Embed Size (px)
Citation preview
M A N AG E M E N T O F S E R I O U S N E W B O R N I N F E C T I O N S
W H E N H O S P I TA L T R E AT M E N T I S N OT
P O S S I B L E
Steve Wall, MD SM MSW FAAP
Saving Newborn Lives/Save the Children
WCPH, Kolkata
February 13, 2015
Questions to be addressed
What is global evidence for community
management of serious newborn infections?
What is additional impact of management of serious
newborn infections at primary level when referral is
not possible?
Can serious newborn infections be treated by
simpler antibiotic regimens?
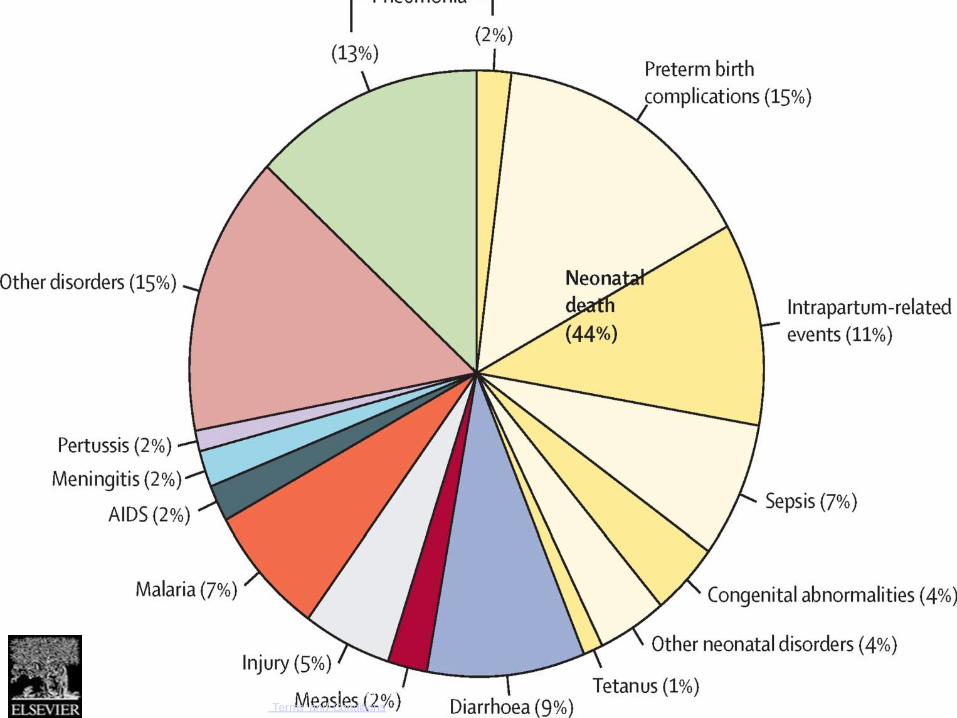
Figure 2
The Lancet 2015 385, 430-440DOI: (10.1016/S0140-6736(14)61698-6)
Copyright © 2015 Elsevier Ltd Terms and Conditions
Current WHO guidelines
Hospitalization with 10 days of antibiotics
Benzylpenicillin (or ampicillin) + gentamicin
IMNCI – initial antibiotics (ampicillin + gentamicin)
at first level facility, with referral to hospital
If referral not possible, outpatient treatment with
7-10 days of injectable antibiotics (ie, 3 injections
per day)
Hospital treatment is often not possible
Lack of accessible hospitals with newborn care
services
Hospitalization not acceptable to many/most
families
Distance
Cost
Family hardship
Perceived poor quality
Socio-cultural factors
Current evidence: Home-based treatment
Evidence from research studies - community-based
packages included home-based treatment of sepsis
Bang (India): 62% NMR reduction
Baqui (Bangladesh): 34% NMR reduction
ADDITIONAL IMPACT OF
TREATING SERIOUS NEWBORN
INFECTIONS AT PRIMARY LEVEL
Where referral is not possible
COMBINE Study (Ethiopia)
Objective: To evaluate additional benefit on mortality of
management of newborn possible serious bacterial
infections (PSBI) by trained community health workers
Ethiopia’s Health Extension Workers (HEW), linked to
community health volunteers, provided management of PSBI
when referral was not possible
HEWs trained to
Identify signs or newborn PSBI and refer to health center
Treat at health post if referral not possible or not accepted
Gentamicin + amoxicillin for 7 days (7 total injections)
COMBINE Design
Cluster RCT
Comparison: MNH package via antenatal & postnatal home
visits by HEWs and volunteers, with referral of newborn
PSBI to facilities
Intervention: Addition of HEW management of newborn
PSBI (7 days of gent + amox) if referral not accepted
Outcome: Newborn mortality after day one
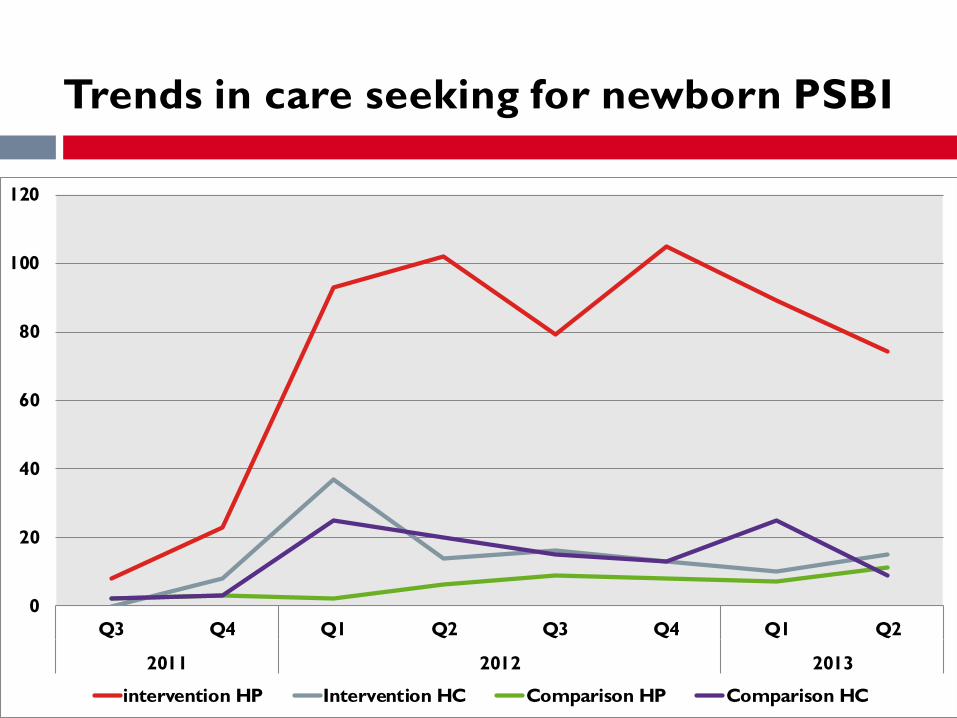
0
20
40
60
80
100
120
Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2
2011 2012 2013
intervention HP Intervention HC Comparison HP Comparison HC
Trends in care seeking for newborn PSBI
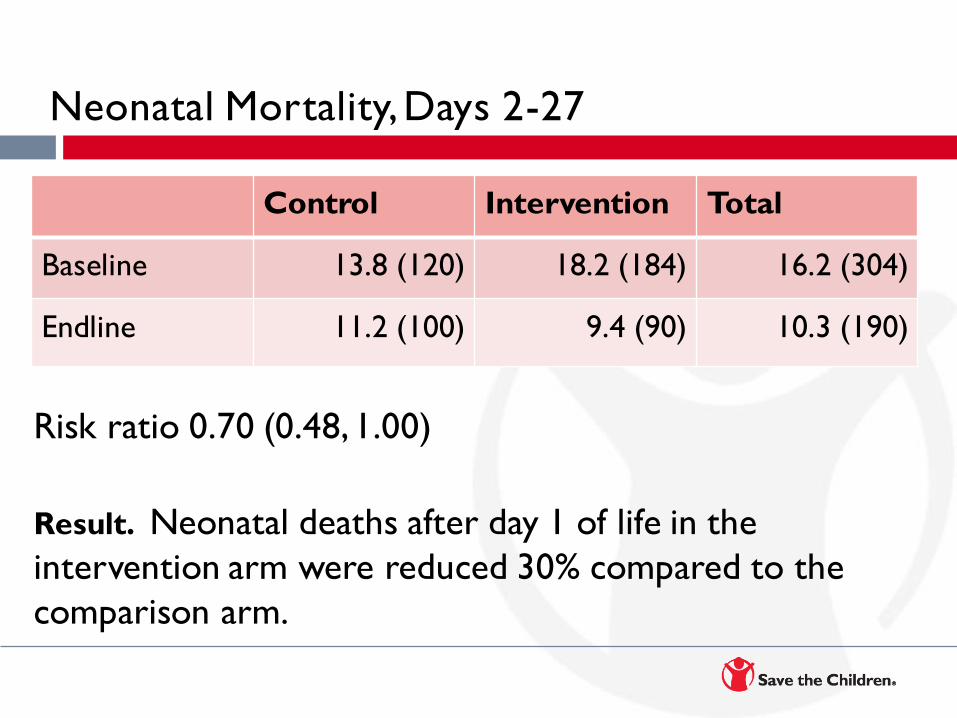
Neonatal Mortality, Days 2-27
Risk ratio 0.70 (0.48, 1.00)
Result. Neonatal deaths after day 1 of life in the
intervention arm were reduced 30% compared to the
comparison arm.
Control Intervention Total
Baseline 13.8 (120) 18.2 (184) 16.2 (304)
Endline 11.2 (100) 9.4 (90) 10.3 (190)
COMBINE Results
Trained community health workers can improve
newborn survival by identifying and treating serious
newborn infections when referral is not possible
Feasible to deliver this intervention effectively
through existing community health platforms
Effective implementation of this intervention requires
programs to ensure supply, create demand, and
continuously monitor to assure coverage & quality
SIMPLER ANTIBIOTIC REGIMENS
FOR SERIOUS NEWBORN
INFECTIONS
In outpatient settings where referral
is not possible
SATT & AFRINEST
SATT – Bangladesh
SATT – Pakistan
AFRINEST
DRC
Kenya
Nigeria
Common study protocol
SATT & AFRINEST Objective
To evaluate if simpler antibiotic regimens are
equivalent to a ‘standard course’ of parenteral
antibiotics for treatment of possible serious
bacterial infections in young infants whose
families do not accept hospitalization.
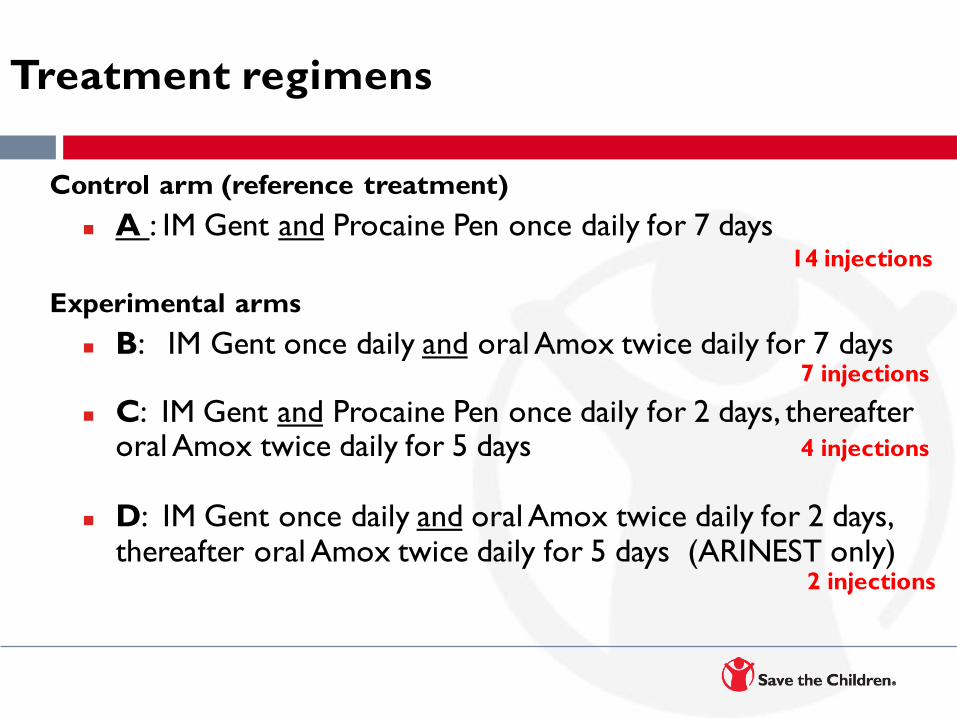
Treatment regimens
Control arm (reference treatment)
A : IM Gent and Procaine Pen once daily for 7 days 14 injections
Experimental arms
B: IM Gent once daily and oral Amox twice daily for 7 days 7 injections
C: IM Gent and Procaine Pen once daily for 2 days, thereafter oral Amox twice daily for 5 days 4 injections
D: IM Gent once daily and oral Amox twice daily for 2 days, thereafter oral Amox twice daily for 5 days (ARINEST only) 2 injections
Inclusion and Exclusion Criteria
Inclusion Criteria:
Fever (temp ≥380 C)
Hypothermia (temp≤35.5 0 C)
Lethargy (movement only with
stimulus)
Severe chest indrawing
Poor feeding
Hospitalization not accepted
Exclusion Criteria:
Signs of very severe infections
Vomiting or unable to take
oral medication
Weight <1500 grams
Results
Simplified antibiotic regimens were equivalent to the
reference regimen with respect to ‘treatment failure’
rates
Caveat: Evidence for simplest regimen (2 injections of
gent) is available from only one trial (AFRINEST)
Implications
Infants with PSBI should be referred for hospital
treatment – and effective treatment ensured
However, majority of families may not be able to
access hospital treatment at all or in time
Where hospitalization is not possible, these infants can
be treated with simplified antibiotic regimens as
outpatients by trained health providers
Acknowledgements
COMBINE
Investigator Team: Saving Newborn Lives/Save the Children Ethiopia, JSI, LSHTM, JHU,
UNICEF, Ethiopia Pediatric Society,
Funding: BMGF
SATT & AFRINEST
Investigators:
SATT Bangladesh: Projahnmo, JHU, AKU,
AFRINEST PIs from DRC, Kenya, and Nigeria
WHO
LSHTM
Funding: BMGF, USAID

Much progress, but much
to do . . .
- Thanks Photo by Jason Tanner/Save the Children





























