Embed Size (px)
DESCRIPTION
Key words: pathogenesis, etiology, clinical manifestations, treatment, morbidity, mortality, prognosis, education
Citation preview

Prof Ariyanto Harsono MD PhD SpA(K)
SLERODERMA

Prof Ariyanto Harsono MD PhD SpA(K) 2
Introduction
The term scleroderma is derived from the Greek words skleros (hard or indurated) and derma (skin) and it is used to describe a disease characterized by progressive skin hardening and induration. Hippocrates first described this condition as thickened skin.

Prof Ariyanto Harsono MD PhD SpA(K) 3
Definition
The term systemic sclerosis is used to describe a systemic autoimmune disease of unknown origin characterized by excessive deposition of collagen and other connective tissue macromolecules in skin and multiple internal organs, prominent and often severe fibroproliferative alterations in the microvasculature, and numerous humoral and cellular immunologic abnormalities. Although systemic sclerosis is not inherited, a genetic predisposition plays an important role in its development.

Prof Ariyanto Harsono MD PhD SpA(K) 4
Systemic sclerosis is a complex and heterogeneous disease with clinical forms ranging from limited skin involvement (limited cutaneous systemic sclerosis) to forms with diffuse skin sclerosis and severe and often progressive internal organ involvement (diffuse cutaneous systemic sclerosis), and occasionally a fulminant course (fulminant systemic sclerosis).

Prof Ariyanto Harsono MD PhD SpA(K) 5
Limited cutaneous systemic sclerosis involves areas distal to the elbows and knees but may involve the face and neck. CREST syndrome (Calcinosis, Raynaud phenomenon, Esophageal dysmotility, Sclerodactyly, and Telangiectasias—although not all are needed for the disorder to be called CREST) is an older term used to describe this subset of limited cutaneous systemic sclerosis.

Prof Ariyanto Harsono MD PhD SpA(K) 6
Diffuse cutaneous systemic sclerosis refers to skin thickening affecting the trunk and the skin of the extremities proximal to the elbows and knees besides involvement of the face. There are rare cases of typical systemic sclerosis internal organ involvement in the absence of clinically apparent cutaneous involvement, a clinical subset known as “scleroderma sine scleroderma”.

Prof Ariyanto Harsono MD PhD SpA(K) 7
Pathophysiology Systemic sclerosis is a systemic disease that besides the skin affects
numerous organ systems. The pathogenesis of systemic sclerosis is complex. The clinical and pathologic manifestations result from three distinct processes:
1) severe fibroproliferative vascular lesions of small arteries and arterioles,
2) excessive and often progressive deposition of collagen and other extracellular matrix (ECM) macromolecules in skin and various internal organs, and
3) alterations of humoral and cellular immunity. It is not clear which of these processes is of primary importance or how they are temporally related during the development and progression of the disease.

8
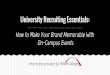
Overall scheme illustrating a current understanding of SSc pathogenesis. Hypothetical sequence of events involved in tissue fibrosis and fibroproliferative vasculopathy in SSc. An unknown causative agent induces activation of immune and inflammatory cells in genetically predisposed hosts resulting in chronic inflammation. Activated inflammatory and immune cells secrete cytokines, chemokines, and growth factors which cause fibroblast activation, differentiation of endothelial and epithelial cells into myofibroblasts, and recruitment of fibrocytes from the bone marrow and the peripheral blood circulation. The activated myofibroblasts produce exaggerated amounts of ECM resulting in tissue fibrosis.

Prof Ariyanto Harsono MD PhD SpA(K) 9
The endothelial cell dysfunction allows the chemokine- and cytokine-mediated attraction of inflammatory cells and fibroblast precursors (fibrocytes) from the bloodstream and bone marrow and their transmigration into the surrounding tissues, resulting in the establishment of a chronic inflammatory process with participation of macrophages and T and B lymphocytes, with further production and secretion of cytokines and growth factors from these cells.

Prof Ariyanto Harsono MD PhD SpA(K) 10
Recent evidence supports the concept that endothelial dysfunction and fibrosis are closely related phenomena and it has been suggested that the vascular alterations, including the phenotypic conversion of endothelial cells into activated mesenchymal myofibroblasts, may be the initiating event and the common pathogenetic alteration leading to the fibrotic and chronic inflammatory involvement of multiple organs.

Prof Ariyanto Harsono MD PhD SpA(K) 11
Etiology The exact etiology of systemic sclerosis is not known. Systemic
sclerosis is not inherited, although a genetic predisposition plays an important role in its development. Environmental factors (eg, triggers or accelerators) may contribute to the development of systemic sclerosis in the proper genetic background. These include the following:
Silica exposure Solvent exposure (vinyl chloride, trichloroethylene, epoxy resins,
benzene, carbon tetrachloride) Radiation exposure or radiotherapy Cytomegalovirus, human herpesvirus 5, and parvovirus B19 have
been proposed as viral accelerating factors.

Prof Ariyanto Harsono MD PhD SpA(K) 12
Complications Complications of systemic sclerosis include the following: o Digital infarctions o Pulmonary hypertension
o Myositis o Renal failure o Wound infections

Prof Ariyanto Harsono MD PhD SpA(K) 13
Mortality/morbiditySystemic sclerosis has the highest case-specific mortality among the systemic
autoimmune diseases. Pulmonary hypertension, pulmonary fibrosis (interstitial lung disease), and scleroderma renal crisis are the most frequent causes of mortality.
Survival has improved in recent decades and correlates best with the clinical disease subtype (diffuse cutaneous vs limited cutaneous) and with the extent of organ involvement. Five-year survival among patients with diffuse cutaneous systemic sclerosis has improved significantly, from 69% in the 1990–1993 cohort to 84% in the 2000–2003 cohort. Five-year survival among the patients with limited cutaneous systemic sclerosis remained very high and unchanged for the same periods (93% and 91%, respectively).
Mortality associated with scleroderma renal crisis has declined significantly during the last decades, as use of angiotensin-converting enzyme (ACE) inhibitors. In contrast, pulmonary involvement (interstitial lung disease and/or pulmonary arterial hypertension) has become the most common cause of death in patients with systemic sclerosis.

Prof Ariyanto Harsono MD PhD SpA(K) 14
Clinical Manifestations Skin manifestations Skin manifestations of systemic sclerosis are as follows:o Progressive skin tightness and induration, often preceded by swelling and
puffiness (edematous stage) that does not respond to diuretic therapy o Skin induration initially affects the fingers (sclerodactyly) and extends proximally.o Tightening of the skin in the face, with a characteristic beaklike facies and paucity
of wrinkles. o Tightening of the skin in the face is often noted very early in the course of the
diseaseo Sclerodactyly with digital ulceration, loss of skin creases, joint contractures, and
sparse hair. o Prominent skin pigmentary changes both hyperpigmentation and
hypopigmentationo Anterior chest demonstrating salt-and-pepper hypopigmentation and diffuse
hyperpigmentation in a white woman. o Diffuse pruritus

15
Vascular manifestationso Raynaud phenomenon is part of the initial presentation in 70% of
patients with systemic sclerosis; 95% eventually develop it during the course of their disease. Raynaud phenomenon may precede obvious systemic sclerosis features by months or even years.Raynaud phenomenon that is not associated with systemic sclerosis or other autoimmune diseases is known as primary Raynaud phenomenon. It occurs in 5-15% of the general population. The female-to-male ratio is 4:1, with onset occurring usually during adolescence.
Other vascular manifestations of systemic sclerosis include the following:
o Healed pitting ulcers in fingertipso Large fingertip ulcers may lead to finger amputationo Cutaneous and mucosal telangiectasiaso Evidence of macrovascular involvement including non-
atherosclerotic myocardial infarction

Prof Ariyanto Harsono MD PhD SpA(K) 16
Gastrointestinal manifestations GI findings in systemic sclerosis include the following:o Gastroesophageal reflux caused by lower esophageal sphincter (LES)
incompetence and decreased or absent peristalsis in the lower two thirds of the esophagus (may lead to hoarseness, dysphagia and aspiration pneumonia)
o Dyspepsia, bloating, and early satietyo Intestinal pseudo-obstructiono Constipation alternating with diarrhea from bacterial overgrowth
(may lead to malabsorption)o Fecal incontinenceo Malnutrition from inadequate caloric intakeo Chronic iron deficiency anemia from occult blood loss

Prof Ariyanto Harsono MD PhD SpA(K) 17
Respiratory manifestations Respiratory compaints in systemic sclerosis include
the following: o Progressive dyspneao Chest pain (precordial) due to pulmonary artery
hypertensiono Dry persistent cough due to restrictive lung
disease

Prof Ariyanto Harsono MD PhD SpA(K) 18
Musculoskeletal manifestations Musculoskeletal complaints in systemic sclerosis include
the following: o Arthralgiao Myalgiao Loss in joint range of motion and joint flexion
contractureso Tendon friction rubso Symptoms of carpal tunnel syndromeo Muscle weakness

Prof Ariyanto Harsono MD PhD SpA(K) 19
Cardiac manifestations Cardiac signs and symptoms in systemic sclerosis include the
following: o Dyspnea due to congestive heart failure or myocardial fibrosiso Palpitations, irregular heart beats, and syncope due to
arrhythmias or conduction abnormalitieso Symptoms of congestive heart failure or right sided heart
failureo Systemic sclerosis is an independent risk factor for acute
myocardial infarction

Prof Ariyanto Harsono MD PhD SpA(K) 20
Renal manifestations Renal signs and symptoms in systemic sclerosis
include the following: o Hypertensiono Renal crisiso Chronic renal insufficiencyo History of high dose corticosteroid use.

Prof Ariyanto Harsono MD PhD SpA(K) 21
Genitourinary manifestations Patients with systemic sclerosis may present with
the following: o Erectile dysfunctiono Bladder fibrosiso Dyspareunia (if introitus is affected)o Vaginal narrowing, dryness and pain caused by
vaginal fibrosis

Prof Ariyanto Harsono MD PhD SpA(K) 22
Eyes, ears, nose, and throat manifestations Patients may present with the following: Sicca syndromeo Poor dentition secondary to sicca syndromeo Loosening of dentition caused by alterations in the tooth
suspensory ligament and thickening of the periodontal membrane
o Hoarseness due to acid reflux with vocal cord inflammation or fibrosis
o Decreased oral apertureo Blindness caused by retinal artery occlusion

Prof Ariyanto Harsono MD PhD SpA(K) 23
Neurologic/psychiatric manifestations Patients may present with the following: o Facial pain and decreased sensation due to trigeminal
neuralgiao Hand paresthesias and weakness due to carpal tunnel
peripheral entrapment neuropathyo Headache and stroke during hypertensive renal crisiso Depression and anxiety

Prof Ariyanto Harsono MD PhD SpA(K) 24
Constitutional manifestations Constitutional complaints in systemic sclerosis
include the following: o Fatigueo Weight losso Loss of appetite

Prof Ariyanto Harsono MD PhD SpA(K) 25
Physical Examination Skin The skin of the hands may be edematous or swollen early in systemic
sclerosis and the patient may initially report these changes as puffiness. This edematous stage precedes the indurated sclerotic stage. Slow progression of the sclerotic phase is associated with a better prognosis, whereas a rapid progression of cutaneous sclerosis indicates a worse prognosis and more extensive and severe visceral organ involvement with an increased risk of renal crisis or interstitial lung disease and higher mortality.
In the sclerotic phase, the skin appears tight and shiny (see image below), with a characteristic loss of hair, decreased sweating, and loss of the ability to make a skin fold. This process of skin thickening usually begins distally on the fingers (sclerodactyly) and progresses proximally in a continuous symmetrical fashion.

Prof Ariyanto Harsono MD PhD SpA(K) 26
Reduced oral aperture (microstomia) caused by perioral fibrosis (assessed by measurements of the incisor-to-incisor distance)

Prof Ariyanto Harsono MD PhD SpA(K) 27
Tightening of the skin in the face, with a characteristic beaklike facies and paucity of wrinkles.

Prof Ariyanto Harsono MD PhD SpA(K) 28
Sclerodactyly with digital ulceration, loss of skin creases, joint contractures, and sparse hair.

Prof Ariyanto Harsono MD PhD SpA(K) 29
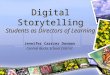
Skin pigmentary changes include a salt-and-pepper appearance, with areas of hyperpigmentation and hypopigmentation, or an overall appearance of darkened skin not related to sun exposure
Anterior chest demonstrating salt-and-pepper hypopigmentation and diffuse hyperpigmentation in a white woman.

Prof Ariyanto Harsono MD PhD SpA(K) 30
Calcinosis may develop in the fingers and extremities, most commonly in the finger tips, the extensor surface of the forearms and in the prepatellar
regions; however, any area of the body can be affected. Occasionally, large calcium deposits with the appearance of tumoral calcinosis may occur
A radiograph of the distal digits demonstrating calcinosis and distal phalanx reabsorption (acral osteolysis).

Prof Ariyanto Harsono MD PhD SpA(K) 31
Eyes, ears, nose, and throat o Salivary production may be decreased and spontaneous
sublingual pooling of saliva may be absent. o Xerostomia and xerophthalmia may be part of the
examination findings. A confirmatory minor salivary gland biopsy may show fibrosis without the pronounced lymphocytic aggregates that would be expected with primary Sjögren syndrome. Furthermore, patients with systemic sclerosis typically do not harbor anti-Ro and anti-La antibodies.
o Funduscopic examination during the hypertensive episodes of scleroderma renal crisis may reveal exudates and vascular alterations. Retinal artery occlusion causing acute loss of vision has been described in rare instances.

Prof Ariyanto Harsono MD PhD SpA(K) 32
Vascular changes Raynaud phenomenon results in characteristic color changes
of pallor, cyanosis, and then erythema (white, blue, red) in the fingers, toes and other acral body parts, and is usually accompanied by numbness, tingling, or pain. These events are triggered by cold exposure, smoking, or emotional stress. Subintimal hyperplasia, typically present in systemic sclerosis vessels, can cause a severe reduction of their luminal diameter, limiting blood flow. The baseline reduction in vessel lumen coupled to an exaggerated response to vasoconstricting stimuli accounts for the severity of Raynaud phenomenon in systemic sclerosis.

Prof Ariyanto Harsono MD PhD SpA(K) 33
Other manifestations of vascular involvement are as follows:o Infarction and dry gangrene of the fingers and toes may be caused
by severe vasospasm superimposed to structural fibrotic and fibroproliferative vascular narrowing
o Some studies suggest that patients with systemic sclerosis have an increased risk of coronary atherosclerosis, peripheral vascular disease, and cerebrovascular calcification compared with healthy individuals, and may develop non-atherosclerotic myocardial infarction

Prof Ariyanto Harsono MD PhD SpA(K) 34
Nail-fold capillary microscopy demonstrates fewer capillaries than normal (ie, capillary loop drop) and numerous dilated and tortuous capillary loops
Fingernail capillary bed demonstrating capillary dropout with large dilated vessels.

Prof Ariyanto Harsono MD PhD SpA(K) 35
Diagnosis Approach Considerations The diagnosis of systemic sclerosis is based on the clinical manifestations.
Nevertheless, a number of tests and procedures may be used in the initial diagnosis (eg, to exclude alternative diagnosis), the assessment of organ involvement, and monitoring of disease progression.
Laboratory testing may include the following:o Complete blood cell count (CBC)o Serum muscle enzyme levelso Erythrocyte sedimentation rateo N-terminal pro-brain natriuretic peptideo Autoantibody assays: Fibrillarin antibodies and antibodies to ribonucleoprotein
(RNP) may be present. Anti-RNP is present mostly in patients with diffuse disease with overlap syndromes and in patients with MCTD. These antibodies are more common in patients with skeletal muscle involvement and pulmonary disease.
o Assessment of gastrointestinal involvement

Prof Ariyanto Harsono MD PhD SpA(K) 36
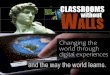
Atrophy of smooth muscle and submucosal fibrotic changes leading to decreased peristalsis throughout the gastrointestinal (GI) tract cause gastroesophageal reflux
disease [GERD], gastroparesis, severe constipation, and pseudo-obstruction.
Barium swallow demonstrating reflux into the distal esophagus, as well as an accordion appearance in the duodenum.

Prof Ariyanto Harsono MD PhD SpA(K) 37
Electrocardiograms (ECGs) should be performed routinely to identify arrhythmias and conduction defects. ECGs can identify early changes of right ventricular strain caused by pulmonary hypertension, and in advanced states, right atrial hypertrophy. Perform 24-hour ambulatory Holter monitoring to evaluate arrhythmias and serious conduction defects.

Prof Ariyanto Harsono MD PhD SpA(K) 38
Histologic Findings The histopathological findings in the skin include marked thickening of the dermis with massive accumulation of dense collagen causing epidermal atrophy, flattening of the rete pegs, and replacement of sebaceous and sweat glands, as well as hair follicles. A prominent inflammatory infiltrate is often present at the dermal-adipose tissue interphase, especially in early lesions. The small vessels of the lower dermis show fibrous thickening but evidence of vasculitis is absent.

Prof Ariyanto Harsono MD PhD SpA(K) 39
Skin biopsy showing severe fibrosis. The fibrosis reflects a widening of collagen bundles in concert with an increase in the number of collagen fibers. Note the superimposed deposition of the newly synthesized delicate collagen
bundles interposed between the preexisting collagen bundles, the latter appearing wide and manifesting a hyalinized morphology.

Prof Ariyanto Harsono MD PhD SpA(K) 40
Lung biopsy demonstrating severe interstitial fibrosis and medial fibrosis and smooth muscle hyperplasia of a pulmonary arteriole compatible with
pulmonary hypertension.

Prof Ariyanto Harsono MD PhD SpA(K) 41
Lung biopsy demonstrating expansion of the interstitium of the lung by fibrous tissue along with chronic inflammatory cells.

Prof Ariyanto Harsono MD PhD SpA(K) 42
Treatment Approach Considerations Current treatment of systemic sclerosis is directed toward
managing complications and providing symptomatic relief. In addition, a range of disease-modifying treatments have been investigated.
Disease-modifying treatment aims at inhibiting tissue fibrosis and
vascular and immune system alterations, which are the three crucial components of disease pathogenesis. To date, however, the US Food and Drug Administration (FDA) has not approved any disease-modifying therapies for systemic sclerosis.

Prof Ariyanto Harsono MD PhD SpA(K) 43
o No placebo-controlled studies have demonstrated clear superiority for any drug except for a modest benefit from use of methotrexate. Numerous uncontrolled prospective and retrospective trials along with post-hoc analysis have suggested a beneficial effect from mycophenolate mofetil.
o Retrospective uncontrolled studies also supported a beneficial role for D-penicillamine, but a large high-dose versus low-dose controlled trial failed to demonstrate benefits of the higher dose versus the lower dose.

Prof Ariyanto Harsono MD PhD SpA(K) 44
o Sildenafil, an inhibitor of phosphodiesterase 5 (PDE-5), has been approved for treatment of pulmonary hypertension. In addition, it has been shown to be effective and well tolerated in patients with Raynaud phenomenon.
Treatments for gastrointestinal symptoms of systemic sclerosis include the following:
o Antacids o Histamine 2 (H2) blockers

Prof Ariyanto Harsono MD PhD SpA(K) 45
Pulmonary Fibrosis/AlveolitisAlthough there is some controversy regarding the
beneficial effects of immunosuppressive therapy in idiopathic pulmonary fibrosis, numerous studies support the use of these agents in systemic sclerosis–associated interstitial lung disease. Pulmonary fibrosis in systemic sclerosis has been successfully treated with
o cyclophosphamide, either orally or in intravenous pulses. Several recent nonrandomized studies have also shown benefit from
o mycophenolate mofetil.

Prof Ariyanto Harsono MD PhD SpA(K) 46
Myositis may be treated cautiously with steroids (first choice), or with methotrexate or azathioprine in corticosteroid-resistant cases or when there are contraindications to corticosteroid use. Doses of prednisone greater than 40 mg/d are associated with a higher incidence of scleroderma renal crisis.

Prof Ariyanto Harsono MD PhD SpA(K) 47
PrognosisSurvival in patients with diffuse cutaneous disease has improved
significantly; currently, the 5-year survival is estimated to be about 80%. Five-year survival in patients with limited cutaneous disease is approximately 90%.
Factors associated with a more severe prognosis are as follows:o Younger ageo African descento Rapid progression of skin symptomso Greater extent of skin involvemento Anemiao Elevated erythrocyte sedimentation rate (ESR)o Pulmonary, renal, and cardiac involvement

Prof Ariyanto Harsono MD PhD SpA(K) 48
Patient Education
To minimize the risk of Raynaud phenomenon flare, instruct patients to maintain their core body temperature; strongly encourage smoking cessation in patients who smoke, and advise all patients to avoid exposure to cigarette smoke. Instruct the patient to avoid digital or skin trauma and prolonged cold exposure.

Prof Ariyanto Harsono MD PhD SpA(K) 49
Reference
Jimenez SA; Chief Editor: Diamond HS: Sleroderma. http://emedicine.medscape.com/article/331864-overview, Accessed 3-Oct, 2014.

Prof Ariyanto Harsono MD PhD SpA(K) 50
Thank you