Embed Size (px)
Citation preview

Simulation-based education: How could simulation be used for technical skills development in the future Mersin Űniversitesi, Faculty of Medicine MESEKOK
October 27, 2015
Deborah Rooney PhD
MEDICAL SCHOOL UNIVERSITY OF MICHIGAN
Copyright 2015. All Rights Reserved.
Disclosures and conflicts of interest
• None

My Background

My Background
My Background
• Medical education since 1991
• Nine years in surgical education
• PhD in Educational Psychology
• Director of Education and Research, Clinical Simulation Center, University of Michigan (UMCSC)
UM Clinical Simulation Center (UMCSC)
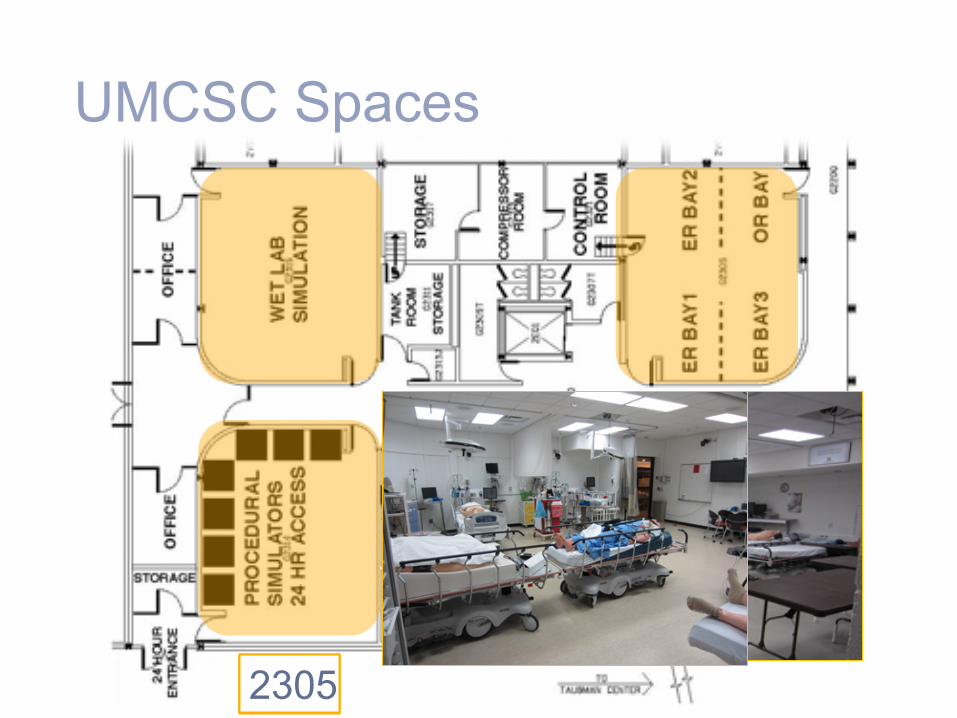
2315 2314 2305
UMCSC Spaces
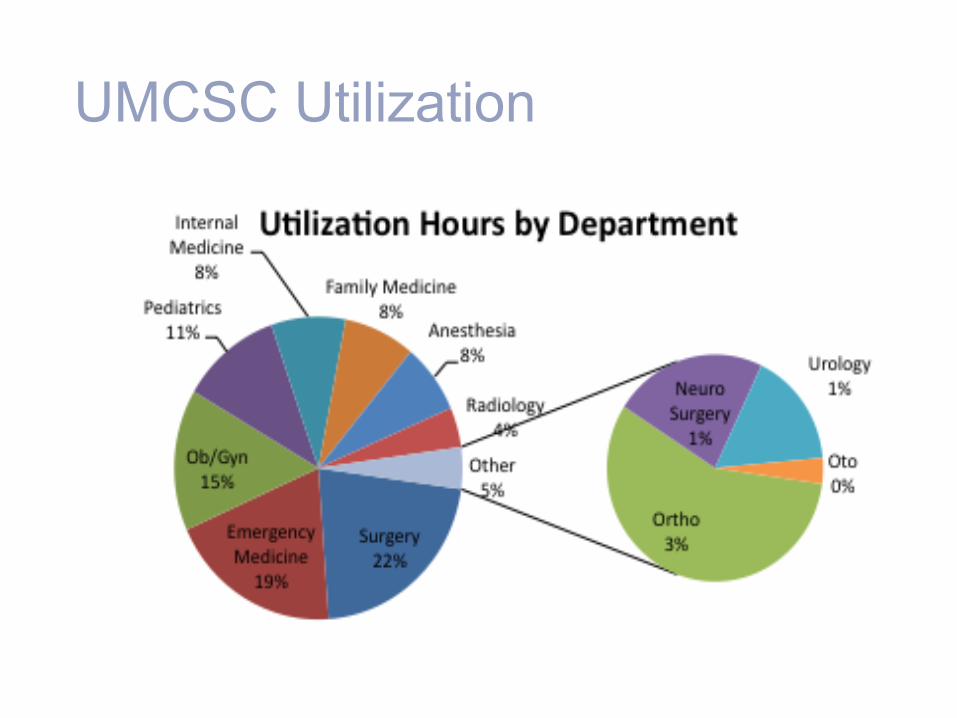
UMCSC Utilization
Today’s talk: Simulation-based education
• Brief history of developments that impacted simulation
• Current applications of simulation-based training for technical skills
• Projected trends in simulation-based training
Simulation-based education is not new
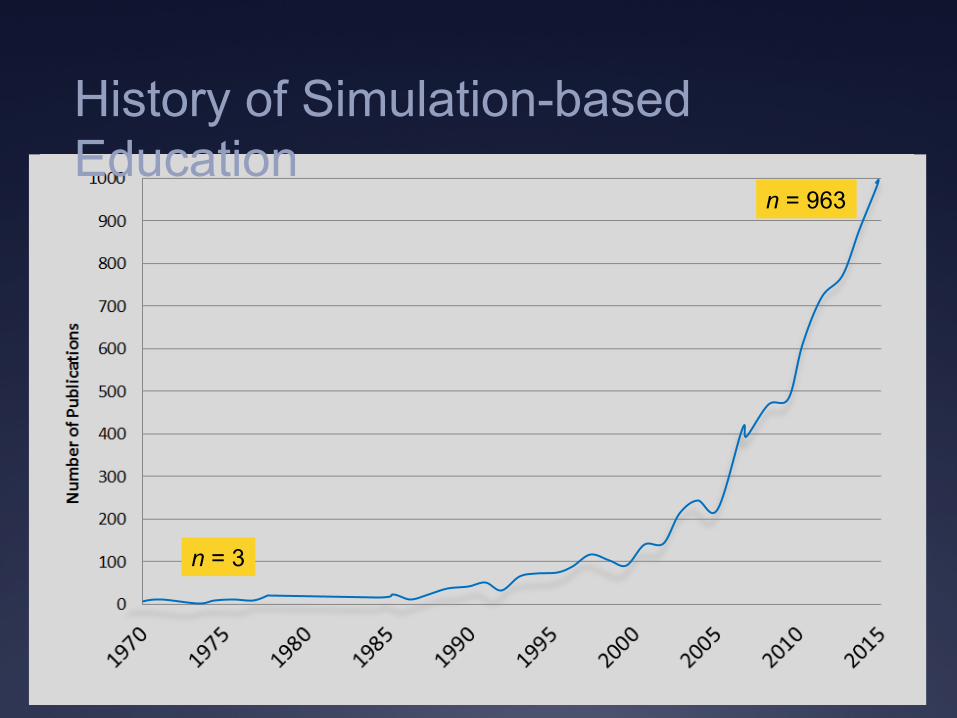
n = 3
n = 963
History of Simulation-based Education
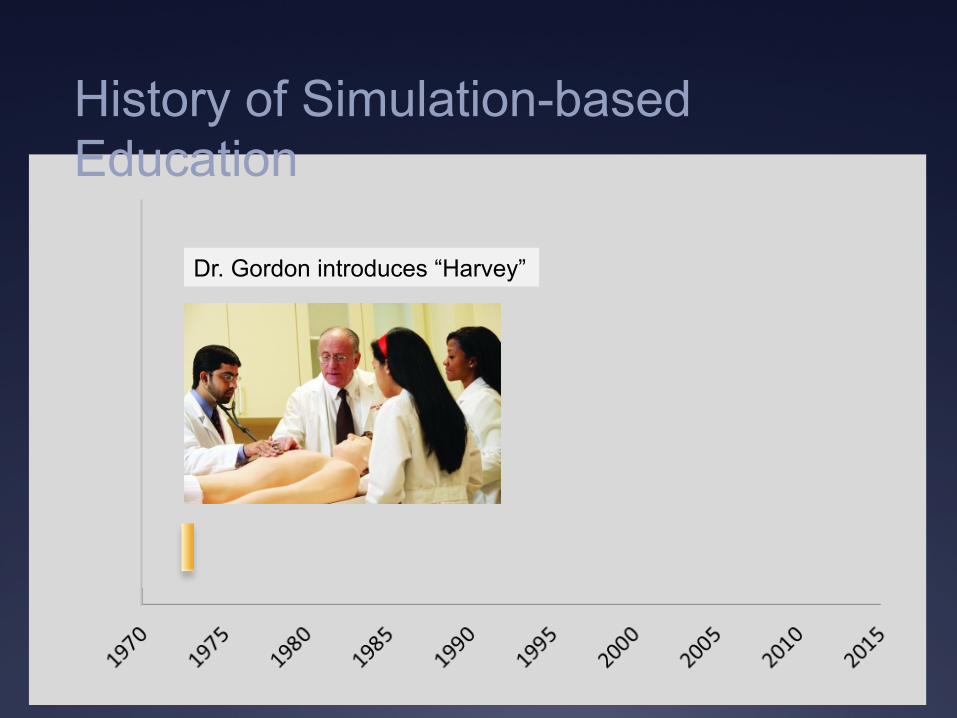
Dr. Gordon introduces “Harvey”
History of Simulation-based Education
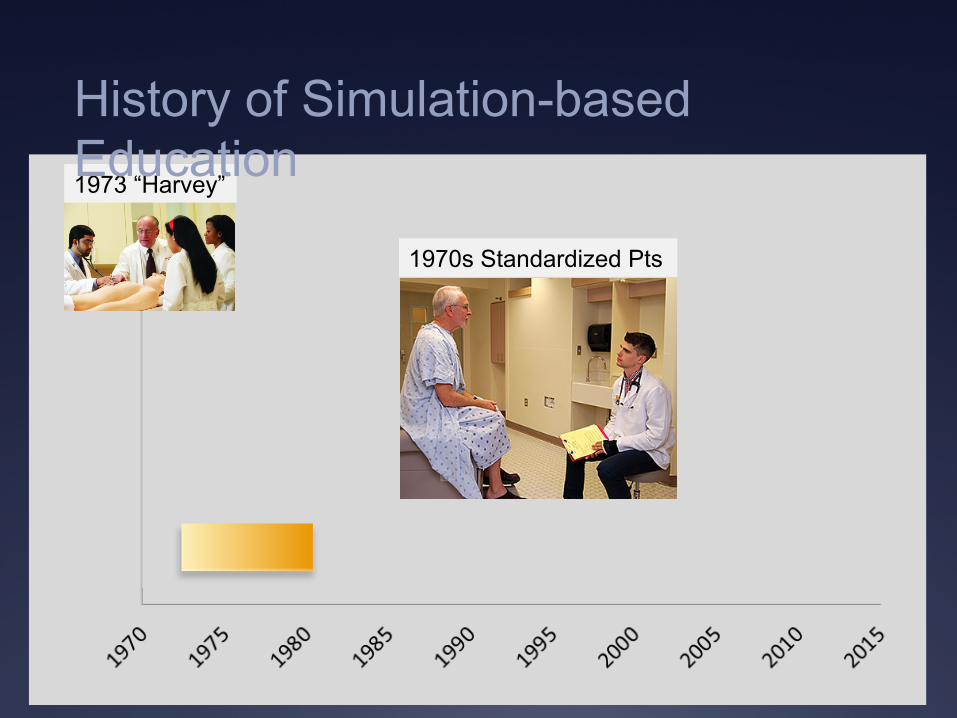
1973 “Harvey”
1970s Standardized Pts
History of Simulation-based Education
1980-90s MIS training 1973 “Harvey”
1970s Std Pts
History of Simulation-based Education
1980-90s Computers
1973 “Harvey”
1970s Std Pts
1980-90s MIS
History of Simulation-based Education
1998 Standards 1973 “Harvey”
1970s Std Pts
1980-90s MIS
Computers
History of Simulation-based Education
2000 Error
1973 “Harvey”
1970s Std Pts
1980-90s MIS
Computers
1998 Standards
History of Simulation-based Education
Development & refinement of best practices • Invention and proof of concept of specific
simulators, skills curricula
• Development of practical tools to support learning and assessment in complex settings
• Application of educational theories
History of SBE* for technical skills: 2000 to present
*SBE= Simulation-based Education
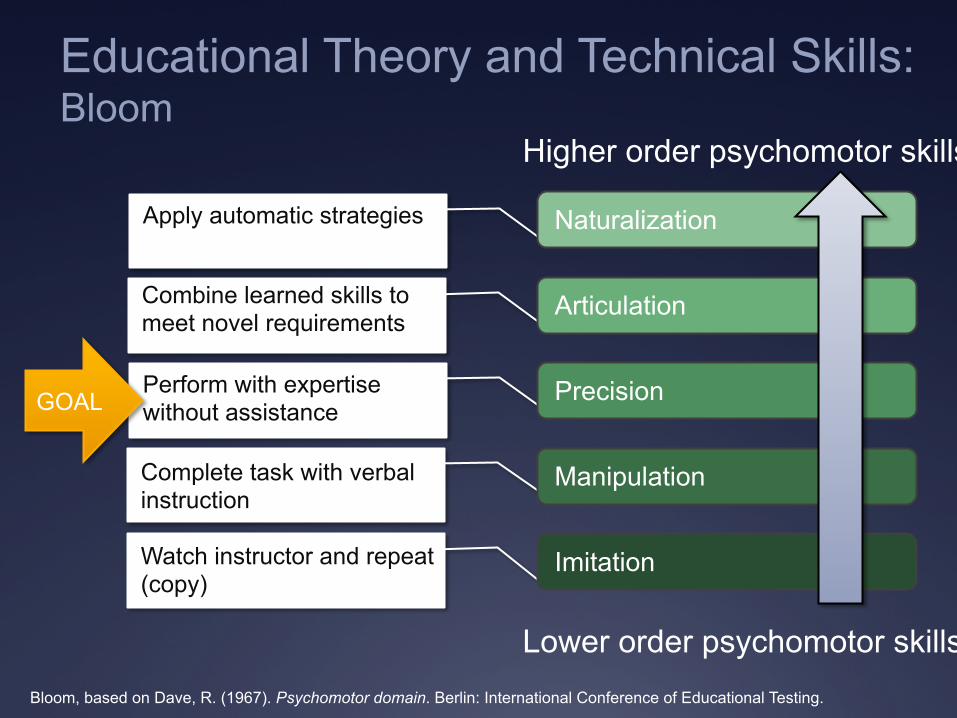
Educational Theory and Technical Skills: Bloom
Bloom, based on Dave, R. (1967). Psychomotor domain. Berlin: International Conference of Educational Testing.
Higher order psychomotor skills
Lower order psychomotor skills
Watch instructor and repeat (copy)
Complete task with verbal instruction
Combine learned skills to meet novel requirements
Apply automatic strategies
Perform with expertise without assistance
Naturalization
Articulation
Precision
Manipulation
Imitation
GOAL
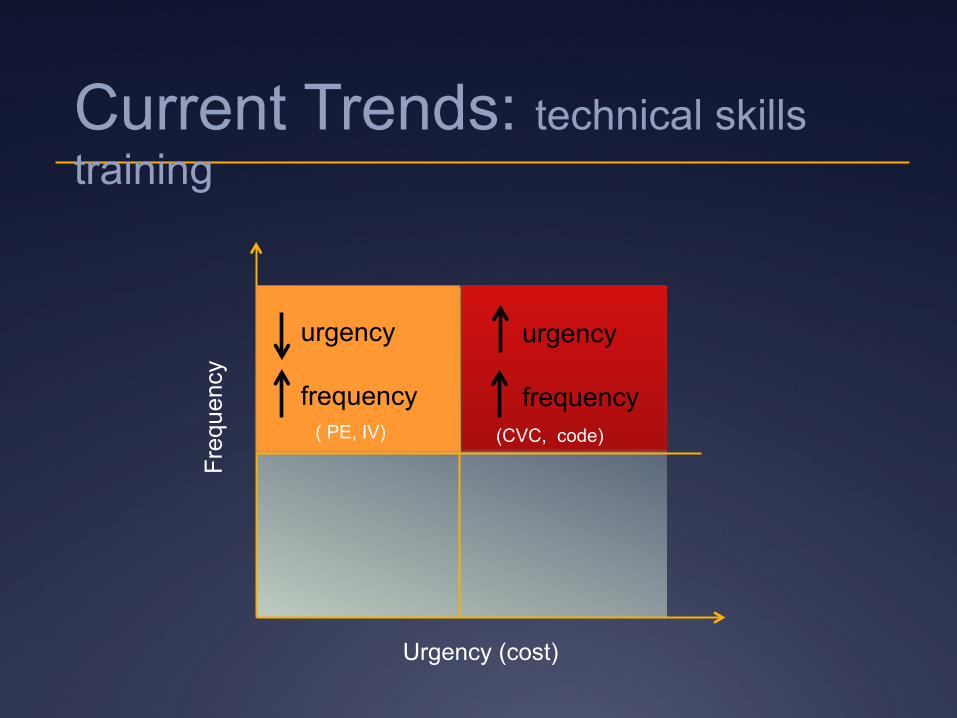
Freq
uenc
y
Urgency (cost)
urgency frequency
urgency frequency
(CVC, code) ( PE, IV)
Current Trends: technical skills training
Address Gap
Impact Pt Care
Value ?
Current Trends: technical skills training
Benefits of SBE for technical skills training
Addresses the gap (improving KSA*) • Lumbar puncture (LP) skills in the Neonatal Intensive Care Unit
(Shafer et al, 2013)
Improves patient outcomes • Central venous catheter placement skills in the Medical Intensive
Care Unit (Barsuk et al, 2009)
Decreases hospital costs
• Central line placement skills in the Medical Intensive Care Unit (Cohen et al, 2010)
*KSA= knowledge, skills, attitude
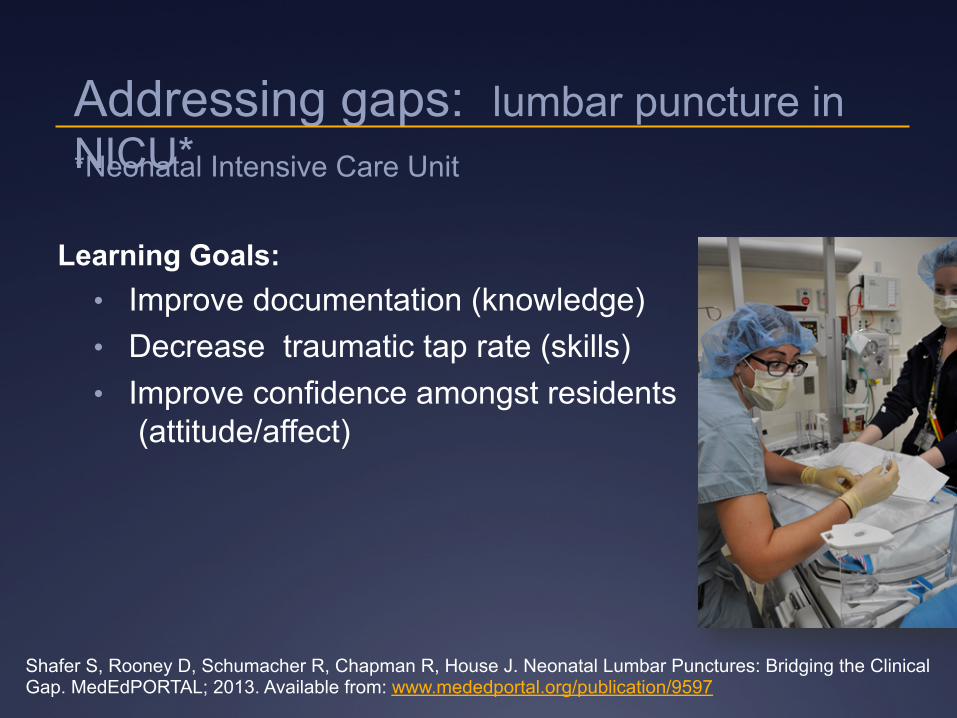
Learning Goals: • Improve documentation (knowledge) • Decrease traumatic tap rate (skills) • Improve confidence amongst residents
(attitude/affect)
Shafer S, Rooney D, Schumacher R, Chapman R, House J. Neonatal Lumbar Punctures: Bridging the Clinical Gap. MedEdPORTAL; 2013. Available from: www.mededportal.org/publication/9597
Addressing gaps: lumbar puncture in NICU* *Neonatal Intensive Care Unit
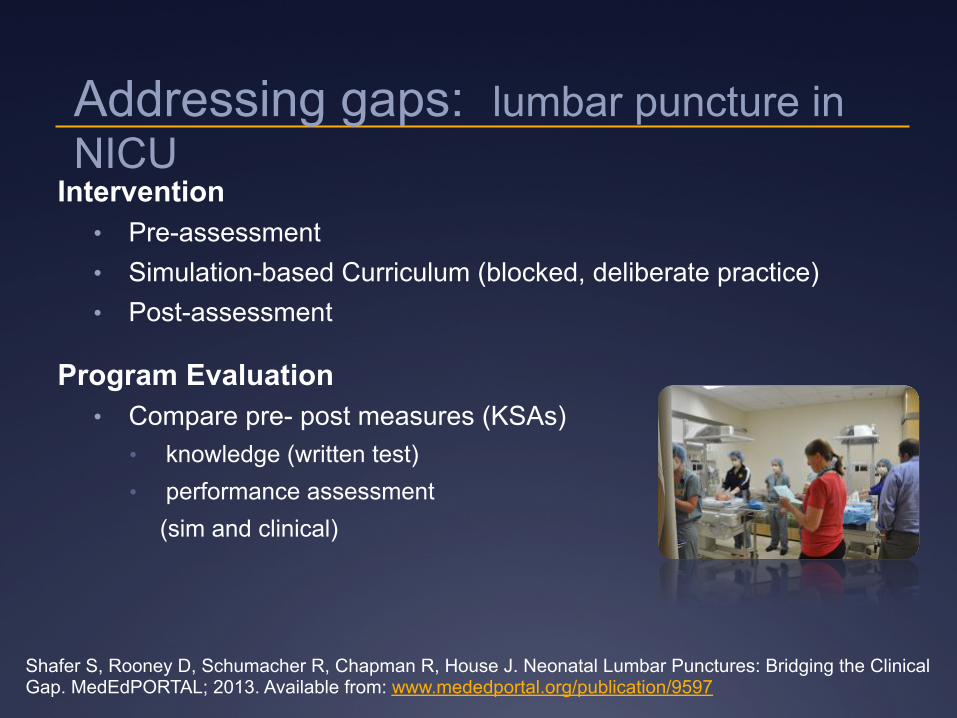
Intervention • Pre-assessment • Simulation-based Curriculum (blocked, deliberate practice) • Post-assessment
Program Evaluation • Compare pre- post measures (KSAs)
• knowledge (written test) • performance assessment
(sim and clinical)
Shafer S, Rooney D, Schumacher R, Chapman R, House J. Neonatal Lumbar Punctures: Bridging the Clinical Gap. MedEdPORTAL; 2013. Available from: www.mededportal.org/publication/9597
Addressing gaps: lumbar puncture in NICU
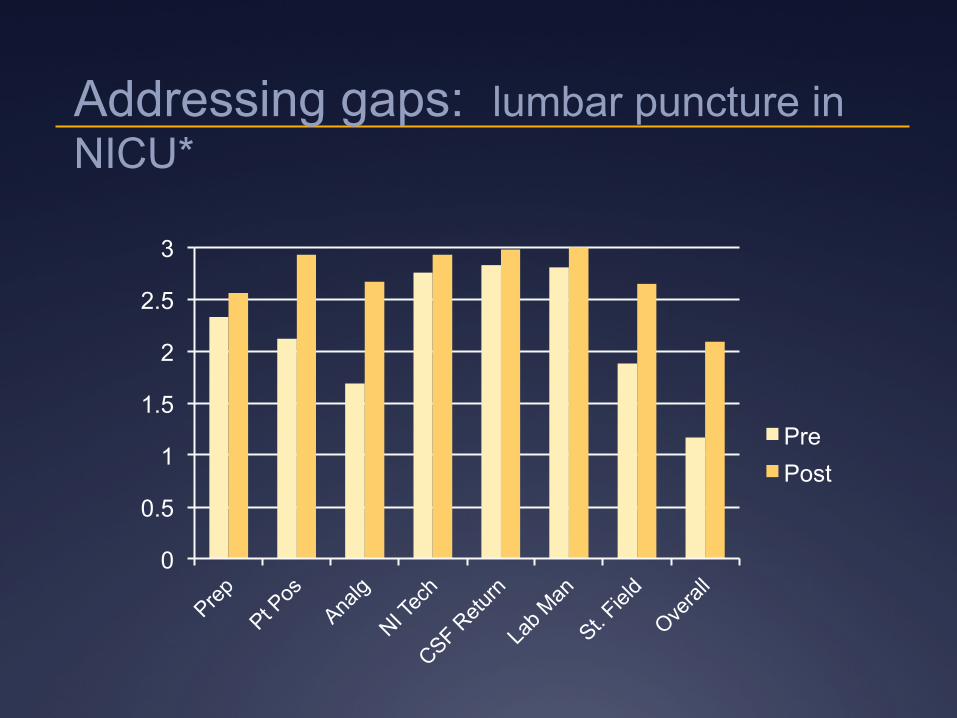
0
0.5
1
1.5
2
2.5
3
Pre Post
Addressing gaps: lumbar puncture in NICU*

What about impact to patient care?
Improves patient outcomes: Central Venous Catheter (CVC) placement in MICU
Sim-based, mastery training central line placement skills in Medical ICU (MICU);
• Presentation with contra/indications for CVC • Video demonstration of CVC IJ placement • One-on-one instructor & trainee practice with
feedback • Pre-post training assessment
Barsuk JH, McGaghie WC, Cohen ER, O'Leary KJ, Wayne DB. Simulation based mastery learning reduces complications during central venous catheter insertion in a medical intensive care unit. Crit Care Med. 2009 Oct;37(10):2697-701.
CVC placement in Medical Intensive Care Unit (MICU)
Sim-based, mastery training improved clinical measures;
• Fewer needle passes • Fewer arterial punctures • Fewer catheter adjustments
Barsuk JH, McGaghie WC, Cohen ER, O'Leary KJ, Wayne DB. Simulation based mastery learning reduces complications during central venous catheter insertion in a medical intensive care unit. Crit Care Med. 2009 Oct;37(10):2697-701.
Cohen ER, Feinglass J, Barsuk JH, et al. Cost savings from reduced catheter-related bloodstream infection after simulation-based education for residents in a medical intensive care unit. Simul Healthc. 2010 Apr;5(2):98-102.
Follow-up research compared pre-post Catheter-Related Bloodstream Infections (CRBSI) and potential cost-savings for the hospital
-Cohen and colleagues
CVC placement in Medical Intensive Care Unit (MICU)
Cohen ER, Feinglass J, Barsuk JH, et al. Cost savings from reduced catheter-related bloodstream infection after simulation-based education for residents in a medical intensive care unit. Simul Healthc. 2010 Apr;5(2):98-102.
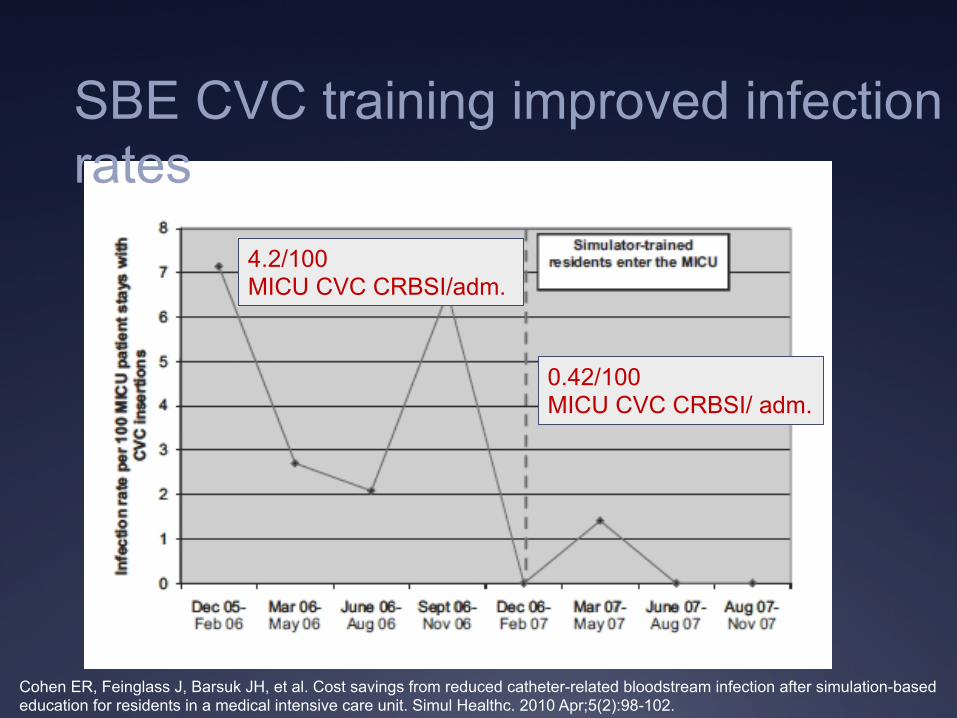
4.2/100 MICU CVC CRBSI/adm.
0.42/100 MICU CVC CRBSI/ adm.
SBE CVC training improved infection rates
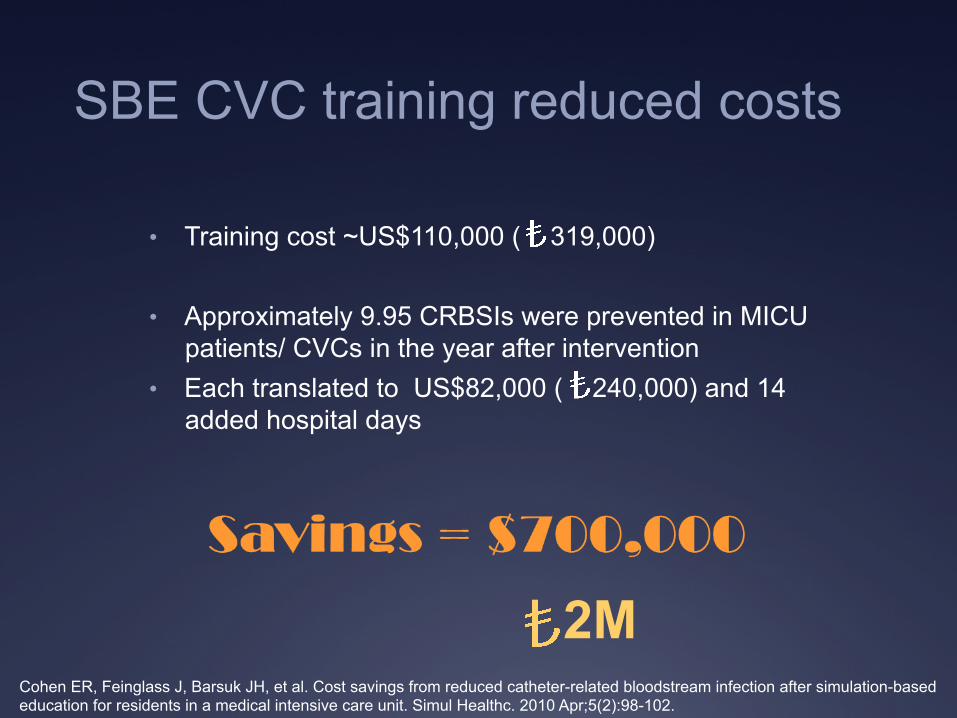
• Training cost ~US$110,000 ( 319,000)
• Approximately 9.95 CRBSIs were prevented in MICU patients/ CVCs in the year after intervention
• Each translated to US$82,000 ( 240,000) and 14 added hospital days
Cohen ER, Feinglass J, Barsuk JH, et al. Cost savings from reduced catheter-related bloodstream infection after simulation-based education for residents in a medical intensive care unit. Simul Healthc. 2010 Apr;5(2):98-102.
2M
SBE CVC training reduced costs

What about the future?
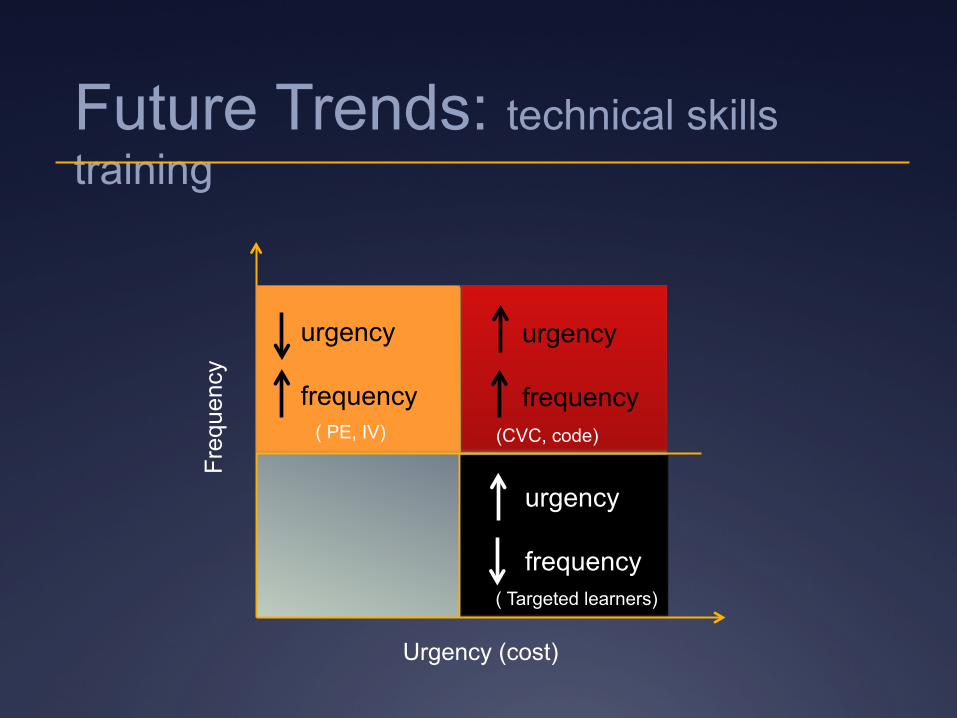
Future Trends: technical skills training
Freq
uenc
y
Urgency (cost)
urgency frequency
urgency frequency
urgency frequency
(CVC, code)
( Targeted learners)
( PE, IV)
Future trends: targeted procedural training
-Tavlasoglu et al (Diyarbakir Military Medical Hospital)
Future trends: targeted procedural training
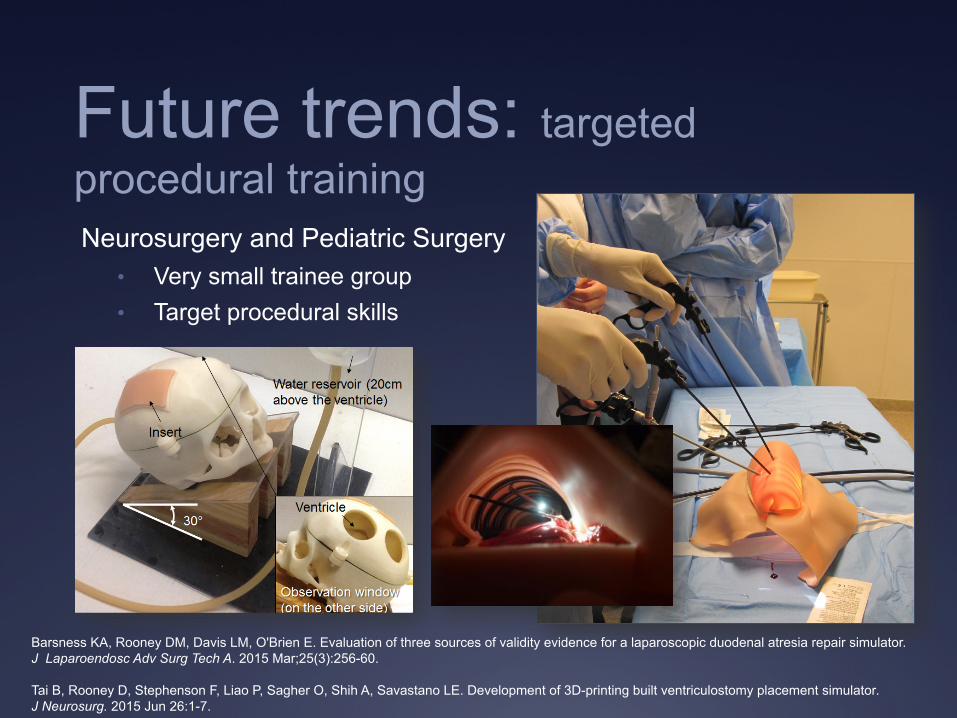
Barsness KA, Rooney DM, Davis LM, O'Brien E. Evaluation of three sources of validity evidence for a laparoscopic duodenal atresia repair simulator. J Laparoendosc Adv Surg Tech A. 2015 Mar;25(3):256-60. Tai B, Rooney D, Stephenson F, Liao P, Sagher O, Shih A, Savastano LE. Development of 3D-printing built ventriculostomy placement simulator. J Neurosurg. 2015 Jun 26:1-7.
Future trends: targeted procedural training Neurosurgery and Pediatric Surgery
• Very small trainee group • Target procedural skills
Challenges associated with SBE
• Cost
• Space
• Expertise
• Time (development and delivery)
• Decrease space requirements
• Decrease faculty time commitment
• Increase learner access
Addressing the challenges: Future training targets technical skills
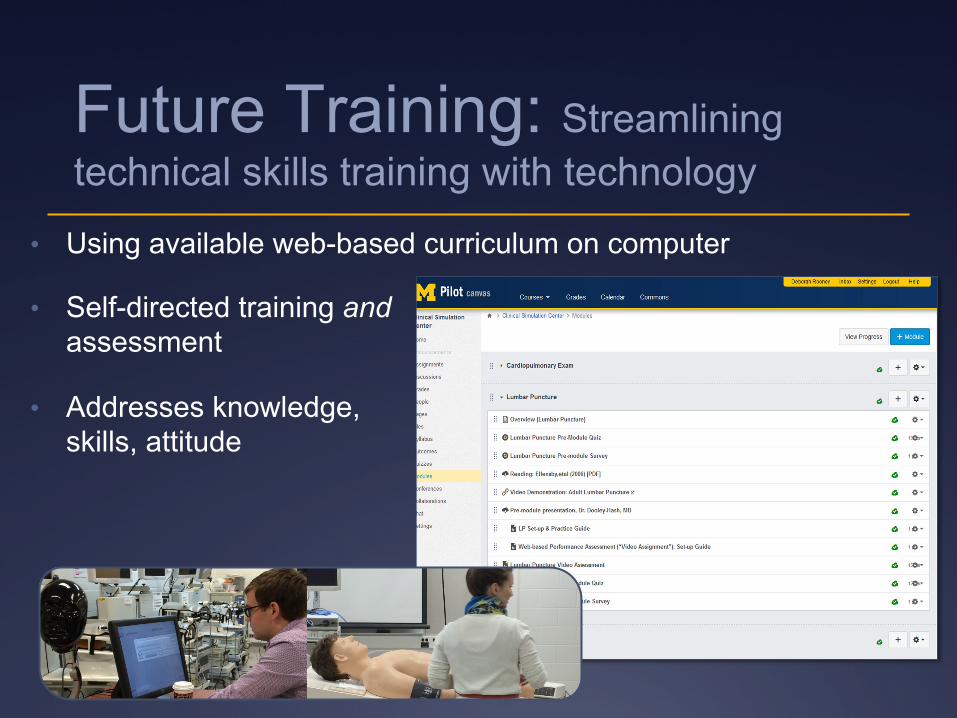
• Using available web-based curriculum on computer
• Self-directed training and assessment
• Addresses knowledge, skills, attitude
Future Training: Streamlining technical skills training with technology
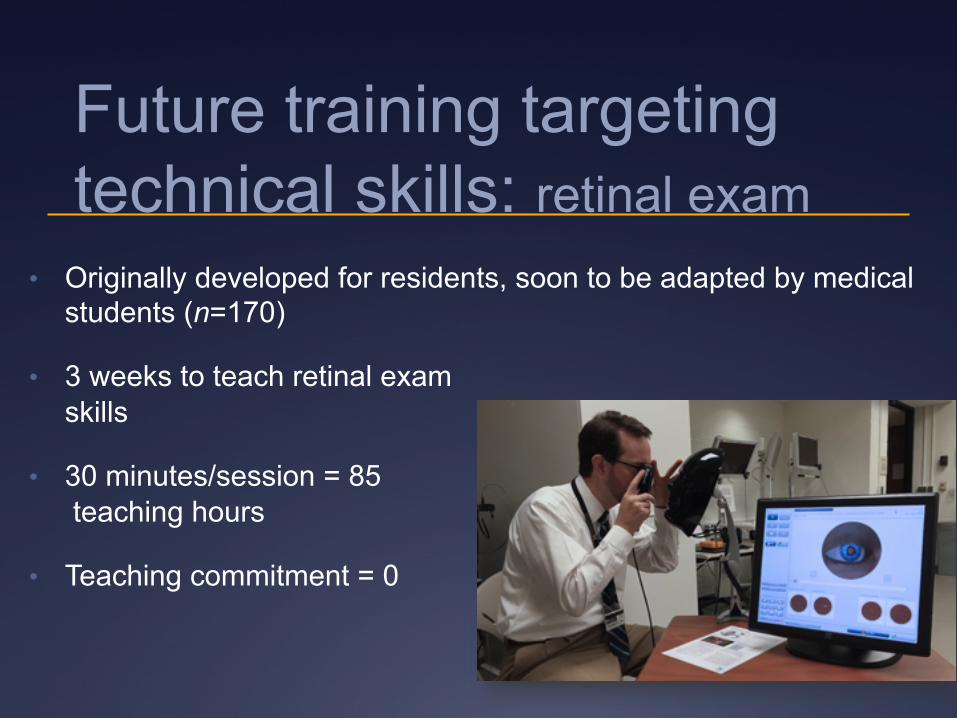
Future training targeting technical skills: retinal exam
• Originally developed for residents, soon to be adapted by medical students (n=170)
• 3 weeks to teach retinal exam skills
• 30 minutes/session = 85 teaching hours
• Teaching commitment = 0

Future training targeting technical skills: endoscopy
Residents; • Family medicine • IM-Gastroenterology • Surgery
ü Self-directed learning
ü 24 hour access
ü Built-in assessment
and there’s more than technical skills…
Future SBE targets: moving beyond technical skills
• Communication and professionalism
• Patient safety & quality improvement
• More complex skills (decision-making)
Communication skills Pediatric ICU (PICU) “Bootcamp”
Trainees: PICU fellows
Learning Goals:
Improve PICU fellows’ reflection/awareness of own communication skills Improve fellows’ awareness of patient/families’ perceptions Improve fellows’ communication skills with patients and families
Day 1 • Introductions • Presentation of family’s story from parent/child • Self-evaluation
Day 2 • Faculty/Parent-educator facilitated simulation
Ongoing Assessment & Evaluation • 360° (nursing staff, faculty, patient/parent, trainee-self)
• On-unit assessment
Communication Bootcamp: logistics
Communication Skills: third-year medical students in Turkey

Conclusions