Embed Size (px)
Citation preview

LIVER TRAUMA
Dr. D.K.SharmaM.S., MCh. (GI Surgery)Prof. & Head, Deptt. Of SurgeryRNT Medical College, Udaipur, Raj.

Synopsis

Epidemiology Relevant Anatomy Pathophysiology
Mechanisms of Injury Grades of Liver Trauma
Clinical Features Investigations Treatment Important Concepts
DPL FAST / eFAST ALTS DCS Death Triangle Total Vascular Exclusion

Epidemiology

Associations
Isolated liver injury occurs in less than 50% of patients.
Blunt trauma 45% with spleen
Rib fracture 33% with Liver injury
Bowel injuries
Pancreatic Injuries
Gall Bladder & Bile Duct Injuries Rare
Contusions, avulsions, lacerations or perforations.

Relevant Anatomy

Pathophysiology

Why the liver…
Large organ
Friable parenchyma, thin capsule, fixed position in relation to spine prone to blunt injury
Wide bore, thin walled blood vessels with high blood flow Excessive blood loss
Right lobe larger, closer to ribs more injury
In children:
compliant ribs
transmitted force

Mild injuries heal in 3 months.
Moderate injuries heal in 6 months.
Severe injuries in 9-15 months.
Healing

Classification & Grading

Grade VI Hepatic Avulsion


Clinical Features

Blood Loss Peritonism Symptoms Abdominal Pain Radiation to shoulder Altered Sensoium
Signs Hypotension RUQ tenderness, and guarding Generalized Peritonism
Hemoperitoneum Biliary Peritonitis
Delayed – Intra-abdominal abscess

Investigations

Labs & Radiology
Hematologic
Elevated LFTs
DPL -- high sensitivity
CT scan is the diagnostic procedure of choice.
USG
MRI ??
Diagnostic Laparoscopy

USG
FAST
eFAST

Angiography
Active bleeding
Transcatheter embolization
Embolization & stenting for fistulas.

CT Scan
Localization.
Monitor healing.
Grades 1-6

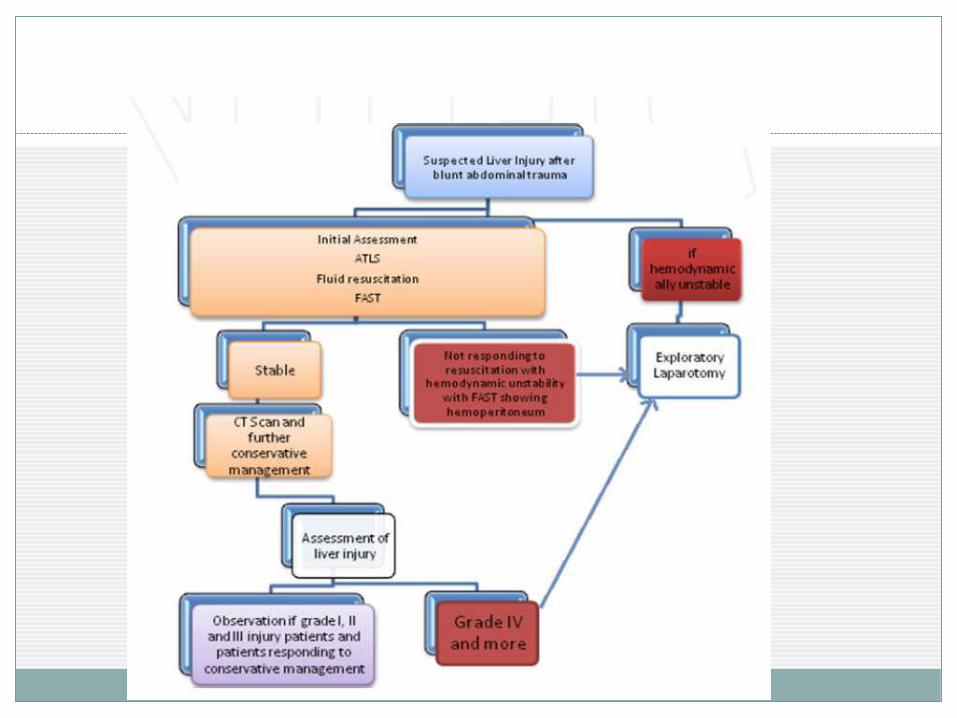
Management

Management
In the Past vs Now treatment of blunt liver trauma Stopped bleeding at Laparotomy- 86% Non-therapeutic explorations- 67% Conservative Management-
Adults-80% Children-97%
Reasons MDCT TAE Liver regenerative capacity Improved Critical Care
Operative / Non-Operative CT scan diagnosis and follow up

Remember associated injuries Spleen
Pancreas
Bowel
Resuscitate
Consider Cryoprecipitate, FFP
Assessment of injury Spiral CT
Laparotomy
♦ Treatment♦ OM
♦ NOM
Management

Damage Control Surgery Perihepatic packing Hepatorrhaphy Mesh Wrapping
Enough Tension Anchoring
Hepatotomy & Selective Vascular Ligation Resection
Non-anatomical Anatomical
Intrahepatic Balloon Tamponade Total Vascular exclusion Liver Transplantation

Post-Operative Complications
Hemorrhage Correct coagulopathy
TAE
Operative Control
Remove perihepatic packing bet 36-72 h
Sepsis & Abscess Percutaneous drainage
Surgical Drainage
Biliary Complications Biloma
Biliary Ascites
Biliary Fistulae

ATLS
Advanced Trauma Life Support
Aggressive fluid resuscitation
CVP
UO Monitoring
Avoidance of “Death Triangle”
Hypothermia
Coagulopathy
Acidosis

Damage Control Surgery
Stone (1980); Univ. of Pennsylvania (1983)
To avoid or deal with Danger Triad
Early recognition
Already at physiologic limit
Concepts & Sequence
Control of Hemorrhage & Contamination
Temporary closure & Return to ICU
Deal with the Triad
Return to OT Definitive repair

Death Triangle
Danger Triad; Bloody Vicious Cycle
Components
Hypothermia
Decreasing Temp
<34 C
Coagulopathy
Non-surgical Oozing
PT > 50% of normal
Acidosis
<7.2 despite adequate volume resuscitation

surgeryclasses.blogspot.in

Thank you

![Liver trauma: WSES position paper · 2017. 8. 25. · The liver is the most injured organ in abdominal trauma [1–3]. Road traffic crashes and antisocial, violent behavior account](https://img.pdfslide.net/doc/110x75/61197537f2aa24014c356d17/liver-trauma-wses-position-paper-2017-8-25-the-liver-is-the-most-injured-organ.jpg)











