Embed Size (px)
Citation preview

Old and newOld and newwelfare: their relative effect welfare: their relative effect
on child nutritionon child nutritionJulieta TriasJulieta Trias
(joint with Orazio Attanasio – Marcos Vera-Hernandez)
FAO – Chile, December 1 2008

InterventionsInterventions Interventions that can potentially improve nutrition: a)Interventions that can potentially improve nutrition: a)
conditional cash transfers (CCT), b)unconditional cash transfers, conditional cash transfers (CCT), b)unconditional cash transfers, c) price subsidies, d)distribution of nutritional supplements, and c) price subsidies, d)distribution of nutritional supplements, and e) childcare centres where children are fed and taken care. e) childcare centres where children are fed and taken care.
CCT programs have become very popular tools for CCT programs have become very popular tools for governments to relieve poverty and increase human capital governments to relieve poverty and increase human capital accumulation. There is a consensus that they are effective accumulation. There is a consensus that they are effective tools at increasing the uptake of preventive care (Lagarde tools at increasing the uptake of preventive care (Lagarde 2007) but there is also controversy about their effect on 2007) but there is also controversy about their effect on nutritional status. nutritional status.
For instance, PROGRESA increased the height of children For instance, PROGRESA increased the height of children under 36 months by 1 cm (Behrman and Hoddinott 2005, under 36 months by 1 cm (Behrman and Hoddinott 2005, Gertler 2004, and Rivera Gertler 2004, and Rivera et alet al 2004). Honduran CCT 2004). Honduran CCT programme was not found to achieve any improvement in programme was not found to achieve any improvement in nutritional status (IFPRI 2003). nutritional status (IFPRI 2003).

ObjectiveObjective The objective of the paper is to compare the relative The objective of the paper is to compare the relative
merits of CCT programs with more traditional merits of CCT programs with more traditional programs to improve children nutritional status.programs to improve children nutritional status.
As far as we know, there has been no research As far as we know, there has been no research comparing these type of programs.comparing these type of programs.
We will compare the effect of We will compare the effect of Familias en Acción, Familias en Acción, a CCT a CCT program with the effect of program with the effect of Hogares Comunitarios,Hogares Comunitarios, a a childcare and feeding program in Colombia on childcare and feeding program in Colombia on nutritional outcomesnutritional outcomes (HAZ, WAZ, WHZ, chronic, (HAZ, WAZ, WHZ, chronic, global and acute malnutrition and risk of malnutrition) global and acute malnutrition and risk of malnutrition) and and morbidity outcomesmorbidity outcomes ( (diarrheadiarrhea (EDA) and acute (EDA) and acute respiratory infection (ARI) ).respiratory infection (ARI) ).

““Hogares Comunitarios”Hogares Comunitarios” Nutrition and childcare program introduced all over Nutrition and childcare program introduced all over
Colombia in the mid 1980s.Colombia in the mid 1980s. The program is targeted to poor children between 0-6 years The program is targeted to poor children between 0-6 years
old. old. Parents are required to pay a monthly fee about $US 4 per Parents are required to pay a monthly fee about $US 4 per
month per child, although there is considerable variation in month per child, although there is considerable variation in the amount across towns. the amount across towns.
Children attending to the nurseries receive a lunch and two Children attending to the nurseries receive a lunch and two snacks that include a nutritional beverage called snacks that include a nutritional beverage called bienestarinabienestarina. . Children attending to HC should receive the 70% of Children attending to HC should receive the 70% of recommended daily intake.recommended daily intake.

““Familias en AcciFamilias en Acción”ón” Large-scale welfare program introduced in 2001. In 2002, the Large-scale welfare program introduced in 2001. In 2002, the
program registered 365,000 and currently involves more than program registered 365,000 and currently involves more than 1.5 million households.1.5 million households.
The program gives a monetary transfer to mothers provided The program gives a monetary transfer to mothers provided their children are up to date with growth and development their children are up to date with growth and development monitoring visits and attend school regularly. monitoring visits and attend school regularly.
Nutritional subsidy: $CO 46,500 (U$20) monthly per family Nutritional subsidy: $CO 46,500 (U$20) monthly per family with children under 7. Primary School ($CO 14,000 ($US 5) with children under 7. Primary School ($CO 14,000 ($US 5) pcm) and Secondary School ($CO 28,000 ($10 pcm)). pcm) and Secondary School ($CO 28,000 ($10 pcm)).
EligibilityEligibility. Families with children under 18 classified as being . Families with children under 18 classified as being in the lowest level of the official socio-economic classification in the lowest level of the official socio-economic classification (Sisben level 1).(Sisben level 1).
No nutritional supplementation. Program perceived as an No nutritional supplementation. Program perceived as an alternative to alternative to HC HC for families with children 0-6.for families with children 0-6.

Other issues:Other issues: FA operates by transferring money to the mother FA operates by transferring money to the mother
(unclear how much of this transfer ends up (unclear how much of this transfer ends up benefiting the child). HC should provide food benefiting the child). HC should provide food directly to the child while the child is in the HC directly to the child while the child is in the HC centre. centre.
FA program is relatively easy to expand to other FA program is relatively easy to expand to other households or municipalities but HC requires setting households or municipalities but HC requires setting up the logistic of food purchase, providing training up the logistic of food purchase, providing training to the child carers, monitoring to prevent the food to the child carers, monitoring to prevent the food from being resold or used by individuals different from being resold or used by individuals different from the children for whom it is intended, as well as from the children for whom it is intended, as well as to have adequate premises for the children. to have adequate premises for the children.

OutlineOutline
DataData Basic StatisticsBasic Statistics MethodologyMethodology ResultsResults Summary & concluding remarksSummary & concluding remarks

Data - ColombiaData - Colombia Survey collected to evaluate FA program + Survey collected to evaluate FA program +
administrative dataadministrative data First WaveFirst Wave: 2002. Collected in 122 communities, 57 are : 2002. Collected in 122 communities, 57 are
targeted by FA. (9.080 children 0-6 / 3.940 households)targeted by FA. (9.080 children 0-6 / 3.940 households) Second WaveSecond Wave: 2003 (8.880 children 0-6 / 2.760 households): 2003 (8.880 children 0-6 / 2.760 households) Third WaveThird Wave: 2005/2006 (not used): 2005/2006 (not used)
FA surveyFA survey also collected data on the participation of the also collected data on the participation of the children on HCchildren on HC as well as on variables that are important as well as on variables that are important determinants of the participation in HC.determinants of the participation in HC.
Information: socio-demographic characteristics, Information: socio-demographic characteristics, anthropometric variables, distances to important places in the anthropometric variables, distances to important places in the town such as nearest health centre and school, distance from town such as nearest health centre and school, distance from the household to the nearest HC centre, current and the household to the nearest HC centre, current and retrospective information on participation in the HC retrospective information on participation in the HC program.program.

0.1
.2.3
.4D
ensi
ty
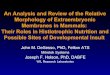
0 1 2 3 4 5 6 7 8number of payments
Payments Distribution Familias en Accion - 2003
Basic StatisticsBasic Statistics

Age
Ever attended to HC
None Ever attended to HC
Only HC FA + HC in the past
Only FA None
0 2.4 97.6 2.0 0.5 1.5 78.5 19.51 9.9 90.1 12.8 2.8 10.0 69.4 17.82 27.9 72.1 24.2 0.9 23.3 69.9 6.03 34.1 65.9 38.2 1.1 37.1 61.8 0.04 43.7 56.3 37.3 0.9 36.4 62.7 0.05 40.9 59.1 47.2 0.4 46.8 52.8 0.06 43.8 56.2 42.8 0.6 42.2 57.2 0.0
Age2002 2003
Ever attended to HC
None Ever attended to HC
None
0 3.3 96.7 4.2 95.81 19.6 80.4 22.0 78.02 43.2 56.8 44.8 55.23 52.0 48.0 55.6 44.44 53.8 46.2 62.2 37.85 56.0 44.0 61.6 38.46 58.4 41.6 58.0 42.0
Municipalities where FA was implemented2002 2003
Municipalities where FA was not implemented

Prevalence of chronic malnutrition (z-score HAZ <-2 s.d)
FA Treatment ControlAge 2002 2003 2002 2003
0 13.48 8.87 13.52 10.501 30.57 29.89 25.44 35.812 23.08 21.89 22.57 20.283 22.93 27.87 25.15 23.614 28.00 24.66 25.14 25.095 23.97 26.08 24.66 23.296 23.79 21.81 23.68 23.40
Total 24.06 23.71 23.52 23.54
Prevalence of global malnutrition (z-score WAZ <-2 s.d)
FA Treatment ControlAge 2002 2003 2002 2003
0 7.83 8.87 8.54 6.301 16.60 19.16 15.38 22.302 15.73 8.42 12.86 13.803 10.22 13.22 10.02 11.584 11.25 9.73 10.85 8.055 9.36 8.84 11.11 10.866 10.28 8.45 9.94 9.98
Total 11.34 10.56 11.10 11.38

Empirical SpecificationEmpirical Specification
YYihmtihmt : nutritional status of child i of household h, living in municipality m, in year t.
EFAEFA ihtiht: nutritional subsidy per child in household h until time t (or exposure for child i at until t)
EHCEHC ihtiht: months in HC for child i until time t (or exposure for child i until t)
XX ihtiht :contains variables that are specific to child i and household h including a dummy whether or not household h has a child eligible for the FA program.
TTt t : dummy variable for each wave
θθmm : municipality fixed effects
Problem: EFA and EHC are endogenous variables
Strategy: IV approach with municipality FE
Identification: βFA relies on the availability of the program. βHC relies on some households living closer to a HC centre than others (Attanasio and Vera-Hernandez (2006)).
yihmt= βFA (EFA)ihmt+βHC(EHC)ihmt+ βXXiht +βTTimet+θm+εihmt

Treatments and InstrumentsTreatments and Instruments Treatments: Treatments:
FA: accumulated conditional payments per child and life FA: accumulated conditional payments per child and life exposure (#months FA/ child’s age), exposure scaled exposure (#months FA/ child’s age), exposure scaled #children (#months FA/children under 17)#children (#months FA/children under 17)
HC: # months child ever attended and life exposure.HC: # months child ever attended and life exposure.
Instruments:Instruments: FA: potential conditional payments per child, potential life FA: potential conditional payments per child, potential life
exposure and potential exposure. Treatment in the exposure and potential exposure. Treatment in the municipalitymunicipality
HC: distance to the nearest HC (controls for other distance)HC: distance to the nearest HC (controls for other distance) Non linear prediction of months in HC (PHC). Interaction Non linear prediction of months in HC (PHC). Interaction
between PHC with FA treatment in the municipality. between PHC with FA treatment in the municipality.

Child characteristicsChild characteristics: age, birth order, gender. : age, birth order, gender. (inverse of age)(inverse of age)
Mother’s characteristicsMother’s characteristics: age, education, height, : age, education, height, marital status (single)marital status (single)
Household characteristics: Household characteristics: Children under 7 in the household potentially eligible for FA Children under 7 in the household potentially eligible for FA
(0 or 1 for controls and treatment)(0 or 1 for controls and treatment) # children 8-12, # children 13-17# children 8-12, # children 13-17 household head’s age and education.household head’s age and education.
Location:Location: area, travel time to health center, school and area, travel time to health center, school and town center.town center.
ControlsControls

Results – First StageResults – First Stage Distance to HCDistance to HC: 30 min. of extra travel to the HC increases the : 30 min. of extra travel to the HC increases the
subsidy per child by $CO 1,232 and reduces the time attending a subsidy per child by $CO 1,232 and reduces the time attending a HC by 9.8 days (21.6 days considering distance at each wave).HC by 9.8 days (21.6 days considering distance at each wave).
FA programFA program (treatment + 1 year pot. subsidy): reduces the (treatment + 1 year pot. subsidy): reduces the attendance to HC in 6.1 months for children at the average age attendance to HC in 6.1 months for children at the average age (48 months) and increases the transfer in $CO 502,000. (48 months) and increases the transfer in $CO 502,000.
Households with schooling age childHouseholds with schooling age child: An additional sibling in : An additional sibling in secondary school age increases the nutritional subsidy by $CO secondary school age increases the nutritional subsidy by $CO 2000 per child and reduces the attendance to HC by 6.2 days. 2000 per child and reduces the attendance to HC by 6.2 days.
Single Mothers:Single Mothers: increases child’s attendance to HC by 28 days increases child’s attendance to HC by 28 days and reduces the transfer per child by $CO 2,000. and reduces the transfer per child by $CO 2,000.
Distance to health facilitiesDistance to health facilities: 30 min. of extra travel reduces the : 30 min. of extra travel reduces the transfer by $CO 234 per child and increases the attendance to transfer by $CO 234 per child and increases the attendance to HC by 3.4 days. However, those effects are not significant.HC by 3.4 days. However, those effects are not significant.

First Stage for program effect on HAZNegative Binomial
First Stage FA First Stage HC
Months in HC Conditional Money per Child¹ (mill)
Months in HC
FA treatment available in the community 0.525** 0.049*** 0.599[0.234] [0.013] [0.891]
Potential conditional money per child¹ (mill) -4.198* 0.168 0.209[2.177] [0.119] [5.552]
Potential conditional money per child¹ (mill) ^2 3.117 -0.014 8.961[2.198] [0.192] [6.759]
age_m x potential conditional money per child¹ (mill) -0.02 0.006** -0.139[0.071] [0.003] [0.160]
age_m^2 x potential conditional money per child¹ (mill) 0.001 0.000 -0.001[0.001] [0.000] [0.002]
travel time to the nearest HC in minutes (at the time of the first wave)/100 -1.508*** 0.007 -1.252
[0.294] [0.008] [1.407][travel time to the nearest HC in minutes (at the time of the first wave)/100] ^2 0.252* -0.004 0.421
[0.145] [0.004] [0.542]travel time to the nearest HC in minutes/100 -2.134*** 0.003 -3.152**
[0.305] [0.009] [1.341](travel time to the nearest HC in minutes/100)^2 0.663*** -0.001 0.807
[0.159] [0.004] [0.527]travel time to HC at wave 1 x FA treatment available in the community -1.165*** -0.005 -0.568
[0.254] [0.010] [0.910]travel time to HC x FA treatment available in the community 0.522** -0.018 0.969
[0.238] [0.011] [0.916]prediction of months in HC 0.000 0.576***
[0.000] [0.066]prediction of months in HC^2 0.000 -0.004***
[0.000] [0.001]prediction of months in HC x treatment available in the community 0.000 0.058
[0.000] [0.071]Observations 8640 8640 8640R-squared 0.56 0.36Test instruments 638.19 91.03 30.13Prob inst 0.00 0.00 0.00

Program effect HAZChronic
Malnutrition
Risk of Chronic
Malnutrition WAZGlobal
Malnutrition
Risk of Global
MalnutritionConditional money pc (mill) ¹ 0.620*** -0.101 -0.329*** 0.978*** -0.187*** -0.367***
[0.225] [0.086] [0.110] [0.237] [0.066] [0.113]Months in HC 0.010** -0.003* -0.004** 0.005 -0.001 -0.001
[0.004] [0.002] [0.002] [0.004] [0.001] [0.002]Observations 8640 8640 8640 8640 8640 8640R-squared 0.22 0.14 0.16 0.14 0.07 0.10Effect of one year FA 0.09 -0.01 -0.05 0.14 -0.03 -0.05t-test 2.75 -1.18 -3.00 4.13 -2.82 -3.25Effect of one year HC 0.12 -0.04 -0.04 0.06 -0.01 -0.01t-test 2.44 -1.72 -2.00 1.20 -0.46 -0.40F Test- Same effect of one year program 0.38 0.96 0.00 2.20 1.52 2.67Prob 0.54 0.33 0.94 0.14 0.22 0.10Robust standard errors in brackets (standard errors clustered at household level)
* significant at 10%; ** significant at 5%; *** significant at 1%
¹ Only includes nutritional componet
One year program effectOne year program effect

Program effect WHZAcute
Malnutrition
Risk of Acute
Malnutrition EDA IRAConditional money pc (mill) ¹ 0.837*** -0.098*** -0.119 -0.216** -0.254*
[0.238] [0.030] [0.081] [0.092] [0.142]Months in HC -0.003 0.001 0.000 -0.002* -0.004***
[0.004] [0.000] [0.001] [0.001] [0.002]Observations 8640 8640 8640 9315 9314R-squared 0.10 0.02 0.05 0.04 0.06Effect of one year FA 0.12 -0.01 -0.02 -0.03 -0.04t-test 3.51 -3.24 -1.46 -2.35 -1.79Effect of one year HC -0.04 0.01 0.00 -0.03 -0.05t-test -0.94 1.33 0.32 -1.91 -2.66F Test- Same effect of one year program 9.24 9.34 1.53 0.01 0.41Prob 0.00 0.00 0.22 0.91 0.52Robust standard errors in brackets (standard errors clustered at household level)
* significant at 10%; ** significant at 5%; *** significant at 1%
¹ Only includes nutritional componet

HAZHAZ: one year in FA program for a child with 3 : one year in FA program for a child with 3 siblings under 17, increases the z-score by 0.09, siblings under 17, increases the z-score by 0.09, reduces prevalence of chronic malnutrition (cn) reduces prevalence of chronic malnutrition (cn) by 1% and the risk cn by 4%. For the case of by 1% and the risk cn by 4%. For the case of HC the effect is 0.12, -4% and -5%, respectively.HC the effect is 0.12, -4% and -5%, respectively.
F-Test equal effect FA and HC: no rejection.F-Test equal effect FA and HC: no rejection. WAZWAZ: FA increase z-score by 0.14 and reduce : FA increase z-score by 0.14 and reduce
the probability of global malnutrition by 3% the probability of global malnutrition by 3% while for HC is 0.06 sd and 1%, respectively.while for HC is 0.06 sd and 1%, respectively.
EDA:EDA: reduction in about 3% in both programs reduction in about 3% in both programs IRA: IRA: reduction in 4% for FA and 5% for HC.reduction in 4% for FA and 5% for HC.

Summary and ConclusionsSummary and Conclusions Both programs improve the nutritional status and morbidity Both programs improve the nutritional status and morbidity
outcomes of children under 7 and there is not significant outcomes of children under 7 and there is not significant difference in their impact. This result is consistent with difference in their impact. This result is consistent with previous studies where FA program improves the quality of previous studies where FA program improves the quality of the food consumed. It also complements studies of the the food consumed. It also complements studies of the effectiveness of HC. effectiveness of HC.
This result This result doesn’t doesn’t imply that the programs are substitutes. imply that the programs are substitutes. Different groups of the population may prefer different Different groups of the population may prefer different programs. Our estimates provide some programs. Our estimates provide some insight about the insight about the characteristics that are relevant in the choice of FA vs HC –characteristics that are relevant in the choice of FA vs HC –for instance, single mothers for instance, single mothers prefer HC program. prefer HC program.
Further research on the potential complementarities of both Further research on the potential complementarities of both programs should be carried out. programs should be carried out.