Embed Size (px)
Citation preview
SURGICAL DISEASES OF THE PARATHYROID GLANDS
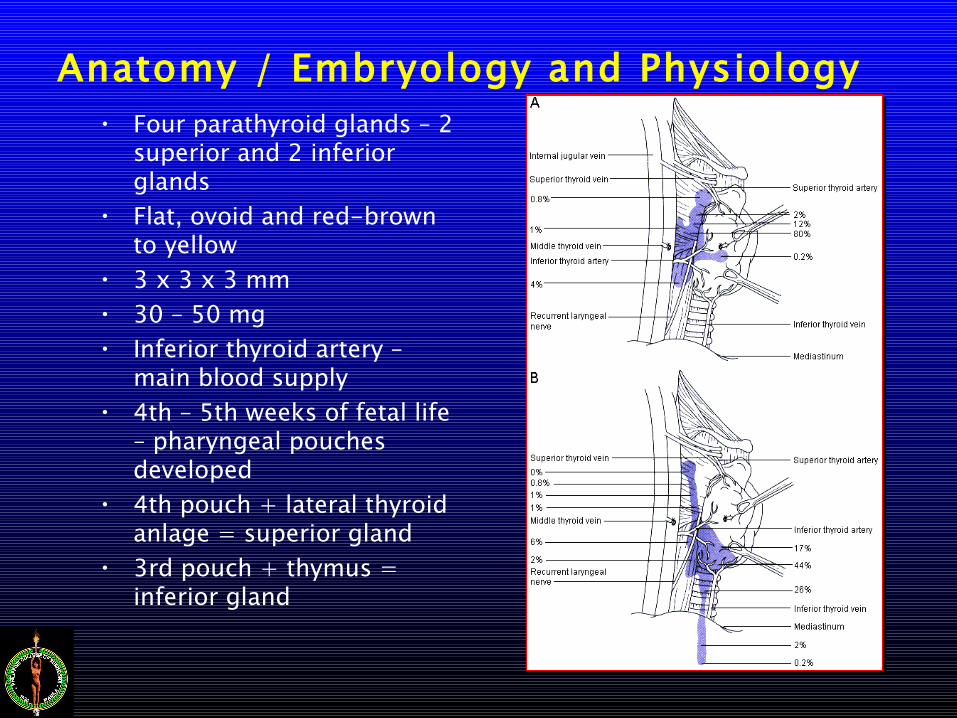
Anatomy / Embryology and Physiology• Four parathyroid glands – 2
superior and 2 inferior glands
• Flat, ovoid and red-brown to yellow
• 3 x 3 x 3 mm• 30 – 50 mg• Inferior thyroid artery –
main blood supply• 4th – 5th weeks of fetal life
– pharyngeal pouches developed
• 4th pouch + lateral thyroid anlage = superior gland
• 3rd pouch + thymus = inferior gland
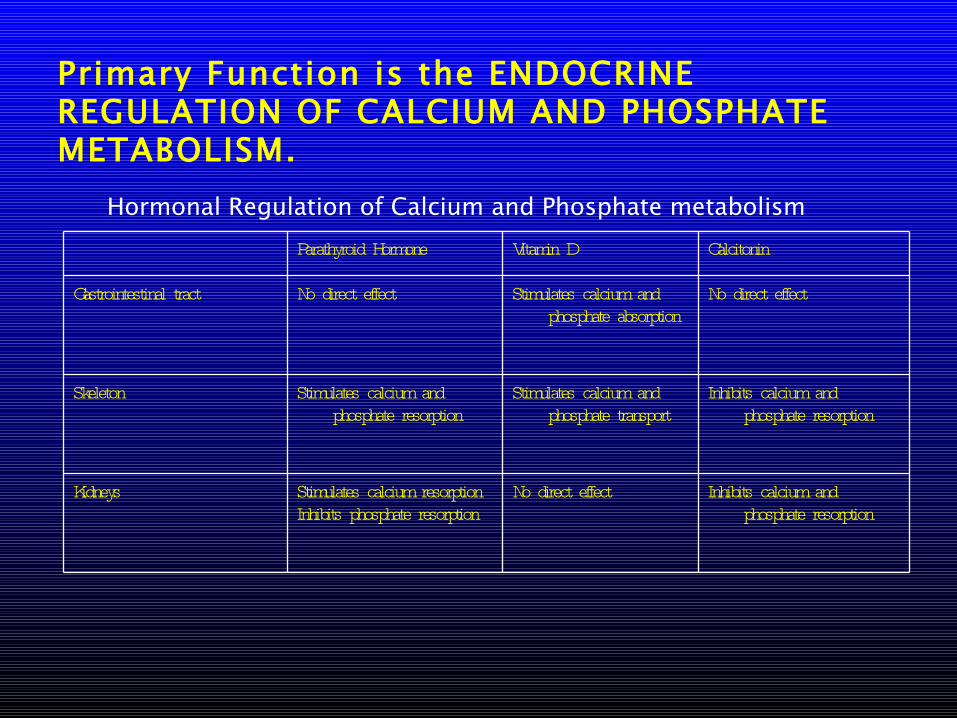
Primary Function is the ENDOCRINE REGULATION OF CALCIUM AND PHOSPHATE METABOLISM.
Parathyroid Hormone Vitamin D Calcitonin
Gastrointestinal tract No direct effect Stimulates calcium and phosphate absorption
No direct effect
Skeleton Stimulates calcium and phosphate resorption
Stimulates calcium and phosphate transport
Inhibits calcium and phosphate resorption
Kidneys Stimulates calcium resorption Inhibits phosphate resorption
No direct effect Inhibits calcium and phosphate resorption
Hormonal Regulation of Calcium and Phosphate metabolism
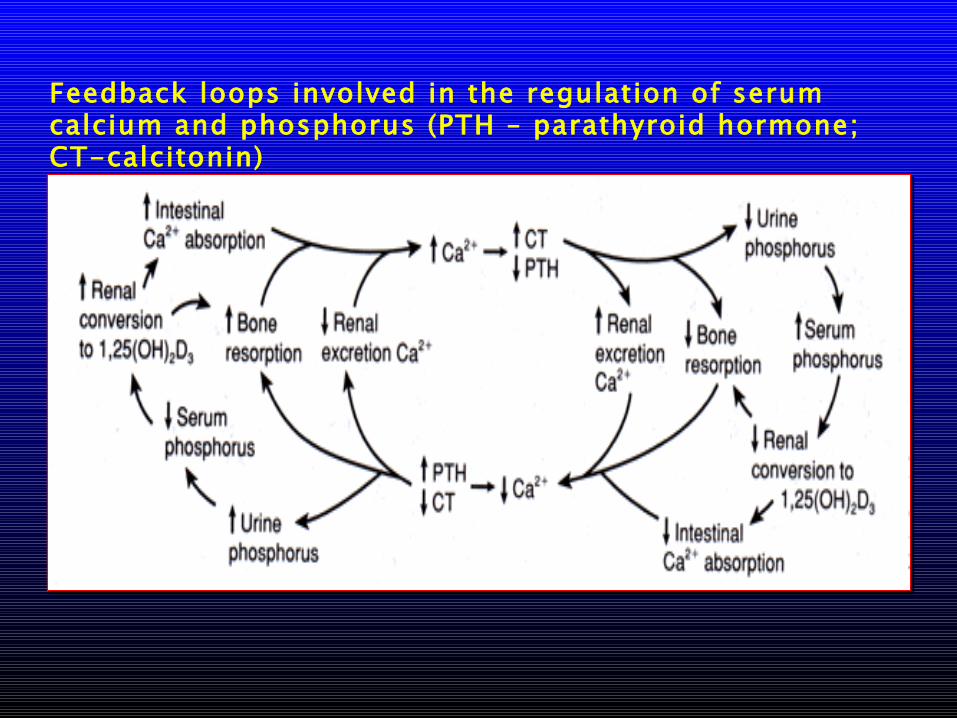
Feedback loops involved in the regulation of serum calcium and phosphorus (PTH – parathyroid hormone; CT-calcitonin)
PRIMARY HYPERPARATHYROIDISM
• Inappropriately increased amounts of parathyroid hormone (PTH) relative to the serum calcium level
• Occurs in 1:1000 population• Increased detection due to increase use of
serum calcium determination
• Three histologic pattern:– SINGLE ADENOMA– HYPERPLASIA– PARATHYROID CARCINOMA
Three histologic patterns are seen: (primary hyperparthyroidism)
• Single adenoma• 90% of cases• A rim of normal parathyroid tissue around the
adenoma distinguishes adenoma from hyperplasia• Hyperplasia
• 10% of cases. • No rim of normal parathyroid tissue and lack of
stromal fats• All 4 glands are involved. • The hyperparathyroidism of MEN syndromes is due to
hyperplasia.• Parathyroid carcinoma - <1% of cases.
• Exceptionally high calcium or palpable neck mass should raise suspicion.
• Excision with thyroid lobectomy is indicated. • Radical neck dissection for recurrent disease. Recur
locally 30%; distant metastasis to lung liver and bone in 30%.
Clinical presentation – primary hyperparathyroidism• 70% are asymptomatic• Stones
• Nephrolithiasis or nephrocalcinosis (never both). • 10-20% of patient• Usually calcium phosphate. Calcium oxalate less
common.• Bones
• Bone pain, arthralgias, and muscular aches.• 20% of symptomatic patients.• Cortical resorption with medullary bone sparing
secondary to increased turnover.• Osteitis fibrosa cystica is the condition where
resorption leads to “Brown cysts” in the bone. Predisposes to fractures.
• Groans• Peptic ulcer disease and pancreatitis• 20% of symptomatic patients
• Psychic overtones• Fatigue, depression, anxiety, irritability, lack of
concentration, and sleep disturbances.• 40% of symptomatic patients.• No relationship of PTH or calcium levels to the
severity of symptoms
• Surgery improves all symptoms except anxiety.
Clinical presentation – primary hyperparathyroidism
Physical examination – primary hyperparathyroidism
• Usually not helpful in diagnosis.
• If a mass is palpable, suspect thyroid pathology or parathyroid carcinoma
Laboratory exam – primary hyperparathyroidism• Hypercalcemia, hypophosphatemia, and hypercalciuria are the
classic hallmarks of hyperparathyroidism• PTH levels are elevated relative to the serum ionized calcium
level (normal or upper normal)• Serum phosphorus will be low in primary
hyperparathyroidism, high in secondary hyperparathyroidism.• Chloride will be high secondary to renal HCO3, wasting (direct
effect of PTH)• Chloride to phosphorus ratio of >33 is diagnostic of primary
hyperparathyroidism; “Poor man’s” parathyroid hormone assay
• Malignancy with or without bone metastasis is the cause of >50% of hypercalcemia (hematologic, lung, pancreas, bone, ovary, breast, and prostate).
Other causes of hypercalcemia include:
• Endocrine disorders - hyperthyroidism, adrenal insufficiency, pheochromocytoma
• Vitamin D toxicity• Lymphomas with ectopic Vitamin D3 production• Granulomatous disease – sarcoidosis, tuberculosis,
histoplasmosis, Coccidioidomycosis, leprosy.• Drugs – thiazides, lithium, milk alkali syndrome.
Immobilization
Radiologic Examinations:
• Subperiosteal resorption in the classic distribution on the radial aspect of the 2nd and 3rd phalangeal tufts, and distal clavicles.
• Solitary bone cysts (Brown tumors)• Intravenous pyelogram (IVP) may show urolithiasis
or nephrocalcinosis.
Medical treatment of hypercalcemic crisis.
• Symptoms include anorexia, nausea, vomiting, polyuria, polydipsia, abdominal pain, lethargy, bone pain, and muscular weakness.
• If untreated may progress to dehydration, oliguria, acute tubular necrosis and delirium within hours.
• Rapid rehydration with normal saline to restore urine output.• Forced diuresis with Furosemide drip (10-20 mg/hr).• Steroids• Etidronate Disodium 7.5 mg/kg IV daily for 3 days followed by
5-20 mg/kg PO daily inhibits bone metabolism in hypercalcemia of malignancy. This should not be used in renal failure patients.
• Mithramycin may be used as a last resort. If not used properly, can lead to aplastic anemia (25 microgram/kg over 4 hours IVPB).
• Dialysis can be used to lower serum calcium emergently.
Management – primary hyperparathyroidism• Surgery is treatment for the hypercalcemia of hyperthyroidism, but
only after hydration with adequate urine output is established.• Surgical indications
– Parathyroid carcinoma– Asymptomatic patients with:
• Persistent calcium elevation 1-1.6 mg/dl above normal• Calciuria >400 mg/day• Decreased bone density > 2 standard deviation points from
normal for age, sex and race.• Creatinine clearance decrease by 30% below normal for age,
sex, and race– Symptomatic patients– Urolithiasis or nephrocalcinosis– Peptic ulcer disease– Pancreatitis– Musculoskeletal symptoms
Surgical options – primary hyperparathyroidism• With single adenoma, resection is curative.
• For hyperplasia, – 3 ½ gland resection – 4-gland resection with ½ gland reimplanted in the
forearm or sternocleidomastoid muscle is indicated.• For parathyroid carcinoma
– Wide excision including involved structures is indicated.
• Initial exploration is successful in 90-95% of cases without pre-op localization studies.
• Ectopic locations: Thymic – substernal – 20%; Posterior neck – 5-10%; Intrathyroid – 5%; Carotid sheath – 1%; Anterior mediastinum – 1-2%.
• If initial exploration fails – localization studies are indicated.
Localization techniques
• Ultrasound – 80% accuracy for glands as small as 3mm. Will not detect mediastinal tumors.
• CT scan / MRI – will detect mediastinal tumors >2 cm.
• Thallium-technetium subtraction scan – 80% accuracy
• Arteriography – 50% accuracy• Selective venous sampling for PTH - 70%
accuracy
Post-operative care.• Airway management• Hypocalcemia is common and occurs almost
immediately.• Monitor serum calcium• Symptoms – anxiety, hyperventilation, Chvostek’s
and Trousseau’s signs, acral and circumoral paresthesias.
• Some advocate treating only symptomatic hypocalcemia.
• Treat hypocalcemia with oral calcium carbonate 1 g PO q6h, or IV calcium gluconate for severe hypocalcemia (< 7.0).
• Vitamin D supplementation may be necessary for refractory hypocalcemia
• Watch out for bleeding and infection

SECONDARY HYPERPARATHYROIDISM• Hyperparathyroidism secondary to malfunction of
another organ system• Usually occurs in patients with chronic renal failure,
but may also be due to osteogenesis imperfecta, Paget’s disease, or multiple myeloma
• Pathophysiology in renal failure– Increased phosphate because of poor renal
excretion Decreased serum calcium, decreased gut absorption of calcium due to decreased renal 1-hydroxylation of vitamin D2 and decreased renal clearance of PTH breakdown products.
Secondary hyperparathyroidism• Clinically manifests as psychiatric disorders, headache,
muscle weakness, weight loss, fatigue, renal osteodystrophy (bone resorption with pathologic fractures) and soft tissue calcifications (vessels, tendons and joint sheaths)
• Treatment is directed at underlying disorder – phosphate-binding antacids, oral calcium and vitamin D, increased calcium dialysate for chronic renal insufficiency patients.
• Surgery is indicated for uncontrolled symptoms – either 3-½-gland parathyroidectomy or 4-gland parathyroidectomy with implantation of minced glands into sternocleidomastoid or forearm muscles marked by a surgical clip.
TERTIARY HYPERPARATHYROIDISM
• Persistent hyperparathyroidism and hypercalcemia following successful renal transplant or resolution of underlying disorder
• Up to 30% of patients who have pre-transplant hyperparathyroidismPathophysiology is irreversible
• Parathyroid gland hyperplasia with autonomous PTH production.
Tertiary hyperparathyroidism
• Surgery is indicated for symptomatic patients or patients unresponsive to medical management 6 months post - transplant – either 3 ½ gland parathyroidectomy with implantation of minced glands into muscle.
THANK YOU