
Available online at www.sciencedirect.com
(2009) 448–454
Clinical Biochemistry 42The urinary steroid profile in patients diagnosed with adrenal incidentaloma
Alicja Kotłowska a,b, Edmund Maliński a, Krzysztof Sworczak c,Jolanta Kumirska a, Piotr Stepnowski a,⁎
a Department of Environmental Analysis, Faculty of Chemistry, University of Gdańsk, Sobieskiego 18, 80-952 Gdańsk, Polandb Department of Inorganic Chemistry, Faculty of Pharmacy, Medical University of Gdańsk, Al. Gen. J. Hallera 107, 80-416 Gdańsk, Polandc Department of Endocrinology and Internal Medicine, Medical University of Gdańsk, M. Curie-Skłodowskiej 3a, 80-210 Gdańsk, Poland
Received 27 May 2008; received in revised form 12 December 2008; accepted 29 December 2008Available online 18 January 2009
Abstract
Objective: The aim of this study was to investigate the possible urinary markers of hormonal activity in patients with non-functioning adrenalincidentalomas. In order to evaluate the endocrine activity of forementioned tumours, urinary steroid metabolite levels were analyzed in samplesfrom patients and controls. Possible blocks in metabolic pathways of the examined hormones were determined by comparing selected urinarysteroid metabolite sums and ratios in both groups of interest.
Design: Urine samples were collected from 20 patients with non-functioning adrenal incidentalomas and from 25 controls matched in terms ofage, sex and BMI. Excretion of 19 major urinary steroid metabolites was analyzed by gas chromatography. The results were subjected to statisticalanalysis.
Results: In patients with adrenal incidentalomas sum of total urinary cortisol metabolites was significantly increased in respect to the controlgroup. We also observed a shift towards tetrahydrocorticosterone, cortisol and etiocholanolone production in patients. No significant differences inproduction of other urinary steroid metabolites were noted in patients with adrenal incidentalomas in respect to control group.
Conclusions: Our data suggests that not only urinary free cortisol but also its metabolite such as tetrahydrocortisol and other steroids includingetiocholanolone and corticosterone tetrahydrometabolite might be urinary markers for the endocrine activity of adrenal incidentalomas. Enhancedlevels of these urinary steroid metabolites indicate an impairment of 11β-hydroxysteroid dehydrogenase activity and slightly increased activity of5β-reductase in patients with adrenal incidentalomas.© 2009 The Canadian Society of Clinical Chemists. Published by Elsevier Inc. All rights reserved.
Keywords: Adrenal incidentaloma; Urinary steroids; Gas chromatography; 11β-hydroxysteroid dehydrogenase; 5β-reductase; Tetrahydrocortisol
Introduction
Adrenal incidentalomas (AIs) are adrenal tumours inciden-tally detected with very high frequency (4–10%) duringimaging procedures such as computed tomography (CT),magnetic resonance (MRI) or ultrasonography [1–3]. Thediscovery of these masses is not preceded by symptoms ofclinical nature or any signs of adrenal disease. AIs prevail withincreasing age and are most often found in individuals over50 years old. The majority of these tumours are benign andhormonally inactive and only a small number of patients requiresurgical removal of AIs [4,5]. Some of incidentalomas are
⁎ Corresponding author. Fax: +48 58 5235 572.E-mail address: [email protected] (P. Stepnowski).
0009-9120/$ - see front matter © 2009 The Canadian Society of Clinical Chemistsdoi:10.1016/j.clinbiochem.2008.12.027
pheochromocytomas and others are responsible for hypersecre-tion of cortisol or aldosterone. However, additional examinationmay reveal the presence of adrenal cortex carcinomas which arerare but malignant and therefore surgical intervention hasalways to be taken into consideration.
The majority of hormonal assessments are based onevaluation of adrenal glucocorticoid secretion by measuringserum cortisol after dexamethasone (DXM) suppression testsand on determination of urinary free cortisol (UFC) level whichis commonly examined in 24-h urine [6,7]. Androgen excretionis investigated by measuring the concentration of dehydroe-piandrosterone sulfate (DHEA-S) in serum, although thismethod might be questionable in discrimination of malignantfrom benign mass. The tests for UFC carried out on 24-h urineoften prove to be insufficiently sensitive to recognize mild
. Published by Elsevier Inc. All rights reserved.

449A. Kotłowska et al. / Clinical Biochemistry 42 (2009) 448–454
steroid overproduction and the patients are diagnosed with non-functional incidentalomas [8,9].
In this study urinary steroid excretion has been compared inpatients with non-functioning adrenal incidentalomas toexamine whether these tumours are hypersecretive. An attemptwas also made to evaluate which urinary steroid metabolitescould serve as urinary markers of endocrine activity of adrenalincidentalomas. Furthermore, enzymatic efficiencies of certainenzymes involved in metabolic pathways of steroids weredetermined by calculating the sums and ratios of urinary steroidmetabolites in patients with AIs and controls.
Materials and methods
Subjects
24-h urine collections were obtained from 25 controls (3 menand 22 women) as well as 20 patients (2 men and 20 women)diagnosed with adrenal incidentalomas. Both groups werematched according to age, sex and BMI. All investigatedindividuals were minimum 40 years of age. The subjects withadrenal incidentaloma were outpatients of Department ofEndocrinology and Internal Medicine of Medical Universityof Gdańsk and were not treated with any steroid-likemedications. Laboratory evaluation of endocrine activity ofadrenal incidentalomas indicated that the masses were ‘hor-monally silent’ (non-hypersecretory). The examination wasbased on the determination of UFC in 24-h urine and serumcortisol levels after suppression test with DXM using immuno-fluorescent assay. The concentration of cortisol in serum ofpatients with AIs after DXM suppression test did not exceed140 nmol/L what suggested that none of the patients sufferedfrom pre-Cushing's syndrome (PCS). DHEA-S level in serumas well as aldosterone level in serum and urine were determinedby radioimmunoassay. The levels of potassium in blood and thelevel of methoxycatecholamines in 24-h urine were alsoinvestigated. The diameter of incidentalomas did not exceed4 cm (larger masses were surgically removed). Imagingprocedures were repeated every 12 months to monitor tumourgrowth. Adrenal cancer was excluded by taking into considera-tion the diameter of the tumour, its clinical image and theproperties revealed during additional examination. None of thepatients suffered from congenital adrenal hyperplasia (CAH).The control subjects underwent screening procedures such asultrasonography in order to eliminate the possibility of adrenaltumours. The studies were in compliance with the Local EthicalCommittee from Medical University of Gdańsk.
Extraction
A 10 mL aliquot obtained from each urine sample was spikedwith two internal standards: methyltestosterone and predniso-lone (Sigma) and extracted using two Sep-pak C18 cartridges(JT Baker, Bakerbond). The cartridges were primedwith 6mL ofmethanol and 6 mL of distilled water, after loading the sample,the Sep-paks were washed with 5 mL distilled water. Free andconjugated steroids were eluted with 6 mL of methanol.
Hydrolysis
The extracts from each urine sample were combined and thesolvent was evaporated to dryness in vacuo and using stream ofdry nitrogen. The residuewas dissolved in 10mLof acetate buffer(pH 5.2) to which 7500 U of glucuronidase/arylsulfatase fromHelix Pomatia (Sigma) were added. The enzymatic hydrolysiswas carried out overnight at 37 °C. Steroids were extracted usingthe procedure described above, solvent was evaporated.
Derivatization
The residue was dissolved in 100 μL of pyridine (POCh) and2 mg of methoxyloamine hydrochloride (Sigma) was added.The mixture was incubated for 2 h at 60 °C, afterwards thesolvent was evaporated in stream of nitrogen. Next, 85 μL ofTMSIM (POCh) and 15 μL of BSTFA:TMCS (Sigma) reagentmixture were added. The derivatization was carried outovernight at 110 °C producing methyloxime-trimethylsilylethers (MO-TMS).
Chromatography
Gas chromatography analyses were performed on Carlo Erba8000 TOP gas chromatograph equipped with flame ionizationdetector. The capillary column used for separations was30 m×0.25 mm×0.25 μm SolGel-1ms (SGE). The temperatureprogram was: initial temperature 150 °C was increased to200 °C at 4 °C/min, next it was increased to 320 °C at 1 °C/minand held for 30 min. The injector temperature was 310 °C andthe detector was 320 °C. Compounds were quantified on thebase of peak areas.
Excretion of 19 major urinary steroids was analyzed insamples from controls and patients. The following 19 majorurinary steroid metabolites including: androsterone (A),etiocholanolone (Et), 11-keto-androsterone (11-OA), 11-hydroxy-androsterone (11-OHA), 11-hydroxy-etiocholanolone(11-OHEt), pregnanetriol (PT), androstenetriol (Δ5-AT), tetra-hydro-11-deoxycortisol (THS), 11-keto-pregnanetriol (11-OPT),pregnenetriol (Δ5-PT), tetrahydrocortisone (THE), tetrahydro-11-dehydrocorticosterone (THA), tetrahydrocorticosterone(THB), allo-tetrahydrocorticosterone (aTHB), tetrahydrocortisol(THF), allo-tetrahydrocortisol (aTHF), α-cortolone (α-CL),β-cortolone (β-CL), α-cortol (α-C) and two internal standards:methyltestosterone (MT, IS1) as well as prednisolone (PR, IS2)were measured.
To assess the production rate of testosterone and andros-tendione metabolites the sum of A+Et was calculated. Totalcortisol metabolites production rate was estimated on the basisof the sum of THE, THF, aTHF, α-CL, β-CL and α-C. Relativeenzymatic activity of 5α-reductase was calculated using theratio of A/Et and aTHF/THF. The conversion of cortisol tocortisone was investigated by determination of the ratio of THE/(THF+aTHF) and enabled the evaluation of 11β-hydroxyster-oid dehydrogenase (11β-HSD) enzyme activity. Another testfor the activity of forementioned enzyme was performed on thebasis of (THB+aTHB/THA) ratio calculation.

Fig. 1. Separation of urinary steroids in a patient with adrenal incidentaloma by gas chromatography.
450 A. Kotłowska et al. / Clinical Biochemistry 42 (2009) 448–454
EvaluationKolgomorov–Smirnov normality test was used to investigate
the distribution of examined steroid metabolites. Statisticalevaluation of the values with Gaussian distribution wasperformed with two-tailed Student's t-test, otherwise Mann–Whitney test was applied. Statistical analysis was carried outusing Microsoft Excel and Statsoft Statistica. As the level ofsignificance, pb0.05 was accepted.
Results
Chromatogram representing separation of urinary steroidmetabolites is shown in Fig. 1. Daily excretion values of
Fig. 2. Box-whisker diagram of urinary excretion of andr
androgen metabolites in patients with adrenal incidentalomasand controls are presented as a box-whisker diagram in Fig. 2and are also summarized in Table 1. The results indicate that inpatients with adrenal incidentalomas, etiocholanolone concen-tration was significantly increased (pb0.05) with respect tocontrol subjects. There were no significant differences inurinary androsterone (A), 11-keto-androsterone (11-OA), 11-hydroxy-androsterone (11-OHA), 11-hydroxy-etiocholanolone(11-OHEt) and androstenetriol (Δ5-AT) levels when comparingpatients with AIs and controls.
Daily excretion values of corticosterone and cortisolmetabolites as well as pregnane metabolites examined inpatients with adrenal incidentalomas and controls are depicted
ogen metabolites in controls and patients. *pb0.05.
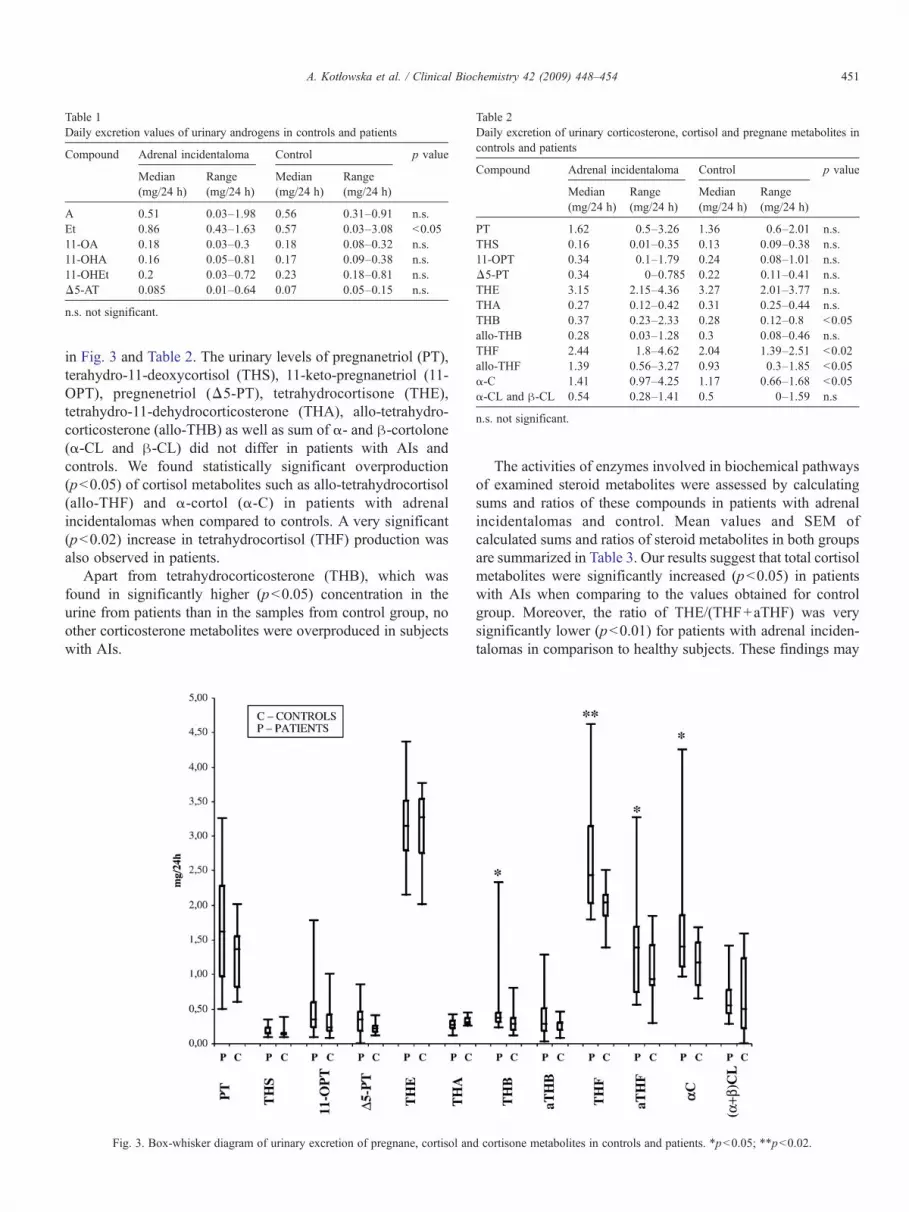
Table 1Daily excretion values of urinary androgens in controls and patients
Compound Adrenal incidentaloma Control p value
Median(mg/24 h)
Range(mg/24 h)
Median(mg/24 h)
Range(mg/24 h)
A 0.51 0.03–1.98 0.56 0.31–0.91 n.s.Et 0.86 0.43–1.63 0.57 0.03–3.08 b0.0511-OA 0.18 0.03–0.3 0.18 0.08–0.32 n.s.11-OHA 0.16 0.05–0.81 0.17 0.09–0.38 n.s.11-OHEt 0.2 0.03–0.72 0.23 0.18–0.81 n.s.Δ5-AT 0.085 0.01–0.64 0.07 0.05–0.15 n.s.
n.s. not significant.
Table 2Daily excretion of urinary corticosterone, cortisol and pregnane metabolites incontrols and patients
Compound Adrenal incidentaloma Control p value
Median(mg/24 h)
Range(mg/24 h)
Median(mg/24 h)
Range(mg/24 h)
PT 1.62 0.5–3.26 1.36 0.6–2.01 n.s.THS 0.16 0.01–0.35 0.13 0.09–0.38 n.s.11-OPT 0.34 0.1–1.79 0.24 0.08–1.01 n.s.Δ5-PT 0.34 0–0.785 0.22 0.11–0.41 n.s.THE 3.15 2.15–4.36 3.27 2.01–3.77 n.s.THA 0.27 0.12–0.42 0.31 0.25–0.44 n.s.THB 0.37 0.23–2.33 0.28 0.12–0.8 b0.05allo-THB 0.28 0.03–1.28 0.3 0.08–0.46 n.s.THF 2.44 1.8–4.62 2.04 1.39–2.51 b0.02allo-THF 1.39 0.56–3.27 0.93 0.3–1.85 b0.05α-C 1.41 0.97–4.25 1.17 0.66–1.68 b0.05α-CL and β-CL 0.54 0.28–1.41 0.5 0–1.59 n.s
n.s. not significant.
451A. Kotłowska et al. / Clinical Biochemistry 42 (2009) 448–454
in Fig. 3 and Table 2. The urinary levels of pregnanetriol (PT),terahydro-11-deoxycortisol (THS), 11-keto-pregnanetriol (11-OPT), pregnenetriol (Δ5-PT), tetrahydrocortisone (THE),tetrahydro-11-dehydrocorticosterone (THA), allo-tetrahydro-corticosterone (allo-THB) as well as sum of α- and β-cortolone(α-CL and β-CL) did not differ in patients with AIs andcontrols. We found statistically significant overproduction(pb0.05) of cortisol metabolites such as allo-tetrahydrocortisol(allo-THF) and α-cortol (α-C) in patients with adrenalincidentalomas when compared to controls. A very significant(pb0.02) increase in tetrahydrocortisol (THF) production wasalso observed in patients.
Apart from tetrahydrocorticosterone (THB), which wasfound in significantly higher (pb0.05) concentration in theurine from patients than in the samples from control group, noother corticosterone metabolites were overproduced in subjectswith AIs.
Fig. 3. Box-whisker diagram of urinary excretion of pregnane, cortisol an
The activities of enzymes involved in biochemical pathwaysof examined steroid metabolites were assessed by calculatingsums and ratios of these compounds in patients with adrenalincidentalomas and control. Mean values and SEM ofcalculated sums and ratios of steroid metabolites in both groupsare summarized in Table 3. Our results suggest that total cortisolmetabolites were significantly increased (pb0.05) in patientswith AIs when comparing to the values obtained for controlgroup. Moreover, the ratio of THE/(THF+aTHF) was verysignificantly lower (pb0.01) for patients with adrenal inciden-talomas in comparison to healthy subjects. These findings may
d cortisone metabolites in controls and patients. *pb0.05; **pb0.02.

Table 3Mean values±SEM of sums and ratios of excreted urinary steroids
Sums and ratiosof steroids
Adrenalincidentaloma
Control p value
Mean±SEM(mg/24 h)
Mean±SEM(mg/24 h)
A+Et 1.39±0.30 1.47±0.07 n.s.A/Et 0.86±0.09 0.72±0.06 n.s.Total cortisol metabolites 9.78±0.77 8.03±0.23 b0.05THE/(THF+aTHF) 0.84±0.04 1.06±0.07 b0.01aTHF/THF 0.54±0.06 0.54±0.04 n.s.(THB+aTHB)/THA 3.68±0.73 1.84±0.16 b0.01
n.s. not significant.SEM standard error of mean.
452 A. Kotłowska et al. / Clinical Biochemistry 42 (2009) 448–454
indicate that in patients with adrenal incidentalomas thereoccurs a possible shift towards cortisol metabolites productionand the reduction in the enzymatic activity of 11β-hydroxyster-oid dehydrogenase involved in cortisone synthesis. The valuesfor sum of A+Et, ratios of A/Et and ratio of aTHF/THF werecomparably similar and did not differ significantly in bothgroups of interest. Finally, the ratio of (THB+aTHB)/THAproved to be very significantly (pb0.01) higher in the samplesfrom patients with AIs than from controls. This observationsuggests enhanced activity of 11β-HSD in patients with adrenalincidentalomas.
Discussion
With the advance of noninvasive abdominal imagingtechniques, adrenal incidentalomas have become a commonproblem in clinical endocrinology [10]. 2–20% of patients arediagnosed with hormonally active tumours [11,12] which areoften responsible for excessive cortisol production manifestingitself as Cushing's syndrome. In most cases these masses are
Fig. 4. Metabolic pathway of co
classified as non-functional incidentalomas (NFI) and are notresponsible for hypersecretion of steroidal hormones orcatecholamines. However, it is possible, that the majority ofso-called NFIs overproduce hormones in an amount which isinsufficient to be measured by conventional methods andtherefore are not classified as functional [13,14]. In many ofthese cases patients suffer from pre-clinical Cushing's syn-drome and hypersecrete cortisol in a subtle way [15].
In case of urinary hormonal evaluation of the activity ofadrenal incidentalomas, UFC is taken into consideration andsince this method may be not sensitive enough to determinesubclinical hypercortisolism [16,17], we decided to examinemore informative indicators of daily cortisol production. Inorder to achieve this, urinary steroid profiling applying gaschromatography was carried out using samples from patientswith so-called non-functioning incidentalomas.
In clinical diagnostics urinary steroid profiling usually servesas a useful tool in giving clues of malignancy and adrenalcancer. Moreover, urinary steroid profiles can provide informa-tion about signs of recurrence by comparing the profile frompost-surgery sample to pre-surgery one. However, in our studywe concentrated on finding possible urinary steroid metabolitemarkers which would enable the identification of theendocrine activity of non-functioning adrenal incidentalomas.Our data revealed that the urinary levels of cortisol metabolitessuch as tetrahydrocortisol and α-cortol were significantlyincreased in the patients with AIs in comparison to controlgroup. These findings may suggest that both the decreasedurinary ratio of THE/(THF+aTHF) as well as the shifttowards cortisol metabolites production could be the result ofimpaired conversion of cortisol to cortisone. The interconver-sion is carried out by two isoenzymes of the 11β-hydroxysteroid dehydrogenase (11β-HSD) (Fig. 4) [18,19].Type 1 isoenzyme mainly serves the function of a reductase byconverting keto-glucocorticosteroids such as cortisone (E) or
rtisol (F) and cortisone (E).

453A. Kotłowska et al. / Clinical Biochemistry 42 (2009) 448–454
11-dehydrocorticosterone into biologically active 11β-hydroxy-glucocorticosteroids such as cortisol (F) or corticos-terone (B). Due to these properties the enzyme regulates theaccess and binding of the forementioned compounds to theirreceptors [20–22]. Type 2 of 11β-HSD acts as a dehydro-genase catalyzing the reverse reaction resulting in theconversion of active into inactive compounds [23]. Thedecrease in the conversion rate of cortisol to cortisone couldbe the effect of impaired activity of either type 1 or type 2 ofthe enzyme. Similar conclusions were drawn by Fuster et al.[24] who reported that apparent mineralocorticoid excess canbe caused by the absence of 11β-HSD2. To add, it was alsostated by Reincke et al. [25] that 11β-hydroxylase deficiencymay be involved in adrenal tumourgenesis. The fact thatexcessive level of tetrahydrocorticosterone was present and theratio of (THB+aTHB)/THA was significantly increased inurine samples from patients with AIs implies another piece ofevidence supporting the hypothesis that the impairment ofactivity of 11β-hydroxylase might occur in case of adrenalincidentalomas. The association of altered urinary ratio oftetrahydrocorticosterone/tetrahydro-11-dehydrocorticosteroneand reduced renal activity of 11β-HSD2 has also beenreported by Vogt et al. [20] who investigated the activity ofthe enzyme in experimental nephrotic syndrome.
The connection between altered urinary levels of cortisolmetabolites and defective activity of 11β-hydroxysteroiddehydrogenase was also reported by numerous authors in caseof patients suffering from congenital adrenal hyperplasia. It isworth mentioning that subjects diagnosed with CAH present anincreased risk of adrenal tumours and sometimes adrenaltumours might be caused by 21-hydroxylase deficiency or 11β-hydroxylase deficiency [26]. In cases of congenital adrenalhyperplasia due to 11β-hydroxylase deficiency patients areunable to convert 11-deoxycortisol to cortisol. If the illness isdue to 21-hydroxylase deficiency, 11-deoxycorticosteronecannot be converted to corticosterone, which later serves as aprecursor of aldosterone [27]. However, none of the examinedpatients with AIs was diagnosed with CAH. Moreover, ourstudy did not reveal elevated levels of 11-deoxycortisol or 11-deoxycorticosterone in urine samples of patients with AIs. Onthe contrary, the results indicated increased concentrations oftetrahydrometabolites of cortisol and corticosterone in thesamples from subjects with incidentalomas and these steroidswould not be produced in case of CAH due to 21-hydroxylasedeficiency or 11β-hydroxylase deficiency.
In majority of publications covering the subject of adrenalincidentalomas the attention is paid mainly to UFC examinationand therefore not much is know about possible abnormalitiesconcerning other urinary steroid metabolites production. Fullurinary hormonal profiling enabled us to investigate theproduction of major urinary androgen metabolites in samplesfrom patients with adrenal incidentalomas. Our results imply aslight overproduction of etiocholanolone in patients with AIs.This observation may be presumably related to increased 5β-reductase activity as it was shown by Vierhapper et al. [28]. Toadd, it has been suggested that the elevation of terahydrocortisolproduction may be connected to the increased 5β-reductase
activity in the liver [29,30]. However, we did not observestatistically significant differences in the ratios of aTHF/THF ofcontrol and patient groups that would indicate a strong shifttowards THF synthesis.
In conclusion, our findings indicate that not only UFC andserum cortisol levels after DXM suppression tests but alsotetrahydrocortisol, tetrahydrocorticosterone and etiocholano-lone must be taken into consideration during examination ofhormonal activity of AIs. As these compounds may serve therole of possible urinary markers of endocrine activity of adrenalincidentalomas, their investigation may be useful in revealingthe possible occurrence of pre-clinical Cushing's syndrome inpatients with so-called NFIs. Otherwise, evaluation of hormonalactivity of such incidentalomas basing only on determination ofUFC or serum cortisol after DXM suppression may lead tomisleading conclusions stating lack of hormonal activity ofthese tumours [31]. We propose that 11β-hydroxysteroiddehydrogenase type 2 deficiency as well as slightly enhancedactivity of 5β-reductase might play a vital role in the primaryhormonal defects in adrenal incidentaloma. However, bearing inmind the small number of experimental subjects, further studiesare required to understand the mechanism of 11β-hydroxyster-oid dehydrogenase and 5β-reductase action in case of adrenalincidentalomas and pre-clinical Cushing's syndrome.
Acknowledgment
Financial support was provided by the Polish Ministry ofEducation and Research under grant DS 8200-4-0085-8.
References
[1] Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. Theclinically inapparent adrenal mass: update in diagnosis and management.Endocr Rev 2004;25:309–40.
[2] Furtado CD, Aguirre DA, Sirlin CB, Dang D, Stamato SK, Lee P, et al.Whole-body CT screening: spectrum of findings and recommendations in1192 patients. Radiology 2005;237:385–94.
[3] Suzuki T, Kudoh S, Takahashi N. Management of adrenal incidentaloma inJapan. Biomed Pharmacother 2000;54:203–6.
[4] Arnaldi G, Masini AM, Giacchetti G, Taccaliti A, Faloia E, Mantero F.Adrenal incidentaloma. Br J Med Biol Res 2000;33:1177–89.
[5] Meyer A, Behrend M. Indications and results of surgery for incidentallyfound adrenal tumors. Urol Int 2006;77:173–8.
[6] Garrapa GM, Pantanetti P, Arnaldi G, Mantero F, Faloia E. Bodycomposition and metabolic features in women with adrenal incidentalomaor Cushing's syndrome. J Clin Endocrinol Metab 2001;86:5301–6.
[7] Valli N, Catargi B, Ronci N, Vergnot V, Leccia F, Ferriere JM, et al.Biochemical screening for subclinical cortisol-secreting adenomasamongst adrenal incidentalomas. Eur J Endocrinol 2003;144:401–8.
[8] Lavoix H, Lacroix A. Partially autonomous cortisol secretion by incidentallydiscovered adrenal adenoma. Trends Endocrinol Metab 1995;46:191–7.
[9] Reincke M. Subclinical Cushing's syndrome. Endocrinol Metab Clin NAm 2000;29:43–57.
[10] Copeland PM. The incidentally discovered adrenal mass. Ann Int Med1983;98:940–5.
[11] Favia G, Lumachi F, Basso S, D'Amico EE. Management of incidentallydiscovered adrenal masses and risk of malignancy. Surgery 2000;128:918–24.
[12] Barzon L, Fallo F, Sonino N, Boscaro M. Development of overt Cushing'ssyndrome in patients with adrenal incidentalomas. Eur J Endocrinol2002;146:61–6.

454 A. Kotłowska et al. / Clinical Biochemistry 42 (2009) 448–454
[13] McLeod M, Thompson N, Gross M, Bendeson AG, Bendeson L. Sub-clinical Cushing's syndrome in patients with adrenal gland incidentalomas.Pitfalls in diagnosis and management. Am Surg 1990;56:398–403.
[14] Bogner U, Eggens U, Hensen J, Oelkers W. Incidentally discoveredACTH-dependent adrenal adenoma presenting as “pre-Cushing's syn-drome”. Acta Endocrinol (Copenh) 1986;111:89–92.
[15] Terzolo M, Bovio S, Pia A, Osella G, Borretta G, Angeli A, et al.Subclinical Cushing's syndrome. Arq Bras Endocrinol Metab 2007;51:1272–9.
[16] Griffing GT. Editorial: A-I-D-S: the new endocrine epidemic. J ClinEndocrinol Metab 1994;79:1530–1.
[17] Oelkers W. Diagnostic puzzle of the adrenal incidentaloma. Eur JEndocrinol 1995;132:419–21.
[18] Norman AW, Litwack G. Hormones. New York Academic Press; 1997.[19] Morineau G, Marc JM, Boudi A, Galons H, Gourmelen M, Corvol P, et al.
Genetic, biochemical and clinical studies of patients with A328Vor R213Cmutations in 11βHSD2 causing apparent mineralocorticoid excess.Hypertension 1999;34:435–41.
[20] Vogt B, Dick B, Marti HP, Frey FJ, Frey BM. Reduced 11β-hydroxysteroid dehydrogenase activity in experimental nephrotic syn-drome. Nephrol Dial Transplant 2002;17:753–8.
[21] Escher G, Galli I, Vishwanath BS, Frey BM, Frey FJ. Tumor necrosisfactor α and interleukin 1β enhance the cortisone/cortisol shuttle. J ExpMed 1997;186:189–98.
[22] White PC, Mune T, Agarwal AK. 11β-hydroxysteroid dehydrogenase andthe syndrome of apparent mineralocorticoid excess. Endocr Rev 1997;18:135–56.
[23] Carvajal CA, Gonzalez AA, Romero DG, Gonzalez A, Mosso LM, LagosET, et al. Two homozygous mutations in the 11β-hydroxysteroiddehydrogenase type 2 gene in a case of apparent mineralocorticoid excess.J Clin Endocrinol Metab 2003;88:2501–7.
[24] Fuster D, Escher G, Vogt B, Ackermann D, Dick B, Frey BM, et al.Furosemide inhibits 11β-hydroxysteroid dehydrogenase type 2. Endocri-nology 1998;139:3849–54.
[25] Reincke M, Peter M, Sippell WG, Allolio B. Impairment of 11β-hydroxylase but not 21-hydroxylase in adrenal incidentalomas. Eur JEndocrinol 1997;132:169–200.
[26] Ravichandran R, Lafferty F, McGinniss MJ, Taylor HC. Congenitaladrenal hyperplasia presenting as massive adrenal incidentalomas in thesixth decade of life: report of two patients with 21-hydroxylase deficiency.J Clin Endocrinol Metab 1996;81:1776–9.
[27] New MI. Inborn errors of steroidogenesis. Steroids 1998;63:238–42.[28] Vierhapper H, Nowotny P, Waldhäusl W. Urinary steroid excretion rates in
acromegaly. Horm Res 2005;63:234–7.[29] Maser-Gluth C, Reincke M, Allolio B, Schulze E. Metabolism of
glucocorticoids and mineralocorticoids in patients with adrenal incidenta-lomas. Eur J Clin Investig 2000;30:83–6.
[30] Lewicka S, Nowicki M, Vecsei P. Effect of sodium restriction on urinaryexcretion of cortisol and its metabolites in humans. Steroids 1998;63:401–5.
[31] Reincke M, Nieke J, Krestin GP, Saeger W, Allolio B, Winkelmann W.Preclinical Cushing's syndrome in adrenal “incidentalomas”: comparisonwith adrenal Cushing's syndrome. J Clin Endocrinol Metab 1992;75:826–32.
Recommended

















