
lable at ScienceDirect
The American Journal of Surgery 214 (2017) 811e819
Contents lists avai
The American Journal of Surgery
journal homepage: www.americanjournalofsurgery.com
Distal scar-to-midline distance in pilonidal Limberg flap surgery is arecurrence-promoting factor: A multicenter, case-control study
Mehmet Kaplan, M.D. a, *, Onder Ozcan, M.D. b, Ethem Bilgic, M.D. c,Elif Tugce Kaplan, M.S. d, Tugba Kaplan, MS. e, Fatma Cigdem Kaplan, M.D f
a Department of General Surgery, Bahcesehir University (BAU) School of Medicine, _Istanbul, Turkeyb Department of General Surgery, Sitki Kocman University School of Medicine, Mugla, Turkeyc Department of General Surgery, Karasu Government Hospital, Sakarya, Turkeyd MP Research Program, Kemerburgaz University Medical School, Istanbul, Turkeye GAZU Research Program, Gaziantep University Medical School, Gaziantep, Turkeyf 25-Aralik Health Center, Ministry of Health Republic of Turkey, Gaziantep, Turkey
a r t i c l e i n f o
Article history:Received 1 January 2017Received in revised form3 February 2017Accepted 5 February 2017
Keywords:Sacrococcygeal pilonidal sinusOff-midline closureLimberg flapModified LimbergPilonidal diseaseRecurrence
* Corresponding author. Medical Park GazianteDepartmani, 27100, Gaziantep, Turkey.
E-mail addresses: [email protected], me(M. Kaplan).
http://dx.doi.org/10.1016/j.amjsurg.2017.02.0080002-9610/© 2017 Elsevier Inc. All rights reserved.
a b s t r a c t
Background: The Limberg flap (LF) procedure is widely performed for the treatment of sacrococcygealpilonidal sinus (SPS); however, recurrences continues to be observed. The aim of this study was to assessthe relationship between LF designs and the risk of SPS recurrence.Methods: Sixty-one cases with recurrent disease (study group) and 194 controls, with a minimum of 5recurrence-free years following surgery (control group), were included in the study. LF reconstructionsperformed in each group were classified as off-midline closure (OMC) and non-OMC types. Subsequently,the 2 groups were analyzed.Results: After adjustment for all variables, non-OMC types showed the most prominent correlation withrecurrence, followed by interrupted suturing type, family history of SPS, smoking, prolonged healingtime, and younger age. The best cut-off value for the critical distance from the midline was found to be11 mm (with 72% sensitivity and 95% specificity for recurrence).Conclusions: We recommend OMC modifications, with the flap tailored to create a safe margin of at least2 cm between the flap borders and the midline.
© 2017 Elsevier Inc. All rights reserved.
1. Introduction
Sacrococcygeal pilonidal sinus (SPS) is a common disorder, withan estimated incidence of 1.1% in the community and 9% in soldiersin Turkey.1 Pilonidal disease results from the interplay between hairtype, force, and vulnerability of the skin2 and from hair follicleobstruction and enlargement,3 the process of which often becomesactive during the vulnerable phase at the beginning ofadolescence.4
Despite plentiful research and a substantial number of publi-cations, no clear consensus regarding the gold-standard treatmentmodality for SPS has been established. However, off-midline
p Hospital, Genel Cerrahi
closure (OMC) techniques, such as the Bascom procedure, Kar-ydakis flap, asymmetric Z-plasty, asymmetric V-Yadvancement flapand the Limberg transposition flap have become popular for thetreatment of SPS.5e7 In all such procedures, the suture line ispositioned off the midline to ensure uncomplicated healing and aminimal likelihood of recurrence.5,6
One of these techniques, the Limberg flap (LF), is widely per-formed as a primary surgical treatment for SPS in Turkey8e13 withthe suggestion that the LF procedure results in better outcomesthan other techniques.9e11 Nevertheless, recurrences may beobserved despite wide excision and flap transposition12,13; there-fore, successful implementation of the LF technique in the sacro-coccygeal area requires thorough understanding of both flapcharacteristics and the challenging anatomy of the gluteal cleft.
Despite originally performing the LF procedure for SPS patientswith acceptable results until 2008, we have recently shifted sur-gical preference to an alternative OMC technique, Bascom proced-ure, for cosmetic reasons. However, an increasing number of cases

M. Kaplan et al. / The American Journal of Surgery 214 (2017) 811e819812
have been admitted to our institution following complications orrecurrence after LF procedures performed elsewhere.
Although some modifications of LF have already been suggestedto avoid recurrence,9e11 its use has never been proven to be justi-fied. Therefore, we investigated the distal scar-to-midline distanceand other technical factors that are risk factors associated withrecurrence and hypothesized that modifications that increase thescar-to-midline distance, especially on the caudal side, wouldreduce the recurrence rates in patients who underwent LF recon-struction for primary SPS.
2. Materials and methods
2.1. Study design and setting
A multicenter, hospital-based, case-control study was designedto evaluate relationships between LF designs to the risk of SPSrecurrence. Sixty and one cases with clinically confirmed recur-rence of SPS following LF surgery (study group, SG), and 194 con-trols without recurrence who underwent the same surgery (controlgroup, CG) were recruited into the study.
The study was undertaken at the General Surgery Departmentsof Medical Park Gaziantep Hospital, Mugla Sitki Kocman UniversityHospital and Karasu Government Hospital in Turkey under the di-rection of a principal investigator (MK). In this way patients werecollected from different parts of the country with the aim of rep-resenting the general population.
The study was reviewed and approved by the review board ofeach center, and was registered at ClinicalTrials.gov(NCT02663466). All procedures and study protocols were under-taken in accordance with the Declaration of Helsinki. Patientswilling to participate in the trial received both verbal and writteninformation at the time of recruitment via the outpatient clinic.
2.2. Data collection
Each hospital database was searched separately using Turkishnational procedural classification codes, with 528 patients whoreceived LF surgery identified. After initial assessment of eligibilityand excluding individuals who did not meet the inclusion criteria, atotal of 255 patients who were willing to participate in the studywere included. All patients were examined in each study center,and high-resolution close-up photos of the patients' sacrococcygealarea were taken. These photos were distributed to all authors forassessment, with a collective decision reached regarding the cate-gorization of the OMC technique used. Furthermore, the distancebetween the flap border and cleft midline was precisely measured.Following completion of assessments, all digitalized patient datawas permanently deleted.
Using a prearranged questionnaire, patients were interviewedin a face-to-face manner. Patient demographics, clinical character-istics, operative and postoperative data were obtained from eachinstitution's database and patient interviews separately, andcollected into a single study database pool.
2.3. Participants
After the initial assessment of eligibility (n ¼ 528) at recruit-ment centers, 187 patients who did not meet the inclusion criteriawere excluded and the potential participants were invited to un-dergo detailed examination. After exclusion of another 86 patientswho were unavailable, the remaining 255 well-documented pa-tients were included in the study population, with 61 patients inthe SG, and 194 patients in the CG. Flow of participants through thecase-control study is illustrated in Fig. 1 and the distribution of
patients according to the participating centers is shown in Table 1.
2.3.1. Study groupThe study was initiated in July 2014. Since that time until the
date of the study was completed in December 2015, all recurrentcases, whether underwent LF surgery for primary SPS in trial cen-ters or elsewhere, were enrolled into the SG and their data wereprospectively maintained. Patients were excluded if they wereyounger than 16-years-old, had a clinical history of multiplerecurrence, recurrence due to reasons other than closure technique(such as traumatic injury, newly diagnosed sinus openings outsidethe surgical area etc.), those with diabetes mellitus or using ste-roids, skin disorders such as hidradenitis suppurativa, previousphenol treatment, or patients for whom a legal representativerefused to give informed consent for interview or studyparticipation.
2.3.2. Control groupControls were selected from patients who underwent LF surgery
for primary SPS between January 2008 and July 2014. The two in-clusion criteria were absence of recurrence and having beenfollowed-up at least 5 years. Because majority of recurrence occurduring this postoperative interval,14 we excluded patients who didnot complete 5 years interval after surgery. Other exclusion criteriawere the same as in the SG.
2.3.3. Number of controls per caseOriginally, we aimed to select at least five controls for every case
in the population who had no recurrence of the disease (n ¼ 439).However, after excluding individuals who did not meet the inclu-sion criteria (i.e. patients with incomplete follow-up time, n ¼ 153;or no available photographic documentation, n ¼ 9) and afterexcluding patients who could not be reached (n¼ 64) or declined inparticipate in the study (n ¼ 11) or were not included in the studyfor other reasons (n ¼ 8), only three non-recurrent controls whomet all the inclusion criteria could be identified for each recurrentcase.
2.4. Variables
The primary outcome evaluated was the difference in the fre-quency of OMC and non-OMC LF closure types between the SG andCG. Secondary outcomes included critical distance, age, sex, BMI,family history, body hair status, duration of symptoms, suturingmethod, anesthesia type, drain usage, initial healing time. All var-iables were compared between the recurrent cases and non-recurrent controls.
Recurrence-prone area, critical distance, and a typical LF designare illustrated in Fig. 2A and B. The Limberg flap procedure con-sisted of the excision of the involved area down to the presacralfascia by means of a rhombus-shaped incision, which is usually anequilateral parallelogram with internal acute and obtuse angles2 � 60� and 2 � 120�, respectively. Next, a rhomboid flap ismobilized full-thickness down to the gluteal fascia and transposedto close the defect. Depending on the preference of the surgeon,methylene blue injection may have been used to delineate sinustracts at the beginning of the procedure. However, because theavailable data in the records were not sufficient, methylene blueusage could not be measured as a variable. Recurrence was definedclinically as the presence of symptoms and findings of acute ab-scess, or moisture and minimal to copious drainage and occasionalbleeding from one or more openings which often hairs singly or intufts lies within, or a larger granulation-filled slit opening intocavity at the intersection of the previous suture line and midline ofthe buttocks, with/without a secondary opening usually lie cranial
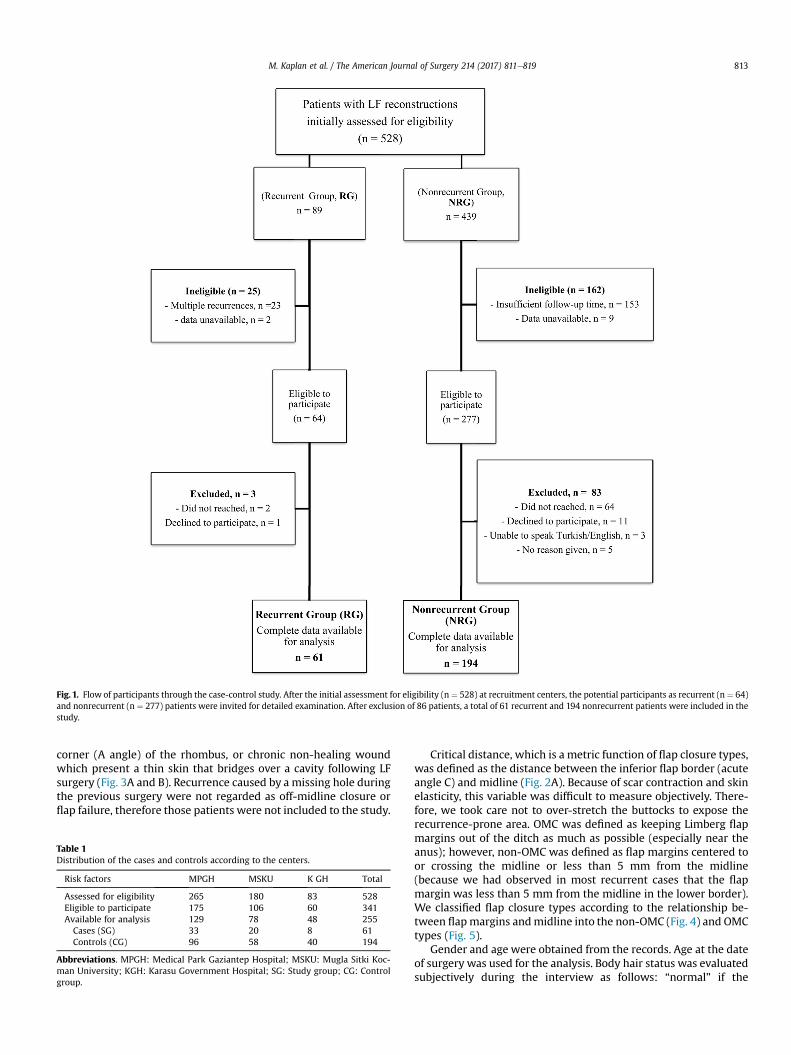
Fig. 1. Flow of participants through the case-control study. After the initial assessment for eligibility (n ¼ 528) at recruitment centers, the potential participants as recurrent (n ¼ 64)and nonrecurrent (n ¼ 277) patients were invited for detailed examination. After exclusion of 86 patients, a total of 61 recurrent and 194 nonrecurrent patients were included in thestudy.
M. Kaplan et al. / The American Journal of Surgery 214 (2017) 811e819 813
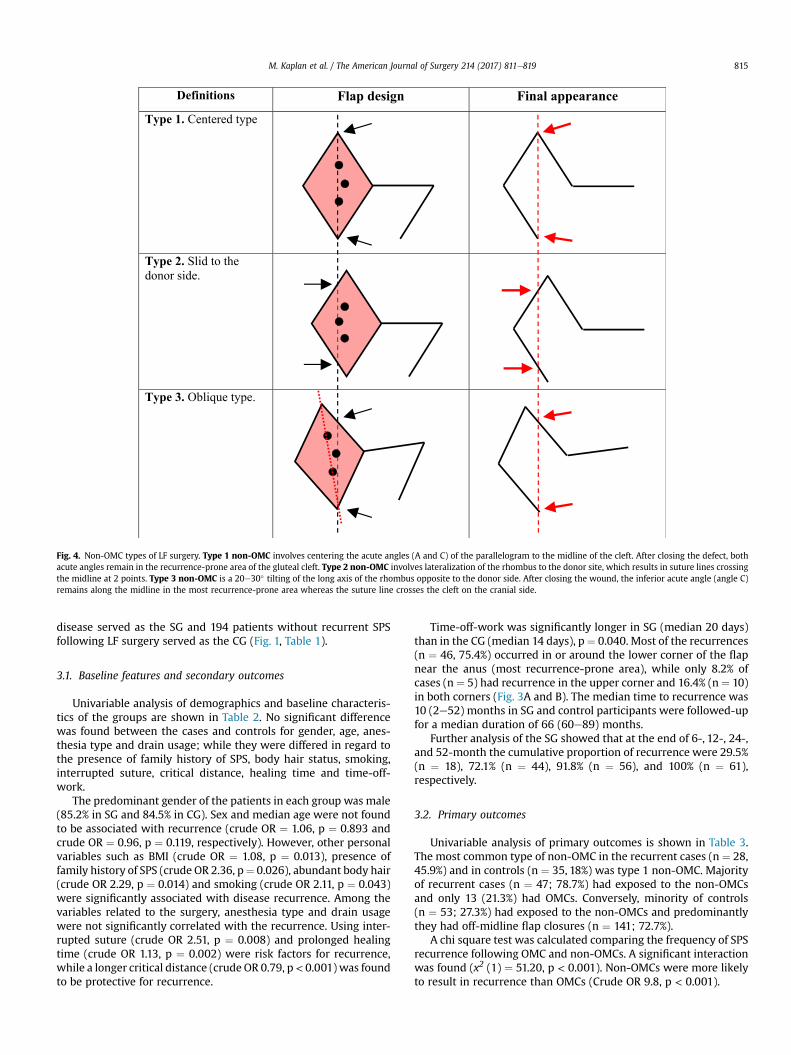
corner (A angle) of the rhombus, or chronic non-healing woundwhich present a thin skin that bridges over a cavity following LFsurgery (Fig. 3A and B). Recurrence caused by a missing hole duringthe previous surgery were not regarded as off-midline closure orflap failure, therefore those patients were not included to the study.
Table 1Distribution of the cases and controls according to the centers.
Risk factors MPGH MSKU K GH Total
Assessed for eligibility 265 180 83 528Eligible to participate 175 106 60 341Available for analysis 129 78 48 255Cases (SG) 33 20 8 61Controls (CG) 96 58 40 194
Abbreviations. MPGH: Medical Park Gaziantep Hospital; MSKU: Mugla Sitki Koc-man University; KGH: Karasu Government Hospital; SG: Study group; CG: Controlgroup.
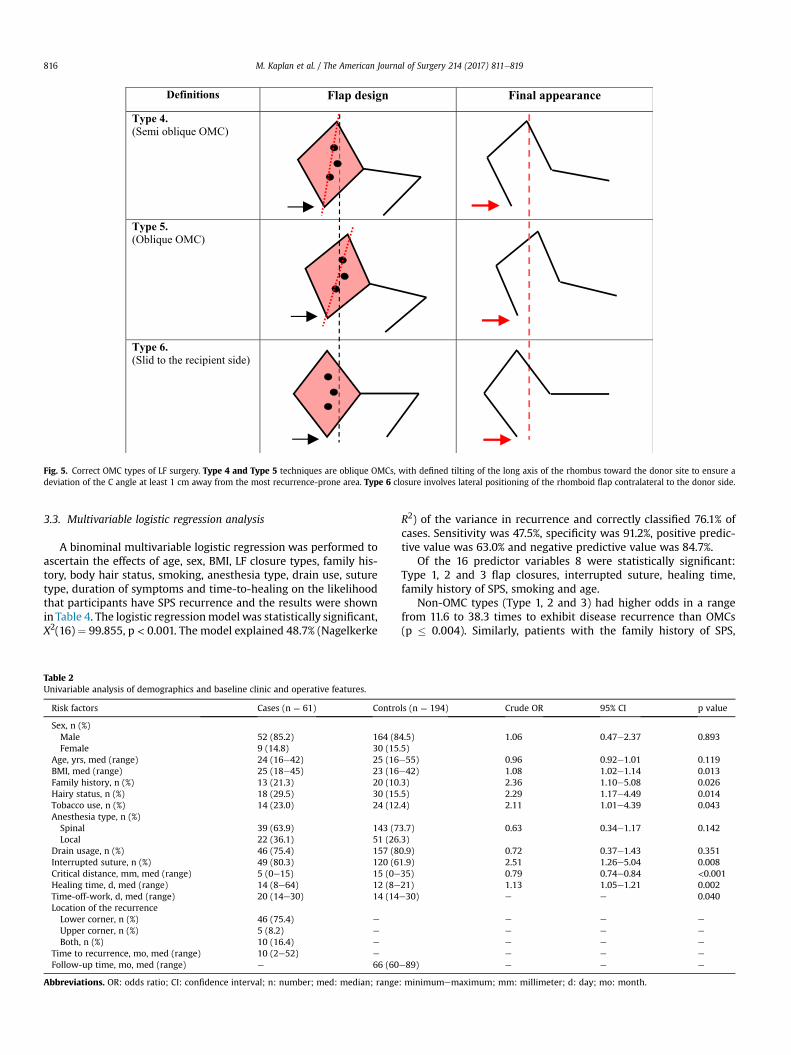
Critical distance, which is a metric function of flap closure types,was defined as the distance between the inferior flap border (acuteangle C) and midline (Fig. 2A). Because of scar contraction and skinelasticity, this variable was difficult to measure objectively. There-fore, we took care not to over-stretch the buttocks to expose therecurrence-prone area. OMC was defined as keeping Limberg flapmargins out of the ditch as much as possible (especially near theanus); however, non-OMC was defined as flap margins centered toor crossing the midline or less than 5 mm from the midline(because we had observed in most recurrent cases that the flapmargin was less than 5 mm from the midline in the lower border).We classified flap closure types according to the relationship be-tween flapmargins andmidline into the non-OMC (Fig. 4) and OMCtypes (Fig. 5).
Gender and age were obtained from the records. Age at the dateof surgery was used for the analysis. Body hair status was evaluatedsubjectively during the interview as follows: “normal” if the
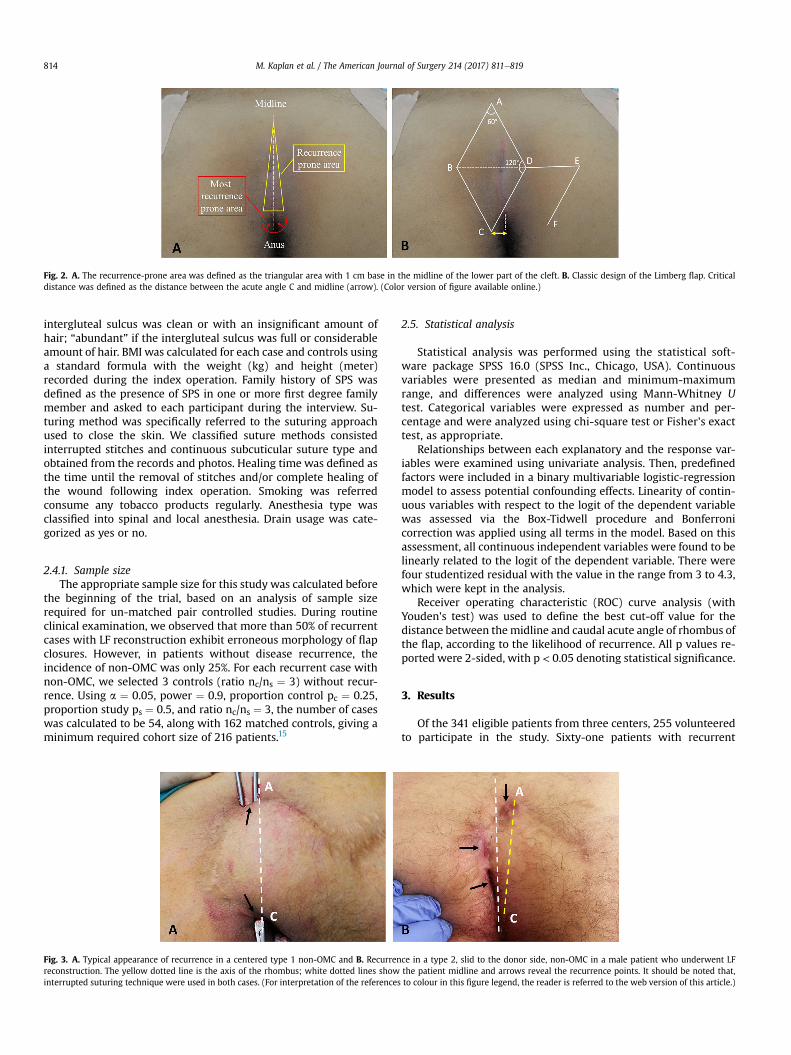
Fig. 2. A. The recurrence-prone area was defined as the triangular area with 1 cm base in the midline of the lower part of the cleft. B. Classic design of the Limberg flap. Criticaldistance was defined as the distance between the acute angle C and midline (arrow). (Color version of figure available online.)
M. Kaplan et al. / The American Journal of Surgery 214 (2017) 811e819814
intergluteal sulcus was clean or with an insignificant amount ofhair; “abundant” if the intergluteal sulcus was full or considerableamount of hair. BMI was calculated for each case and controls usinga standard formula with the weight (kg) and height (meter)recorded during the index operation. Family history of SPS wasdefined as the presence of SPS in one or more first degree familymember and asked to each participant during the interview. Su-turing method was specifically referred to the suturing approachused to close the skin. We classified suture methods consistedinterrupted stitches and continuous subcuticular suture type andobtained from the records and photos. Healing time was defined asthe time until the removal of stitches and/or complete healing ofthe wound following index operation. Smoking was referredconsume any tobacco products regularly. Anesthesia type wasclassified into spinal and local anesthesia. Drain usage was cate-gorized as yes or no.
2.4.1. Sample sizeThe appropriate sample size for this study was calculated before
the beginning of the trial, based on an analysis of sample sizerequired for un-matched pair controlled studies. During routineclinical examination, we observed that more than 50% of recurrentcases with LF reconstruction exhibit erroneous morphology of flapclosures. However, in patients without disease recurrence, theincidence of non-OMC was only 25%. For each recurrent case withnon-OMC, we selected 3 controls (ratio nc/ns ¼ 3) without recur-rence. Using a ¼ 0.05, power ¼ 0.9, proportion control pc ¼ 0.25,proportion study ps ¼ 0.5, and ratio nc/ns ¼ 3, the number of caseswas calculated to be 54, along with 162 matched controls, giving aminimum required cohort size of 216 patients.15
Fig. 3. A. Typical appearance of recurrence in a centered type 1 non-OMC and B. Recurrenreconstruction. The yellow dotted line is the axis of the rhombus; white dotted lines showinterrupted suturing technique were used in both cases. (For interpretation of the references
2.5. Statistical analysis
Statistical analysis was performed using the statistical soft-ware package SPSS 16.0 (SPSS Inc., Chicago, USA). Continuousvariables were presented as median and minimum-maximumrange, and differences were analyzed using Mann-Whitney Utest. Categorical variables were expressed as number and per-centage and were analyzed using chi-square test or Fisher's exacttest, as appropriate.
Relationships between each explanatory and the response var-iables were examined using univariate analysis. Then, predefinedfactors were included in a binary multivariable logistic-regressionmodel to assess potential confounding effects. Linearity of contin-uous variables with respect to the logit of the dependent variablewas assessed via the Box-Tidwell procedure and Bonferronicorrection was applied using all terms in the model. Based on thisassessment, all continuous independent variables were found to belinearly related to the logit of the dependent variable. There werefour studentized residual with the value in the range from 3 to 4.3,which were kept in the analysis.
Receiver operating characteristic (ROC) curve analysis (withYouden's test) was used to define the best cut-off value for thedistance between themidline and caudal acute angle of rhombus ofthe flap, according to the likelihood of recurrence. All p values re-ported were 2-sided, with p < 0.05 denoting statistical significance.
3. Results
Of the 341 eligible patients from three centers, 255 volunteeredto participate in the study. Sixty-one patients with recurrent
ce in a type 2, slid to the donor side, non-OMC in a male patient who underwent LFthe patient midline and arrows reveal the recurrence points. It should be noted that,to colour in this figure legend, the reader is referred to the web version of this article.)
Definitions Flap design Final appearance
Type 1. Centered type
Type 2. Slid to the donor side.
Type 3. Oblique type.
Fig. 4. Non-OMC types of LF surgery. Type 1 non-OMC involves centering the acute angles (A and C) of the parallelogram to the midline of the cleft. After closing the defect, bothacute angles remain in the recurrence-prone area of the gluteal cleft. Type 2 non-OMC involves lateralization of the rhombus to the donor site, which results in suture lines crossingthe midline at 2 points. Type 3 non-OMC is a 20e30� tilting of the long axis of the rhombus opposite to the donor side. After closing the wound, the inferior acute angle (angle C)remains along the midline in the most recurrence-prone area whereas the suture line crosses the cleft on the cranial side.
M. Kaplan et al. / The American Journal of Surgery 214 (2017) 811e819 815
disease served as the SG and 194 patients without recurrent SPSfollowing LF surgery served as the CG (Fig. 1, Table 1).
3.1. Baseline features and secondary outcomes
Univariable analysis of demographics and baseline characteris-tics of the groups are shown in Table 2. No significant differencewas found between the cases and controls for gender, age, anes-thesia type and drain usage; while they were differed in regard tothe presence of family history of SPS, body hair status, smoking,interrupted suture, critical distance, healing time and time-off-work.
The predominant gender of the patients in each group was male(85.2% in SG and 84.5% in CG). Sex and median age were not foundto be associated with recurrence (crude OR ¼ 1.06, p ¼ 0.893 andcrude OR ¼ 0.96, p ¼ 0.119, respectively). However, other personalvariables such as BMI (crude OR ¼ 1.08, p ¼ 0.013), presence offamily history of SPS (crude OR 2.36, p¼ 0.026), abundant body hair(crude OR 2.29, p ¼ 0.014) and smoking (crude OR 2.11, p ¼ 0.043)were significantly associated with disease recurrence. Among thevariables related to the surgery, anesthesia type and drain usagewere not significantly correlated with the recurrence. Using inter-rupted suture (crude OR 2.51, p ¼ 0.008) and prolonged healingtime (crude OR 1.13, p ¼ 0.002) were risk factors for recurrence,while a longer critical distance (crude OR 0.79, p< 0.001) was foundto be protective for recurrence.
Time-off-work was significantly longer in SG (median 20 days)than in the CG (median 14 days), p¼ 0.040. Most of the recurrences(n ¼ 46, 75.4%) occurred in or around the lower corner of the flapnear the anus (most recurrence-prone area), while only 8.2% ofcases (n¼ 5) had recurrence in the upper corner and 16.4% (n¼ 10)in both corners (Fig. 3A and B). The median time to recurrence was10 (2e52) months in SG and control participants were followed-upfor a median duration of 66 (60e89) months.
Further analysis of the SG showed that at the end of 6-, 12-, 24-,and 52-month the cumulative proportion of recurrence were 29.5%(n ¼ 18), 72.1% (n ¼ 44), 91.8% (n ¼ 56), and 100% (n ¼ 61),respectively.
3.2. Primary outcomes
Univariable analysis of primary outcomes is shown in Table 3.The most common type of non-OMC in the recurrent cases (n ¼ 28,45.9%) and in controls (n ¼ 35, 18%) was type 1 non-OMC. Majorityof recurrent cases (n ¼ 47; 78.7%) had exposed to the non-OMCsand only 13 (21.3%) had OMCs. Conversely, minority of controls(n ¼ 53; 27.3%) had exposed to the non-OMCs and predominantlythey had off-midline flap closures (n ¼ 141; 72.7%).
A chi square test was calculated comparing the frequency of SPSrecurrence following OMC and non-OMCs. A significant interactionwas found (x2 (1) ¼ 51.20, p < 0.001). Non-OMCs were more likelyto result in recurrence than OMCs (Crude OR 9.8, p < 0.001).
Definitions Flap design Final appearance
Type 4. (Semi oblique OMC)
Type 5. (Oblique OMC)
Type 6. (Slid to the recipient side)
Fig. 5. Correct OMC types of LF surgery. Type 4 and Type 5 techniques are oblique OMCs, with defined tilting of the long axis of the rhombus toward the donor site to ensure adeviation of the C angle at least 1 cm away from the most recurrence-prone area. Type 6 closure involves lateral positioning of the rhomboid flap contralateral to the donor side.
M. Kaplan et al. / The American Journal of Surgery 214 (2017) 811e819816
3.3. Multivariable logistic regression analysis
A binominal multivariable logistic regression was performed toascertain the effects of age, sex, BMI, LF closure types, family his-tory, body hair status, smoking, anesthesia type, drain use, suturetype, duration of symptoms and time-to-healing on the likelihoodthat participants have SPS recurrence and the results were shownin Table 4. The logistic regressionmodel was statistically significant,X2(16) ¼ 99.855, p < 0.001. The model explained 48.7% (Nagelkerke
Table 2Univariable analysis of demographics and baseline clinic and operative features.
Risk factors Cases (n ¼ 61) Contro
Sex, n (%)Male 52 (85.2) 164 (8Female 9 (14.8) 30 (15
Age, yrs, med (range) 24 (16e42) 25 (16BMI, med (range) 25 (18e45) 23 (16Family history, n (%) 13 (21.3) 20 (10Hairy status, n (%) 18 (29.5) 30 (15Tobacco use, n (%) 14 (23.0) 24 (12Anesthesia type, n (%)Spinal 39 (63.9) 143 (7Local 22 (36.1) 51 (26
Drain usage, n (%) 46 (75.4) 157 (8Interrupted suture, n (%) 49 (80.3) 120 (6Critical distance, mm, med (range) 5 (0e15) 15 (0eHealing time, d, med (range) 14 (8e64) 12 (8eTime-off-work, d, med (range) 20 (14e30) 14 (14Location of the recurrenceLower corner, n (%) 46 (75.4) e
Upper corner, n (%) 5 (8.2) e
Both, n (%) 10 (16.4) e
Time to recurrence, mo, med (range) 10 (2e52) e
Follow-up time, mo, med (range) e 66 (60
Abbreviations. OR: odds ratio; CI: confidence interval; n: number; med: median; range
R2) of the variance in recurrence and correctly classified 76.1% ofcases. Sensitivity was 47.5%, specificity was 91.2%, positive predic-tive value was 63.0% and negative predictive value was 84.7%.
Of the 16 predictor variables 8 were statistically significant:Type 1, 2 and 3 flap closures, interrupted suture, healing time,family history of SPS, smoking and age.
Non-OMC types (Type 1, 2 and 3) had higher odds in a rangefrom 11.6 to 38.3 times to exhibit disease recurrence than OMCs(p � 0.004). Similarly, patients with the family history of SPS,
ls (n ¼ 194) Crude OR 95% CI p value
4.5) 1.06 0.47e2.37 0.893.5)e55) 0.96 0.92e1.01 0.119e42) 1.08 1.02e1.14 0.013.3) 2.36 1.10e5.08 0.026.5) 2.29 1.17e4.49 0.014.4) 2.11 1.01e4.39 0.043
3.7) 0.63 0.34e1.17 0.142.3)0.9) 0.72 0.37e1.43 0.3511.9) 2.51 1.26e5.04 0.00835) 0.79 0.74e0.84 <0.00121) 1.13 1.05e1.21 0.002e30) e e 0.040
e e e
e e e
e e e
e e e
e89) e e e
: minimumemaximum; mm: millimeter; d: day; mo: month.
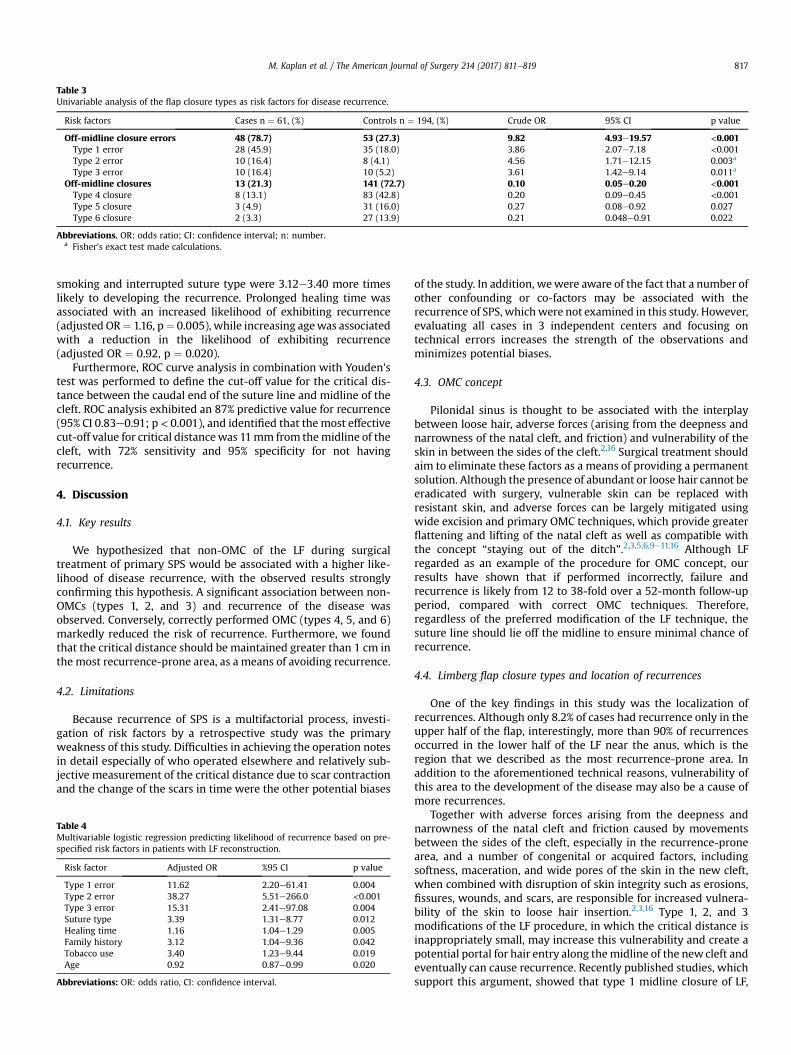
Table 3Univariable analysis of the flap closure types as risk factors for disease recurrence.
Risk factors Cases n ¼ 61, (%) Controls n ¼ 194, (%) Crude OR 95% CI p value
Off-midline closure errors 48 (78.7) 53 (27.3) 9.82 4.93e19.57 <0.001Type 1 error 28 (45.9) 35 (18.0) 3.86 2.07e7.18 <0.001Type 2 error 10 (16.4) 8 (4.1) 4.56 1.71e12.15 0.003a
Type 3 error 10 (16.4) 10 (5.2) 3.61 1.42e9.14 0.011a
Off-midline closures 13 (21.3) 141 (72.7) 0.10 0.05e0.20 <0.001Type 4 closure 8 (13.1) 83 (42.8) 0.20 0.09e0.45 <0.001Type 5 closure 3 (4.9) 31 (16.0) 0.27 0.08e0.92 0.027Type 6 closure 2 (3.3) 27 (13.9) 0.21 0.048e0.91 0.022
Abbreviations. OR: odds ratio; CI: confidence interval; n: number.a Fisher's exact test made calculations.
M. Kaplan et al. / The American Journal of Surgery 214 (2017) 811e819 817
smoking and interrupted suture type were 3.12e3.40 more timeslikely to developing the recurrence. Prolonged healing time wasassociated with an increased likelihood of exhibiting recurrence(adjusted OR¼ 1.16, p¼ 0.005), while increasing agewas associatedwith a reduction in the likelihood of exhibiting recurrence(adjusted OR ¼ 0.92, p ¼ 0.020).
Furthermore, ROC curve analysis in combination with Youden'stest was performed to define the cut-off value for the critical dis-tance between the caudal end of the suture line and midline of thecleft. ROC analysis exhibited an 87% predictive value for recurrence(95% CI 0.83e0.91; p < 0.001), and identified that the most effectivecut-off value for critical distancewas 11mm from themidline of thecleft, with 72% sensitivity and 95% specificity for not havingrecurrence.
4. Discussion
4.1. Key results
We hypothesized that non-OMC of the LF during surgicaltreatment of primary SPS would be associated with a higher like-lihood of disease recurrence, with the observed results stronglyconfirming this hypothesis. A significant association between non-OMCs (types 1, 2, and 3) and recurrence of the disease wasobserved. Conversely, correctly performed OMC (types 4, 5, and 6)markedly reduced the risk of recurrence. Furthermore, we foundthat the critical distance should be maintained greater than 1 cm inthe most recurrence-prone area, as a means of avoiding recurrence.
4.2. Limitations
Because recurrence of SPS is a multifactorial process, investi-gation of risk factors by a retrospective study was the primaryweakness of this study. Difficulties in achieving the operation notesin detail especially of who operated elsewhere and relatively sub-jective measurement of the critical distance due to scar contractionand the change of the scars in time were the other potential biases
Table 4Multivariable logistic regression predicting likelihood of recurrence based on pre-specified risk factors in patients with LF reconstruction.
Risk factor Adjusted OR %95 CI p value
Type 1 error 11.62 2.20e61.41 0.004Type 2 error 38.27 5.51e266.0 <0.001Type 3 error 15.31 2.41e97.08 0.004Suture type 3.39 1.31e8.77 0.012Healing time 1.16 1.04e1.29 0.005Family history 3.12 1.04e9.36 0.042Tobacco use 3.40 1.23e9.44 0.019Age 0.92 0.87e0.99 0.020
Abbreviations: OR: odds ratio, CI: confidence interval.
of the study. In addition, wewere aware of the fact that a number ofother confounding or co-factors may be associated with therecurrence of SPS, whichwere not examined in this study. However,evaluating all cases in 3 independent centers and focusing ontechnical errors increases the strength of the observations andminimizes potential biases.
4.3. OMC concept
Pilonidal sinus is thought to be associated with the interplaybetween loose hair, adverse forces (arising from the deepness andnarrowness of the natal cleft, and friction) and vulnerability of theskin in between the sides of the cleft.2,16 Surgical treatment shouldaim to eliminate these factors as a means of providing a permanentsolution. Although the presence of abundant or loose hair cannot beeradicated with surgery, vulnerable skin can be replaced withresistant skin, and adverse forces can be largely mitigated usingwide excision and primary OMC techniques, which provide greaterflattening and lifting of the natal cleft as well as compatible withthe concept “staying out of the ditch”.2,3,5,6,9e11,16 Although LFregarded as an example of the procedure for OMC concept, ourresults have shown that if performed incorrectly, failure andrecurrence is likely from 12 to 38-fold over a 52-month follow-upperiod, compared with correct OMC techniques. Therefore,regardless of the preferred modification of the LF technique, thesuture line should lie off the midline to ensure minimal chance ofrecurrence.
4.4. Limberg flap closure types and location of recurrences
One of the key findings in this study was the localization ofrecurrences. Although only 8.2% of cases had recurrence only in theupper half of the flap, interestingly, more than 90% of recurrencesoccurred in the lower half of the LF near the anus, which is theregion that we described as the most recurrence-prone area. Inaddition to the aforementioned technical reasons, vulnerability ofthis area to the development of the disease may also be a cause ofmore recurrences.
Together with adverse forces arising from the deepness andnarrowness of the natal cleft and friction caused by movementsbetween the sides of the cleft, especially in the recurrence-pronearea, and a number of congenital or acquired factors, includingsoftness, maceration, and wide pores of the skin in the new cleft,when combined with disruption of skin integrity such as erosions,fissures, wounds, and scars, are responsible for increased vulnera-bility of the skin to loose hair insertion.2,3,16 Type 1, 2, and 3modifications of the LF procedure, in which the critical distance isinappropriately small, may increase this vulnerability and create apotential portal for hair entry along themidline of the newcleft andeventually can cause recurrence. Recently published studies, whichsupport this argument, showed that type 1 midline closure of LF,

M. Kaplan et al. / The American Journal of Surgery 214 (2017) 811e819818
themost frequently performed non-OMC type in our series (64%), isassociated with 6% recurrence rate even in a very short medianfollow-up of 24e33 month.12,13
On the other hand, among the correct OMC types, type 4was themost frequently performed off-midline LF closure modificationwith up to 56% in this series. This modification (Fig. 5), which in-volves particularly the inferior acute angle of the rhombus, hasbeen implemented by some authors with a significant reduction inearly recurrence noted.9e12 Although most of their studies wereretrospective with relatively small sample size and short follow-upperiods, they supported our hypothesis.
4.5. Critical distance
Critical distance can be viewed as a measure of whether theoperation has been performed in accordance with the OMCconcept. We found a cut-off value of 11 mm for the ‘critical dis-tance’, using ROC analysis, as satisfactorily safe for the prevention ofrecurrence. To our best knowledge, this is the first attempt in theliterature to measure the distance between LF border and midlineto accurately guide the surgeon in deciding the best flap design andavoiding risk of recurrence.
In contrast to openwounds, there are insufficient data regardingthe contraction rate of primarily closed linear wounds. It is statedthat any linear incisional scarmade in a single plane, nomatter howold, is the same length as it was when it was first made; however,linear scars in certain multi-planar sites (such as the sacrococcygealarea) produce webbing and therefore appear to contract.17 There-fore, the critical distance at the time of surgerymay be needed to bemuch larger than 11 mm, because postoperative scar contraction aswell as the healing process may shorten the distance from the scarto the midline. Although there is no objective evidence of how longthis distance should be, we believe that a critical distance of at least2 cm would be more ideal considering the shortening that mayoccur over time.
However, it is possible that this cut-off valuemay vary accordingto the other OMC procedure implemented, as each procedure variesin technical specifications. Therefore, further research is required inorder to determine minimum safe values for each OMC techniquein SPS surgery.
4.6. Secondary outcomes
Study results showed that 21.3% of recurrent cases had exposedto correct OMC procedures, whereas 27.3% of non-recurrent con-trols had exposed to non-OMC procedures during the study inter-val. This indicated that some individual and/or environmentalfactors, other than the type of LF closure, must play a role in therecurrence process as co-factors.
4.6.1. Family history of SPS, abundant hair growth, BMI andyounger age
It has been known that recurrence rate after primary surgery iselevatedwhen family history of SPS is positive.18 Likewise, we founda 3.1-fold higher risk of recurrence in patients with positive familyhistory (p ¼ 0.042). This might be explained partly by geneticanatomic differences found in the posterior raphe and genetic pre-disposition leading vulnerable skin and familial hygienic habits.18
Although two of the commonly known confounder factors,BMI19 and abundant body hair status,2 were significantly differedbetween the SG and CG in univariate analysis, contrary to somepublications, interestingly we could not found a significant rela-tionship between these variables and recurrence after adjusted forall other variables. Because terminal hair development20 andobesity21 are strong hereditary linked traits, it leads to the
conclusion that these two variables are dependent on familyhistory.
Age was found to be inversely related with the recurrence.Because SPS is mostly active at vulnerable phase at the beginning ofadolescence; therefore, the patients who underwent surgery at alater age passed the vulnerable phase and they may exhibit lessrecurrence rate.4
4.6.2. Type of suturing and healing timeWe observed a 3.4-fold increase in recurrence for interrupted
suturing type as an independent factor. This might be due to thefact that using interrupted stitches (usually silk or other multifila-ment sutures) can cause more defects or inversion in suturedwounds or inflamed suture holes in the skin, compared withcontinuous suturing technique.22 Using intradermal continuoussutures for primary closure of sacral defects produce more accurateco-aptation of the skin edges which may help to avoid entrappingthe growing and falling hairs and may also have advantages interms of the cosmetic results and patient satisfaction.23 We havealso observed that as the healing prolonged, recurrence was morelikely. This may be explained by hair piercing easily because theweakness of the new scars.2,3,22 Because LF procedure consists ofwide tissue removal, recurrence due to inadequate excision of sinusopenings during the index operation seems unlikely.
4.6.3. SmokingCigarette smoking is well-known to be associated with an
increased the risk of various postoperative complications24 as wellas is a risk factor for various flap or graft complications.19,25e27 Wefound a 3.4-fold increased relationship between cigarette smokingand recurrence when compared with non-smokers. These adverseeffects of smoking on the postoperative outcome can be partlyexplained by its deleterious effect on both morphological andfunctional aspects of the microcirculation in tissues which mayresult in decreased viability of skin flaps.28
As a result, the process underlying recurrence in cases of SPSappears to be complex and multifactorial. We believe that thecontribution of each factor in the process of recurrence varieswidely in each case, according to the type of surgery performed forSPS. In addition, some factors involved in the etiopathogenesis ofthe disease may not be associated with the recurrence process.
5. Conclusions
In this study, we focused primarily on the importance of non-OMC techniques for recurrence in patients receiving LF re-constructions. Our results indicate that classic LF should no longerbe used; however, if the LF procedure is preferred for the treatmentof SPS, then type 4, 5, and 6 modifications are effective, convenient,and exhibit the best outcomes with respect to recurrence.Furthermore, it is important to tailor the flap to create a safe marginmore than 2 cm between flap borders and the midline, especiallyon the caudal side. Subcuticular continuous sutures, using amonofilament nonabsorbable thread, typically exhibit betterrecurrence outcomes, and should have entrance and exit pointskept away from the midline for best results.
Conflicts of interest and source of funding
None declared.
Authorship
Mehmet Kaplan contributed to conception and design, oracquisition of data, analysis and interpretation of data, drafting the

M. Kaplan et al. / The American Journal of Surgery 214 (2017) 811e819 819
article and revising it critically for important intellectual contentand final approval of the version to be published. Onder Ozcan andEthem Bilgic contributed to design of the study, acquisition of dataand revising the article critically for important intellectual content.Elif Tugce Kaplan, Tugba Kaplan and Fatma Cigdem Kaplancontributed to searching and collecting literature material, acqui-sition of data, analysis and interpretation of data, drafting thearticle.
Category
Benign colorectal disease.
Acknowledgements
We wish to dedicate this article to the memory of a dear friendand teacher, Dr. John Bascom. It was upon his request that thisarticle was conceived, and we are hugely appreciative of the op-portunity to realize his request. He will always be rememberedwith love and gratitude, and his contribution to teaching andtransfer of knowledge will persist with fond thought.
The authors wish to thank to Zeynep Sude Kaplan for hercontribution in the technical artwork of the illustrations.
References
1. Akinci OF, Bozer M, Uzunk€oy A, et al. Incidence and aetiological factors inpilonidal sinus among Turkish soldiers. Eur J Surg. 1999;165:339e342.
2. Karydakis GE. Easy and successful treatment of pilonidal sinus after explana-tion of its causative process. Aust N. Z J Surg. 1992;62:385e389.
3. Bascom J. Pilonidal disease: long-term results of follicle removal. Dis ColonRectum. 1983;26:800e807.
4. Doll D, Friederichs J, Dettmann H, et al. Time and rate of sinus formation inpilonidal sinus disease. Int J Colorectal Dis. 2008;23:359e364.
5. McCallum IJ, King PM, Bruce J. Healing by primary closure versus open healingafter surgery for pilonidal sinus: systematic review and meta-analysis. BMJ.2008;336:868e871.
6. Al-Khamis A, McCallum I, King PM, Bruce J. Healing by primary versus sec-ondary intention after surgical treatment for pilonidal sinus. Cochrane DatabaseSyst Rev. 2010;1:CD006213.
7. Enriquez-Navascues JM, Emparanza JI, Alkorta M, Placer C. Meta-analysis ofrandomized controlled trials comparing different techniques with primaryclosure for chronic pilonidal sinus. Tech Coloproctol. 2014;18:863e872.
8. Guner A, Boz A, Ozkan OF, et al. Limberg flap versus Bascom cleft lift techniquesfor sacrococcygeal pilonidal sinus: prospective, randomized trial. World J Surg.
2013;37:2074e2080.9. Akin M, Leventoglu S, Mentes BB, et al. Comparison of the classic Limberg flap
and modified Limberg flap in the treatment of pilonidal sinus disease: aretrospective analysis of 416 patients. Surg Today. 2010;40:757e762.
10. Cihan A, Mentes BB, Tatlıcıoglu E, et al. Modified Limberg flap reconstructioncompares favourably with primary repair for pilonidal sinus surgery. ANZ JSurg. 2004;74:238e242.
11. Mentes BB, Leventoglu S, Cihan A, et al. Modified Limberg transposition flap forsacrococcygeal pilonidal sinus. Surg Today. 2004;34:419e423.
12. Arslan K, Said Kokcam S, Koksal H, et al. Which flap method should bepreferred for the treatment of pilonidal sinus? A prospective randomizedstudy. Tech Coloproctol. 2014;18:29e37.
13. Sevinc B, Karahan O, Okus A, et al. Randomized prospective comparison ofmidline and off-midline closure techniques in pilonidal sinus surgery. Surgery.2016;159:749e754.
14. Doll D, Krueger CM, Schrank S, et al. Timeline of recurrence after primary andsecondary pilonidal sinus surgery. Dis Colon Rectum. 2007;50:1928e1934.
15. Machin D, Campbell MJ, Fayers PM, Pinol APY. Sample Size Tables for ClinicalStudies. second ed. Oxford, London, Berlin: Blackwell Science Ltd.; 1997.
16. Karydakis GE. New approach to the problem of pilonidal sinus. Lancet. 1973;2:1414e1415.
17. Robbins TH. The confusion of scar contraction. Plast Reconstr Surg. 1978;62:600.18. Doll D, Matevossian E, Wietelmann K, et al. Family history of pilonidal sinus
predisposes to earlier onset of disease and a 50% long-term recurrence rate. DisColon Rectum. 2009;52:1610e1615.
19. Al-Khayat H, Al-Khayat H, Sadeq A, et al. Risk factors for wound complication inpilonidal sinus procedures. J Am Coll Surg. 2007;205:439e444.
20. Shimomura Y, Christiano AM. Biology and genetics of hair. Annu Rev GenomicsHum Genet. 2010;11:109e132.
21. Price RA, Gottesman II . Body fat in identical twins reared apart: roles for genesand environment. Behav Genet. 1991;21:1e7.
22. Marzouk DM, Abou-Zeid AA, Antoniou A, et al. Sinus excision, release of coc-cycutaneous attachments and dermal-subcuticular closure (XRD procedure): anovel technique in flattening the natal cleft in pilonidal sinus treatment. Ann RColl Surg Engl. 2008;90:371e376.
23. Milone M, Musella M, Maietta P, et al. Intradermal absorbable sutures to closepilonidal sinus wounds: a safe closure method? Surg Today. 2014;44:1638e1642.
24. Grønkjær M, Eliasen M, Skov-Ettrup LS, et al. Preoperative smoking status andpostoperative complications: a systematic review and meta-analysis. Ann Surg.2014;259:52e71.
25. Spear SL, Ducic I, Cuoco F, Hannan C. The effect of smoking on flap and donor-site complications in pedicled TRAM breast reconstruction. Plast Reconstr Surg.2005;116:1873e1880.
26. Zimmerman DD, Delemarre JB, Gosselink MP, et al. Smoking affects theoutcome of transanal mucosal advancement flap repair of trans-sphinctericfistulas. Br J Surg. 2003;90:351e354.
27. Goldminz D, Bennett RG. Cigarette smoking and flap and full-thickness graftnecrosis. Arch Dermatol. 1991;127:1012e1015.
28. Lehr HA. Microcirculatory dysfunction induced by cigarette smoking. Micro-circulation. 2000;7:367e384.
Recommended

















