Embed Size (px)
DESCRIPTION
CT FINDINGS OF ACUTE EPIPLOEIC APPENDAGITIS
Citation preview

Young male patient presented with pain Right lumbar & flank
region. CECT abdomen was done .
SPIRAL CT MRI
PET-CT Centre Sector 44-C Chandigarh
www.spiralctmricentre.com
Dr Arun Gupta Director Imaging DepttDr Rakhee Gupta Dr Nitu Narula Dr Ritesh MahajanDr R K Gandhi
AcuteEpiploic
Appendagitis CT findings

The inflammation of epiploic appendages can be the result of
torsion or venous occlusion.
Epiploic appendages are peritoneal outpouchings that arise from the serosal surface of the colon, contain adipose tissue and vessels, and can be up to 5 cm in length.

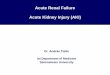
FATTY CENTREINFLAMMATORY CHANGESBASE NARROWER THAN EQUATOR
IMPORTANT CT
FINDING
A fatty central core abutting the colon wall with surrounding inflammatory changes and a base narrower than the equator.

ACUTE EPIPLOIC APPENDAGITIS
Acute epiploic appendagitis is an uncommon cause of abdominal pain .
The diagnosis primarily relies on cross-sectional imaging and is made most often on CT.
Clinically, it is most often mistaken for acute diverticulitisWhen acute epiploic appendagitis involves the cecum, it may
be mistaken clinically for acute appendicitis. Because of the benign self-limiting course of this condition, it
is important to recognize and understand its various manifestations as it mimics a surgical abdomen.
Patients with epiploic appendagitis most commonly present with localized abdominal pain, more commonly on the left. The presenting clinical symptoms of epiploic appendagitis are nonspecific, leading to clinical misdiagnosis .

CT scans of the Epiploic appendagitis is evaluated for the presence of Colon wall thickening Focal fatty center of the lesion Inflammatory changes around the fatty central core Location in relation to the colon Size Presence or absence of central high density within
the fat representing thrombosed vessels
PRESENCE OR ABSENCE OF LEUKOCYTOSIS IS ALSO ASSESSED.
ACUTE EPIPLOIC APPENDAGITIS- CT FINDINGS

The most common CT appearance of acute epiploic appendagitis is :
The presence of 1.5- to 3.5-cm-diameter fat-density lesion with surrounding inflammatory changes abutting the wall of the adjacent colon.
Involvement of the proximal colon is less common, although not unusual.
Although the presence of a central high-attenuation focus within the fat is a helpful finding in making the diagnosis, its absence does not exclude the diagnosis of acute epiploic appendagitis.
The high-density central focus within the fat is believed to represent a thrombosed vessel within the inflamed appendix epiploica.
ACUTE EPIPLOIC APPENDAGITIS- CT FINDINGS

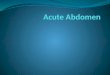
BASE OF INFLAMMATION IS SMALLER THAN EQUATOR
FAT DENSITY CENTRE WITH SURROUNDING HYPERDENSE RIM
AND INFLAMMATION ABUTTING THE ASCENDING COLON
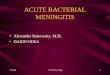
AXIAL IMAGES

FATTY CORE APPRECIATED
ADJACENT INFLAMMTORY
STRANDING
AXIAL IMAGES

CORONAL REFORMATIONS

Differential Diagnosis
The differential diagnosis of an Inflammatory fatty lesion on CT includes Acute epiploic appendagitis Mesenteric panniculitis Acute diverticulitis Trauma Omental neoplasm such as a liposarcoma. Omental infarction can have an appearance similar to
that of epiploic appendagitis, it lacks the hyperdense ring that is seen in epiploic appendagitis. The CT features of omental infarction typically consist of a right lower quadrant well-circumscribed nonenhancing oval soft-tissue mass that is located deep relative to the anterior abdominal muscles.

INFLAMMTION VENTRAL TO ASCENDING COLON.FOCAL FATTY CENTRE SUBCENTIMETRE HIGH ATTENUATION AREAS IN THE CORE OF THE INFLAMMATION FOCUS ( Thrombosed Vessels)COLONIC WALL THICKENING
TO SUMMARIZE, RADIOLOGICAL
ASSESMENT INCLUDES
Presence of colon wall thickening,
Focal fatty center
Inflammatory changes
Location in relationship to the colon
Size, and presence or absence of central high density within the fat.
CT findings usually resolve by 6 months

•G B A H R E M A N I G G, W H I T E M , H O F F F L , E T A L : A P P E N D I C E S E P I P L O I C A E O F T H E C O L O N: R A D I O L O G I C A N D PAT H O L O G I C F E AT U R E S. R A D I O G R A P H I C S 1 2 : 5 9 - 7 7 , 1 9 9 2 .
•S I N G H A K , G E RVA I S D A , H A H N P F E T A L : C T A P P E A R A N C E O F A C U T E A P P E N D A G I T I S. A J R 1 8 3 : 1 3 0 3 - 7 , 2 0 0 4 .
REFERENCES