Embed Size (px)
Citation preview

RECONSTRUCTIVE
Improving Outcomes of the Distally BasedHemisoleus Flap: Principles of Angiosomes inFlap Design
Clark F. Schierle, M.D.,Ph.D.
Vinay Rawlani, B.S.Robert D. Galiano, M.D.
John Y. S. Kim, M.D.Gregory A. Dumanian, M.D.
Chicago, Ill.
Background: The reliability of the distally based pedicled hemisoleus flap forcoverage of relatively small medial distal third leg wounds has been continuouslydebated among reconstructive surgeons. Whereas some authors report that thedistally based hemisoleus can be elevated safely, other authors argue that theflap’s retrograde blood supply is problematic. The authors believe that appli-cation of angiosome principles may help surgeons to better design the distallybased hemisoleus flap such that outcomes are optimized.Methods: Seventeen patients received a distally based hemisoleus flap for cov-erage of a small distal third leg wound. Flaps were designed to capture one fullangiosome and only a portion of the adjacent angiosome.Results: Reliable soft-tissue coverage and wound healing were achieved in allpatients. Mean operative time of 130 minutes reflected the relative technicalease and efficiency of the surgery. Only one patient suffered distal tip flapnecrosis, which did not compromise soft-tissue coverage and ultimately resultedin a healed wound and fracture.Conclusions: The distally based hemisoleus flap is an efficacious method oftreating small distal third medial tibial wounds. Flap design based on vascularperforator angiosome principles may help surgeons improve the reliability ofthis flap. (Plast. Reconstr. Surg. 123: 1748, 2009.)
Wounds of the distal third of the leg posea unique challenge for the reconstructivesurgeon. These wounds are usually asso-
ciated with underlying orthopedic fracture, whichoften requires soft-tissue coverage for healing.1Traditional teaching emphasizes the use of freetissue transfer for soft-tissue coverage of the lowerthird of the leg because of the paucity of localsoft-tissue flaps.2–6 Some patients, however, maynot be candidates for free tissue transfer due tomedical comorbidities, and some institutions maynot be equipped for microvascular surgery. Fur-thermore, initial free tissue transfer may be asso-ciated with donor-site morbidity, and often theflap is too bulky for these relatively small defects.7
Refinements in local tissue reconstruction,specifically use of the distally based pedicled hemi-soleus flap, may provide reconstructive surgeonswith another option for treating distal third leg
wounds.7,8 Tobin first advocated the use of thedistally based hemisoleus flap in 1985, and a dia-gram from that article illustrates creating a hugepedicled flap.9 Although refinements in tech-nique were reported,10,11 the flap was never pop-ularized because of concerns over reliability.12,13
Specifically, surgeons cited variability in distal per-forators and retrograde blood supply as reasons toavoid use of the flap. Recently, however, severalauthors have reported successful outcomes usingthe distally based hemisoleus flap for soft-tissuecoverage of distal third leg wounds.14–16 The largestseries of 11 patients has been reported by Pu,16 whoadvocates use of the distally based hemisoleus flap innearly all patients with distal third leg wounds lessthan 50 cm2.
The variability in outcomes reported by au-thors seems to be attributed to technique. Pu’s
From the Division of Plastic and Reconstructive Surgery,Feinberg School of Medicine, Northwestern University.Received for publication November 9, 2008; accepted De-cember 29, 2008.Copyright ©2009 by the American Society of Plastic SurgeonsDOI: 10.1097/PRS.0b013e3181a65a74
Disclosure: The authors have no financial interestin any of the products or techniques mentioned inthis article. The authors have no commercial asso-ciation with any company related to this study.
www.PRSJournal.com1748

emphasis on preservation of “critical perforators”is essential to elevating a viable distally based hemi-soleus flap. These “critical perforators” arise dis-tally off the posterior tibial artery just above thelevel of the medial malleous and supply the infe-riomedial aspect of the soleus muscle. Althoughultimately successful, three of 11 patients in thatseries suffered distal tip flap necrosis that requireddebridement and surgical advancement. This in-dicates that retrograde blood supply in the distalportions of the flap remains problematic evenwhen “critical perforators” are preserved.
The application of angiosome principles mayhelp address this limitation and improve out-comes of the distally based hemisoleus flap. Re-cent experience with single perforator flaps givessurgeons confidence that a flap can be elevatedand transferred based on only one or two perfo-rators. The proximal extent to which a perforatorflap can be reliably elevated is defined by retro-grade blood supply off the distal perforators andcan be determined using the angiosome principle,first described by Taylor and Palmer.17 A singleperforator can reliably carry axial blood flow to thenext adjacent perforator. Furthermore, the sameperforator can supply a variable distance beyondthe location of the adjacent perforator dependingon the index perforator’s location and size.
The senior author (G.A.D.) incorporated theangiosome principle into his distally based hemi-soleus flap design in 1997. Since then, 17 patientswith relatively small distal third leg wounds havebeen successfully managed using this technique atthe senior author’s institution. The purpose of thisstudy is to report the authors’ experience with thedistally based medial hemisoleus muscle flap, withan emphasis on flap design. We propose that at-tention to this principle will improve reliabilityand enhance outcomes in the management ofwounds in this difficult to treat area.
SURGICAL TECHNIQUEPatients with distal third leg wounds measur-
ing less than 50 cm2 are good candidates for dis-tally based hemisoleus flap soft-tissue coverage.18
In this series, only patients with strong and un-ambiguous pedal pulses and no evidence of me-dial soleus muscle trauma underwent the proce-dure described. The soleus muscle is a bipenniformmuscle with type II Mathes and Nahai bloodsupply.19 Anatomic studies demonstrate that themuscle receives its blood supply from two proxi-mal dominant vascular pedicles to the medial andlateral heads and from minor pedicles that orig-inate from the distal posterior tibial artery just
proximal to the level of the medial malleolus9,20
(Fig. 1). The distal perforators form the basis ofthe distally based hemisoleus flap. According tothe angiosome principle, the axial retrogradeblood supply of the most cephalad distal perfora-tor extends to the next most proximal perforatorthat originates off the proximally based dominantpedicle. Depending on the size of the perforatorand location of the distal perforator relative toperforators of the dominant pedicle, the distalperforator will also supply any area 2 to 3 cmbeyond to the dominant pedicle perforator (Fig.1). Patients, especially those with orthopedic frac-tures, may benefit from a preoperative angiogramto map the location and confirm the patency ofdistal perforators of the posterior tibial vessels thatsupply the soleus muscle (Fig. 2, above, right).
Fig. 1. Schematic anatomical drawing of blood supply to themedial hemisoleus muscle flap and illustration of the angio-some principle. Both proximal and distal perforators originateof the medial hemisoleus muscle originate from the posteriortibial artery. The distal perforator is often the largest and formsthe basis of the distally based medial hemisoleus muscle flap.In general, the axial retrograde blood supply of this perforatorextends to the proximal perforator (green). Depending on thesize of the perforator and location of the distal perforator rel-ative to the proximal perforator of the dominant pedicle, thedistal perforator will also supply any area 2 to 3 cm beyond tothe dominant pedicle perforator (yellow). The muscle may behorizontally divided at this level. The dashed line indicates thelongitudinal division of the muscle.
Volume 123, Number 6 • Distally Based Hemisoleus Flap
1749

A longitudinal incision is made overlying thesoleus muscle on the medial leg just anterior to theedge of the Achilles tendon and extending par-allel to the tibia. The open wound can be incor-porated into the incision. The skin is gently re-tracted, and perforators arising from the distalposterior tibial artery to the soleus muscle arelocated both visually and by handheld Doppler.The distal perforators serve as the pivot point anddetermine how far the flap can reach to the distalleg when the flap is transposed or turned over.Dissecting this perforator down to the posteriortibial artery will optimize the arc length of theflap.18 Once distal perforators are located, thenext large cephalad perforator is identified. Thisperforator enters the soleus muscle approximatelyat the point where the gastrocnemius muscle in-serts into the Achilles tendon. According to theangiosome principle, the distance between thesetwo perforators and a few centimeters proximal to thehigher perforator is the length of the flap (Fig. 1,above,
right). The medial hemisoleus muscle is divided atthis point.
Next, the medial hemisoleus muscle is sharplydissected off the Achilles tendon until the muscleraphe is encountered. The muscle is split longi-tudinally along the raphe down to the level of thedistal perforators. Sharp dissection is used again tomobilize the flap inferiorly toward the distal per-forators and to allow an adequate arc of rotationfor wound coverage. An audible Doppler signalconfirming flow into the muscle along with someelement of bleeding from the tip of the flap con-firms a viable flap and typically looks less robustthan other pedicled flaps. The medial hemisoleusmuscle is turned over or transposed into thewound and inset with absorbable sutures, takingcare to minimize tension on the flap. The donordefect is closed over a suction drain, and the flapis covered with a split-thickness skin graft. A pos-terior plaster splint is applied with care to preventany compression of the pedicle or the flap.
Fig. 2. Patient 8. (Above, left) Preoperative defect. (Above, right) Angiogram demonstrating a robust distal branch of the pa-tient’s posterior tibial artery. (Below, left) Intraoperative view with flap elevated. (Below, right) Appearance at long-term post-operative follow-up.
Plastic and Reconstructive Surgery • June 2009
1750

Postoperatively, patients are managed withbed rest and leg elevation for 4 to 5 days tominimize flap congestion and edema. No dan-gling protocols are required as in free flaps.Weight-bearing status is dictated by concomi-tant orthopedic issues, otherwise patients mayresume weight bearing after the period of bedrest. Unless other medical issues require an ex-tended hospital stay, most patients are dis-charged 5 days after surgery.
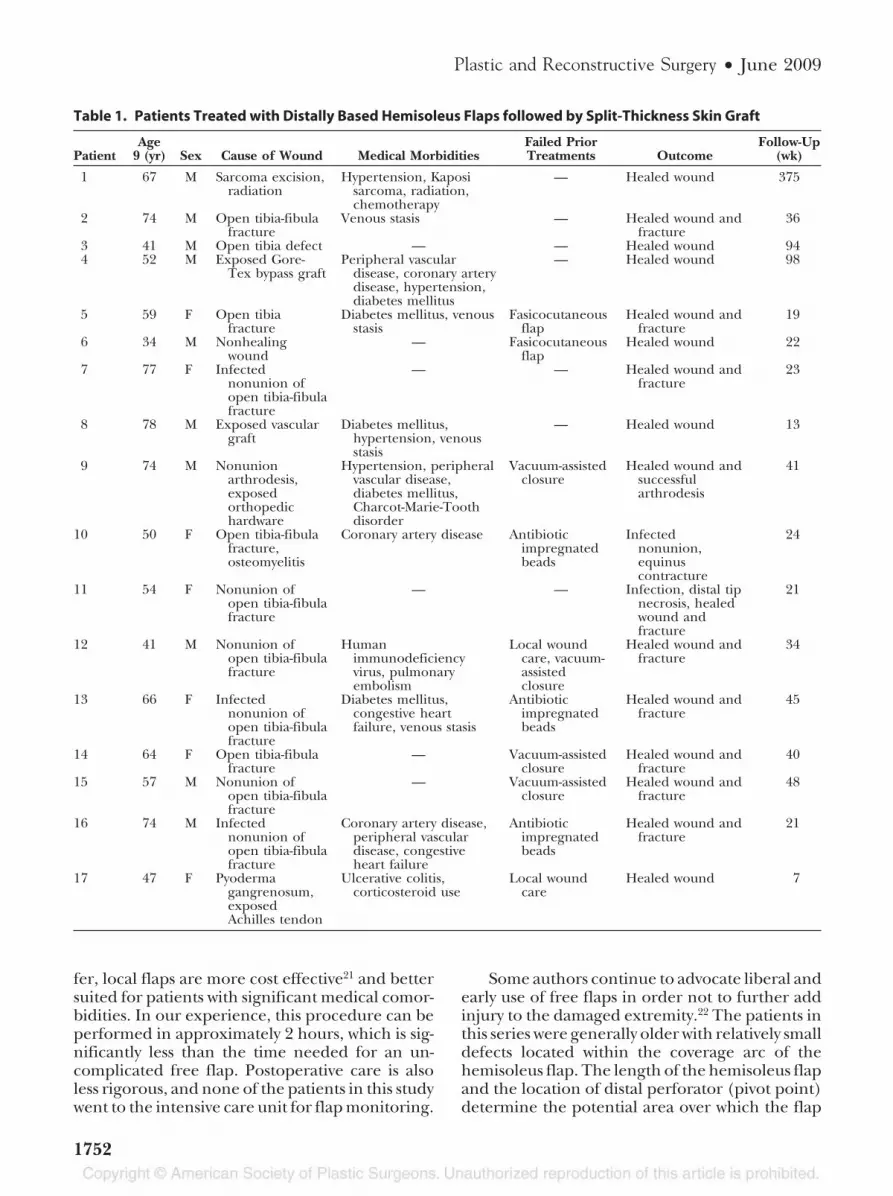
RESULTSOver 11 years, 17 patients (six women and 11
men, aged 34 to 78 years old) with distal third legwounds received a distally based medial hemiso-leus pedicled flap for definitive soft-tissue cover-age (Table 1). Wounds were located on the medialor anteromedial aspect of the leg between thejunction of the middle and distal thirds of the legand the ankle. Eleven patients had an either anopen fracture or exposed hardware at the time ofthe procedure.
In this series, the distally based hemisoleus flapwas the primary management option in nine pa-tients. Four patients were treated with a vacuum-assisted closure, and three patients with infectionswere treated with antibiotic-impregnated beadsbefore definite soft-tissue reconstruction. Attemptswere made to manage two patients (patients 5 and6) with local fasciocutaneous flaps based on distalposterior tibial artery perforators. These skin flapsdid not seem dependable enough for coverage ofthe open fractures at the time of their elevation,so the soleus flap was raised through the sameincision as a “bail-out” flap during the same op-eration. All muscle flaps were performed using thedescribed technique. Adequate debridement ofthe wound and bony stabilization of the leg wereachieved before soft-tissue reconstruction. Aver-age operative time of cases from incision to skinclosure was 130 minutes. The average size diam-eter of the distal perforator measured was 0.5 to1.5 mm.
The distally based hemisoleus flap was success-fully elevated in all patients. All patients were fol-lowed for a minimum of 2 months. The flap pro-vided reliable soft-tissue coverage and woundhealing in all patients, and all but one patient withan orthopedic fracture underwent complete frac-ture healing (Table 1 and Figs. 2 and 3). Patient4 eventually required a below-the-knee amputa-tion secondary to proximal arterial insufficiency.At the time of amputation, the flap site demon-strated complete wound healing with no signs ofinfection. Patient 8 did suffer a small area of skin
graft loss, which was successfully regrafted. Patient10 had an infected nonunion of his fracture andan equinus contracture that required Achilles ten-don lengthening. Only one patient (patient 11)suffered distal tip necrosis and was successfullytreated with in-office debridement and vacuum-assisted closure. From a reconstructive surgeryperspective, most patients were appropriate fordischarge on postoperative day 5 days after take ofthe skin graft was confirmed. There were no fur-ther restrictions placed on activity other thanthose required by the orthopedic surgery service.
DISCUSSIONAlthough traditional teaching emphasizes
the use of free tissue transfer,8 many authorsagree that local reconstructive options could bea reasonable alternative for soft-tissue coverageof smaller distal third leg wounds. In this study,the distally based hemisoleus flap was success-fully used for definitive treatment of 17 patients.The authors attribute their favorable outcomesto the application of angiosome principles dur-ing flap design.
The distally based soleus muscle flap is a usefulmodel to illustrate how detailed knowledge of an-giosomes is critical to the optimal design of flaps.Identification of an arterial perforator defines thepresence of an angiosome. The vascular territoryof this perforator can be reliably defined as de-scribed above. Generally, a flap designed on a singleperforator will include the entire angiosome andpart of the adjacent angiosome. When this principleis applied to the distally based hemisoleus flap,identification of perforators off of the distal pos-terior tibial artery will allow the surgeon to createa muscle flap, which is useful for coverage of distallower extremity defects. Without knowledge andapplication of the angiosome principle, a surgeonmay be tempted to use a larger portion of thehemisoleus muscle to increase its length or toincrease the bulk of the flap. This haphazard ap-proach will ultimately result in distal muscle prob-lems and increased complications and had led tosome of the controversy in prior series regardingthe reliability of this flap.
Careful peripheral vascular examination, ju-dicious use of the handheld Doppler, possibleconsideration of angiographic imaging, and in-traoperative confirmation of a viable bleeding flapall serve to ensure the integrity of the distal bloodsupply to the soleus muscle. Previous studies havedemonstrated the usefulness of the distally basedhemisoleus flap for soft-tissue coverage of distalleg wounds.14–16,20 Compared with free tissue trans-
Volume 123, Number 6 • Distally Based Hemisoleus Flap
1751
fer, local flaps are more cost effective21 and bettersuited for patients with significant medical comor-bidities. In our experience, this procedure can beperformed in approximately 2 hours, which is sig-nificantly less than the time needed for an un-complicated free flap. Postoperative care is alsoless rigorous, and none of the patients in this studywent to the intensive care unit for flap monitoring.
Some authors continue to advocate liberal andearly use of free flaps in order not to further addinjury to the damaged extremity.22 The patients inthis series were generally older with relatively smalldefects located within the coverage arc of thehemisoleus flap. The length of the hemisoleus flapand the location of distal perforator (pivot point)determine the potential area over which the flap
Table 1. Patients Treated with Distally Based Hemisoleus Flaps followed by Split-Thickness Skin Graft
PatientAge
9 (yr) Sex Cause of Wound Medical MorbiditiesFailed PriorTreatments Outcome
Follow-Up(wk)
1 67 M Sarcoma excision,radiation
Hypertension, Kaposisarcoma, radiation,chemotherapy
— Healed wound 375
2 74 M Open tibia-fibulafracture
Venous stasis — Healed wound andfracture
36
3 41 M Open tibia defect — — Healed wound 944 52 M Exposed Gore-
Tex bypass graftPeripheral vascular
disease, coronary arterydisease, hypertension,diabetes mellitus
— Healed wound 98
5 59 F Open tibiafracture
Diabetes mellitus, venousstasis
Fasicocutaneousflap
Healed wound andfracture
19
6 34 M Nonhealingwound
— Fasicocutaneousflap
Healed wound 22
7 77 F Infectednonunion ofopen tibia-fibulafracture
— — Healed wound andfracture
23
8 78 M Exposed vasculargraft
Diabetes mellitus,hypertension, venousstasis
— Healed wound 13
9 74 M Nonunionarthrodesis,exposedorthopedichardware
Hypertension, peripheralvascular disease,diabetes mellitus,Charcot-Marie-Toothdisorder
Vacuum-assistedclosure
Healed wound andsuccessfularthrodesis
41
10 50 F Open tibia-fibulafracture,osteomyelitis
Coronary artery disease Antibioticimpregnatedbeads
Infectednonunion,equinuscontracture
24
11 54 F Nonunion ofopen tibia-fibulafracture
— — Infection, distal tipnecrosis, healedwound andfracture
21
12 41 M Nonunion ofopen tibia-fibulafracture
Humanimmunodeficiencyvirus, pulmonaryembolism
Local woundcare, vacuum-assistedclosure
Healed wound andfracture
34
13 66 F Infectednonunion ofopen tibia-fibulafracture
Diabetes mellitus,congestive heartfailure, venous stasis
Antibioticimpregnatedbeads
Healed wound andfracture
45
14 64 F Open tibia-fibulafracture
— Vacuum-assistedclosure
Healed wound andfracture
40
15 57 M Nonunion ofopen tibia-fibulafracture
— Vacuum-assistedclosure
Healed wound andfracture
48
16 74 M Infectednonunion ofopen tibia-fibulafracture
Coronary artery disease,peripheral vasculardisease, congestiveheart failure
Antibioticimpregnatedbeads
Healed wound andfracture
21
17 47 F Pyodermagangrenosum,exposedAchilles tendon
Ulcerative colitis,corticosteroid use
Local woundcare
Healed wound 7
Plastic and Reconstructive Surgery • June 2009
1752

may be used. Generally, the width of the hemiso-leus muscle, from its medial edge to the raphe,determines the axial length of the defect that canbe covered. In this series, the critical area of tissuecoverage was no greater than 4 cm in all patients.The use of a free flap seems too aggressive forthese small yet clinically significant wounds.
Further advantages are apparent when com-paring the hemisoleus flap with other local recon-structive options. Preserving the lateral half of thehemisoleus flap aids in maintaining plantar flex-ion strength and provides a larger arc of rotationthan a traditional soleus muscle flap.9 Comparedwith fasicocutaneous flaps, the hemisoleus musclemay provide a better supply for improved fracturehealing when orthopedic trauma is present. In thisseries, attempts at treating two patients with fasi-cocutaneous flaps based on posterior tibial arteryperforators did not seem adequate during intra-operative assessment. In these cases, the hemiso-leus flap was successfully performed as a salvage
procedure. The distally based sural artery flap isanother option for distal third leg defects,23–25 butthese medially located wounds would require asural flap to wrap around the entire leg, limitingits usefulness. The vacuum-assisted closure de-vice has greatly improved the options for thesurgical timing and management of patientswith distal third leg wounds. Four patients weretemporarily managed with vacuum-assisted clo-sure after wound debridement but ultimatelyrequired definitive soft-tissue reconstruction,especially when tibial fractures and orthopedichardware were present.
In summary, the distally based pedicled hemi-soleus muscle flap is a viable option for soft-tissuecoverage of medial distal third leg wounds. The au-thors contend that outcomes of the procedure canbe improved by incorporation of the angiosomeprinciples in flap design. This flap can be used asa primary, secondary, or salvage option for small
Fig. 3. Patient 5. (Above, left) Preoperative defect. (Above, right) Intraoperative view with the distally based hemisoleus flapelevated. A proximal V-Y flap was used to reduce the size of the defect. (Below, left) Postoperative follow-up with externalfixation still in place. (Below, right) Long-term postoperative follow-up.
Volume 123, Number 6 • Distally Based Hemisoleus Flap
1753

medial lower leg defects and provides an alterna-tive to free flap reconstruction.
Clark F. Schierle, M.D., Ph.D.Division of Plastic and Reconstructive Surgery
Northwestern University, Feinberg School of Medicine675 North St. Clair Street
Gaiter Suite 19-250Chicago, Ill. [email protected]
REFERENCES1. Holden CEA. The role of blood supply to soft tissue in the
healing of diaphyseal fracture. J Bone Joint Surg (Am). 1977;54:99–1000.
2. May JW Jr, Jupiter JB, Gallico GG 3rd, Rothkopf DM,Zingarelli P. Treatment of chronic traumatic bone wounds.Microvascular free tissue transfer: A 13-year experience in 96patients. Ann Surg. 1991;214:241–250.
3. May JW Jr, Gallico GG 3rd, Lukash FN. Microvasculartransfer of free tissue for closure of bone wounds of thedistal lower extremity. N Engl J Med. 1982;306:253–257.
4. Lineaweaver WC, Hui K, Yim K, et al. The role of the plasticsurgeon in the management of surgical infection. Plast Re-constr Surg. 1999;103:1553–1560.
5. Anthony JP, Mathes SJ, Alpert BS. The muscle flap in thetreatment of chronic lower extremity osteomyelitis: Resultsin patients over 5 years after treatment. Plast Reconstr Surg.1991;88:311–318.
6. Gayle LB, Lineaweaver WC, Oliva A, et al. Treatment ofchronic osteomyelitis of the lower extremities with debride-ment and microvascular muscle transfer. Clin Plast Surg.1992;19:895–903.
7. Marek CA, Pu LLQ. Refinements of free tissue transfer foroptimal outcome in lower extremity reconstruction. AnnPlast Surg. 2004;52:270–275.
8. Heller L, Levin LS. Lower extremity microvascular recon-struction. Plast Reconstr Surg. 2002;108:1029–1041.
9. Tobin GR. Hemisoleus and reversed hemisoleus flaps. PlastReconstr Surg. 1985;76:87–96.
10. Fayman MS, Orak F, Hugo B, Berson SD. The distally basedsplit soleus muscle flap. Br J Plast Surg. 1987;40:20.
11. Hallock GG. Getting the most from the soleus muscle. AnnPlast Surg. 1996;36:139–146.
12. Magee WP Jr, Gilbert DA, McInnis WD. Extended muscleand musculocutaneous flaps. Clin Plast Surg. 1980;7:57–70.
13. Townsend PL. An inferiorly based soleus muscle flap. Br JPlast Surg. 1978;31:210–213.
14. Pu LLQ. Successful soft-tissue coverage of a tibial wound inthe distal third of the leg with a medial hemisoleus muscleflap. Plast Reconstr Surg. 2005;115:245–251.
15. Beck JB, Stile F, Lineaweaver W. Reconsidering the soleusmuscle flap for coverage of wounds of the distal third of theleg. Ann Plast Surg. 2003;50:631–635.
16. Pu LLQ. The reversed medial hemisoleus muscle flap and itsrole in reconstruction of an open tibial wound in the distalthird of the leg. Ann Plast Surg. 2006;56:59–64.
17. Taylor GI, Palmer JH. The vascular territories (angiosomes)of the body: Experimental study and clinical applications. Br JPlast Surg. 1987;40:113–141.
18. Pu LLQ. Further experience with the medial hemisoleusmuscle flap for soft-tissue coverage of a tibial wound in thedistal third of the leg. Plast Reconstr Surg. 2008;121:2024–2028.
19. Mathes SJ, Nahai F. Classification of the vascular anatomy ofmuscles: Experimental and clinical correlation. Plast ReconstrSurg. 1981;67:177–187.
20. Raveendran SS, Kumaragama KG. Arterial supply of the so-leus muscle: Anatomical study of fifty lower limbs. Clin Anat.2003;16:248–252.
21. Thornton BP, Rosenblum WJ, Pu LLQ. Reconstruction oflimited soft-tissue defect with open tibial fracture in the distalthird of the leg: A cost and outcome study. Ann Plast Surg.2005;54:276–280.
22. Godina M. Early microsurgical reconstruction of complextrauma of the extremities. Plast Reconstr Surg. 1986;78:285–292.
23. Hollier L, Sharma S, Babigumira E, Klebuc M. Versatility ofthe sural fasciocutaneous flap in the coverage of lower ex-tremity wounds. Plast Reconstr Surg. 2002;110:1673–1679.
24. Huisinga RL, Houpt P, Dijkstra R, Storm van Leeuwen JB.The distally based sural artery flap. Ann Plast Surg. 1998;41:58.
25. Hsieh CH, Liang CC, Kueh NS, et al. Distally based suralisland flap for the reconstruction of a large soft tissue defectin an open tibial fracture with occluded anterior and pos-terior tibial arteries: a case report. Br J Plast Surg. 2005;58:112–115.
Plastic and Reconstructive Surgery • June 2009
1754





























