure, in selected patients histopathological examination after surgery.
Indication surgical treatment: Patients with increased basal serum CT values, pentagastrin
stimulated CT levels > 100 pg/l, regardless of FNAC result, FNAC suggestive of thyroid
carcinoma (n = 7), compressive goitre (n = 4).
Type of surgical treatment: For suspected MTC total thyroidectomy and central neck
dissection. Bilateral modified neck dissection was performed only in the presence of evident
lymph node involvement in one or both sides. For all other types of thyroid carcinoma, total
thyroidectomy and lymph node dissection on the side of the thyroid nodule(s) or bilaterally
(as appropriate).
Calcitonin negative (n = 465)
Number FNAC: Not reported.
Number operated: 11 patients.
Calcitonin positive (n = 4)
Number FNAC: 4 patients.
Number operated: 4 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results of
the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Not reported.
Type: -
Duration: -
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No

Appendices
163
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Not reported.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: "to asses the prevalence of sporadic MTC in nodular and non -
nodular thyroid diseases by routine basal serum CT measurements"
Abbreviations FNAC: fine needle aspiration cytology, CT: calcitonin.
Notes

Appendices
164
Ozgen 1999
Patient Selection
A. Risk of Bias
Patient Sampling Design: Prospective study.
Inclusion criteria: Patients with nodular goiter.
Exclusion criteria: Patients with previously known medullary
carcinoma and their relatives.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 773 patients.
Clinical features: Patients with nodular goiter.
Number with NTD: 773 patients.
Number with NTD and calcitonin testing: 773 patients.
Sex (female%)(n): 75,8% (586).
Age (mean/SD): range: 42.1 years, range 17-78.
Number with MTC: 4 patients.
Type of thyroid nodules: Multinodular goiter (nontoxic/toxic), solitary (nontoxic/toxic)
thyroid nodules.
Thyroid nodules detected by palpation or US: Both; number not specified.
Nodule size: Not reported.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Both (US guidance in
nonpalpable nodules), number not specified.
Setting: Outpatient clinic.
Country: Turkey.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal calcitonin.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay: Commercial kit; DSL-5200 Ultrasensitive calcitonin RIA kit, Diagnostic
System Laboratories Inc., Webster, Tx.
Sensitivity: Not reported.
Stimulated calcitonin: No
Indication: -
Stimulative: -
Dose: -
Time: -
Reported and extracted cut-off values
Basal: Reported: 30 pg/ml; extracted:30 pg/ml, 50 pg/ml, 100 pg/ml.
Stimulated: -
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability

Appendices
165
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern
Reference Standard
A. Risk of Bias
Target condition and
reference standard(s)
Target condition: MTC.
Reference standards: FNAB and in selected cases histopathological examination after
surgery,
Indication surgical treatment: Malignant or suspicious results in FNAB, or elevated
calcitonin levels regardless of the result of FNAB.
Type of surgical treatment: Thyroid surgery.
Calcitonin negative (n = 669)
Number FNAB: 669 patients.
Number operated: 171 patients.
Calcitonin positive (n = 4)
Number FNAB: 4 patients.
Number operated: 4 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference
standard does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Described for 3 MTC patients.
Type: Basal and stimulated calcitonin levels.
Duration: 14-18 months
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Not reported.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: " To identify MTC by screening patients who have thyroid nodules
with basal calcitonin measurements and to determine whether basal serum calcitonin
measurement should be a part of the routine evaluation of a nodular goiter."
Abbreviations FNAB: Fine needle aspiration biopsy.
Notes

Appendices
166
Hahm 2001
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study.
Inclusion criteria: Patients with nodular thyroid disease.
Exclusion criteria: Not reported.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 1448 patients.
Number with NTD: 1448 patients.
Number with NTD and calcitonin testing: 1448 patients.
Sex (female%)(n): 80,3% (1163).
Age (mean/SD): 46 years Range: 14-86 years.
Number with MTC: 10 patients.
Type of thyroid nodules: Not reported.
Thyroid nodules detected by palpation or US: Not reported.
Nodule size: Not reported.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Thyroid clinic of Samsung Medical Center.
Country: Korea.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal and stimulated calcitonin.
Used calcitonin assay: Two-site immunoradiometric assay commercial kit (MED-GENIX CT-
US.-IRMA kit) BioSource Europe S.A.,Belgium.
Sensitivity: 0.8 pg/ml.
Stimulated calcitonin: Yes.
Indication: Reported for 39 patients: basal calcitonin > 10 pg/ml (n=23), family members of
MEN2 or MTC patients (n=14) and FNAC findings suspicious for MTC (n=2).
Stimulative: Pentagastrin (Peptavlon, Ayerst Laboratories Ind. Philadelphia, PA).
Dose: 0.5 ug/kg body weight.
Time: Just before, 2, 5, and 10 min.
Reported and extracted cut-off values
Basal: Reported: 10 pg/ml (n = 56); extracted: 10, 20, 30, 50, 100 pg/ml.
Stimulated: Reported: 100 pg/ml; extracted: 100, 200 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern

Appendices
167
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNAC in all patients with palpable or visible thyroid nodule by US, in
selected patients histopathological examination after surgery.
Indication surgical treatment: Abnormal findings suspicious of malignancy by FNAC, patients
who had basal or stimulated calcitonin concentrations of more than 100 pg/ml.
Type: Thyroidectomy.
Calcitonin negative (n = 1392 patients)
Number FNAC: Not reported.
Number operated: 169 patients.
Calcitonin positive (n = 56 patients)
Number FNAC: 55 patients.
Number operated: 25 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported
Type: -
Duration: -
Follow-up calcitonin positive: Not reported
Type:
Duration:
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English
FUNDING: OTHER FUNDING
PUBLICATION STATUS: PEER REVIEW JOURNAL / JOURNAL SUPPLEMENT / FULL ARTICLE /
CONFERENCE PAPER / OTHER)
Stated aim of
study
Quote from publication: "To evaluate the usefulness of routine measurement of serum
calcitonin concentration in patients with nodular thyroid diseases, and to identify the validity
of pentagastrin simulation test and FNAC "
Abbreviations US: Ultrasonography, FNAC: Fine needle aspiration cytology.
Notes

Appendices
168
Hatzl-Griesenhofer 2002
Patient Selection
A. Risk of Bias
Patient Sampling Design: Retrospective cohort study.
Inclusion criteria: Patients with nodular thyroid disease or with evidence of nodular growth
in follow-up examinations.
Exclusion criteria: Not reported.
Was a consecutive or random sample of patients enrolled? Unclear
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? High risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 3899 patients.
Number with NTD: 3899 patients.
Number with NTD and calcitonin testing: 3899 patients.
Sex (female%)(n): 78,8% (3073).
Age (mean/SD): 54.6 (+11.2) yrs range: 6 - 90 yrs.
Number with MTC: 12 patients.
Type of thyroid nodules: Not reported.
Thyroid nodules detected by palpation or US: Not reported.
Nodule size: Not reported.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Only reported for MTC patients.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Outpatient ward of the department of Nuclear Medicine and Endocrinology of the
General Hospital Linz.
Country: Austria.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal and stimulated calcitonin.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay: a two-site chemoluminesence immunoassay, Nichols institute diagnostics.
Sensitivity: 0.7 pg/ml
Stimulated calcitonin: Yes.
Indication: Patients with slightly or moderately elevated normal calcitonin levels (< 80 pg/ml).
Stimulative: Pentagastrin, Peptavlon, Zeneca, Vienna.
Dose: 0.5 ug/kg.
Time: before, 2, 5, and 8 min.
Reported and extracted cut-off values
Basal: Reported: females: 4.6 pg/ml; males 11.5 pg/ml; extracted: females: 4.6 pg/ml; males 11.5
pg/ml.
Stimulated: Reported:100 pg/ml (males and females); extracted: 100 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern

Appendices
169
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: Histological evaluation in patients referred to surgery.
Indication surgical treatment: Markedly elevated bCT and positive pentagastrin stimulation
tests.
Type: Hemithyroidectomy, (sub)total thyroidectomy, node dissection in selected patients.
Calcitonin negative ( n = 3639 patients)
Number FNA: -
Number operated: Not reported.
Calcitonin positive (n= 230 patients)
Number FNA: -
Number operated: 39 patients (?)
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported
Type: -
Duration: -
Follow-up calcitonin positive: (1) Patients with pathological stimulation test in which the
consultant for internal medicine dissuaded against surgery because of elevated risks (n =2).
(2) patients with elevated basal calcitonin levels who declined pentagastrin stimulation (n
=41).
Type: (1) Ultrasound and determination of basal and stimulated calcitonin (2) clinical and
biochemical follow up.
Number with follow-up: 43 patients.
Duration: Not reported
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? No
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English
FUNDING: Not reported
PUBLICATION STATUS: Full article
Stated aim of
study
Quote from publication: "To evaluate retrospectively the results of routine calcitonin
measurements in patients with nodular thyorid disease "
Abbreviations bCT: basal calcitonin,
Notes

Appendices
170
Elisei 2004
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study.
Inclusion criteria: Patients with nodular thyroid disease.
Exclusion criteria: Not reported.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 10864 patients.
Number with NTD: 10864 patients.
Number with NTD and calcitonin testing: 10864 patients.
Sex (female%)(n): 81.4% (8692).
Age (mean/SD): 49 yr SD not reported Range: 12 - 82 yr.
MTC: 44 patients.
Type of thyroid nodules: Single nodules, nontoxic multinodular goiter, autonomous
functioning thyroid nodules, and autoimmune thyroid disease associated with distinct cold
nodules.
Thyroid nodules detected by palpation or US: Not reported.
Nodule size: Not reported.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Not reported.
Country: Italy
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal and stimulated calcitonin.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay: Solid phase 2 site immunoradiometric assay (ELSA-hCT, CIS, Gif Sur
Yvette, France).
Sensitivity: 14 pg/ml.
Stimulated calcitonin: Yes.
Indication: Patients with detectable levels of basal CTand twice confirmed.
Stimulative: Pentagastrin.
Dose: 0.5 ug/kg.
Time: before, 2, 5, 15 and 30 min.
Reported and extracted cut-off values
Basal: reported: 20 pg/ml; extracted: 20 pg/ml.
Stimulated: reported 60 pg/ml; extracted: 60, 100 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern

Appendices
171
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNAC in nodules > 1 cm or in nodules < 1 cm with suspicious aspects at
neck US, in selected patients histopathological examination after surgery.
Indication surgical treatment: Patients with elevated bCT levels (confirmed by abnormal Pg-
stimulated CT levels) regardless of the results of FNAC and in those with FNAC suspicious of
malignancy indepently from the results of serum CT.
Type:Total thyroidectomy and dissection of the central neck compartment
Calcitonin negative (n = 10817)
Number FNAC: Not reported.
Number operated: Not reported.
Calcitonin positive (n = 47)
Number FNAC: 47 patients.
Number operated: 44 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Only reported of MTC patients.
Type: Not reported.
Number with follow-up: 44 patients.
Duration: Mean 6.2 + 2.5 yr (range, 3-10 yr).
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? No
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Non-commercial.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: "To asses whether we could confirm the results of our preliminiary
study of 1991 and to compare the outcome of patients diagnosed by serum CT measurement
with that of a historical group of MTC patients diagnosed and treated before the introduction
of serum CT screening".
Abbreviations CT: Calcitonin, FNAC: fine needle aspiration cytology, US: Ultrasonography.
Notes

Appendices
172
Karanikas 2004
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study
Inclusion criteria: Patients referred for the work-up of various suspected thyroid disorders.
Exclusion criteria: Not reported.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 414 patients.
Number with NTD: 195 patients.
Number with NTD and calcitonin testing: 195 patients.
Sex (female%)(n): 79.5% (329) NB only reported for whole study population.
Age (mean/SD): 56 year; SD not reported range: 18 - 88 years, NB only reported for whole
study population.
MTC: 1 patients. (1 MTC patient in non-nodular study population)
Type of thyroid nodules: Uni and multinodular disease.
Thyroid nodules detected by palpation or US: Not reported.
Nodule size: Only for patients with elevated CT; volume 21 + 10 ml.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Out-patient department.
Country: Austria.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Calcitonin as a triage or add-on test: Not reported.
Index test: Basal and stimulated calcitonin.
Used calcitonin assay: Commercial assay by a Nichols Advantage Chemiluminescence System
(Nichols Institute Diagnostics, San Juan Capistrano, Ca, USA)
Sensitivity: 1 pg/ml.
Stimulated calcitonin: Yes.
Indication: Basal serum CT equal to or exceeding 10 pg/ml.
Stimulative: Pengagastrin Injection BP, Cambridge Laboratories, Tyne & Wear, UK
Dose: 0.5 ug/kg
Time: Before, 2 and 5 min after injection.
Reported and extracted cut-off values
Basal: reported: 10 pg/ml; extracted: 10 pg/ml, 100 pg/ml.
Stimulated: reported: 100 pg/ml (abnormal), 500 pg/ml (pathological); extracted 100 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern

Appendices
173
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: In selected patients histological examination after total thyroidectomy,
follow-up.
Indication surgical treatment: Patients with abnormal and pathological PG tests.
Type of surgical treatment: Total thyroidectomy and lymph node dissection along both
recurrent nerves in patients.
Calcitonin negative (n = 182)
Number FNAC: -
Number operated: Not reported.
Calcitonin positive (n = 13)
Number FNAC: -
Number operated: 1 patient.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Only for MTC patient.
Type: Basal and stimulated CT.
Number with follow-up: 1.
Duration: Not reported
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Not reported.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: "To compare the distribution and relevance of elevated CT levels in
referrals with nonneoplastic and neoplastic thyroid disease (...)"
Abbreviations CT: calcitonin.
Notes

Appendices
174
Vierhapper 2005
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study.
Inclusion criteria: Patients with suspected thyroid disorders.
Exclusion criteria: Patients with a known elevation of hCT.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 25669 patients.
Number with NTD: 10292 patients.
Number with NTD and calcitonin testing: 10157 patients.
Sex (female%)(n): 79.9% (8114).
Age (mean/SD): Not reported range: Not reported.
MTC: 36 patients.
Type of thyroid nodules: Not reported.
Thyroid nodules detected by palpation or US: Both.
Nodule size: Only reported of MTC patients.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Thyroid outpatient clinic.
Country: Austria
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal and stimulated calcitonin.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay:
1994-1999: A commercially available immunoradiometric assay (CIS-biointernational, Gif-Sur-
Yvette, France).
1999-2004: Acridinium-ester-labeled chemiluminescent immunoassay, running on the
‘Advantage’ auto-analyser (Nichols Institute Diagnostics, US).
Sensitivity: Not reported.
Stimulated calcitonin: Yes.
Indication: All patients with basal hCT> 10.0 pg/ml.
Stimulative: Pentagastrin (CambridgeLaboratories, Wallsend, UK).
Dose: 0.5 ug/kg.
Time: Prior to, 2, 5 and 10 min.
Reported and extracted cut-off values
Basal: Reported: 10 pg/ml extracted: 10 pg/ml.
Stimulated: Reported 100 pg/ml extracted: 100 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from Low concern

Appendices
175
the review question?
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNAB, in selected patients histopathological examination after surgery,
follow-up.
Indication surgical treatment: Elevated basal and/or pentagastrin stimulated serum
concentrations of hCT(>100 pg/ml) or cytological findings.
Type: In patients with elevated basal and/or stimulated calcitonin a total thyroidectomy was
performed. Routinely both recurrent nerves were dissected carfully and a systematic
microdissection of the central lymph node compartment. If MTC was documented
intraoperatively a systematic bilateral microdissection of the lateral lymph node
compartments was added.
Calcitonin negative (n = 9960)
Number FNA: Not reported.
Number operated: Not reported, at least 1 pt.
Calcitonin positive (n = 507)
Number FNAB: 15 patients (only reported for MTC patients)
Number operated: 75 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference
standard does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Only reported of MTC patients.
Type: stimulated hCTs.
Number with follow-up: 32 patients.
Duration: 1-9 years.
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? No
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication details LANGUAGE OF PUBLICATION: English.
FUNDING: Non-commercial.
PUBLICATION STATUS: Full article.
Stated aim of study Quote from publication: Not reported.
Abbreviations hCT; serum calcitonin.
Notes

Appendices
176
Papi 2006
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study of consecutive patients.
Inclusion criteria: (1) male & female pts > 18 yrs (2) palpable nodules (3) non-palpable
nodules > 10 mm (4) non palpable nodule < 10 mm with malignant features on US.
Exclusion criteria: (1) patients < 18 years (2) non palpable nodules < 10 mm without
malignant US features (3) pts previously evaluated for nodular goiter by FNA and/or CT
measurement (4) patients reporting familial history of MEN and pts with known MTC (5) pts
with hyper- and hypothyroidism without thyroid nodules (6) patients in follow-up for thyroid
disease (7) patients not confirmed as having thyroid diseases.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 1474 patients.
Number with NTD: 1474 patients.
Number with NTD and calcitonin testing: 1425 patients.
Sex (female%)(n): 80% (1144).
Age (mean/SD): 49.6(+ 6.8) yr range: 18 - 91 yr.
MTC: 9 patients.
Type of thyroid nodules: Euthyroid nodular thyroid disease (n = 1369), hypothyroid nodular
thyroid disease (n = 32), sub acute de Quervain's thyroiditis (n = 1), Graves' disease (n=2),
toxic nodular goiter (n = 21).
Thyroid nodules detected by palpation or US: both.
Nodule size: 21.8 + 4 mm
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Ultrasound.
Setting: Not reported.
Country: Italy.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal and stimulated calcitonin.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay: Two-site chemiluminesence assay, Nichols instute diagnostics, San
Juan Capristano, CA92675, USA).
Sensitivity: 1 pg/ml.
Stimulated calcitonin: Yes.
Indication: When basal serum CT concentrations exceeded 5 pg/ml, but not exceeded 100
pg/ml.
Stimulative: Pentagastrin (Cambridge laboratories, Walsend, Tyne and Wear, NE289NX).
Dose: 0.5 ug/kg.
Time: Before, 2, 5 and 10 min after injection.
Reported and extracted cut-off values
Basal: Reported: 5 pg/ml extracted: 5, 10, 15, 20, 30, 50,100 pg/ml.
Stimulated: Reported: 100 pg/ml extracted: 100, 200 pg/ml.
A. Risk of Bias

Appendices
177
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNAC and in selected patients, histopathological examination after
surgical treatment.
Indication surgical treatment: Basal serum CT concentrations > 5 pg/ml < 100 pg/ml and Pg-
stimulated CT levels > 100 pg/ml or basal serum CT concentrations > 100 pg/ml; patients with
a suspicious or repeatedly non-diagnostic FNAC and patients with a benign FNAC and
compressive symptoms.
Type: In patients with benign FNAC and compressive symptoms a lobectomy or near-total
thyroidectomy. In patients with suspicious or non-diagnostic FNAC, surgical extent depended
on histological examination of frozen sections. In patients with malignancy other than MTC a
total thyroidectomy and in case of lymph node involvement a lymphadenectomy. In MTC
patients a total thyroidectomy and a systematic microdissection of both central neck and
bilateral neck compartments. Contralateral lymph node dissection was omitted in MTC
patients with a unilateral thyroid tumor and no ipsilateral and central lymph node
involvement.
Calcitonin negative (n = 1402)
Number FNAC: 1402 patients.
Number operated: 292 patients.
Calcitonin positive: (n = 23)
Number FNAC: 23 patients.
Number operated: 23 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Not reported.
Type: -
Duration: -
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk

Appendices
178
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Not reported.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: " To assess the prevalence of hypercalcitoninemia and MTC in NTD
patients, to compare the ability of CT measurement and fine needle aspiartion cytology (FNAC)
to predict MTC, to identify age groups of NTD patients who should be better candidates than
others to undergo routine measurement of CT."
Abbreviations CT: calcitonin, FNAC: fine needle aspiration cytology.
Notes

Appendices
179
Schuetz 2006
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study
Inclusion criteria: Patients with Hashimoto's thyroiditis with documented positivity for TPOAb,
Negativity for anti-TSH receptor antibodies and thyroid ultrasound imaging suggestive of a
chronic thyroiditis.
Exclusion criteria: Not reported.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 568 patients.
Number with NTD: 105 patients.
Number with NTD and calcitonin testing: 105 patients.
Sex (female%)(n): 88.0% (500) NB only reported for whole study population.
Age (mean/SD): 55 + Not reported range: 18 - 88 years, NB only reported for whole study
population.
MTC: 0 patients. (1 MTC patient in non-nodular study population)
Type of thyroid nodules: Not reported.
Thyroid nodules detected by palpation or US: US.
Nodule size: Only reported for patients with elevated calcitonin (13 + 5 mm; range 4.5-17 mm).
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Only reported for patients with elevated
calcitonin; all nodules were hypoechic/circumscribable.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Out-patient department.
Country: Austria.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Calcitonin as a triage or add-on test: Not reported.
Index test: Basal and stimulated calcitonin.
Used calcitonin assay: Commercial assay by a Nichols Advantage Chemiluminescence System
(Nichols Institute Diagnostics, San Juan Capistrano, Ca, USA)
Sensitivity: 1 pg/ml.
Stimulated calcitonin: Yes.
Indication: Basal serum CT equal to/or exceeded 10 pg/ml.
Stimulative: Pengagastrin Injection BP, Cambridge Laboratories, Tyne & Wear, UK
Dose: 0.5 ug/kg
Time: Before, 2,3 and 5 min after injection.
Reported and extracted cut-off values
Basal: reported: 10 pg/ml; extracted: 10 pg/ml.
Stimulated: reported: 100 pg/ml; extracted 100 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability

Appendices
180
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: In selected patients histological examination after total thyroidectomy,
follow-up.
Indication surgical treatment: Patients with abnormal and pathological PG tests.
Type of surgical treatment: Total thyroidectomy and lymph node dissection along both
recurrent nerves in patients with a abnormal PG tests and an additional lateral lymph node
dissection in patients with a pathological PG test or intraoperatively verified MTC.
Calcitonin negative (n = 100)
Number FNAC: -
Number operated: Not reported.
Calcitonin positive (n = 5)
Number FNAC: Not reported.
Number operated: 0 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Not reported.
Type: -
Number with follow-up: -
Duration: -
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Not reported.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: " To evaluate the relevance of routine CT measurements for
detection of MTC or its premalignant associated conditions (micro MTC and neoplastic C cell
hyperplasia) in HT patients."
Abbreviations CT: calcitonin.
Notes

Appendices
181
Costante 2007
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study.
Inclusion criteria: Patients diagnosed with thyroid nodules.
Exclusion criteria: Renal failure, persistent or recurrent MTC, or a family history of MTC.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 5817 patients.
Number with NTD: 5817 patients.
Number with NTD and calcitonin testing: 5817 patients.
Sex (female%)(n): 80.9% (4706).
Age (mean/SD): 49.7 + 16.6 yr range: 11 - 72 yr.
MTC: 15 patients.
Type of thyroid nodules: Euthryoid nodular/multinodular goiter (n = 4894), hashimoto's
thyroiditis with nodules (n = 436), autonomously functioning thyroid nodules (n = 276), toxic
nodular goiter ( n = 211).
Thyroid nodules detected by palpation or US: Not reported.
Nodule size: Not reported.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: A national healthcare system hospital (outpatient and inpatient) sectors.
Country: Italy.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal and stimulated calcitonin.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay: Chemiluminesence assay (Nichols advantage Calcitonin
Chemiluminesence assay, San Juan Capistrano, CA).
Sensitivity: 1 pg/ml.
Stimulated calcitonin: Yes.
Indication: Basal calcitonin levels > 20 pg/ml and < 100 pg/ml.
Stimulative: Pentagastrin.
Dose: 0.5 ug/kg.
Time: 2 and 5 min after iv injection.
Reported and extracted cut-off values
Basal: 10 pg/ml, 20 pg/ml, 50 pg/ml and 100 pg/ml; extracted 10, 20, 50 and 100 pg/ml
Stimulated: 100 pg/ml; extracted: 100 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern

Appendices
182
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNAB in patients with nonautonomous nodules exceeding 10 mm in
diameter; in selected patients histological examination after surgery, follow-up.
Indication surgical treatment: 1) FNAB indicative or suggestive of thyroid malignancy, 2)
multinodular autonomous or toxic goiters, 3) large euthyroid goiters causing compression, 4)
serum CT levels (basal or PG stimulated) more than 100 pg/ml.
Type: Not reported.
Calcitonin negative (n = 5535)
Number FNAB: Not reported.
Number operated: 723 patients.
Calcitonin positive (n = 216)
Number FNAB: Not reported.
Number operated: 24 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference
standard does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: In patients with basal CT between 10-100 pg/ml and negative
Pg testing.
Type: Basal CT in patients with basal CT between 10-20 pg/ml; yearly stimulated CT in
patients with basal CT between 20-100 pg /ml.
Number with follow-up: 212 patients.
Duration: 2-4 yr.
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Non-commercial.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: " To evaluate the diagnostic accuracy of systematic CT
measurement in non-multiple endocrine neoplasia type 2 patients with nodular thyroid
disease."
Abbreviations CT: calcitonin, FNAB: fine needle aspiration biopsy, PG: pentagastrin.
Notes

Appendices
183
Rink 2009
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study.
Inclusion criteria: Nodular thyroid disease diagnosed by high-resolution US.
Exclusion criteria: Not reported.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 21928 patients.
Number with NTD: 21928 patients.
Number with NTD and calcitonin testing: 21928 patients.
Sex (female%)(n): 76.9% (16857).
Age (mean/SD): not reported range: 8 - 97 yrs.
MTC: 28 patients.
Type of thyroid nodules: Not reported.
Thyroid nodules detected by palpation or US: US.
Nodule size: Only reported for MTC patients.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Four sites in central Germany.
Country: Germany.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal and stimulated calcitonin.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay: Radioimmunoassays Calcitonin-IRMA (IBL GmbH, Hamburg, Germany)
and Calcitonin-IRMA magnum (Medipan GmbH, Dahlewith/Berlin, Germany).
Sensitivity: 0.7 ng/l (IBL), 1.5 ng/L (Medipan).
Stimulated calcitonin: Yes.
Indication: If basal CT > 10 ng/l and if renal insufficiency as well as proton pump inhibiotr
medication could be ruled out.
Stimulative: Pentagastrin (Pentagastrin Injection BP, Cambridge Laboratiries Ltd., Tyne &
Wear, England).
Dose: 0.5 ug/kg.
Time: Not reported.
Reported and extracted cut-off values
Basal: reported: 10 ng/l; extracted: 10, 15 ng/l.
Stimulated: reported males: 80 ng/l, females 50 ng/l.; extracted 50, 80 ng/l.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern

Appendices
184
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: In selected patients histopathological examination after thyroid
surgery, follow-up.
Indication surgical treatment: An abnormal PGT, a basal CT exceeding 30 ng/l, increasing
basal or progressive morphologic alterations during follow-up.
Type: Not reported.
Calcitonin negative (n = 21073)
Number FNA: -
Number operated: Not reported.
Calcitonin positive (n = 855)
Number FNA: -
Number operated: 157 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: In patients not having surgery and without renal insufficiency.
Type: Ultrasound and determination of basal CT.
Number with follow-up: 214 patients.
Duration: mean observation 21 months, median 17 months, range 3-87 months.
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? No
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Non-commercial.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: " the calculation and validation of upper limits for basal and
stimulated pCT-Cs in a large patient population with nodular thyroid disease, to distinguish
bewteen the subgroups with and without MTC."
Abbreviations pCT-C: plasma calcitonin concentration, PGT: pentagastrin test.
Notes

Appendices
185
Hasselgren 2010
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Retrospective study.
Inclusion criteria: Patients with non-toxic nodular goiter.
Exclusion criteria: Patients with missing data or with wrongly registered diagnosis.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 959 patients.
Number with NTD: 959 patients.
Number with NTD and calcitonin testing: 702 patients.
Sex (female%)(n): 84.6% (811) NB of whole study population (n=959).
Age (mean/SD): mean not reported; median 49 yrs range: 13-93 yrs NB of whole study
population (n=959).
MTC: 6 patients.
Type of thyroid nodules: Non toxic nodular goiter.
Thyroid nodules detected by palpation or US: Not reported.
Nodule size: Only reported of MTC patients.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Ultrasound.
Setting: Secondary/tertiarry referral centre.
Country: Denmark.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: Basal calcitonin
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay: (1) double-antibody radioimmunoassay technique (MediLab A/S,
Copenhagen, Denmark) (n =668) (2) solid-phase, enzyme-labelded, 2-site chemiluminescent
immunometric principle (Immulite 2000, Calcitonin, Siemens Medical Solutions Diagnostics,
Erlangen, Germany) (n=14).
Sensitivity: Not reported (1 and 2).
Stimulated calcitonin: No.
Indication: -
Stimulative: -
Dose: -
Time: -
Reported and extracted cut-off values
Basal: reported 0.10 ug/l, 0.20 ug/l, 0.50 ug/l (= 100 ng/l(pg/ml)).
Stimulated: -
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from Low concern

Appendices
186
the review question?
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNAB, in selected patients histopathological examination after surgery,
cross-linkage with the Danish Thyroid Cancer Database.
Indication surgical treatment: Based on the composition of the following variables: (1) clincal
evaluation including age, comorbidity, thyroid size, suspicion of malignancy; (2) sonographic
appearance; (3) result of FNAB; (4) result of serum calcitonin measurement; (5) patient
preference.
Type: Not reported.
Calcitonin negative: (n = 663)
Number FNAB: Not reported.
Number operated: 223 patients.
Calcitonin positive (n = 39)
Number FNAB: Not reported.
Number operated: 23 patients.
Is the reference standards likely to correctly classify the target condition? Yes
Were the reference standard results interpreted without knowledge of the results of
the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced bias? Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: All patients.
Type: Cross linkage with Danish Thyroid Cancer Database.
Number with follow-up: 663 patients
Duration: Median follow-up 7 years (range 3-10 years) (whole study population).
Follow-up calcitonin positive: All patients.
Type: Cross linkage with Danish Thyroid Cancer Database.
Number with follow-up: 39 patients.
Duration: Median follow-up 7 years (range 3-10 years) (whole study population).
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? Yes
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? Yes
Could the patient flow have introduced bias? Unclear risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Not reported.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: "To estimate the validity of serum calcitoin for detection of MTC in a
consecutive population of patients with nontoxic nodular goiter, living in a mild to moderate
iodine-deficient area."
Abbreviations
Notes

Appendices
187
Herrmann 2010
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Retrospective cohort study.
Inclusion criteria: Patients with nodular thyroid disease found by sonography, living in central
Germany (an area with endemic goitre due to previous iodine deficiency).
Exclusion criteria: Known elevation of hCt, Graves' Disease, autoimmune thyroid disease.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 1007 patients.
Number with NTD: 1007 patients.
Number with NTD and calcitonin testing: 1007 patients.
Sex (female%)(n): 56.3% (567)
Age (mean/SD): 55 + 14, range: not reported.
MTC: 2 patients.
Type of thyroid nodules: Not reported.
Thyroid nodules detected by palpation or US: US.
Nodule size: Only reported for patients with elevated bCT.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Division of Endocrinology, Technology Center Bochum, Germany.
Country: Germany.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Index test: basal and stimulated hCT.
Calcitonin as a triage or add-on test: Not reported.
Used calcitonin assay: Solid-phase, enzyme labeled, two site chemiluminescent assay, with
the Immulite 2000, (Siemens Immulite 2000, Munich, Germany).
Sensitivity: Not reported.
Stimulated calcitonin: Yes.
Indication: Basal CT > 10 and < 100 pg/ml.
Stimulative: Pentagastrin (Peptavlon; Laboratoires SERB, Paris, France).
Dose: 0.5 ug/kg bodyweight.
Time: 2 and 5 min after injection.
Reported and extracted cut-off values
Basal: 10 pg/ml; extracted: 10, 15, 20, 30, 50 and 100 pg/ml.
Stimulated: 100 pg/ml; extracted:100 and 200 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern

Appendices
188
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC
Reference standards: FNAB, in selected patients histolopathological examination after
surgery, follow-up.
Indication surgical treatment: Elevated stimulated hCT > 100 pg/ml.
Type: Total thyroidectomy, with careful dissection of both recurrent nerves and a systematic
microdissection of the central lymph node compartments along both nerves from the upper
thoracic outlet up to the larynx.
Calcitonin negative (n = 990)
Number FNAC: Not reported.
Number operated: Not reported.
Calcitonin positive: (n = 17)
Number FNAB: 2 patients.
Number operated: 5 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Calcitonin negative: Not reported.
Type: -
Duration: -
Calcitonin positive: Patients with stimulated hCT < 100 pg/ml.
Type: Re-testing.
Number with follow-up: 12 patients.
Duration: Not reported.
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Other funding.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: "Shedding further light on the hCT measurement and its testing
after pentagastrin stimulation in patients with thyroid nodule disease."
Abbreviations hCT: serum calcitonin.
Notes

Appendices
189
Schneider 2012
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Cohort study.
Inclusion criteria: Patients diagnosed with thyroid nodules > 2 mm based on the spatial
resolution of ultrasound equipment.
Exclusion criteria: Patients referred with elevated or previously determined CT values, MTC
or a family history of MTC, renal insufficiency, bacterial infection, alcohol abuse, proton-
pump inhibitor therapy, Graves'disease or autoimmune thyroid disease.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 11270 patients.
Number with NTD: 11270 patients.
Number with NTD and calcitonin testing: 11270 patients.
Sex (female%)(n): Not reported.
Age (mean/SD): Not reported range: Not reported.
MTC: 12 patients.
Type of thyroid nodules: Not reported.
Thyroid nodules detected by palpation or US: Ultrasound.
Nodule size: Only reported of MTC and PTC patients.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Only reported of patients with elevated basal
CT levels.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Not reported.
Country: Germany
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Calcitonin as a triage or add-on test: Not reported.
Index test: Basal and stimulated calcitonin.
Used calcitonin assay: Solid-phase, enzyme labeld, two-site chemiluminescent assay with
Immulite 2000 (Siemens Immulite 2000, Munich, Germany).
Sensitivity: Not reported.
Stimulated calcitonin: Yes.
Indication: bCT > 13 and < 100 pg/ml (if PG was available and the patients physical condition
allowed testing).
Stimulative: Pentagastrin (Pentagastrin injection BP, Ireland, UK)
Dose: 0.5 ug/kg bodyweight.
Time: 2 and 5 min after injection.
Reported and extracted cut-off values
Basal: Reported 13 pg/ml; extracted: 13, 15, 20, 30, 50, 100 pg/ml.
Stimulated: Reported 100 pg/ml; extracted: 100, 200 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk

Appendices
190
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from the
review question?
Low concern
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC
Reference standards: Histopathological examination after thyroid surgery, follow-up.
Indication surgical treatment: 1) basal CT > 100 pg/ml, PG-stimulated CT > 100 p/ml, 3)
suspicious thyroid nodules based on the patients history, sonography (hypoechogencity,
irregular margins, microcalcifications) or scintigraphy (cold nodules have been consistently
associated with malignancy).
Type: Not reported.
Calcitonin negative (n = 11238)
Number FNAC: -
Number operated: Not reported.
Calcitonin positive (n = 32)
Number FNAC: -
Number operated: 18 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results of
the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced bias? Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Patients with no SCT > 100 pg/ml, patients with no SCT
performed.
Type: Repeated bCT testing.
Number with follow-up: 10 patients.
Duration: Mean 7 months.
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Not reported (no conflicts of interest).
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: "The positive predictive value (PPV) of a slightly elevated basal
calcitonin for the diagnosis of medullary thyroid cancer is still under debate."
Abbreviations
Notes

Appendices
191
Giovanella 2012
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Prospective cohort study.
Inclusion criteria: Patients with nodular thyroid disease.
Exclusion criteria: Pulmonary or pancreatic tumors, kidney failure, Graves' disease,
autonomously functioning thyroid nodules, autoimmune thyroid diseases, sepsis, alcohol
abuse, smoking or the use of proton-pump inhibitor therapy in the last month.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Yes
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 1236 patients.
Number with NTD: 1236 patients.
Number with NTD and calcitonin testing: 1236 patients.
Sex (female%)(n): 54.5% (674).
Age (mean/SD): 53 + 17 yrs range: Not reported.
MTC: 2 patients.
Type of thyroid nodules: Not reported.
Thyroid nodules detected by palpation or US: Not reported.
Nodule size: Not reported.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Not reported.
FNA procedures performed through ultrasound guidance or palpation: Not reported.
Setting: Not reported.
Country: Switzerland
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Calcitonin as a triage or add-on test: Not reported.
Index test: Basal and stimulated calcitonin.
Used calcitonin assay: Immulite 2000XPi platform (Siemens Healthcare Diagnostics, Erlangen,
Germany).
Sensitivity: 2 pg/ml.
Stimulated calcitonin: Yes.
Indication: Patients with true high CT value.
Stimulative: Pentagastrin (Pengagastrin Injection BP, Cambridge Laboratories, Wallsend, UK)
Dose: 0.5 ug/kg.
Time: 2 and 5 min after injection.
Reported and extracted cut-off values
Basal: reported: 10 pg/ml; extracted: 10, 15, 20, 30, 50, 100 pg/ml.
Stimulated: reported 100 pg/ml; extracted: 100, 200 pg/ml.
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern

Appendices
192
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNAC, in selected patients histopathological examination after surgery,
follow-up.
Indication surgical treatment: Basal and/or stimulated CT levels > 100 pg/ml, patients with
indeterminate, suspicious or malignant cytological outcome.
Typeof surgical treatment: Thyroidectomy with bilateral dissection of the central
compartment (in patients with basal and/or stimulated CT levels > 100 pg/m)l.
Calcitonin negative (n = 1222)
Number FNAC: Not reported.
Number operated: Not reported.
Calcitonin positive (n =14)
Number FNAC: 14 patients.
Number operated: 7 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
Unclear
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Patients with benign cytology.
Type: US, basal CT and PCT.
Number with follow-up: 7 patients.
Duration: 24-35 months.
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? No
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English
FUNDING: Other funding
PUBLICATION STATUS: Full article
Stated aim of
study
Quote from publication: " To prospectivevly evaluate the role of routine PCT measuremnet in
detecting MTC among patients with thyroid nodules, and to assess the potential
improvement provided by adding PCT to increased basal CT."
Abbreviations PCT: procalcitonin, CT: calcitonin.
Notes

Appendices
193
Grani 2012
Patient Selection
A. Risk of Bias
Patient
Sampling
Design: Not reported
Inclusion criteria: At least one one discrete nodular lesion of the thyroid or a multinodular
goitre and were referred to our institution to undergo FNAC because of clinical or
ultrasonographic suspicion (irregular margins, micro calcifications, and chaotic pattern
vascularization).
Exclusion criteria: Not reported.
Was a consecutive or random sample of patients enrolled? Yes
Was a case-control design avoided? Yes
Did the study avoid inappropriate exclusions? Unclear
Could the selection of patients have introduced bias? Low risk
B. Concerns regarding applicability
Patient
characteristics
and setting
Number of participants: 1073 patients.
Number with NTD: 1073 patients.
Number with NTD and calcitonin testing: 1073 patients.
Sex (female%)(n): 83.2% (893)
Age (mean/SD): 55.7 + 13.4 yrs range: Not reported.
MTC: 2 patients.
Type of thyroid nodules: One discrete nodular lesion of the thyroid or a multinodular goitre
with clinical or ultrasonographic suspicion (irregular margins, microcalcifications, and chaotic
pattern vascularization).
Thyroid nodules detected by palpation or US: Both.
Nodule size: Not reported.
Number of nodules: Not reported.
Sonographic morphology of thyroid nodules: Irregular margins, microcalcifications, and
chaotic pattern vascularization.
FNA procedures performed through ultrasound guidance or palpation: Ultrasonography.
Setting: The Thyroid Center of Sapienza University of Rome.
Country: Italy.
Are there concerns that the included patients and setting do not match the
review question?
Low concern
Index Test
Index tests Calcitonin as a triage or add-on test: Not reported.
Index test: Basal calcitonin.
Used calcitonin assay: Automated two-site immunochemiluminometric assay.
Sensitivity: 2 pg/ml.
Stimulated calcitonin: No.
Indication: -
Stimulative: -
Dose: -
Time: -
Reported and extracted cut-off values
Basal: reported: 10 pg/ml; extracted: 10 pg/ml.
Stimulated: -
A. Risk of Bias
If a threshold was used, was it pre-specified? Yes
Could the conduct or interpretation of the index test have introduced bias? Low risk

Appendices
194
B. Concerns regarding applicability
Are there concerns that the index test, its conduct, or interpretation differ from
the review question?
Low concern
Reference Standard
A. Risk of Bias
Target condition
and reference
standard(s)
Target condition: MTC.
Reference standards: FNAC, in selected patients histological examination after total
thyroidectomy, follow-up.
Indication surgical treatment: Not reported.
Type of surgical treatment: Total thyroidectomy.
Calcitonin negative (n = 1032)
Number FNAC: 1032 patients.
Number operated: Not reported.
Calcitonin positive (n = 41)
Number FNAC: 41 patients.
Number operated: 3 patients.
Is the reference standards likely to correctly classify the target condition? Unclear
Were the reference standard results interpreted without knowledge of the results
of the index tests?
No
Could the reference standard, its conduct, or its interpretation have introduced
bias?
Unclear risk
B. Concerns regarding applicability
Are there concerns that the target condition as defined by the reference standard
does not match the question?
Low concern
Flow and Timing
A. Risk of Bias
Flow and timing Follow-up calcitonin negative: Not reported.
Type: -
Duration: -
Follow-up calcitonin positive: Patients with unexplained hypercalcitonemia.
Type: basal CT.
Number with follow-up: 34 patients.
Duration: 12-36 months.
Was there an appropriate interval between index test and reference standard? Unclear
Did all patients receive the same reference standard? No
Were all patients included in the analysis? Yes
Did all patients receive the reference standard? Yes
Could the patient flow have introduced bias? High risk
User defined characteristics
Publication
details
LANGUAGE OF PUBLICATION: English.
FUNDING: Other funding.
PUBLICATION STATUS: Full article.
Stated aim of
study
Quote from publication: " To evaluate the basal CT values in patients with and without
thyroid autoimmunity".
Abbreviations CT: calcitonin.
Notes

Appendices
195
Appendix 5
Table Characteristics of excluded studies
Study Reason for exclusion
Lepage 1992 Only abstract available (meeting abstract).
Pacini 1994 (Partially) same study population as Elisei 2004.
Henry 1995 Article in French, (partially) same study population as Henry 1996.
Henry 1996 Article in French, (partially) same study population as Nicolli 1997, Iacobone 2001,
Mirallie 2004.
Shong 1996 Article in Korean.
Vierhapper 1997 (Partially) same study population as Vierhapper 2005.
Niccoli 1997 Evaluation of preoperative calcitonin determination (not part of this review).
Kaserer 1998 Included patients with thyroid disease; number of patients with nodular thyroid
disease not specified. (Partially) same study population as Vierhapper 2005.
Mariss 2001 Only abstract available (meeting abstract).
Mariss 2001 (2) Only abstract available (meeting abstract).
López-Guzmán 2002 Article in Spanish.
Iacobone 2002 Included patients with thyroid disease; number of patients with nodular thyroid
disease not specified.
Mirallie 2004 Included patients with thyroid disease; number of patients with nodular thyroid
disease not specified.
Gibelin 2005 Evaluation of preoperative calcitonin determination (not part of this review).
Papi 2010 Calcitonin testing in isthmic thyroid nodules.
Chambon 2011 Evaluation of preoperative calcitonin determination (not part of this review).
Lipp 2011 Only abstract available (meeting abstract).
Zaplatnikov 2012 Only meeting abstract available
Marui 2012 Only meeting abstract available

Appendices
196
Appendix 6
Differences between protocol and review
No separate meta-analyses for calcitonin testing as a triage or as an add-on test was
performed because all included studies were considered as performing calcitonin testing
as a triage test.
No email requests to contact persons of included studies were send
No studies written in non-English language were included.













![Thyroid carcinoma final [part 2]](https://img.pdfslide.net/doc/110x75/58f9ac081a28ab0f5b8b4659/thyroid-carcinoma-final-part-2.jpg)