Embed Size (px)
Citation preview

Trauma inDisaster
David AlexanderUniversity College London
Evidence
"Now, what I want is, facts. Teach these boys and girls nothing but Facts.Facts alone are wanted in life. Plantnothing else, and root out everythingelse. You can only form the minds ofreasoning animals upon Facts: nothingelse will ever be of any service to them. This is the principle on which Ibring up my own children, and this is theprinciple on which I bring up thesechildren. Stick to Facts, sir!"Thomas Gradgrind in Hard Times
by Charles Dickens
An evidencebase for
everything
Robert Mallet andevidence-based seismology
Evidence can be:-• precise• decisive• equivocal• ambiguous• puzzling• uninterpretable
(evidence of what?)• ignored• distorted• used selectively.
Evidence is no good withoutinterpretation - and the ability tointerpret without misleading people.
Evidence can constrain uncertainty,but cannot eradicate it.
All use of evidence is selective:the criteria of choice determine
the value of the evidence.
Irregular and trending time series poseproblems for the gathering of evidence.
To what extent is evidence asurrogate for experience?
Is evidence "objective data" ormere perception of how the world is?
What is the connectionbetween evidence and wisdom?
How much evidence is enough?Can we do without evidence?.
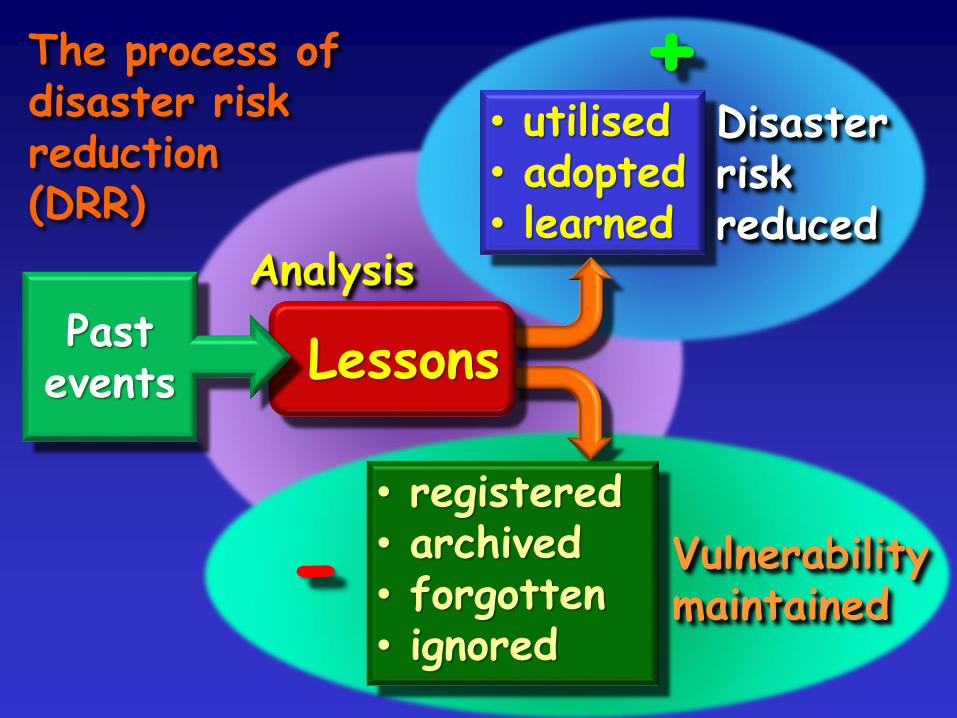
Analysis
• registered• archived• forgotten• ignored
Vulnerabilitymaintained-
• utilised• adopted• learned
Disasterriskreduced
+
LessonsPast
events
The process ofdisaster riskreduction(DRR)

Disaster injuryepidemiology
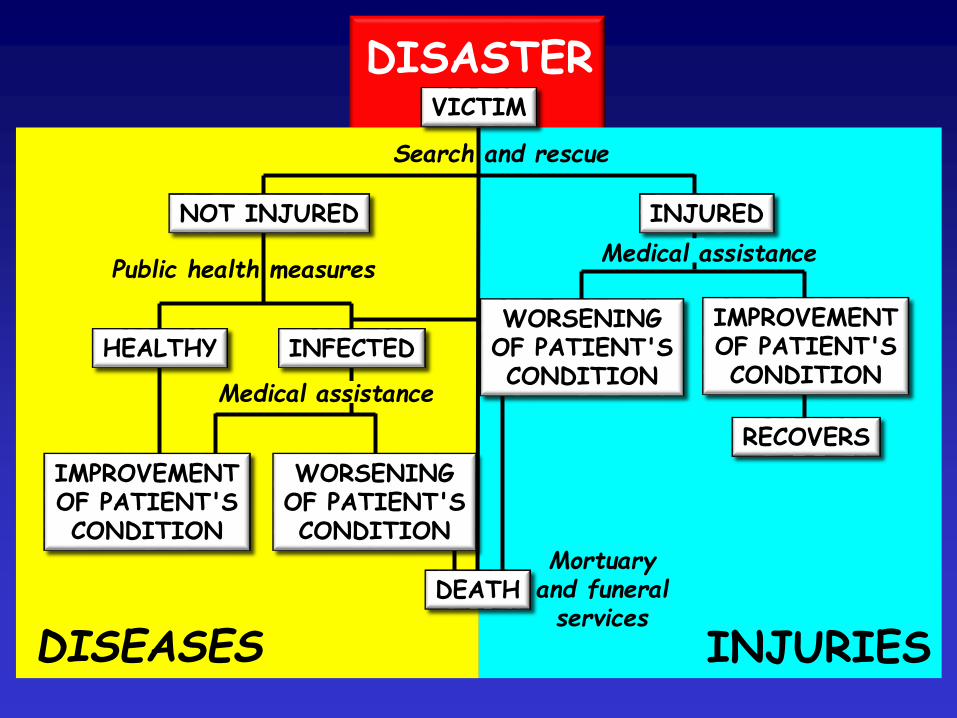
DISASTERVICTIM
NOT INJURED INJURED
HEALTHY INFECTEDWORSENING
OF PATIENT'SCONDITION
IMPROVEMENTOF PATIENT'SCONDITION
RECOVERS
IMPROVEMENTOF PATIENT'SCONDITION
DISEASES INJURIES
Public health measures
Search and rescue
Mortuaryand funeralservices
WORSENINGOF PATIENT'SCONDITION
DEATH
Medical assistance
Medical assistance

Physical injury (physical trauma):-• short-term condition• long-term injury or disease• fatal injury• premature death
Psychological impairment:-• depression• anxiety• post-traumatic stress
(including long-term).
Disaster injury epidemiology
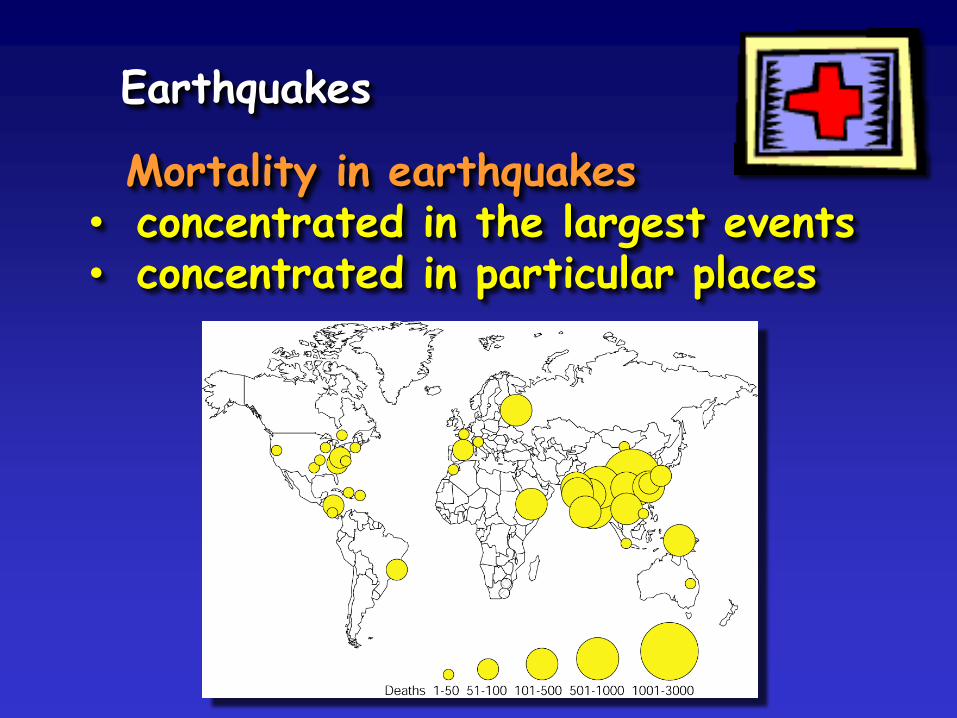
Earthquakes
Mortality in earthquakes• concentrated in the largest events• concentrated in particular places
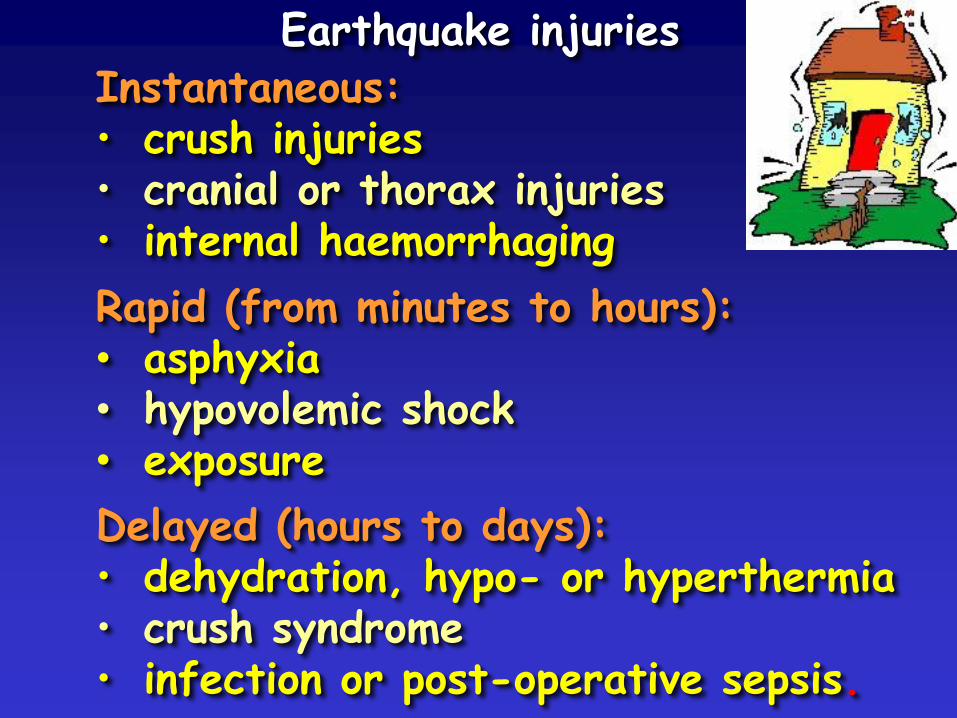
Instantaneous:• crush injuries• cranial or thorax injuries• internal haemorrhaging
Rapid (from minutes to hours):• asphyxia• hypovolemic shock• exposure
Earthquake injuries
Delayed (hours to days):• dehydration, hypo- or hyperthermia• crush syndrome• infection or post-operative sepsis.
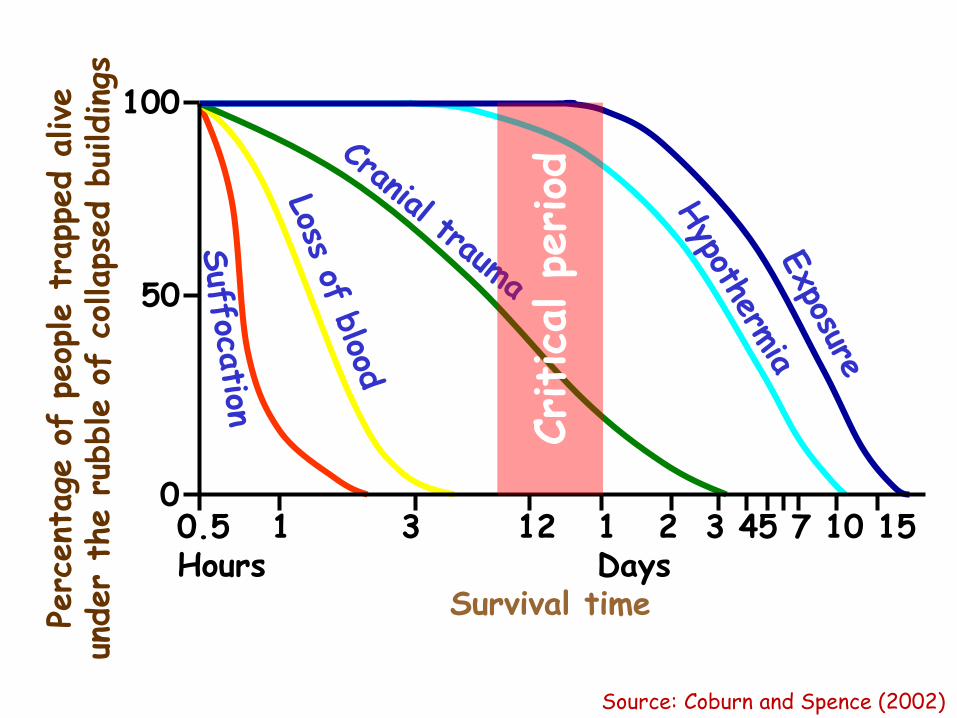
0.5 1 3 12 1 2 3 45 7 10 15Hours Days
Survival time
100
50
0
Perc
ent
age
of
peop
le t
rapp
ed a
live
under
the r
ubble o
f co
llaps
ed b
uildings
Critica
l pe
riod
Source: Coburn and Spence (2002)

No damageto buildings
Damageto buildings
InjuriesEmergency roominjuries
Hospitaladmissions
Source: Linda Bourque, UCLA
In the largest earthquakes
• mortality is 10-85% ofpopulation of the epicentral area
• death/injury ratio 1:3 (hypothesized)
• casualties lessen rapidly withdistance from the epicentre.
Factors that affect mortality andmorbidity in earthquakes
• type, density and state ofmaintenance of buildings
• number of occupants of buildings
• post-earthquake fire
• time of day (aggregatepatterns of human activity).
Active behaviour:• travel to and from work• leisure activities, etc.• mealtimes and family activities
Passive behaviour:• night-time sleep• efficiency and timeliness of post-
earthquake SAR and medical assistance.
At the world scale, most injuriesoccur in nocturnal earthquakes:• a sleeping person is notable to react rapidly
• vernacular housing is particularly at risk• 50-90% of mortality is nocturnal.
Pattern of injured people
• most numerous group: minor injuries
• smaller group: simple fractures
• smaller group: serious multiple injuries
• ratio of serious to slight injuries:from 1:9 to 1:30.
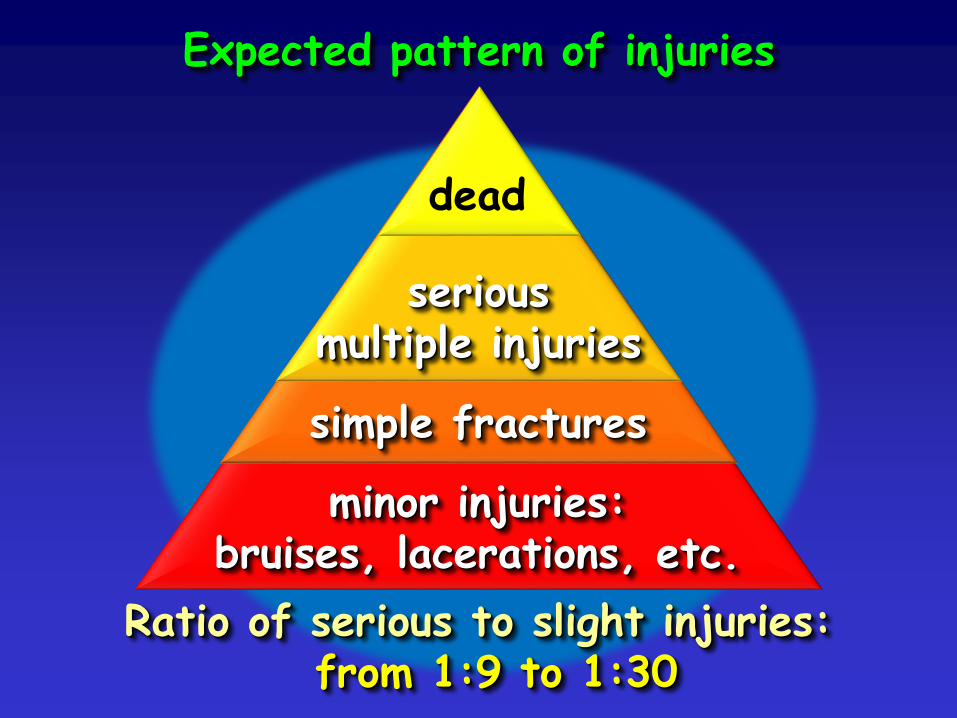
Expected pattern of injuries
minor injuries:bruises, lacerations, etc.
simple fractures
seriousmultiple injuries
Ratio of serious to slight injuries:from 1:9 to 1:30
dead
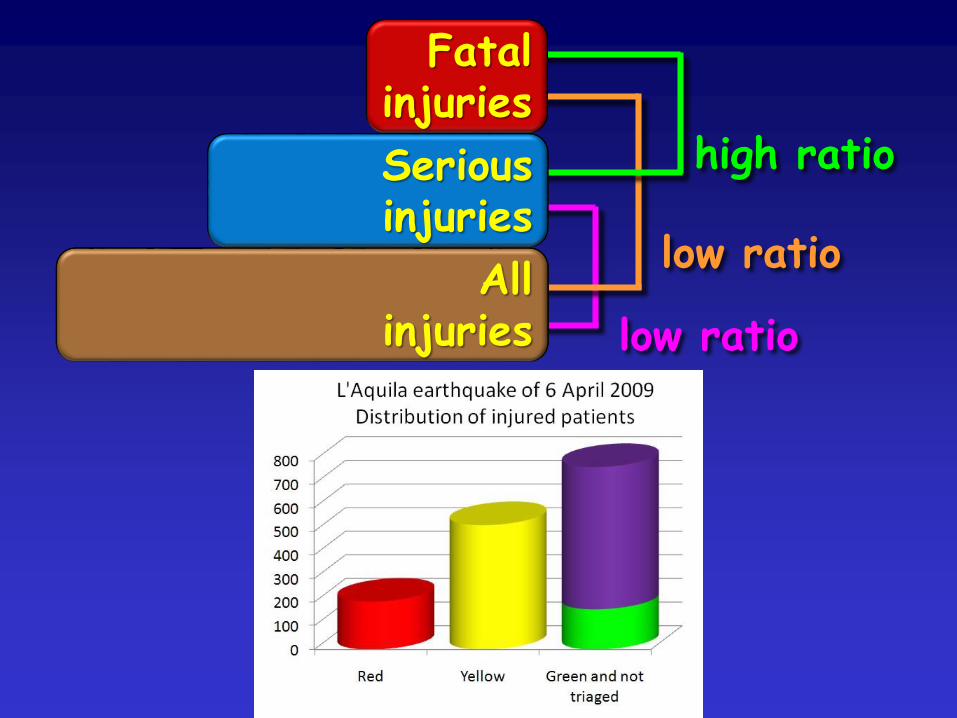
Fatal injuries
Allinjuries
Seriousinjuries
low ratio
low ratio
high ratio
Types of injury
• crush syndrome
• clavicle fracture
• simple lacerations
• bruises and sprains
• fractures of limbs
• surgical cases.
Types of injury (contd.)
• orthopaedic cases
• acute myocardial infarction(heart attack)
• neurosurgery cases
• shock
• severe burns or smoke inhalation
• paraplegia.
Types of injury (contd.)
• gangrene, amputation
• adult respiratory distresssyndrome (ARDS)
• psycho-physical andpsychosomatic problems
• animal bites, electrocutions, drownings
• aggravation of existingmedical conditions.
Ratio of deaths to buildingscollapsed- 8:100 to 16:100
Entrapment increases riskof death 35-100 times
• respiratory difficulties caused bypressure on thorax of fallen objects, orby ingestion of large quantities of dust
• 2-6 hours after earthquake fewer thanhalf of trapped people will still be alive.
Medical procedures
• patient's condition must be stabilisedimmediately after he or she is rescued
• advanced trauma life support (ATLS)
• life support first aid (LSFA)
• resuscitatory surgery
• field analgesia and anesthesia
• resuscitative search and rescue
• intensive therapies.

Disaster Risk Reduction
or disaster risk creation?
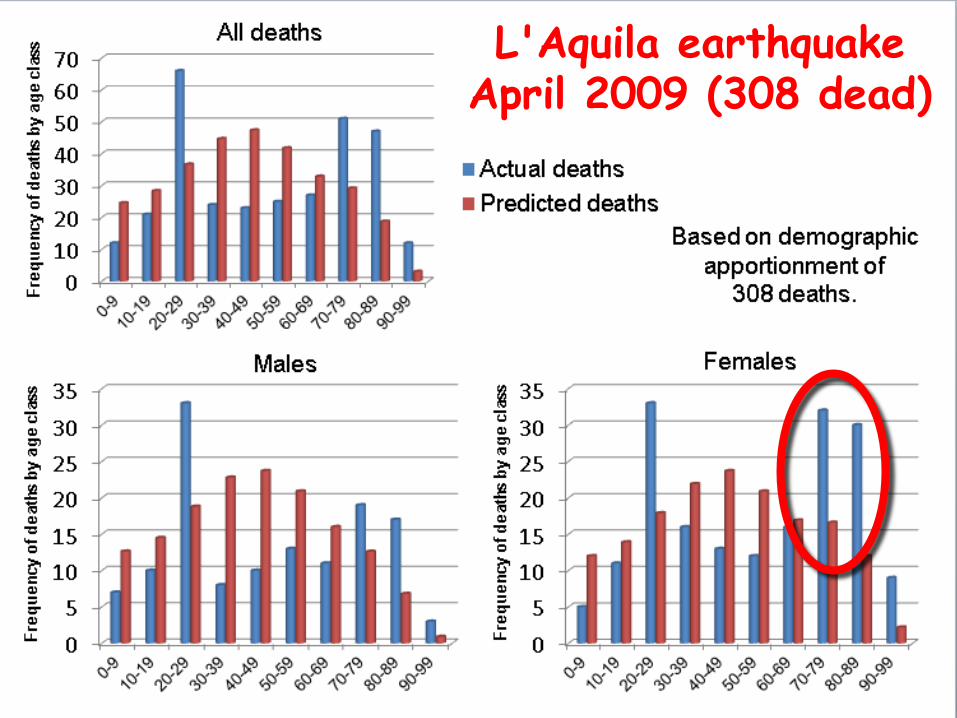
L'Aquila earthquakeApril 2009 (308 dead)
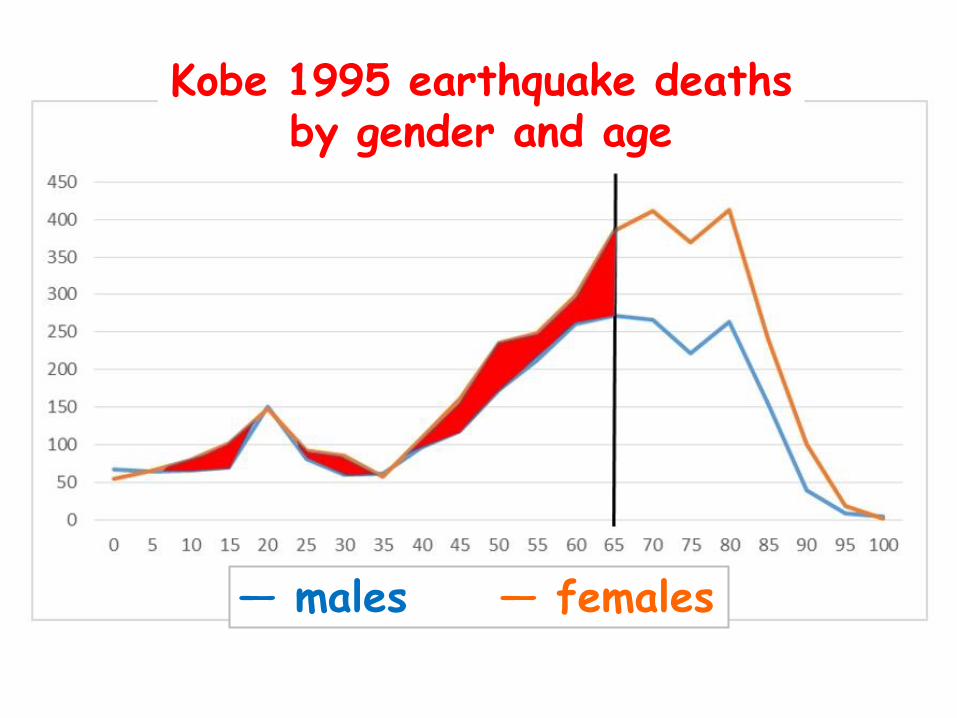
Kobe 1995 earthquake deathsby gender and age
― males ― females
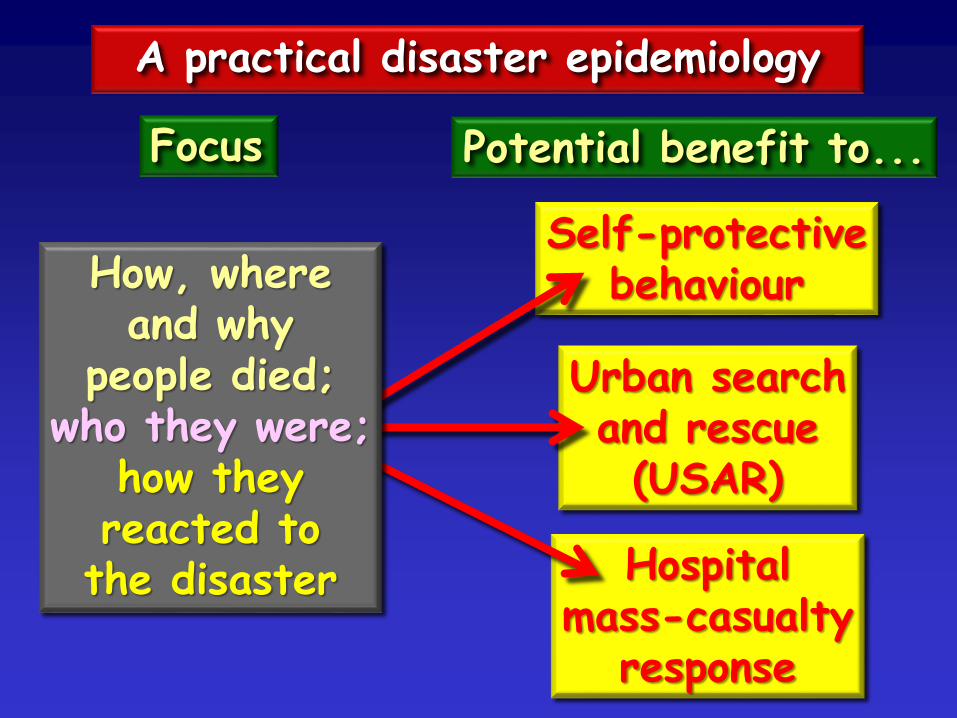
Self-protectivebehaviour
Hospitalmass-casualty
response
Urban searchand rescue(USAR)
A practical disaster epidemiology
Focus Potential benefit to...
How, whereand why
people died;who they were;
how theyreacted tothe disaster
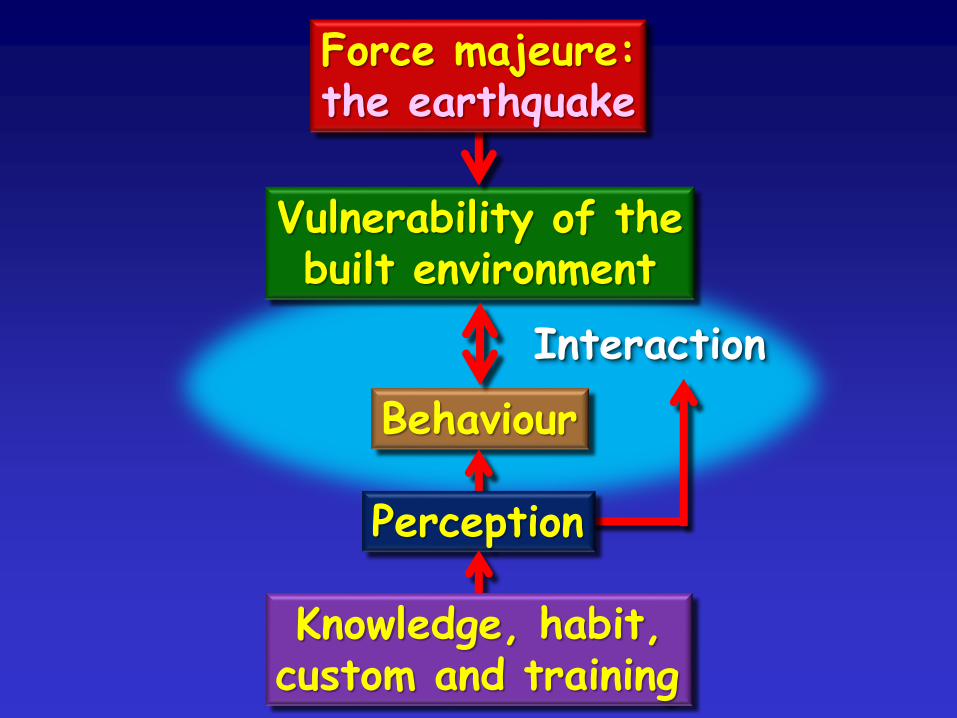
Behaviour
Vulnerability of thebuilt environment
Interaction
Force majeure:the earthquake
Perception
Knowledge, habit,custom and training

?
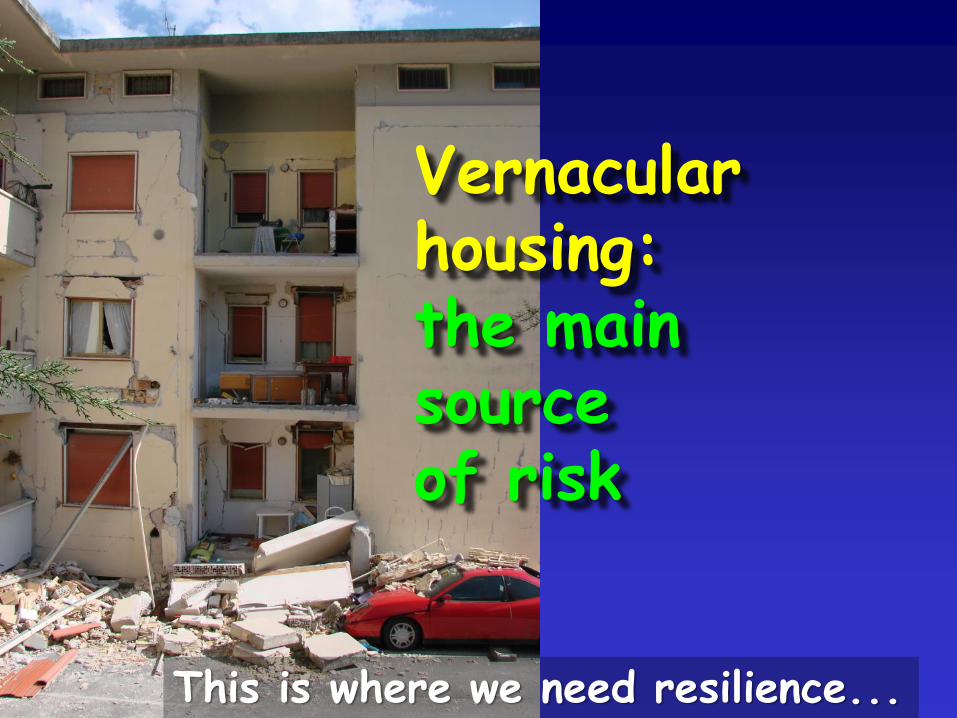
Vernacularhousing:the mainsourceof risk
This is where we need resilience...
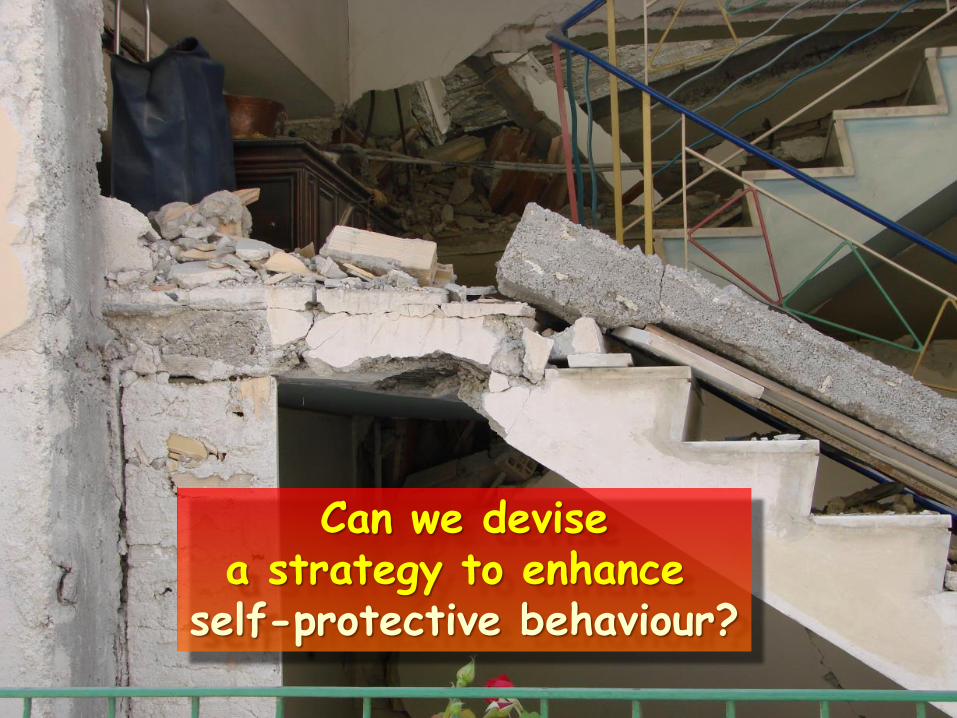
Can we devisea strategy to enhance
self-protective behaviour?
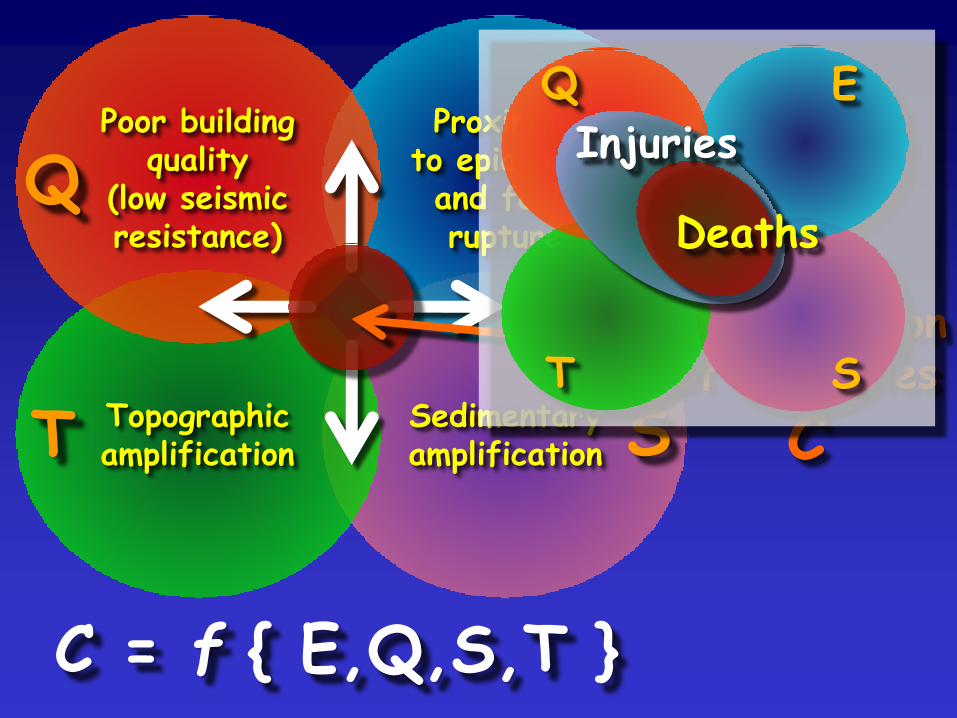
Poor buildingquality
(low seismicresistance)
Proximityto epicentreand faultrupture
Topographicamplification
Sedimentaryamplification
Q E
T S
Concentrationof casualties
C
C = f { E,Q,S,T }
Deaths
Injuries
Q E
T S

Building quality and seismic resistance:
• site factors

Building quality and seismic resistance:
• building type and materials
[Masonry] [Reinforced concrete]

• plan and elevation of building
Building quality and seismic resistance:
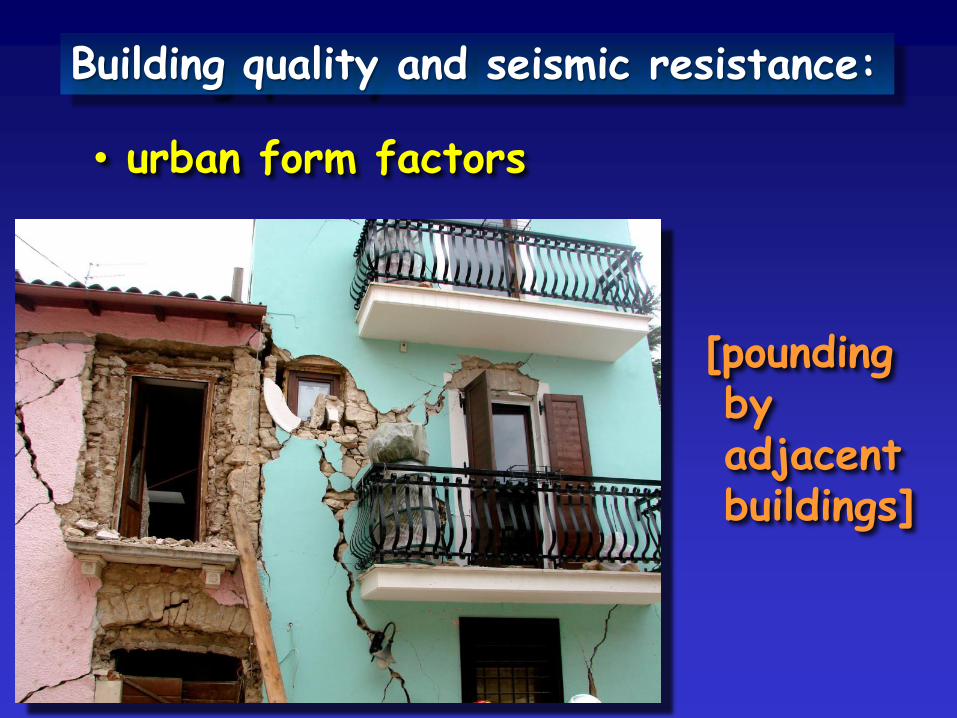
Building quality and seismic resistance:
• urban form factors
[poundingbyadjacentbuildings]
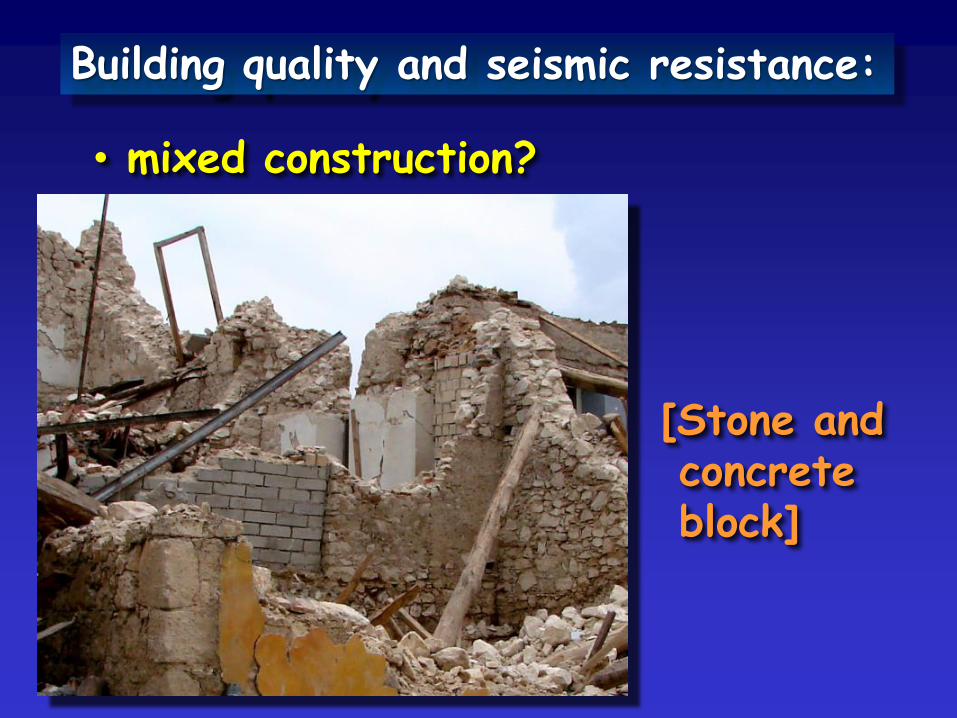
Building quality and seismic resistance:
• mixed construction?
[Stone andconcreteblock]

Building quality and seismic resistance:
• state of maintenance

Building quality and seismic resistance:
• occupancy factors
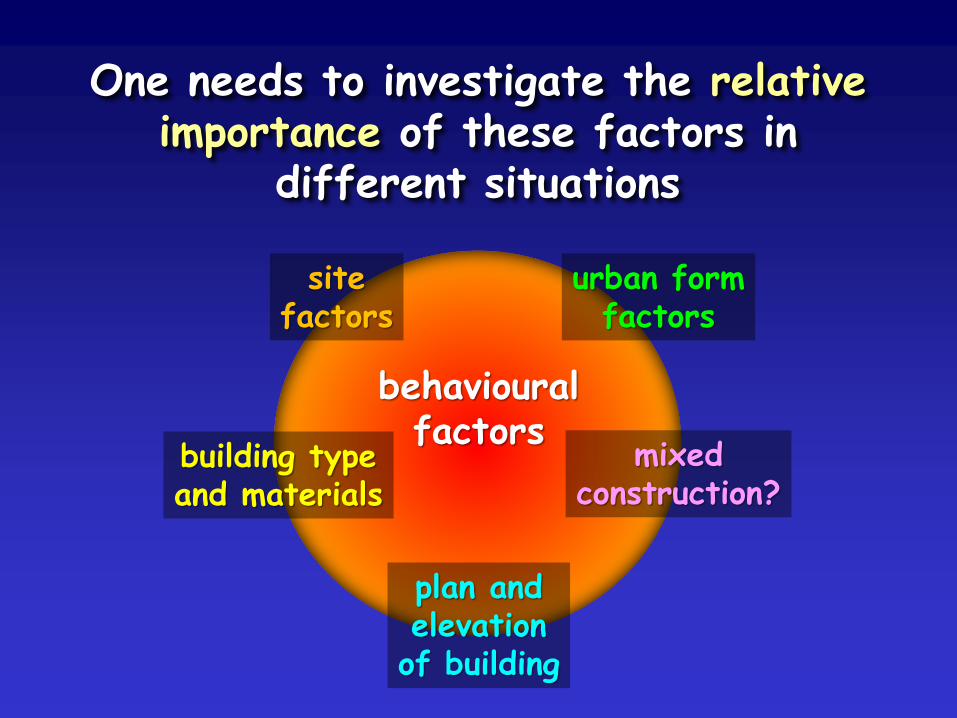
One needs to investigate the relativeimportance of these factors in
different situations
sitefactors
building typeand materials
plan andelevationof building
urban formfactors
mixedconstruction?
behaviouralfactors
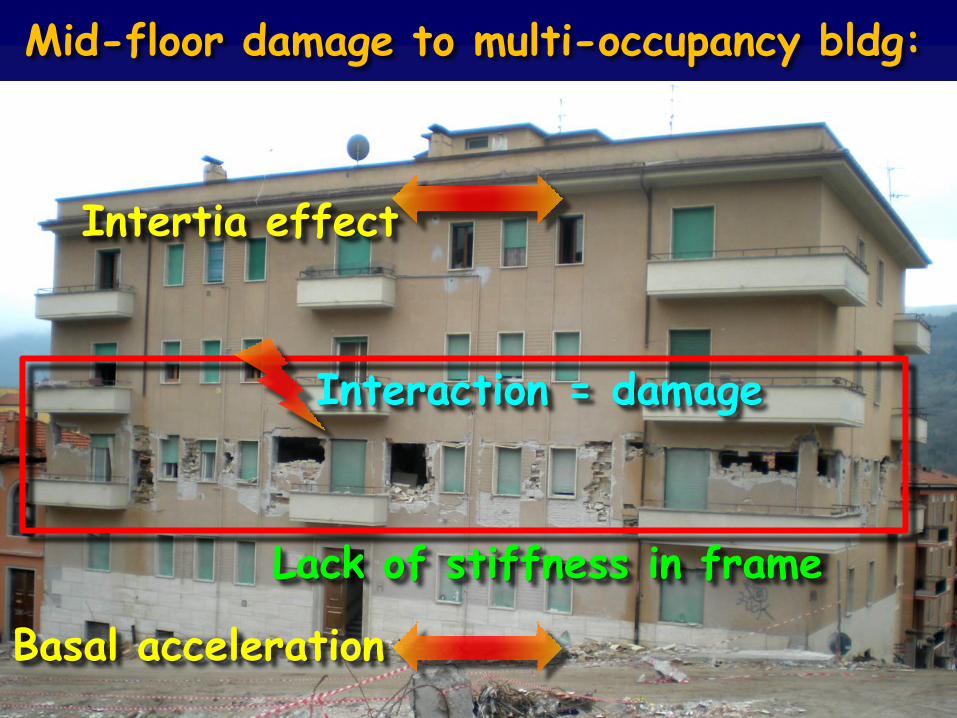
Mid-floor damage to multi-occupancy bldg:
Intertia effect
Basal acceleration
Interaction = damage
Lack of stiffness in frame
For example... what is the typicalpattern of seismic failure of Iranianvernacular housing of any given type?
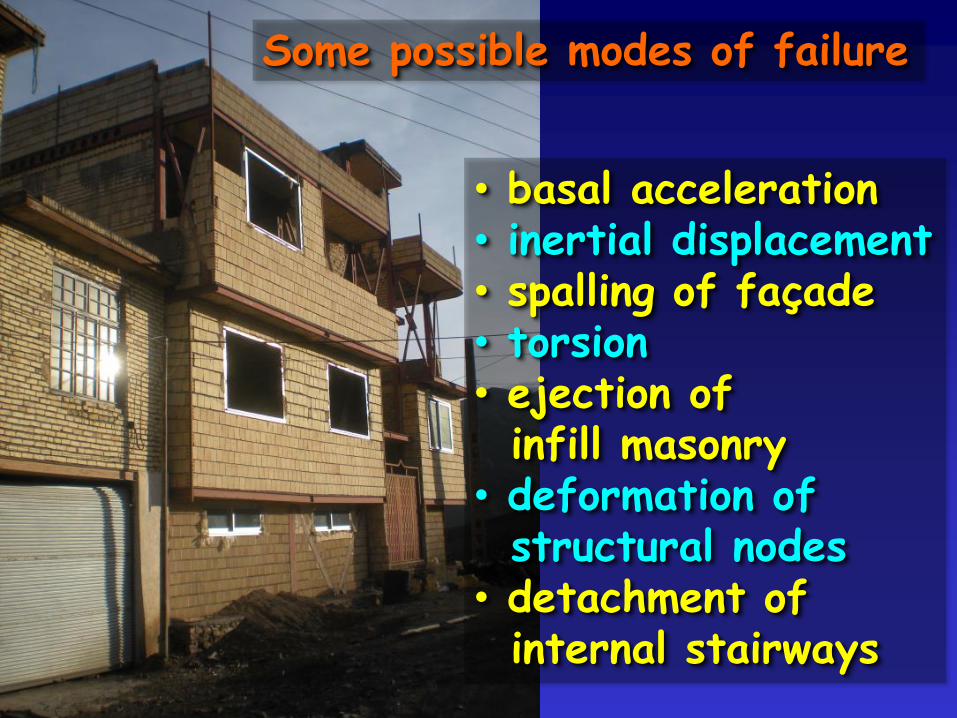
• basal acceleration• inertial displacement• spalling of façade• torsion• ejection ofinfill masonry
• deformation ofstructural nodes
• detachment ofinternal stairways
Some possible modes of failure
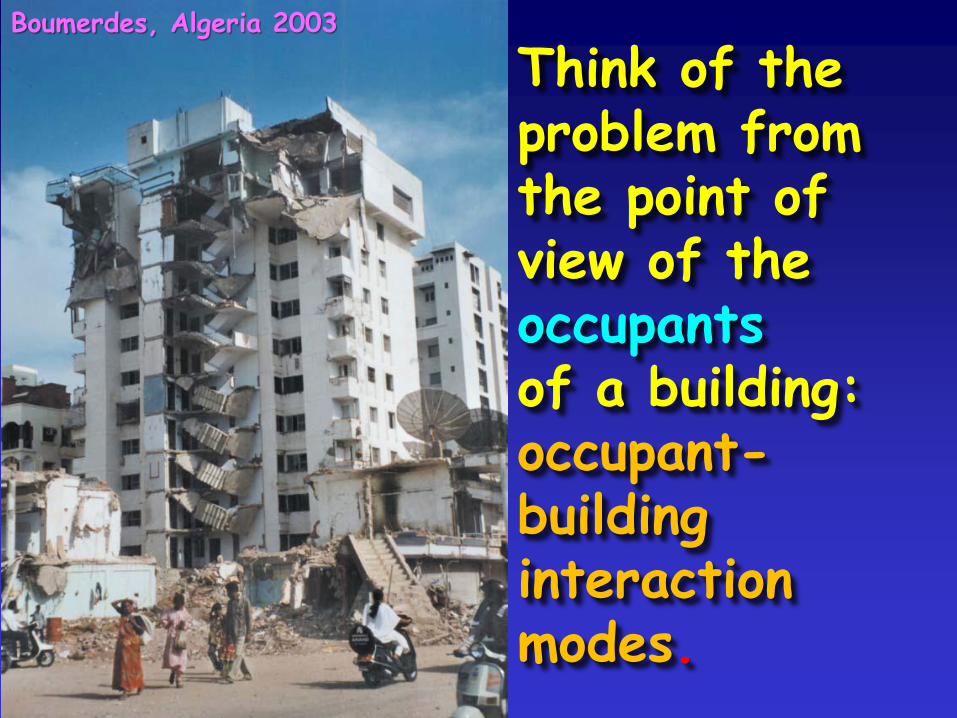
Think of theproblem fromthe point ofview of theoccupantsof a building:occupant-buildinginteractionmodes.
Boumerdes, Algeria 2003
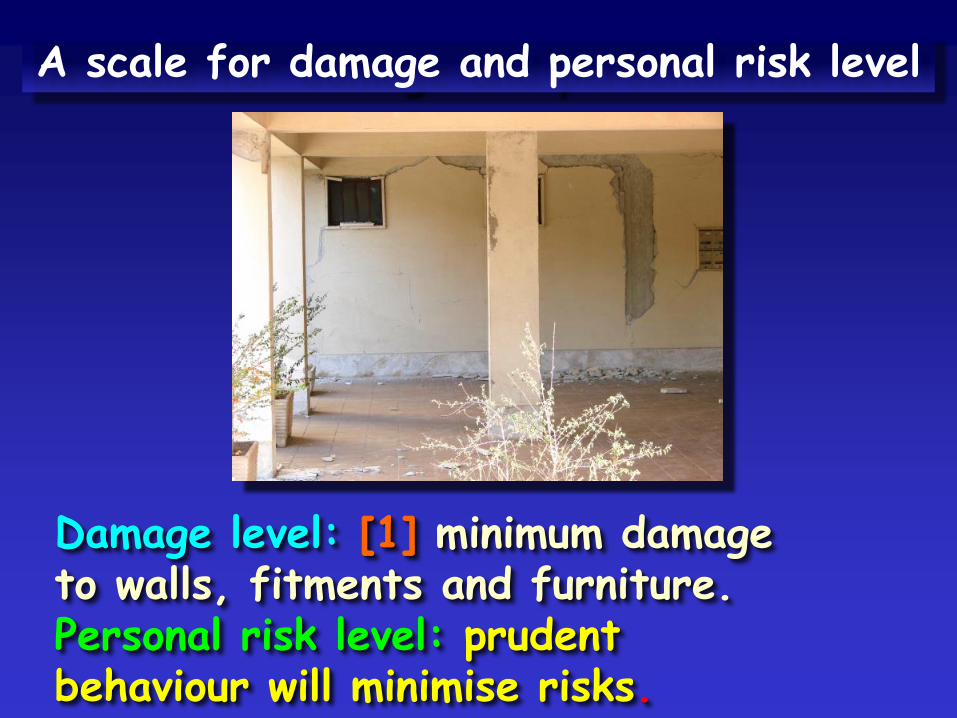
A scale for damage and personal risk level
Damage level: [1] minimum damageto walls, fitments and furniture.Personal risk level: prudentbehaviour will minimise risks.
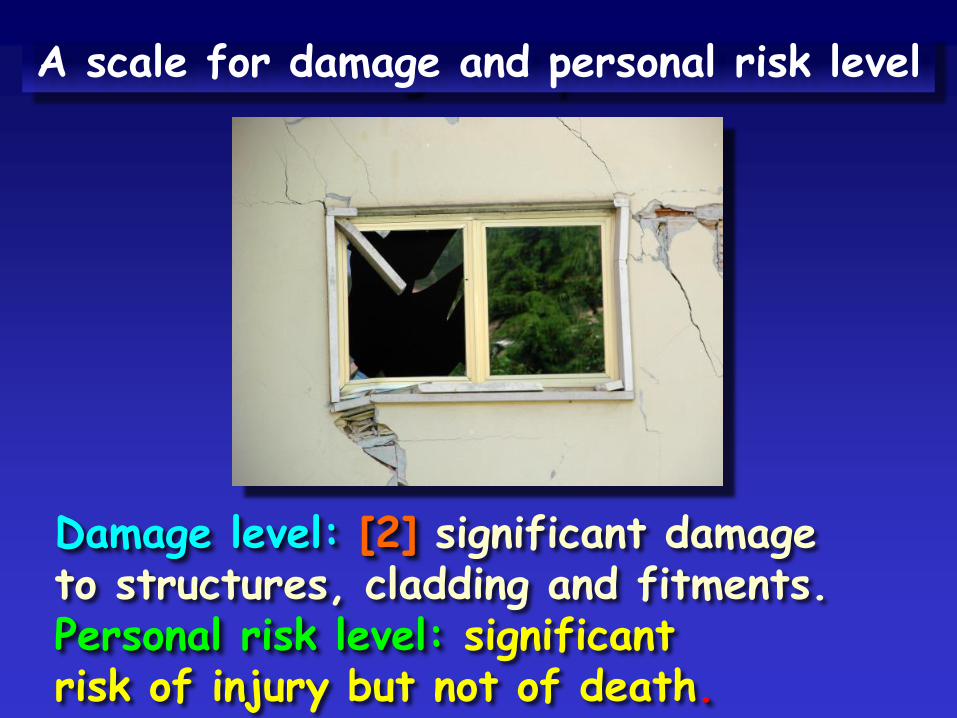
Damage level: [2] significant damageto structures, cladding and fitments.Personal risk level: significantrisk of injury but not of death.
A scale for damage and personal risk level
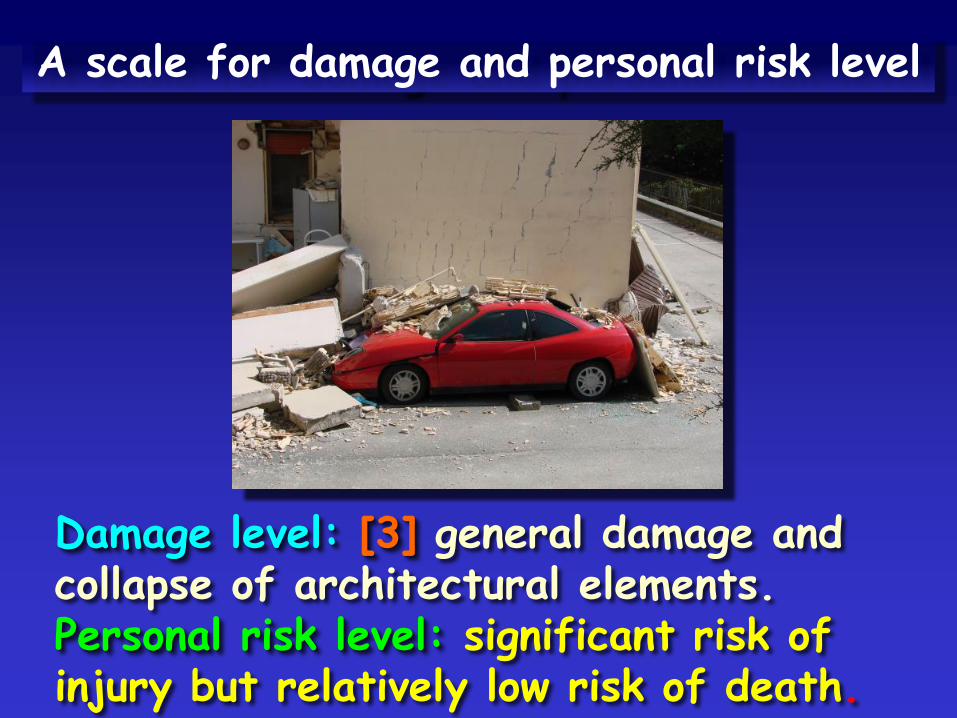
Damage level: [3] general damage andcollapse of architectural elements.Personal risk level: significant risk ofinjury but relatively low risk of death.
A scale for damage and personal risk level
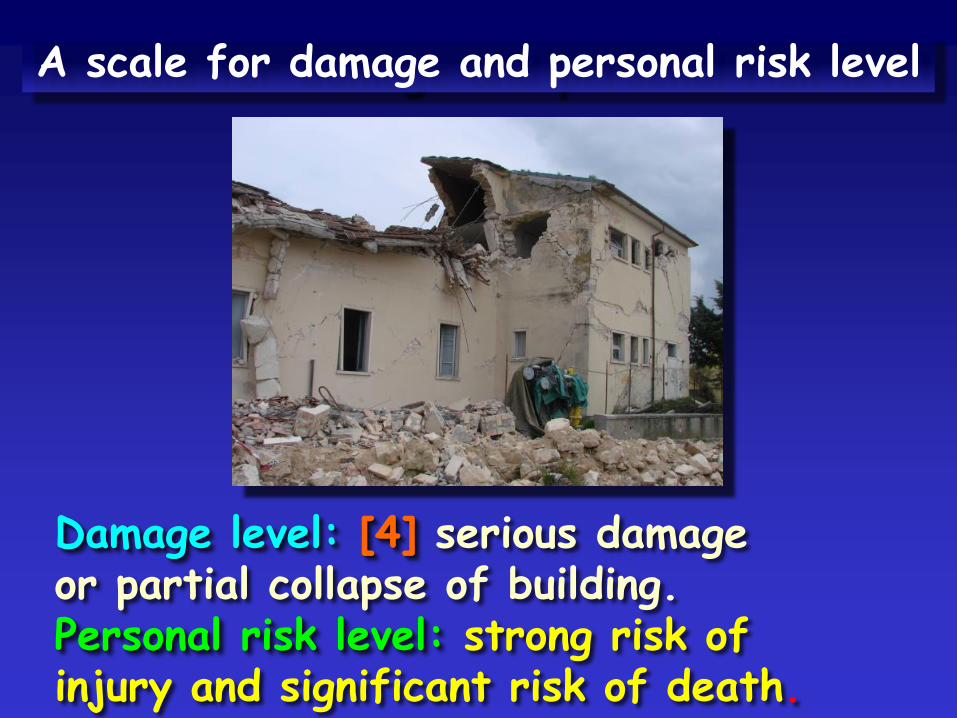
Damage level: [4] serious damageor partial collapse of building.Personal risk level: strong risk ofinjury and significant risk of death.
A scale for damage and personal risk level
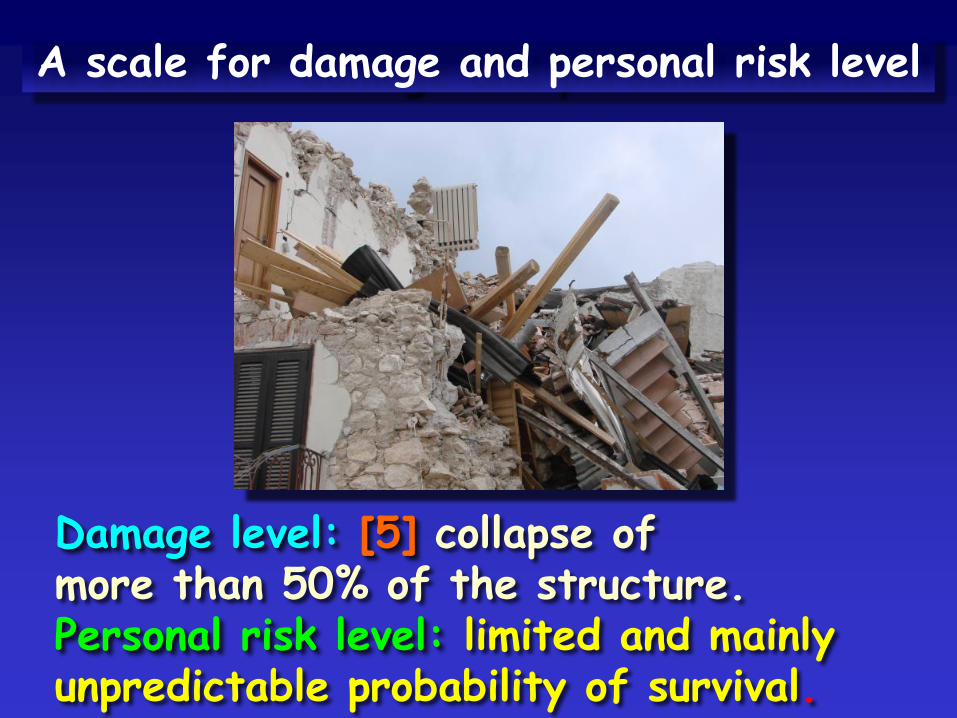
Damage level: [5] collapse ofmore than 50% of the structure.Personal risk level: limited and mainlyunpredictable probability of survival.
A scale for damage and personal risk level
In the case of total collapse, littlecan be done for the occupants of abuilding except urban heavy rescue.
This is up to three times more likelyto be successful if the locationof trapped occupants is known
(e.g. they can attract attention).
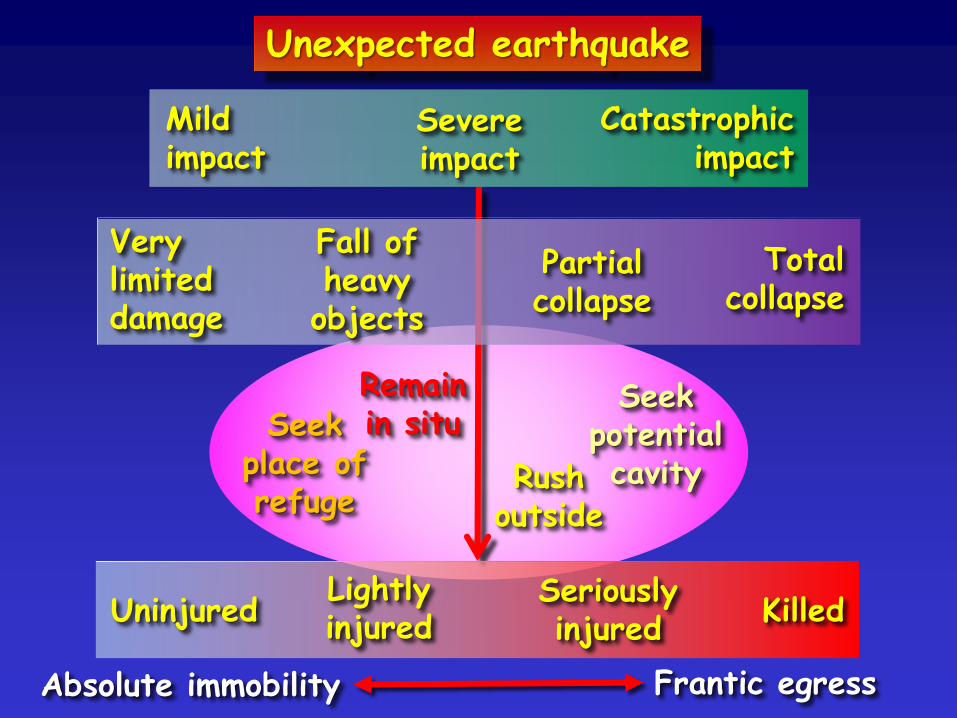
Seekplace ofrefuge
Remainin situ
SeekpotentialcavityRush
outside
Unexpected earthquake
Mildimpact
Severeimpact
Catastrophicimpact
Verylimiteddamage
Fall ofheavyobjects
Partialcollapse
Totalcollapse
Absolute immobility Frantic egress
UninjuredLightlyinjured
Seriouslyinjured
Killed
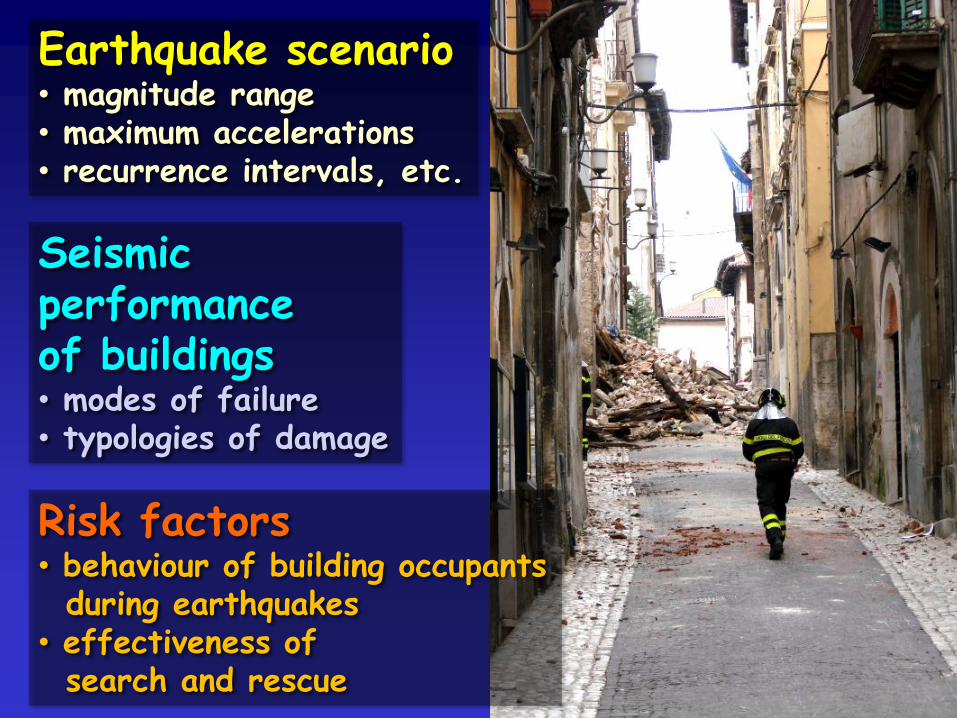
Earthquake scenario• magnitude range• maximum accelerations• recurrence intervals, etc.
Seismicperformanceof buildings• modes of failure• typologies of damage
Risk factors• behaviour of building occupantsduring earthquakes
• effectiveness ofsearch and rescue
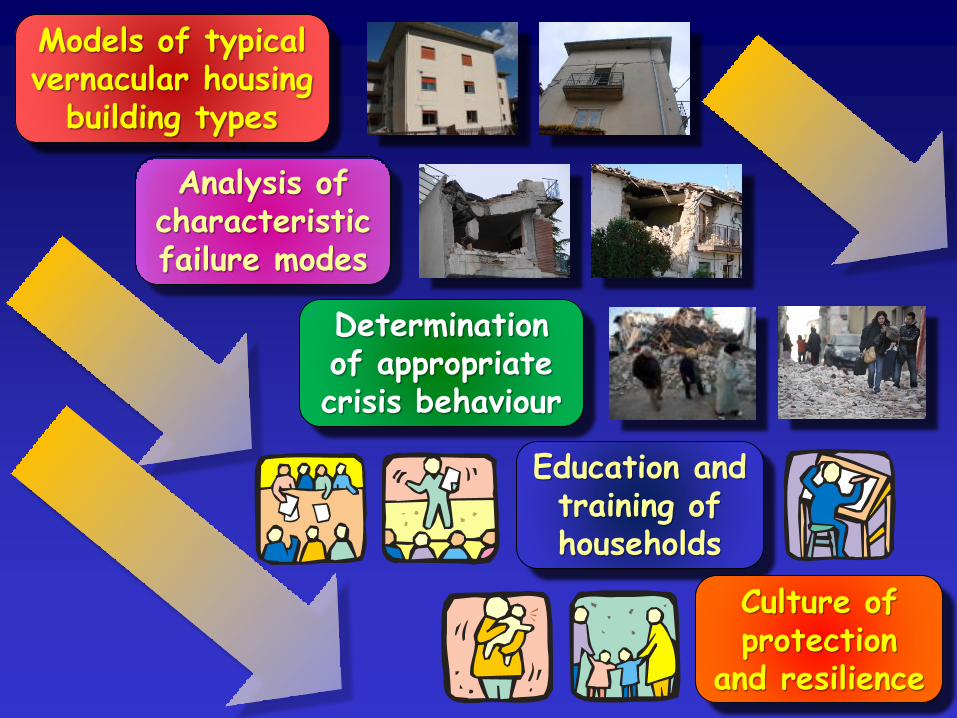
Models of typical vernacular housing
building types
Analysis ofcharacteristicfailure modes
Determinationof appropriatecrisis behaviour
Education andtraining ofhouseholds
Culture ofprotection
and resilience
Psychological trauma
It is very rare that acutepathological reactions and lasting
mental illness are caused by disaster.
Instead, the most commonconsequences are:-
• depression
• post-traumatic stress disorder(PTSD), including criticalincident stress (CIS).
Disaster is a test of thepsychological stability of the individual
• healthy behaviour meansactivating internal mechanismsthat restore a sense of calm
• unhealth behaviour means thenegation of experience ordisintegration of the personality.
How an individual receives signs of danger:
• decoding them and reacting appropriately
• negating them and not reacting
• not understanding their significance andnot reacting in the most appropriate way:- e.g., when the environmental signs of
disaster are neither clear nor familiar
• understanding them, but neverthelesslosing his or her equilibrium:- the persion is overwhelmed
by fear of death and feelsabandoned or too vulnerable.
Riskaversion
Risktolerance
Riskdenial
Risk-seekingbehaviour
Critical incident stress (CIS)is a form of
post-traumatic stress disorderwhich affects first responderswho work in conditions that aredifficult, dangerous or dramatic.
• physical (e.g. nausea, upset stomach)
• cerebral (e.g. repeated bad dream)
• behavioural (e.g. angry outbursts)
• emotional (e.g. anxiety)
• immediate or delayed.
Symptoms of PTSD and CIS
In emergencies loss of sense of perspective can occur, leading to:-
Magna Mater complex: trying to solve all the problems of the moment
Jehovah complex: believing one isable to solve all existing problems
Tiredness can distort perceptionand cause bad decision-making
Solution: take a break, rest and unwind.

Panic?
Criticisms of the concept of panic:-
• social chaos may mask rational individual behaviour
• panic is a stereotypeand a popular myth
• running away might be the mostrational response to imminent danger
• hindsight analysis cangive the wrong perspective
• social bonds can survive major shocks.

Nepal
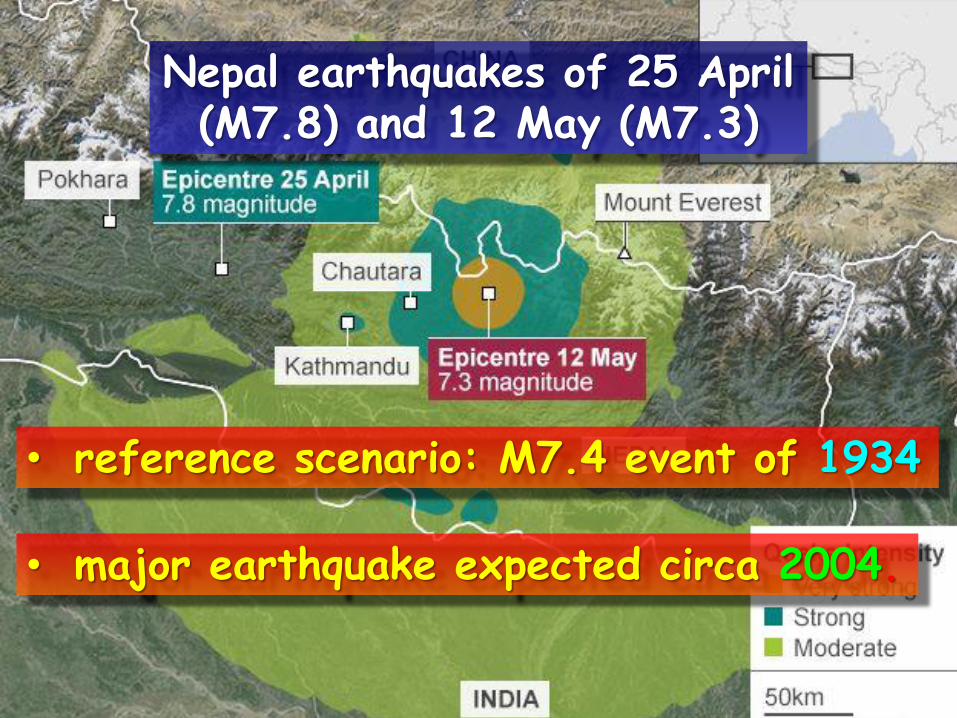
• reference scenario: M7.4 event of 1934
• major earthquake expected circa 2004.
Nepal earthquakes of 25 April(M7.8) and 12 May (M7.3)

1934
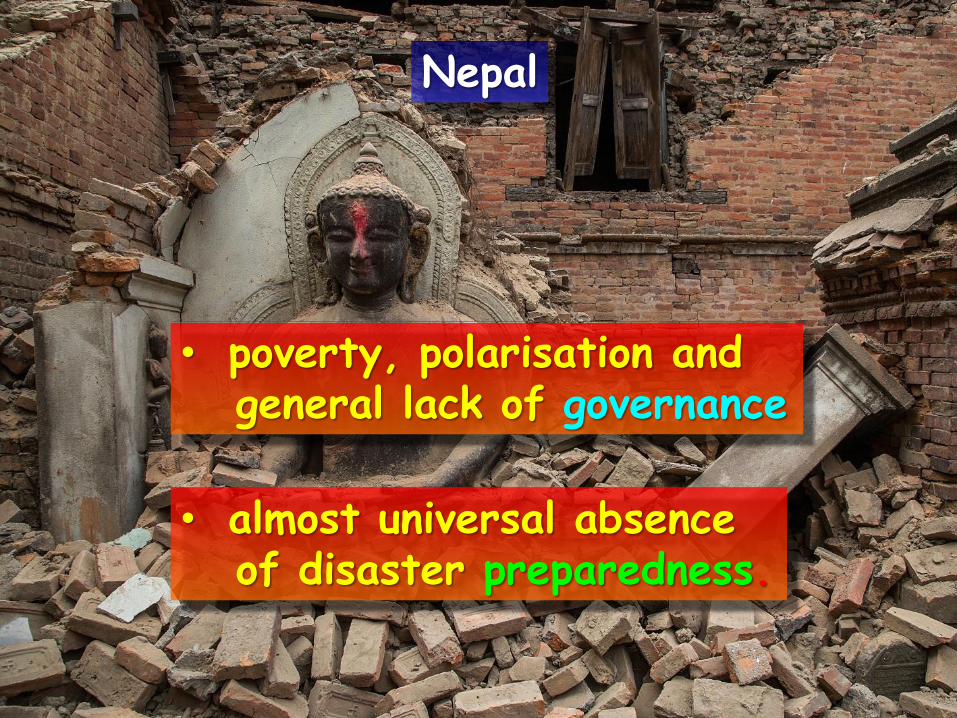
• poverty, polarisation andgeneral lack of governance
• almost universal absenceof disaster preparedness.
Nepal

• municipal disaster managementarrangements adequate for a villageof 1,000-2,000 inhabitants, nota metropolitan area of 1.6 million
• airport far too small (cf. Haiti)
• basic preparedness virtually absent
• international community ineffective
• disaster risk reductionmeasures very recent.
Kathmandu
• Why does disaster risk reduction havesuch a low priority in national agendas?
• Why does so much internationaleffort achieve so few results?
• Why does the international communityfocus on sophisticated aimsand ignore basic preparedness?
• What is the point of the SendaiFramework for Disaster Risk Reductionif it fails to reach the local level?
• Why is it so difficult to achievepositive cultural change?.
Basic preparedness is a matter ofcommitting and organising the resources
that already exist: it is not unaffordable.
The barriers to preparedness:• perception and interests of
powerful decision-makers• corruption (the real cause
of earthquake disasters)• polarisation, ideology and dogma• lack of accountability:
"simulated ignorance".
david.alexander@ucl.ac.ukemergency-planning.blogspot.comPresentations can be downloaded from:-
www.slideshare.com/dealexander
Thank youfor yourattention!