ORIGINAL ARTICLES
Knowledge and Cultural Beliefs About the Etiology and Management ofOrofacial Clefts in Nigeria’s Major Ethnic Groups
Fadekemi O. Oginni, B.Ch.D., F.M.C.D.S., Malachy E. Asuku, M.B.B.S., F.W.A.C.S., Ayodeji O. Oladele, M.B.Ch.B.,
F.W.A.C.S., Ozoemene N. Obuekwe, B.Ch.D., F.W.A.C.S., Richard E. Nnabuko, F.W.A.C.S., F.M.C.S.
Objective: To determine the knowledge and cultural beliefs about theetiology and management of orofacial clefts in Nigeria’s major ethnic groups.
Design: Questionnaires designed to elicit respondents’ knowledge andcultural beliefs about the etiology and management of orofacial clefts.
Setting: Northern and southern Nigerian communities where the major ethnicgroups reside.
Participants: Consenting, randomly selected individuals.Results: There were 650 respondents (350 women and 300 men) from 34 of
Nigeria’s 36 states; 65.5% were aged 21 to 40 years and 52.5% were married. Therewere Yoruba (33.7%), Igbo/Bini/Urhobo (40.5%), and Hausa/Fulani (25.8%), withmost having attained primary and secondary education. Of those responding,75% had seen an individual with an orofacial cleft. A significant level of ignoranceabout the cultural beliefs was found. The Hausa/Fulani considered it mostly an actof God; whereas, the Igbo/Bini/Urhobo and Yoruba groups displayed a greatervariety of cultural beliefs. The latter groups implicated witchcraft, evil spirit ordevil, the mother, and occasionally the child. Of respondents, 40% knew thatsurgery was a possible solution, and 22% would recommend a visit to thehospital. Respondents with higher educational attainment produced significantlymore scientifically related etiologic factors and accurate treatment options.
Conclusion: Of respondents, 75% were aware of the existence of orofacialclefts, and a fair knowledge of treatment of orofacial clefts was elicited. Diversecultural beliefs often may present an obstacle to treatment. Improvedawareness about the etiology and management of orofacial clefts is required.
KEY WORDS: culture, etiology, orofacial clefts
Culture, by definition, is the total way of life of
individuals. Immense variations exist in cultural beliefs,
concepts, and practices on particular issues from place to
place. The combination of culture and knowledge, howev-
er, is a powerful tool influencing the behavioral pattern of
any individual and may be a major determinant of health-
seeking behaviors. Poor health-seeking behaviors are
observed in most developing nations (Meremikwo et al.,
2005) for diverse reasons (Obuekwe and Akapata, 2004;
Uzochukwu and Onwujekwe, 2004).
The treatment of birth defects and other disabilities is
influenced particularly by an interplay of cultural beliefs of
the individual, family, and society, as well as folk and
traditional religious beliefs (Cheng, 1990) and available
knowledge. In the past, reports showed that children born
with defects were a bad omen to the family, and they were
concealed or neglected (Gupta, 1969).
The attitudes of patients, patients’ families, and the
community toward the nature, cause, effect, and treatment
of orofacial clefts are important to the therapeutic process
as well as the social and emotional development of patients
(Patel and Ross, 2003). Cultural diversity has a profound
effect on the ways in which families and professionals
interrelate cross-culturally and participate together in
treatment programs (Louw, 2004). Broder (2001) suggested
that interventions need to be culturally sensitive because
Dr. Oginni is Senior Lecturer, Department of Oral and Maxillofacial
Surgery, Faculty of Dentistry, Obafemi Awolowo University, Ile-Ife,
Nigeria. Dr. Asuku is Consultant Plastic Surgeon, Department of Surgery,
Ahmadu Bello University, Zaria, Kaduna State, Nigeria. Dr. Oladele is
Lecturer, Department of Surgery, Plastic Surgery Unit, Obafemi
Awolowo University, Ile-Ife, Nigeria. Dr. Obuekwe is Associate
Professor, Department of Oral and Maxillofacial Surgery, School of
Dentistry, University of Benin, Benin City, Nigeria. Dr. Nnabuko is
Consultant Plastic Surgeon, Plastic Surgery Department, National
Orthopedic Hospital, Enugu, Nigeria.
A portion of this work was presented orally at the International Cleft
Lip and Palate Foundation Conference, Eastbourne, United Kingdom, in
June 2006 and at the Third International Conference on Birth Defects and
Disabilities in the Developing World, Rio de Janeiro, Brazil, in June 2007.
Submitted May 2007; Accepted September 2008.
Address correspondence to: Dr F. O. Oginni, Department of Oral and
Maxillofacial Surgery, Faculty of Dentistry, Obafemi Awolowo Univer-
sity, Ile-Ife Nigeria. E-mail [email protected] or foginni@oauife.
edu.ng.
DOI: 10.1597/07-085.1
327
parental and extrafamilial contexts may differ acrossvarying cultures and ethnicities. Total care delivery,
therefore, calls for a proper understanding and identifica-
tion of culturally based stigmas and beliefs associated with
such conditions. A rural Mexican belief, for example,
suggests that a pregnant woman is in danger of having a
‘‘harelipped baby during a solar eclipse’’ (Castro, 1995,
pp. 229–238). In China, some people believe that a pregnant
woman should not eat rabbit meat for fear of giving birth to ababy with a ‘‘harelip’’ (Cheng, 1990). However, cultural
beliefs about birth defects in Nigeria are unknown.
Nigeria, Africa’s most populous country, has anestimated population of about 140 million people. Addi-
tionally, the country is blessed with a diverse cultural
heritage, as revealed by Nigeria’s approximately 250 ethnic
groups. Although the country is a multicultural society, the
Hausa/Fulani, Igbo/Bini/Urhobo, and Yoruba are consid-
ered its three major ethnic groups.
As in other African countries, orofacial clefts constitute a
substantial proportion of birth defects in the Nigerian
population (Strauss, 1985; Obuekwe and Akapata, 2004).
Iregbulem (1982) reported that the prevalence of cleft lip
and palate in a Nigerian population was 0.4 per 1000births. It was reported and widely believed that orofacial
birth defects were stigmatized in Nigeria. Furthermore,
infanticide was practiced, and attitudinal barriers to the
development of rehabilitation resources existed there
(Strauss, 1985). The presence of adults and school-aged
children with untreated orofacial clefts in Nigerian
communities suggest enhanced survival of children born
with the defect. Moreover, it is a reflection of poor health-seeking behaviors and financial constraints, among other
probable factors, and some level of adjustment to
stigmatization in affected individuals.
Accordingly, we sought to determine the knowledge,attitudes, and cultural beliefs in Nigeria’s major ethnic
groups regarding the etiology and management of orofacial
clefts. The findings of this research will form a basis for
formulating an effective awareness campaign tool relevant
to educating the public on the etiology, predisposing
factors, and management of orofacial clefts.
MATERIALS AND METHODS
The authors administered a structured questionnaire
(Appendix A) by interview to consenting, randomly
selected individuals in communities of northern and
southern Nigeria. We used the cluster sampling technique
in selecting communities and simple randomization inselecting respondents among passersby and dwellers within
selected clusters. The study was conducted between
October 1, 2006, and December 31, 2006. Principles
outlined in the Declaration of Helsinki were followed.
The questionnaire was designed to elicit respondents’
knowledge of and cultural beliefs about the etiology and
management of orofacial clefts. Questions inquiring about
respondents’ beliefs and knowledge regarding the etiology
of orofacial clefts were open ended. Section A of the
questionnaire inquired about standard socio-demographic
features of respondents, and section B was designed to
assess their knowledge and cultural beliefs about the
etiology of orofacial clefts as well as possible treatment
modalities. The respondents were grouped into three
categories based on ethnicity: Hausa/Fulani, Igbo/Bini/
Urhobo, and Yoruba. The responses given were scored for
correctness.
Data were entered into a computer and analyzed using
Statistical Package for the Social Sciences (SPSS) statistical
software (SPSS, Inc., Chicago, IL). Simple descriptive
statistics, chi-square tests, and Pearson correlations were
used. A p level of # .05 was considered statistically significant.
RESULTS
There were 650 respondents (350 women and 300 men)
from 34 of Nigeria’s 36 states. The ethnic groups
represented were Yoruba (33.7%), Igbo/Bini/Urhobo
(40.5%), and Hausa/Fulani (25.8%). No significant gender
differences by age group were observed (Table 1). Howev-
er, a significant (p , .05) male predilection was observed in
the Hausa ethnic group (Table 1). Of the respondents,
65.5% were aged 21 to 40 years (Table 1) and 52.5% were
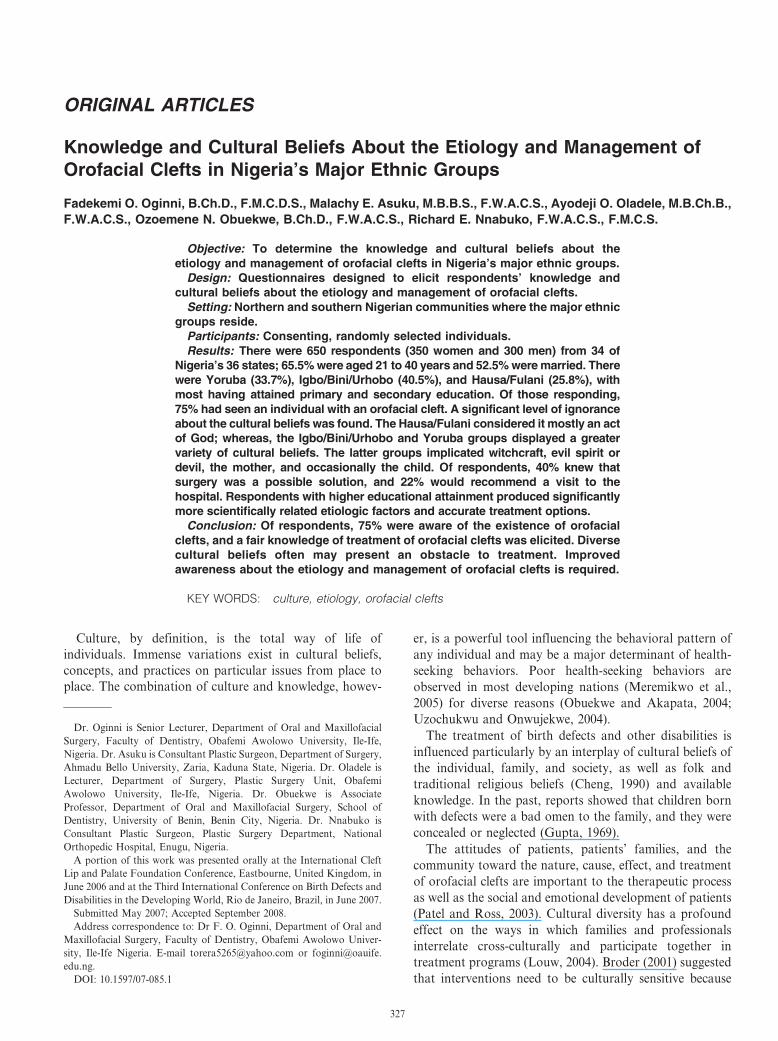
married. About 8% (n 5 54) of respondents had no formal
education, 37.2% (n 5 242) had primary education, and
54.5% (n 5 354) had postsecondary education (Fig. 1).
Three quarters of respondents had seen at least one
individual with an orofacial cleft, and these respondents
were mostly from the Igbo/Bini/Urhobo (85%) and Yoruba
(77%) ethnic groups (Table 2). The individuals seen with
TABLE 1 Respondents’ Ethnic Group, Age, and Marital Status by
Gender (n = 650)
Variables Men, n (%) Women, n (%) Total, n (%)
Ethnic groups
Hausa/Fulani 103 (15.8) 65 (10.0) 168 (25.8)
Igbo/Bini/Urhobo 102 (15.7) 161 (24.8) 263 (40.5)
Yoruba 95 (14.6) 124 (19.1) 219 (33.7)
Total 300 (46.2) 350 (53.8) 650 (100.0)
x2 5 21.95, df 5 2, p # .05
Age group (y)
0–20 22 (3.4) 26 (4.0) 48 (7.4)
21–40 199 (30.6) 227 (34.9) 426 (65.5)
41–60 64 (9.8) 85 (13.1) 149 (22.9)
.60 15 (2.3) 12 (1.8) 27 (4.2)
Total 300 (46.2) 350 (53.8) 650 (100.0)
x2 5 1.63, df 5 3, p . .05
Marital status
Single 144 (22.2) 148 (22.8) 292 (45.0)
Married 155 (23.8) 186 (28.6) 341 (52.4)
Divorced* 0 (0.0) 5 (0.8) 5 (0.8)
Widowed* 1 (0.2) 11 (1.7) 12 (1.9)
Total 300 (46.2) 350 (53.9) 650 (100.1)
x2 5 1.63, df 5 2, p , .05
* Merged for analysis.
328 Cleft Palate–Craniofacial Journal, July 2010, Vol. 47 No. 4
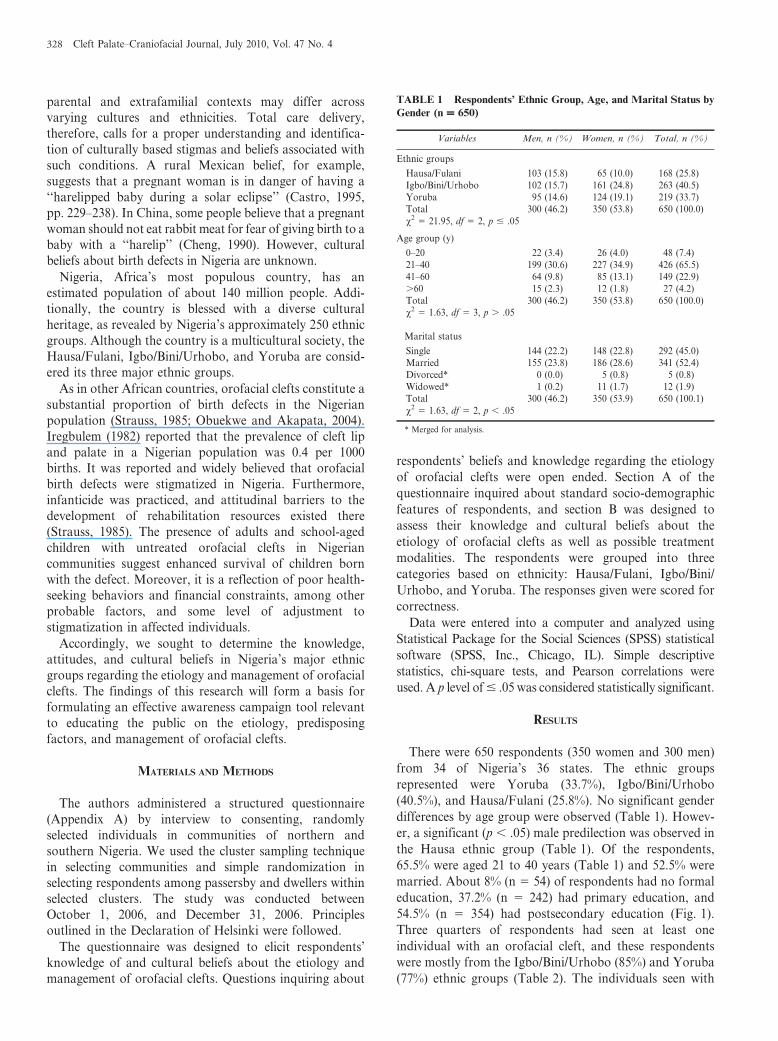
orofacial clefts were identified rarely as their close relations
(4.1%) and usually as an unknown person just passing by
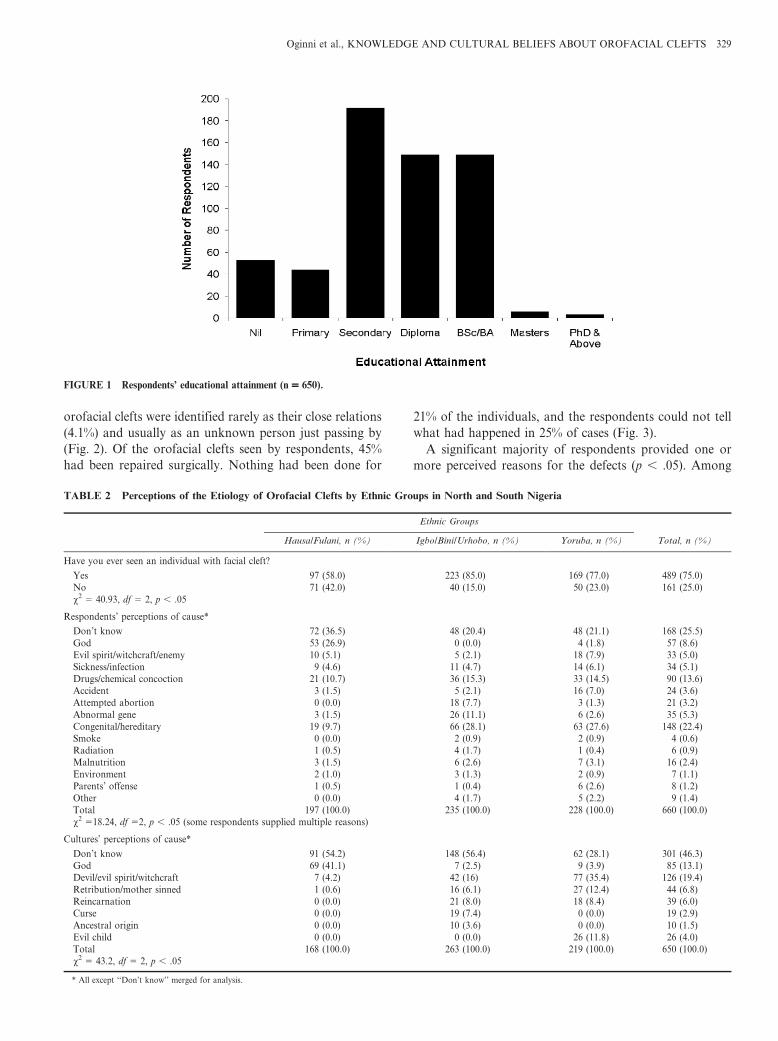
(Fig. 2). Of the orofacial clefts seen by respondents, 45%
had been repaired surgically. Nothing had been done for
21% of the individuals, and the respondents could not tell
what had happened in 25% of cases (Fig. 3).
A significant majority of respondents provided one or
more perceived reasons for the defects (p , .05). Among
FIGURE 1 Respondents’ educational attainment (n = 650).
TABLE 2 Perceptions of the Etiology of Orofacial Clefts by Ethnic Groups in North and South Nigeria
Ethnic Groups
Total, n (%)Hausa/Fulani, n (%) Igbo/Bini/Urhobo, n (%) Yoruba, n (%)
Have you ever seen an individual with facial cleft?
Yes 97 (58.0) 223 (85.0) 169 (77.0) 489 (75.0)
No 71 (42.0) 40 (15.0) 50 (23.0) 161 (25.0)
x2 5 40.93, df 5 2, p , .05
Respondents’ perceptions of cause*
Don’t know 72 (36.5) 48 (20.4) 48 (21.1) 168 (25.5)
God 53 (26.9) 0 (0.0) 4 (1.8) 57 (8.6)
Evil spirit/witchcraft/enemy 10 (5.1) 5 (2.1) 18 (7.9) 33 (5.0)
Sickness/infection 9 (4.6) 11 (4.7) 14 (6.1) 34 (5.1)
Drugs/chemical concoction 21 (10.7) 36 (15.3) 33 (14.5) 90 (13.6)
Accident 3 (1.5) 5 (2.1) 16 (7.0) 24 (3.6)
Attempted abortion 0 (0.0) 18 (7.7) 3 (1.3) 21 (3.2)
Abnormal gene 3 (1.5) 26 (11.1) 6 (2.6) 35 (5.3)
Congenital/hereditary 19 (9.7) 66 (28.1) 63 (27.6) 148 (22.4)
Smoke 0 (0.0) 2 (0.9) 2 (0.9) 4 (0.6)
Radiation 1 (0.5) 4 (1.7) 1 (0.4) 6 (0.9)
Malnutrition 3 (1.5) 6 (2.6) 7 (3.1) 16 (2.4)
Environment 2 (1.0) 3 (1.3) 2 (0.9) 7 (1.1)
Parents’ offense 1 (0.5) 1 (0.4) 6 (2.6) 8 (1.2)
Other 0 (0.0) 4 (1.7) 5 (2.2) 9 (1.4)
Total 197 (100.0) 235 (100.0) 228 (100.0) 660 (100.0)
x2 518.24, df 52, p , .05 (some respondents supplied multiple reasons)
Cultures’ perceptions of cause*
Don’t know 91 (54.2) 148 (56.4) 62 (28.1) 301 (46.3)
God 69 (41.1) 7 (2.5) 9 (3.9) 85 (13.1)
Devil/evil spirit/witchcraft 7 (4.2) 42 (16) 77 (35.4) 126 (19.4)
Retribution/mother sinned 1 (0.6) 16 (6.1) 27 (12.4) 44 (6.8)
Reincarnation 0 (0.0) 21 (8.0) 18 (8.4) 39 (6.0)
Curse 0 (0.0) 19 (7.4) 0 (0.0) 19 (2.9)
Ancestral origin 0 (0.0) 10 (3.6) 0 (0.0) 10 (1.5)
Evil child 0 (0.0) 0 (0.0) 26 (11.8) 26 (4.0)
Total 168 (100.0) 263 (100.0) 219 (100.0) 650 (100.0)
x2 5 43.2, df 5 2, p , .05
* All except ‘‘Don’t know’’ merged for analysis.
Oginni et al., KNOWLEDGE AND CULTURAL BELIEFS ABOUT OROFACIAL CLEFTS 329
the variety of reasons offered, 22% (148/660) referred to it
as a congenital defect (Table 2). A majority of respondents
in the Hausa group (42.4%) attributed it to God but rarely
to witchcraft, evil spirit, or devil (8%), which was the most
common belief in the Igbo/Bini/Urhobo and Yoruba ethnic
groups (Table 2). The mother and occasionally the child
were implicated by the latter tribes. Overall, the Yoruba
and Igbo/Bini/Urhobo groups displayed a greater variety of
cultural beliefs, as shown in Table 2.
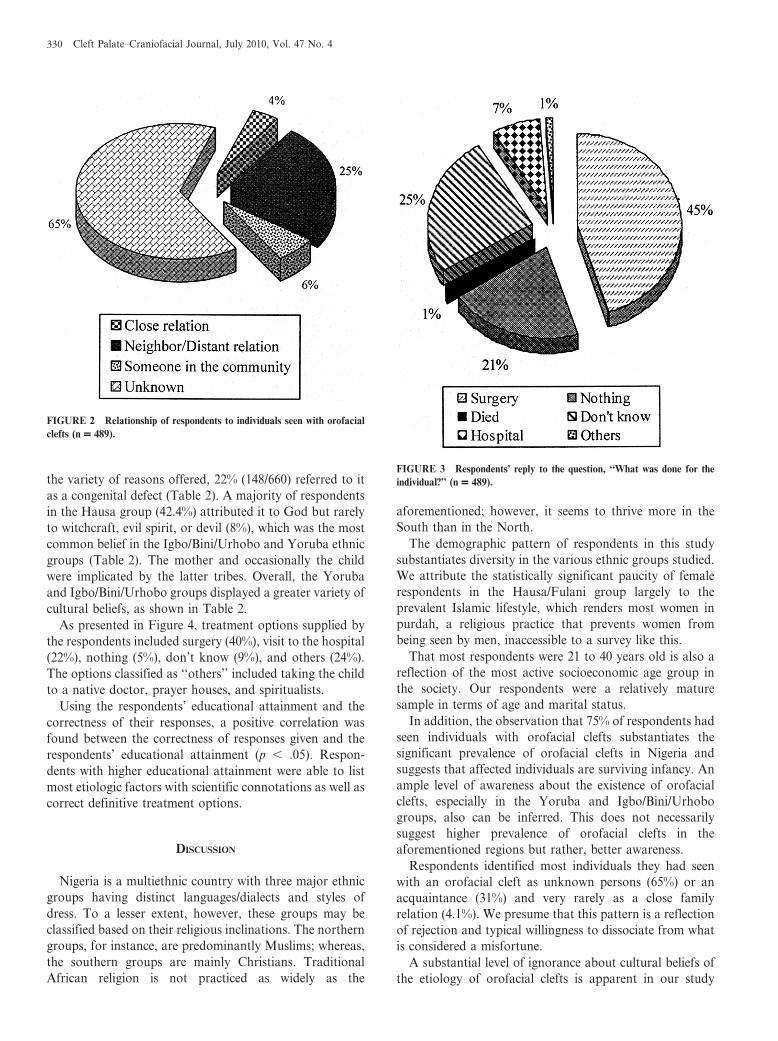
As presented in Figure 4, treatment options supplied by
the respondents included surgery (40%), visit to the hospital
(22%), nothing (5%), don’t know (9%), and others (24%).
The options classified as ‘‘others’’ included taking the child
to a native doctor, prayer houses, and spiritualists.
Using the respondents’ educational attainment and the
correctness of their responses, a positive correlation was
found between the correctness of responses given and the
respondents’ educational attainment (p , .05). Respon-
dents with higher educational attainment were able to list
most etiologic factors with scientific connotations as well as
correct definitive treatment options.
DISCUSSION
Nigeria is a multiethnic country with three major ethnic
groups having distinct languages/dialects and styles of
dress. To a lesser extent, however, these groups may be
classified based on their religious inclinations. The northern
groups, for instance, are predominantly Muslims; whereas,
the southern groups are mainly Christians. Traditional
African religion is not practiced as widely as the
aforementioned; however, it seems to thrive more in the
South than in the North.
The demographic pattern of respondents in this study
substantiates diversity in the various ethnic groups studied.
We attribute the statistically significant paucity of female
respondents in the Hausa/Fulani group largely to the
prevalent Islamic lifestyle, which renders most women in
purdah, a religious practice that prevents women from
being seen by men, inaccessible to a survey like this.
That most respondents were 21 to 40 years old is also a
reflection of the most active socioeconomic age group in
the society. Our respondents were a relatively mature
sample in terms of age and marital status.
In addition, the observation that 75% of respondents had
seen individuals with orofacial clefts substantiates the
significant prevalence of orofacial clefts in Nigeria and
suggests that affected individuals are surviving infancy. An
ample level of awareness about the existence of orofacial
clefts, especially in the Yoruba and Igbo/Bini/Urhobo
groups, also can be inferred. This does not necessarily
suggest higher prevalence of orofacial clefts in the
aforementioned regions but rather, better awareness.
Respondents identified most individuals they had seen
with an orofacial cleft as unknown persons (65%) or an
acquaintance (31%) and very rarely as a close family
relation (4.1%). We presume that this pattern is a reflection
of rejection and typical willingness to dissociate from what
is considered a misfortune.
A substantial level of ignorance about cultural beliefs of
the etiology of orofacial clefts is apparent in our study
FIGURE 2 Relationship of respondents to individuals seen with orofacial
clefts (n = 489).
FIGURE 3 Respondents’ reply to the question, ‘‘What was done for the
individual?’’ (n = 489).
330 Cleft Palate–Craniofacial Journal, July 2010, Vol. 47 No. 4

population. We attribute this to a combination of
modernization and a semirural study population. Perhaps
respondents drawn from a purely rural population would
generate better awareness of the cultural beliefs; nonethe-
less, a significant range of cultural beliefs was volunteered
by the studied groups.
Only a minority of respondents had no opinion about the
etiology of orofacial cleft. Others supplied a range of
reasons that varied by ethnic group. God’s will was the
major reason supplied by Hausa/Fulani respondents. This
is in agreement with previous findings of the same ethnic
group in Nigeria (Olasoji et al., 2007) and also concurs with
the cultural beliefs supplied by a majority in the Hausa/
Fulani ethnic group, thus suggesting a high level of culture
agreement. This is also in agreement with the belief of the
Chamorros, an Asian American group that views a cleft as
FIGURE 4 Percentages of respondents’ answers to the question, ‘‘What can be done to help individuals with these defects?’’.
Oginni et al., KNOWLEDGE AND CULTURAL BELIEFS ABOUT OROFACIAL CLEFTS 331

a gift from God (Cheng, 1990), as well as a rural Indian
population (Weatherley-White et al., 2005).
Unlike the Hausa/Fulani group, the Yoruba and Igbo/
Bini/Urhobo respondents’ personal opinions appeared to
differ considerably from the prevailing cultural beliefs.
Although evil spirit, witchcraft, and devil were prominent
cultural beliefs reported, a majority of the respondents
did not agree with these as reasons for the defect. Rather,
a combination of drugs, chemicals, and concoctions were
implicated by a majority. Furthermore, and closely
related to this, they suggested attempted criminal
abortion through the use of drugs. It is interesting that
sickness, infection, abnormal gene, radiation, malnutri-
tion, and the environment also were offered as reasons
for the defect in these groups. Again, this lends credence
to a shift from the cultural beliefs, which we attribute to
an increase in critical observation and influence of formal
education. A number of the respondents’ opinions of the
etiology of orofacial clefts were classified as ‘‘other’’ in
the results. These included opinions such as ‘‘parents
violated cultural laws,’’ ‘‘parent(s) bore false witness,’’ ‘‘it
is the child’s destiny,’’ and ‘‘mother killed and mutilated
a goat,’’ among others.
The belief of Buddhists (Cheng, 1990), who consider
birth defect a fate for which nothing can be done, can be
likened to seeing orofacial clefts as a gift from God or the
will of God. This belief may be a deterrent for seeking
treatment because the thinking may be ‘‘after all, man
cannot be wiser than God.’’
Unlike the Hausa/Fulani (predominantly Islamic)
group, the cultural beliefs supplied by the other (southern)
ethnic groups indicate the prominence of traditional
African religion in these locations. It is surprising that
none of the cultural beliefs given is comparable with
scientifically supported predisposing factors. Such cultural
beliefs (particularly among the Yorubas) include insinuat-
ing that the child is an evil spirit that gained access to the
mother’s womb because she walked in the hot sun (at
about 1:00 PM) or late at night in the dark (after 7:00 PM)
when it is believed that evil spirits walk around and seek a
place to stay. The belief is that such spirits displace a
healthy child and take his or her place. Also, the spirits of
individuals who died suddenly in vehicle crashes are
believed to replace healthy children in a mother’s womb
with their maimed bodies. Similar to Dagher and Ross’
(2004) findings, others believe that witchcraft or an enemy
could have done it to afflict the parents of the child with
sorrow. Some viewed it as a consequence of hunting
activities by the child’s father, who must have killed a
strange animal. The deformity, according to them, is a
result of the harm done to the strange animal. Similarly,
some believe ardently that the pregnant mother must have
walked amid warriors and in the process, the child
sustained gunshot injuries or machete cuts. Such injuries,
according to them, only become apparent at birth and
take the form of an orofacial cleft.
Traditional African religion is associated with a number
of laws that, according to some of respondents, must have
been violated for a defect like a cleft to have occurred. For
example, some see orofacial clefts as an aftermath of eating
certain food items that are forbidden, failure to fulfill some
obligations like eating and drinking relevant concoctions
during pregnancy, or stealing by either the father or
mother. Oftentimes, wrongdoings were traced to the
mother who, according to the respondents, would be
confronted with implicating and derogatory expressions
like ‘‘You are the only one that can explain where you got a
child like this from’’; ‘‘Your sin has found you out’’; ‘‘We
have never seen this in this family’’; and ‘‘You must have
bad eggs in your body,’’ among others.
Furthermore, some Nigerians believe that there must be
a curse at work and that the problem could have ancestral
origin. This belief was elicited only in the Yoruba and Igbo/
Bini/Urhobo groups. Here, the problem is traced back to
parents, grandparents, or even great-grandparents doing
something evil. This idea is in agreement with the
documented opinion of Filipinos and Chinese (Cheng,
1990). On some occasions, the Yoruba and Igbo/Bini/
Urhobo would also implicate the child directly and call
him/her evil. This may have been a reason for infanticide.
Closely related to infanticide and exclusively common to
the southern ethnic groups is the belief that individuals with
orofacial clefts are reincarnated children (Clarke, 1976).
The infant mortality rate in Nigeria was very high several
decades ago. Most cultures attributed this to activities of
evil spirits. However, with modernization it became
apparent that these were the results of poor infection
control, malnutrition, and inadequate care of the newborn
including lack of immunization against major childhood
killer diseases, among other reasons. The belief was that the
dead child had gone to the spirit world and had been
reincarnated into the same home by his/her choice to afflict
the parents with sorrow. This belief fits perfectly into a
situation where an underlying genetic problem predisposes
to repeated infant mortality, stillbirth, and congenital
deformities in the same couple. They affirm their belief
that the same child is reincarnating on the strength of very
close resemblance between the departed and the newborn,
forgetting that it is still virtually the same gene at work in
the couple. Grandparents, parents, family herbalists, or a
combination of these agree to and do maim the corpses of
such children to make them unacceptable to the spirit
world, hoping that the child would reincarnate with a
maimed body that is cleft lip, palate, or any physical
congenital defect and therefore stay alive. In their thinking,
the deformity guarantees staying alive, and an ardent
believer in this may resist a repair for fear of the child dying
again.
It is quite impressive to note that a majority of our
respondents would suggest surgery and/or a visit to the
hospital as a remedy. Nevertheless, a substantial 38% did
not have any idea of the correct approach to the situation.
332 Cleft Palate–Craniofacial Journal, July 2010, Vol. 47 No. 4

Measures like taking the child to a spiritual home, prayer
house, or doing nothing were offered also.
In view of the fact that successful and complete cleft carerequires recognition and consideration of cultural diversity
and differing ethnic and cultural interactional styles, we
opine that it is probably insufficient to provide surgical
remedies alone for orofacial clefts. The knowledge and
beliefs of potential care recipients may hinder them from
obtaining the maximum benefit from such methods. Based
on the findings of this study, an effective, culturally
sensitive public health and awareness package should beput in place for the population described. A similar
program would work for populations that share similar
cultural beliefs about orofacial clefts and other birth
defects. Such programs must be directed at eliminating
the identified unfounded cultural beliefs as well as other
related issues peculiar to each ethnic group.
We acknowledge that a bigger sample size may have been
desirable. However, financial limitations precluded a largerstudy. To a large extent, the study design has reduced bias
and misrepresentation of respondents’ opinions by the
sampling techniques used. Also, making the aspects on
belief open ended gave the respondents the opportunity to
fully express their opinions. Language barriers were
eliminated by using the authors, who are indigenes of the
various ethnic groups, to administer the questionnaires.
Furthermore, the use of open-ended questions, which gaverespondents the opportunity to fully express their opinions,
represents a strength of this study. In our opinion, these
findings may not differ grossly from those of other
Nigerian ethnic groups.
CONCLUSION
An understanding of the cultural beliefs about theetiology of orofacial clefts in the regions was gained. We
also were able to elicit a fair knowledge of the actual
etiology and treatment of orofacial clefts, particularly in
the southern ethnic groups. Orofacial clefts are seen often
as an act of God by northern ethnic groups. Southern
groups, however, are likely to attribute it to diverse cultural
beliefs, some of which implicate the mother and/or the
child. The need for more enlightenment about etiology and
treatment of orofacial clefts is apparent. The detrimental
beliefs must be debunked through an effective health
education and awareness campaign specially designed and
incorporated into the specified ethnic groups in Nigeria.
This could be applicable to non-Nigerian ethnic groups
that share the same beliefs.
REFERENCES
Broder HI. Using psychological assessment and therapeutic strategies to
enhance well-being. Cleft Palate Craniofac J. 2001;38:248–254.
Castro R. The logic of a traditional health belief: solar eclipse and
pregnancy in Ocuituco, Mexico. Salud Publica Mex. 1995;37:329–338.
Cheng LR. Asian American cultural perspectives on birth defects: focus
on cleft palate. Cleft Palate J. 1990;27:294–300.
Clarke JP. Abiku. In: Senanu KE, Vincent T, eds. A Selection of African
Poetry. London: Longman; 1976:189–193.
Dagher D, Ross E. Approaches of South African traditional healers
regarding the treatment of cleft lip and palate. Cleft Palate Craniofac J.
2004;41:461–469.
Gupta B. Incidence of congenital malformations in Nigerian children.
West Afr Med J Niger Pract. 1969;18:22–27.
Iregbulem LM. The incidence of cleft lip and palate in Nigeria. Cleft
Palate J. 1982;19:201–205.
Louw B. Culture. In: Eloff I, Ebersohn L, eds. Keys to Educational
Psychology. Cape Town: UCT Press; 2004:258–271.
Meremikwo MM, Ehiri JE, Nkanga DG, Udoh EE, Ikpatt OF, Alaje EO.
Socioeconomic constraints to effective management of Burkitt’s lym-
phoma in south-eastern Nigeria. Trop Med Int Health. 2005;10:92–98.
Obuekwe O, Akapata O. Pattern of cleft lip and palate [corrected] in
Benin City, Nigeria. Cent Afr J Med. 2004;50:65–69.
Olasoji HO, Ugboko VI, Arotiba GT. Cultural and religious components
in Nigerian parents’ perceptions of the etiology of cleft lip and palate:
implications for treatment and rehabilitation. Br J Oral Maxillofac
Surg. 2007;45:302–305.
Patel Z, Ross E. Reflections on the cleft experience by South Africans
adults: use of qualitative methodology. Cleft Palate Craniofac J.
2003;40:471–480.
Strauss RP. Culture, rehabilitation and facial birth defects: international
case studies. Cleft Palate J. 1985;22:56–62.
Uzochukwu BSC, Onwujekwe OE. Socio-economic differences and health
seeking behavior for the diagnosis and treatment of malaria: a case
study of four local government areas operating the Bamako initiative
program in south-east Nigeria. Int J Equity Health. 2004;3:6–15.
Weatherley-White RC, Eiserman W, Beddoe M, Vanderberg R. Percep-
tions, expectations, and reactions to cleft lip and palate surgery in
native populations: a pilot study in rural India. Cleft Palate
Craniofac J. 2005;42:560–564.
Oginni et al., KNOWLEDGE AND CULTURAL BELIEFS ABOUT OROFACIAL CLEFTS 333
APPENDIX A
(QUESTIONNAIRE)
SECTION A
1. TRIBE:
2. STATE OF ORIGIN:
3. AGE: [,15yrs] [16–20] [21–30] [31–40] [41–50] [51–60]
[.61]
4. GENDER: [MALE] [FEMALE]
5. EDUC. ATTAINMENT: [Nil] [Pry] [Sec.] [Ordinary Na-
tional Diploma] [Higher National Diploma] [BSc/BA]
[MSc] [PhD] [Others] (Please indicate ……………
……………………………………………….)
6. MARITAL STATUS: [Married] [Single] [Divorced] [Widow]
7. OCCUPATION:
SECTION B
1a. Have you ever seen a child or an individual
like this? [Yes] [No]
B. If Yes to 1a above, whose child or children?
C. What was done for the child / children?
………………
…………………………………………..
2. In your opinion what is responsible for this?
3. What are the beliefs about this condition in
your culture or how does your culture explain
this occurrence?
4. What can be done to help someone in this
condition?
5. Other Remarks
APPENDIX A
(QUESTIONNAIRE)
SECTION A
1. TRIBE:
2. STATE OF ORIGIN:
3. AGE: [,15yrs] [16–20] [21–30] [31–40] [41–50] [51–60] [.61]
4. GENDER: [MALE] [FEMALE]
5. EDUC. ATTAINMENT: [Nil] [Pry] [Sec.] [Ordinary National Diploma] [Higher National Diploma] [BSc/BA] [MSc] [PhD]
[Others] (Please indicate …………………………………………………………….)
6. MARITAL STATUS: [Married] [Single] [Divorced] [Widow]
7. OCCUPATION:
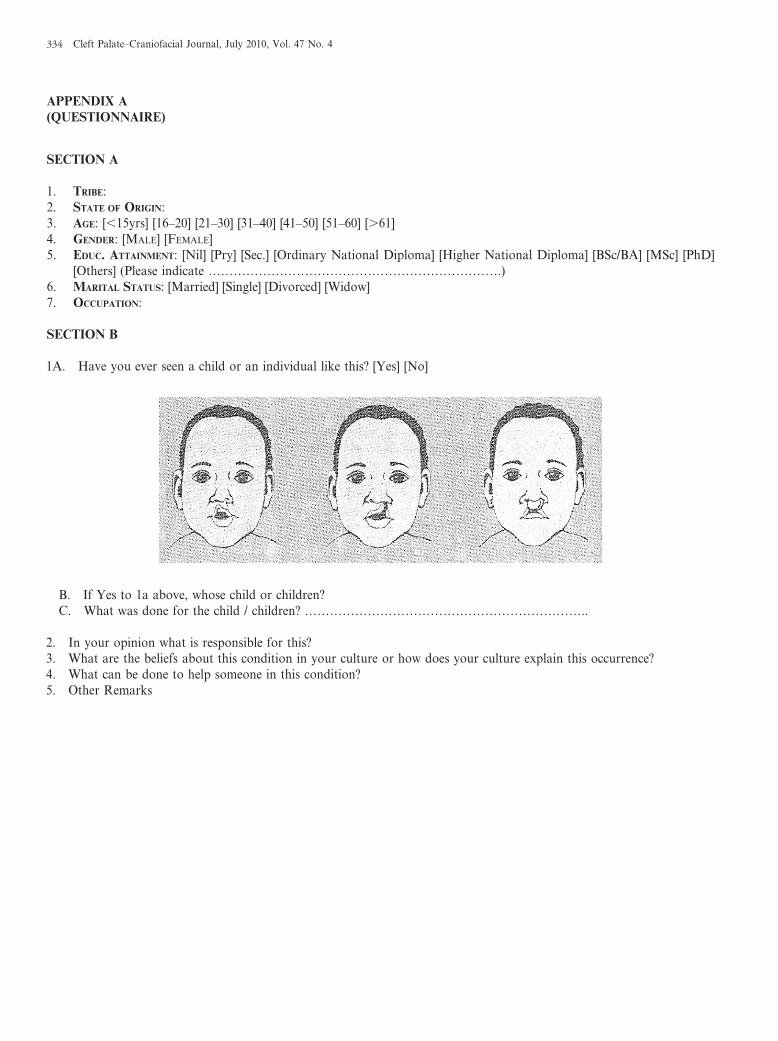
SECTION B
1A. Have you ever seen a child or an individual like this? [Yes] [No]
B. If Yes to 1a above, whose child or children?
C. What was done for the child / children? …………………………………………………………..
2. In your opinion what is responsible for this?3. What are the beliefs about this condition in your culture or how does your culture explain this occurrence?
4. What can be done to help someone in this condition?
5. Other Remarks
334 Cleft Palate–Craniofacial Journal, July 2010, Vol. 47 No. 4
Recommended

















