1998;65:1331-1334 Ann Thorac SurgVassilios Gulielmos, Michael Knaut, Florian M. Wagner and Stephan Schüler
Artery DiseaseMinimally Invasive Surgical Technique for the Treatment of Multivessel Coronary
http://ats.ctsnetjournals.org/cgi/content/full/65/5/1331located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 1998 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from
Minimally Invasive Surgical Technique for theTreatment of Multivessel Coronary Artery DiseaseVassilios Gulielmos, MD, Michael Knaut, MD, Florian M. Wagner, MD, andStephan Schuler, MDCardiovascular Institute, University Hospital Dresden, Dresden, Germany
Background. To avoid sternotomy-related complica-tions after cardiac operations, we developed a minimallyinvasive surgical technique for the treatment of multives-sel coronary artery disease.
Methods. From November 1996 to May 1997, 39 patients(age range, 50 to 78 years) with coronary artery diseasewere treated with the use of this technique. Through asmall (6- to 9-cm) left lateral chest incision in the thirdintercostal space, the left internal mammary artery washarvested directly. With the use of cardiopulmonarybypass and cardioplegic arrest in all patients except 1, theleft internal mammary artery was anastomosed to the leftanterior descending artery. In addition, vein grafts and
other arterial conduits were used for revascularization ofthe other coronary arteries.
Results. There were no intraoperative complications.All the patients survived the procedure and had anuneventful postoperative course. Wound complicationsoccurred in 2 patients. The median (6 standard error ofthe mean) hospital stay was 6 6 1 days.
Conclusions. This technique combines minimally inva-sive surgical conditions with the safety standards ofroutine cardiac operations. With the use of this approach,even extensive coronary artery disease can be treated.
(Ann Thorac Surg 1998;65:1331–4)© 1998 by The Society of Thoracic Surgeons
The successful treatment of single-vessel coronaryartery disease (CAD) using a minimally invasive
surgical approach has been reported recently [1–4]. Ourexperience with this technique started with a Port-Accesssystem (Heartport, Redwood City, CA) included suchsafety standards of cardiac operation as cardiopulmonarybypass and cardioplegic arrest. The technique was intro-duced successfully at our institution in March 1996. Theresults of our first series of 42 patients were very encour-aging, but the technique was limited to patients withsingle-vessel disease [5, 6]. There was a significant risk ofvascular complications with the use of femoral arterialcannulation and the endoaortic occlusion catheter. Fur-ther, Port-Access technology did not allow access to theascending aorta for the attachment of proximal vein graftanastomoses. Therefore, another surgical technique wasdeveloped to avoid sternotomy-related complications[7–14], femoral arterial cannulation, and the use of theendoaortic occlusion catheter. In addition, it allowed thetreatment of triple-vessel disease with the use of the leftinternal mammary artery (LIMA) and additional veingrafts and other arterial conduits when necessary.
Patients and Methods
PatientsBetween October 1996 and May 1997, this minimallyinvasive surgical technique was used in 39 consecutivelytreated patients. The patients ranged in age from 50 to 78
years (median, 66 years). There were 6 women and 33men. The exclusion criteria for this procedure wereobesity (ie, a body mass index of greater than 1.30) andimpaired left ventricular function (ie, a left ventricularejection fraction of less than 0.40). Patients with signifi-cant arteriosclerotic lesions of the aorta on ultrasono-graphic examination also were excluded.
Eight patients had single-vessel disease (stenosis of theleft anterior descending artery [LAD] and the diagonalbranch), 19 patients had double-vessel disease (including6 with significant mainstem stenosis), 8 patients hadstenosis of the LAD and the left circumflex artery, 1patient had stenosis of the LAD and the intermediatebranch of the left circumflex artery, and 4 patients hadsignificant lesions of the LAD and the right coronaryartery (Table 1). Twelve patients had triple-vessel dis-ease.
Surgical TechniqueThe patient was placed in the supine position with arubber cushion under the left shoulder. A single-lumenairway tube was used for double-lung ventilation. A 6- to9-cm skin incision was made at the level of the thirdintercostal space (Fig 1) and the sternal edges of the thirdand fourth ribs were divided but not removed. Theintercostal muscles were divided further laterally under-neath the skin to avoid postoperative pain caused byspreading of the intercostal nerves. Thus, an operativefield measuring 6 by 5 cm was achieved. Even in women,the surgical gate provided no problems because thebreast was pulled caudally using tapes.
With the use of a small wound retractor, the LIMA was
Accepted for publication Dec 23, 1997.
Address reprint requests to Dr Schuler, Cardiovascular Institute, Univer-sity Hospital Dresden, Fetscherstrasse 76, D-01307 Dresden, Germany.
© 1998 by The Society of Thoracic Surgeons 0003-4975/98/$19.00Published by Elsevier Science Inc PII S0003-4975(98)00159-3
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from
harvested as a pedicle through the incision up to the firstand down to the sixth ribs and then divided distally.Mediastinal fat was dissected, the pericardium wasopened toward the ascending aorta, and stay sutureswere placed between the pericardium and the woundsoft tissue to retract the ascending aorta toward the chestincision. During harvest of the LIMA, saphenous veinsegments also were harvested. The ascending aorta wasdissected from the pulmonary trunk. After cannulation ofthe femoral vein and ascending aorta, cardiopulmonarybypass was begun. In 1 patient, the right atrium wascannulated using a two-stage cannula (Fig 2).
The ascending aorta was cross-clamped and cold an-tegrade crystalloid cardioplegia was delivered through astandard cardioplegic cannula. During cardioplegic ar-rest, aortic root venting was performed. Exposure of allcoronary arteries was facilitated by rotating the heart 45degrees for the right coronary artery and 60 degrees forthe marginal branch of the left circumflex artery in allcases. An end-to-side anastomosis was performed be-tween the vein graft and the coronary arteries in a
standard fashion (Fig 3), followed by anastomosis of theLIMA to the LAD (Fig 4).
In 1 patient, total arterial revascularization was per-formed using the left and right internal thoracic mam-mary arteries. The right internal mammary artery washarvested thoracoscopically through the left-sided chestincision. The LIMA was used as a conduit for the LADand the right internal mammary artery was attached tothe intermediate branch. The proximal end of the rightinternal mammary artery was anastomosed end-to-sideas a “T-graft” to the LIMA (Fig 5).
After standard removal of air from the heart, the aorticcross-clamp was removed and the proximal ends of thevein grafts were attached end-to-side to the ascendingaorta (Fig 6). After the placement of temporary pace-maker wires, the patient was weaned from cardiopulmo-nary bypass. The sternal edges of the third and fourthribs were attached to the sternal border with two steel
Table 1. Distribution of Coronary Artery Disease in theStudy Population (n 5 39)
Affected Vessel(s)No. of
Patients
LAD and diagonal branch 8LAD and intermediate branch 1LAD and left circumflex artery 8Mainstem 6LAD and right coronary artery 4LAD, right coronary artery, and intermediate
branch1
LAD, left circumflex artery, and right coronaryartery
11
LAD 5 left anterior descending artery.
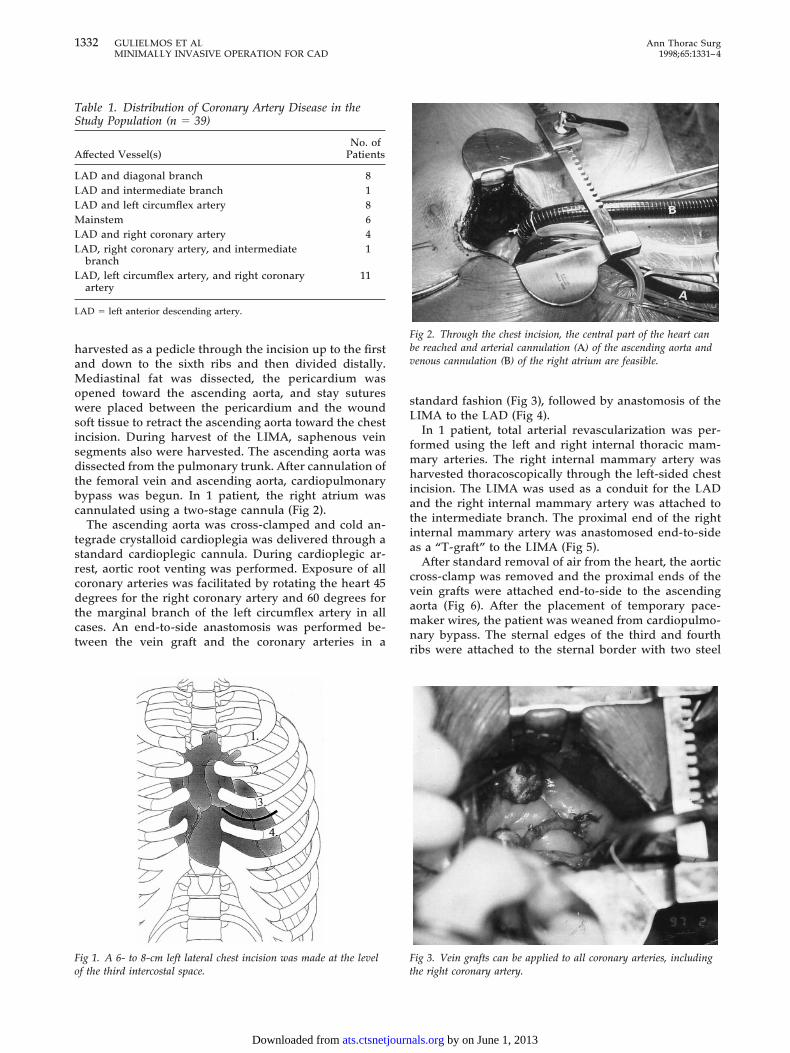
Fig 1. A 6- to 8-cm left lateral chest incision was made at the levelof the third intercostal space.
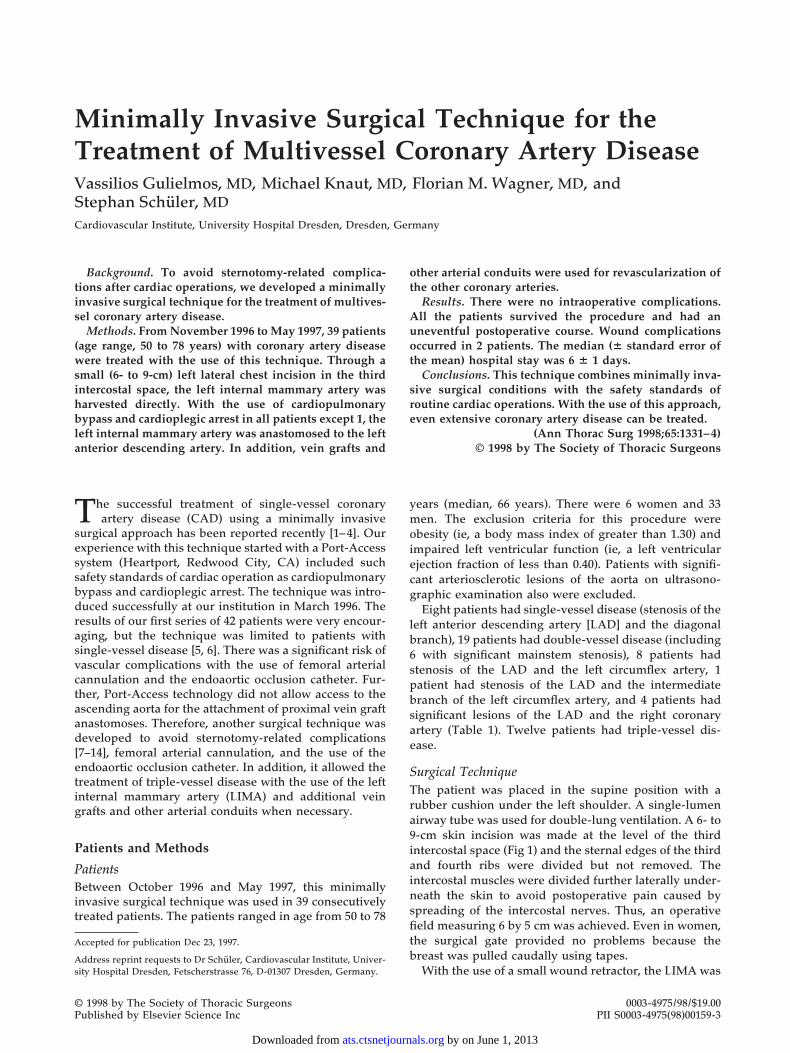
Fig 2. Through the chest incision, the central part of the heart canbe reached and arterial cannulation (A) of the ascending aorta andvenous cannulation (B) of the right atrium are feasible.
Fig 3. Vein grafts can be applied to all coronary arteries, includingthe right coronary artery.
1332 GULIELMOS ET AL Ann Thorac SurgMINIMALLY INVASIVE OPERATION FOR CAD 1998;65:1331–4
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from
wires. The attachment of the ribs still left a certain gapbetween two ribs. To avoid future herniation, the two ribswere approximated further using a 1-mm polydioxanonesuture. Two chest tubes were left in place and the chestincision was closed in layers (Fig 7).
Results
All patients survived the procedure and were weanedfrom cardiopulmonary bypass without inotropic supportin sinus rhythm and with no signs of ischemia. Conver-sion to a median sternotomy was not necessary in anypatient. A total of 39 LIMA anastomoses and 48 veingrafts were performed. The coronary vessels that weregrafted are listed in Table 2.
In 1 patient, the LIMA was discovered to have severearteriosclerotic lesions during harvesting and a vein grafthad to be applied to the LAD. In another patient, theLIMA was used as a free graft to the LAD because of asevere stenotic lesion of the left subclavian artery.
Postoperative complications included delayed woundhealing of the groin in 1 patient, wound infection of thechest incision in 1 patient, and a lymphatic fistula in 1
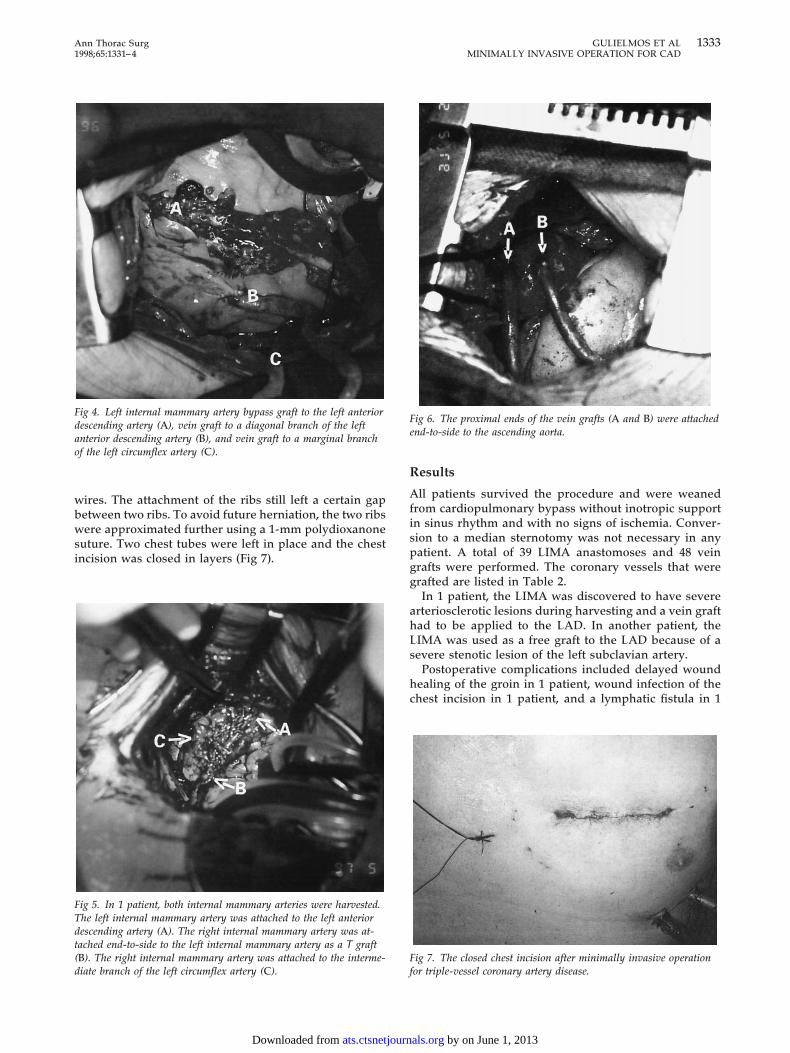
Fig 4. Left internal mammary artery bypass graft to the left anteriordescending artery (A), vein graft to a diagonal branch of the leftanterior descending artery (B), and vein graft to a marginal branchof the left circumflex artery (C).
Fig 5. In 1 patient, both internal mammary arteries were harvested.The left internal mammary artery was attached to the left anteriordescending artery (A). The right internal mammary artery was at-tached end-to-side to the left internal mammary artery as a T graft(B). The right internal mammary artery was attached to the interme-diate branch of the left circumflex artery (C).
Fig 6. The proximal ends of the vein grafts (A and B) were attachedend-to-side to the ascending aorta.
Fig 7. The closed chest incision after minimally invasive operationfor triple-vessel coronary artery disease.
1333Ann Thorac Surg GULIELMOS ET AL1998;65:1331–4 MINIMALLY INVASIVE OPERATION FOR CAD
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from

patient. The median (6 standard error of the mean)postoperative hospital stay was 6 6 1 days (Table 3). At 12weeks’ follow-up, no patient had signs of ischemia onstress electrocardiography and only 1 patient had painwith exercise on pain assessment. All patients except the1 with the wound infection were pleased with the cos-metic results of their operation.
Comment
This surgical technique allows the complete treatment ofmultivessel CAD under minimally invasive surgical con-ditions with the use of current surgical standards such ascardiopulmonary bypass, cardioplegic arrest, use of the
LIMA as a conduit for the LAD, and use of vein grafts orother arterial conduits for the revascularization of othercoronary arteries. Harvesting of the LIMA is performedthrough the chest incision without the need for addi-tional ports. This incision, made in the third intercostalspace, also allows good access to the ascending aorta.Moving the chest incision from the fourth intercostalspace to the third intercostal space enables access to thecentral part of the heart, allowing for cannulation of theascending aorta, the application of cardioplegia, andvolume unloading of the left ventricle. Furthermore,proximal vein grafts can be attached to the ascendingaorta. Cardioplegic arrest allows complete access to allareas of the heart. In some cases, even cannulation of theright atrium using a two-stage cannula is possible. Withthis minimally invasive surgical technique, completerevascularization is feasible in patients with extensivecoronary artery disease with the standards of safety ofregular coronary artery bypass grafting and the ability touse the LIMA and other arterial conduits.
References
1. Benetti FJ, Ballester C, Sani G, Boonstra P, Grandjean J.Video assisted coronary bypass surgery. J Card Surg 1995;10:620–5.
2. Acuff TE, Landreneau RJ, Griffith BP, Mack MJ. Minimallyinvasive coronary artery bypass grafting. Ann Thorac Surg1996;61:135–7.
3. Calafiore AM, De Giammarco G, Teodori G, et al. Leftanterior descending coronary artery grafting via left anteriorsmall thoracotomy without cardiopulmonary bypass. AnnThorac Surg 1996;61:1658–65.
4. Diegeler A, Falk V, Walther T, Mohr FW. Minimally invasivecoronary artery bypass surgery without extracorporeal cir-culation. N Engl J Med 1997;336:1454–5.
5. Reichenspurner H, Gulielmos V, Daniel WG, Schueler S.Minimally invasive coronary artery bypass (CABS) with thesafety of cardiopulmonary bypass and cardioplegic arrest.N Engl J Med 1997;336:67–8.
6. Stevens JH, Burdon TA, Peters WS, et al. Port-Access coro-nary artery bypass grafting: a proposed surgical method.J Thorac Cardiovasc Surg 1996;111:567–73.
7. Weinzweig N, Yetman R. Transposition of the greater omen-tum for recalcitrant median sternotomy wound infections.Ann Plast Surg 1995;43:471–7.
8. Zacharias A, Habib RH. Factors predisposing to mediansternotomy complications. Deep vs superficial infection.Chest 1996;110:1173–8.
9. Moore R, Follette DM, Berkoff HA. Poststernotomy fracturesand pain management in open cardiac surgery. Chest 1994;106:1339–42.
10. Casscells CD, Lindsey RW, Ebersole J, Li B. Ulnar neuropa-thy after median sternotomy. Clin Orthop 1993;291:259–63.
11. Bryan AJ, Lamarra M, Angelini GD, West RR, BreckenridgeIM. Median sternotomy wound dehiscence: a retrospectivecase control study of risk factors and outcome. J R Coll SurgEdinb 1992;37:305–8.
12. Furnary AP, Magovern JA, Simpson KA, Magovern GJ.Prolonged open sternotomy and delayed sternal closureafter cardiac operations. Ann Thorac Surg 1992;54:233–9.
13. Hanson MR, Breuer AC, Furlan AJ, et al. Mechanism andfrequency of brachial plexus injury in open heart surgery: aprospective analysis. Ann Thorac Surg 1983;36:675–9.
14. Merchant RN, Brown WF, Watson BV. Peripheral nerveinjuries in cardiac anesthesia. Can J Anaesth 1990;37:152.
Table 2. Distribution of LIMA and Vein Graft AnastomosesAccording to the Pattern of Coronary Artery Disease
Anastomoses PerformedNo. of
Patients
LIMA (LAD) 2LIMA (LAD) 1 vein graft (right coronary artery) 3LIMA (LAD) 1 vein graft (marginal branch of
left circumflex artery)9
LIMA (LAD) 1 vein graft (intermediate branch) 3LIMA (LAD) 1 vein graft (diagonal branch) 7LIMA (LAD) 1 vein graft (left circumflex artery) 1LIMA (LAD) 1 vein graft (right coronary artery)
1 vein graft (marginal branch of leftcircumflex artery)
6
LIMA (LAD) 1 vein graft (marginal branch ofleft circumflex artery) 1 vein graft (diagonalbranch)
5
LIMA (LAD) 1 right internal mammary artery“T-graft” (intermediate branch)
1
LIMA (LAD) 1 vein graft (marginal branch ofleft circumflex artery) 1 vein graft(intermediate branch)
1
LIMA-“free-graft” (LAD) 1 vein graft(intermediate branch)
1
LAD 5 left anterior descending artery; LIMA 5 left internal mam-mary artery.
Table 3. Intraoperative and Postoperative Data for 39Patients Undergoing a Minimally Invasive Cardiac SurgicalTechniquea
Parameter
AllPatients(n 5 39)
Last 10Patients
Duration of operation (min) 270 6 48 230 6 30LIMA takedown time (min) 49 6 21 28 6 7Duration of CPB (min) 97 6 32 95 6 29Duration of aortic occlusion (min) 50 6 13 48 6 11Ventilation time (min) 580 6 181 505 6 152ICU stay (days) 1 6 0 1 6 0Hospital stay (days) 6 6 1 3 6 2
a Values given are the median plus or minus the standard error of themean.
CPB 5 cardiopulmonary bypass; ICU 5 intensive care unit; LIMA 5left internal mammary artery.
1334 GULIELMOS ET AL Ann Thorac SurgMINIMALLY INVASIVE OPERATION FOR CAD 1998;65:1331–4
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from
1998;65:1331-1334 Ann Thorac SurgVassilios Gulielmos, Michael Knaut, Florian M. Wagner and Stephan Schüler
Artery DiseaseMinimally Invasive Surgical Technique for the Treatment of Multivessel Coronary
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/65/5/1331including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/65/5/1331#BIBL
This article cites 14 articles, 5 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/65/5/1331#otherarticleThis article has been cited by 9 HighWire-hosted articles:
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 1, 2013 ats.ctsnetjournals.orgDownloaded from
Recommended

















