Embed Size (px)
DESCRIPTION
PT treatment for dizziness--presented to NAU doctoral PT students
Citation preview

Benign Paroxysmal Positional Vertigo (BPPV)
Amy Flory PTNAUPT 04/20/09

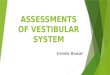
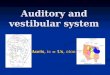
PERIPHERAL VESTIBULAR ANATOMY
• Semi-circular canals– 3 SSC, oriented at right angles to each
other.– Membranous, filled with endolymph,
surrounded by perilymph.– The ampulla contains sensory cells
projecting into the gelatinous cupula.


PERIPHERAL VESTIBULAR ANATOMY
• Otolith organ anatomy– Utricle and saccule are oriented at right
angles to each other.– Sensory hair cells contained within the
macula project into the otolithic membrane.
– The otolithic membrane is embedded with calcium carbonate crystals, called otoconia, or otoliths.

PERIPHERAL VESTIBULAR ANATOMY
• The vestibular nerve is composed of the superior and inferior nerves exiting the vestibular apparatus.– The superior nerve carries information
from anterior and lateral SSCs and the otolith organs.
– The inferior nerve carries information from the posterior SSC and the saccule.

PERIPH. VEST. AFFERENT PHYSIOLOGY
• The sensory receptors of the vestibular nerve are directionally oriented.
• The six SSCs are paired such that each pair is sensitive to motion within one plane of 3D space.
• Matched pairs respond to angular acceleration in an “equal-opposite” fashion.

PERIPH. VEST. AFFERENT PHYSIOLOGY
• Vestibulo-ocular reflex (VOR)– Vestibular apparatus afferents synapse
in vestibular nuclei, then through MLF to Abducens and Oculomotor nuclei, resulting in gaze direction same as endolymph movement.
– Enables gaze stabilization on a stationary target during head movement (image stabilizer)

CENTRAL VESTIBULAR ANATOMY
• The vestibular nuclear complex: 4 “major” nuclei and >7 “minor” nuclei.
• The nuclei are connected with cerebellum, reticular formation, spinal cord, and eye movement systems.

CENTRAL VESTIBULAR EFFERENT ANATOMY
• Medial vestibulospinal tract: originates from medial, superior, descending vest. nuclei and descends bilaterally to the cervical spinal cord in the MLF
• Mediates postural change in response to SSC input (stabilizes head position)

CENTRAL VESTIBULAR ANATOMY
• Lateral vestibulospinal tract: originates from lateral vest. nucleus and descends to the anterior horn cells in the spinal cord
• Mediates postural changes in response to cerebellar and otolithic input (compensates for head tilts and body movements)

CENTRAL VESTIBULAR ANATOMY
• Cervical spinal proprioceptive input–Mostly from facet joints and capsules– Less so from deep paraspinal muscles– None from superficial muscles and skinLuxon, LM. Vertigo: new approaches to
diagnosis and management. British Journal of Hospital Medicine. 1996;56(10):519-520.

CENTRAL VESTIBULAR PHYSIOLOGY
• Varied and widespread vestibular nuc. connections enable postural corrections in different situations (e.g. the postural correction used when the otolithic organs are stimulated is different when the head is forward vs. when it’s turned to the side)

CENTRAL VESTIBULAR PHYSIOLOGY
• Vestibulo-spinal reflex– Actually many different reflexes,
depending on state of system (static, tonic, dynamic). Example: head tilt to one side results in extensor activity ipsilaterally and flexor activity contralaterally while in stance.

CENTRAL VESTIBULAR PHYSIOLOGY
• Smooth pursuit–Maintains gaze on a moving target– Subject follows one finger in 30-40°
arc for 2-3 seconds in each direction
• Saccades– Ballistic eye movements to bring a
periph. visual object to the fovea in shortest possible time
– Subject fixates on target 40° from center on command;3-10 seconds before repeating

CENTRAL VESTIBULAR PHYSIOLOGY
• Nystagmus– Slow phase (peripheral component) is in
opposite direction of perceived head-on-body rotation.
– Fast phase (central component) is in same direction of perceived head-on-body rotation.
• Spontaneous nystagmus usually a central finding, unless <1 week since onset

BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV)
• Cause of 40% of peripheral vestibular cases
• Diagnostic criteria– Nystagmus is predictably produced– Paroxysmal nystagmus (immediate to <10 sec
onset with provoking position)– Symptoms experienced while nystagmus is
present– Fatiguing symptoms and nystagmus– Latency of several seconds– Positionally provoked

BPPV: ETIOLOGY & PRESENTATION
• Cupulolithiasis– Canaliths adhered to the cupula– Immediate onset of symptoms in
provoking position–May continue >1 minute– Eases with return to upright

BPPV: ETIOLOGY & PRESENTATION
• Canalithiasis– Canaliths floating freely in the SSC
endolymph– Latent onset of symptoms in provoking
position– Usually fatigues within 1 minute– Repeats (and reverses) on return to
upright

BPPV: HALLPIKE-DIX TEST
• Patient in long-sitting• Head turned to testing side• “Lie back as quickly as you can”• End position: supine, head 30° below
horizon• Hold position up to a minute without
symptoms

BPPV: VARIANTS
• Posterior canal–Most common form– Nystagmus is torsional and geotropic
toward involved ear in Hallpike-Dix test
• Horizontal/lateral canal– 10% of BPPV cases– Nystagmus is horizontal; may not be
provoked with H-D test (use supine head turns)

BPPV: TREATMENT
• Canalith repositioning–Maneuvers by the therapist in the clinic;
inc. Epley, Modified Liberatory, Semont, BBQ roll, etc..
– Exercises done by the patient at home, TID; inc. Brandt-Daroff exercises, BBQ roll and variants

BPPV: TREATMENT
• Cupulolithiasis– Semont maneuver– Other repositioning maneuver with
mastoid vibration or oscillation– Brandt-Daroff exercises
• Canalithiasis– Canalith repositioning maneuver– Brandt-Daroff exercises

CANALITH REPOSITIONING MANEUVERS
• Goal is to float debris from SSCs and cupula back into utricle
• Timing strategy applied to positioning sequence to approximate migration rate of debris
• All are based on the Epley maneuver

MODIFIED LIBERATORY MANEUVER (MODIFICATION OF EPLEY MANEUVER)
• Patient is quickly moved into H-D position, affected side down; supported there for 4 minutes.
• Turn head slowly (30-45 sec) to opposite H-D position. Hold 4 minutes.
• Patient rolls onto unaffected side, nose pointed to floor, for 30 seconds.
• Return slowly to sitting, then rotate head to face forward, chin slightly tucked.

POST-MANEUVER INSTRUCTIONS
• For 48 hours following maneuver– Avoid looking up or down– Avoid lying below 30 degrees above
horizontal• For 7 days following maneuver– Avoid lying on affected side– Avoid turning head toward affected side
while supine

THANK YOU!
Amy Flory PTCoreBalance Therapy LLC
www.corebalancetherapy.com928-556-9935