Embed Size (px)
Citation preview

A M E R I C A N C O L L E G E O F C A R D I O L O G Y 2 0 1 5
Advanced HFrEF
Pearls
M A R C H 1 5 , 2 0 1 5
Sanjiv J. Shah, MD, FACC, FAHA Associate Professor of Medicine
Division of Cardiology, Department of Medicine
N O R T H W E S T E R N U N I V E R S I T Y F E I N B E R G S C H O O L O F M E D I C I N E

Case #1: 62-year-old woman with NICM,
LVEF 25%, diabetes, CKD, s/p
ICD presents with ADHF: Cr 1.8,
NTproBNP 8232, Na+ 136:
undergoes IV diuresis with
furosemide 80 mg PO TID
After 5 days of IV diuresis: net -8L, BP 114/62, and
Cr increased from 1.8 on admission to 2.4 mg/dl.
What would you do next?
A. Stop IV diuresis and re-check labs the
next day
B. Stop IV diuresis and give 250 cc NS bolus
and re-check labs the next day
C. Continue IV diuresis and check albumin,
total protein, and hematocrit
D. Inform the patient that she has a poor
prognosis


After 5 days of IV diuresis: net -8L, BP 114/62, and
Cr increased from 1.8 on admission to 2.4 mg/dl.
What would you do next?
A. Stop IV diuresis and re-check labs the
next day
B. Stop IV diuresis and give 250 cc NS bolus
and re-check labs the next day
C. Continue IV diuresis and check albumin,
total protein, and hematocrit
D. Inform the patient that she has a poor
prognosis

Hemoconcentration in HF
Testani et al.
Circulation 2010

Hemoconcentration in HF
Testani et al.
Circulation 2010
P<0.0001
No hemoconcentration
Hemoconcentration

Right heart catheterization is performed

How would you interpret the PCWP tracing?
A. There is evidence of significant mitral
regurgitation
B. PCWP is no longer elevated
C. The patient is still markedly fluid
overloaded
D. The PA catheter is over-wedged


Right heart catheterization is performed
How would you interpret the PCWP tracing?
A. There is evidence of significant mitral
regurgitation
B. PCWP is no longer elevated
C. The patient is still markedly fluid
overloaded
D. The PA catheter is over-wedged

How would you interpret the PCWP tracing?
A. There is evidence of significant mitral
regurgitation
B. PCWP is no longer elevated
C. The patient is still markedly fluid
overloaded
D. The PA catheter is over-wedged

Respiratory variation in PCWP
End-expiratory
PCWP = 27 mmHg

62-year-old woman with HFrEF
• The patient is diuresed an additional 5L and then discharged
• 3 months later: worsening breathlessness, no overt fluid overload
• NYHA class III

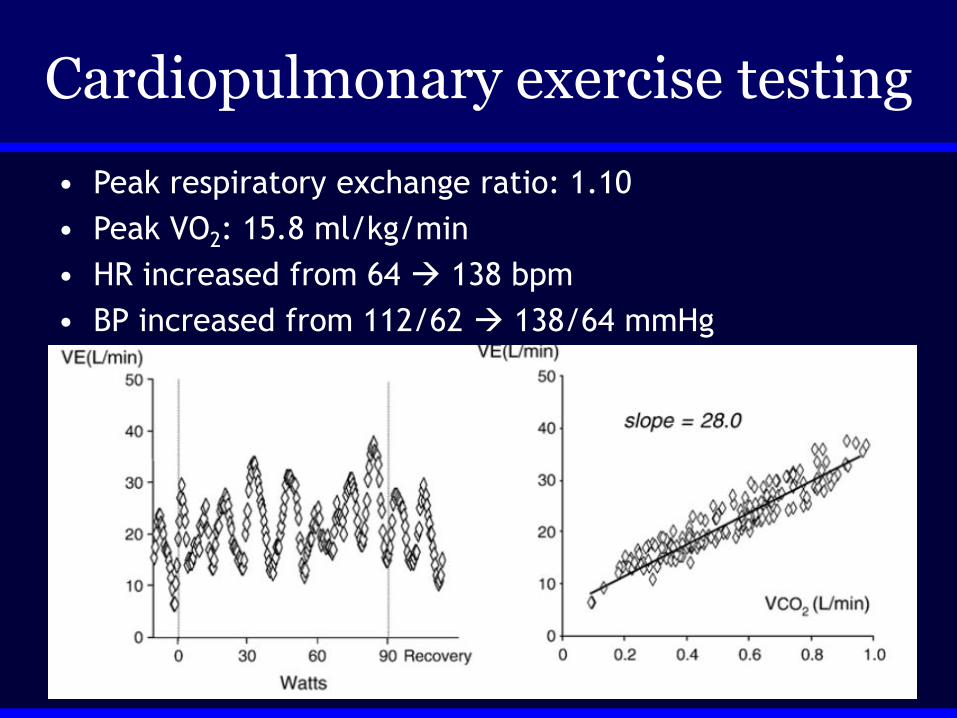
Cardiopulmonary exercise testing
• Peak respiratory exchange ratio: 1.10
• Peak VO2: 15.8 ml/kg/min
• HR increased from 64 138 bpm
• BP increased from 112/62 138/64 mmHg

How would you interpret this patient’s
cardiopulmonary exercise test?
A. The patient has a poor prognosis
B. The patient did not achieve an adequate
effort for the test
C. There is evidence of pulmonary vascular
disease
D. There is evidence of chronotropic
incompetence

Cardiopulmonary exercise testing
• Peak respiratory exchange ratio: 1.10
• Peak VO2: 15.8 ml/kg/min
• HR increased from 64 138 bpm
• BP increased from 112/62 138/64 mmHg

How would you interpret this patient’s
cardiopulmonary exercise test?
A. The patient has a poor prognosis
B. The patient did not achieve an adequate
effort for the test
C. There is evidence of pulmonary vascular
disease
D. There is evidence of chronotropic
incompetence

Exercise oscillatory breathing in HFrEF
Guazzi et al.
Am Heart J 2007

Exercise oscillatory breathing in HFrEF
Guazzi et al.
Am Heart J 2007
Normal VE/VCO2 Elevated VE/VCO2
No EOB
+EOB
No EOB
+EOB

Calculation of chronotropic incompetence in HF
• %Heart rate reserve = (HRpeak-HRrest)
(220-age-HRrest)
• CI is present if:
» %HRR < 80% (not on beta-blocker)
» %HRR < 62% (on beta-blocker)
• %HRR in this case = (138-64)/(220-age-64)
= 79% (on beta-blocker) = No CI

62-year-old woman, s/p OHT
• 2 months post-op
• Meds: » Tacrolimus
» Prednisone
» Diltiazem
» Pravastatin
• Pt doing well
• Biopsy = 0R

62-year-old woman, s/p OHT
• 7 months post-op
• Presented to ER with fatigue, SOB, abdominal distension

62-year-old woman, s/p OHT
• 7 months post-op
• Presented to ER with fatigue, SOB, abdominal distension

What is the most likely diagnosis?
A. Need more information: check IVRT
B. Need more information: check speckle-
tracking echocardiography
C. Tacrolimus toxicity
D. Coronary allograft vasculopathy
E. Acute cellular rejection


What is the most likely diagnosis?
A. Need more information: check IVRT
B. Need more information: check speckle-
tracking echocardiography
C. Tacrolimus toxicity
D. Coronary allograft vasculopathy
E. Acute cellular rejection

62-year-old woman, s/p OHT
• 7 months post-op
• Presented to ER with fatigue, SOB, abdominal distension
• Right heart cath: » CVP 25 mmHg
» PCWP 30 mmHg
» CO 2 L/min

62-year-old woman, s/p OHT
• Endomyocardial biopsy performed
• Urgently taken to OR for V-A ECMO
• Treated with thymo, plasmapheresis, rituxan, IVIG
• ECMO removed 4 days later

62-year-old woman, s/p OHT
• Endomyocardial biopsy performed
• Urgently taken to OR for V-A ECMO
• Treated with thymo, plasmapheresis, rituxan, IVIG
• ECMO removed 4 days later
Grade 3R rejection

62-year-old woman, s/p OHT
• Doing well 1 month later, taking all medications
Echo 1 month later

BASELINE REJECTION RECOVERY
Grade 3R cellular rejection

BASELINE
s’ = 7.5 cm/s
e’ = 8 cm/s
REJECTION
s’ = 4.2 cm/s
e’ = 5.5 cm/s
RECOVERY
s’ = 7.2 cm/s
e’ = 9 cm/s
Grade 3R cellular rejection

Acute cellular rejection (ACR)
• Major cause of 1-year mortality, highest
risk in first 6 months
• Effector T cells mediate inflammatory
response myocardial edema/damage
• Routine surveillance currently performed
with cardiac bx works well but invasive
• Problems with cardiac bx:
» Sampling error, interobserver variability,
wide variability in frequency and duration

Acute cellular rejection (ACR)
• Grade 2R or higher rejection considered
clinically significant:
» Rx with high-dose corticosteroids
» Add lymphocyte-depleting agents if
hemodynamic compromise is present
Echo for diagnosis of ACR
• Increased LV wall thickness and LV mass:
» Indicative of myocardial edema
• Pericardial effusion:
» 49% sensitivity, 74% specificity
• Diastolic function:
» Influenced by donor age, heart rate
(increased due to cardiac denervation),
loading conditions, dissociation of atria

Echo for diagnosis of ACR
• Mena et al. (JASE 2006) performed a
systematic review of the published
literature between 1967-2005:
» E, A velocities: did not predict ACR
» PHT: sensitivity 23-87%, specificity 76-98%
» IVRT: sensitivity 28-85%, specificity 80-98%
» Conclusions: inconsistent quality, low
sensitivity
• Newer modalities (e.g., speckle-
tracking): conflicting results

Acute cellular rejection: imaging algorithm
Estep JD et al. JACC Imaging 2009

62-year-old woman, s/p OHT now 3 years post-transplant with dyspnea, syncope
• Prior work-up for dyspnea:
» RHC: normal hemodynamics
» RV biopsy: Grade 0R
» V/Q scan: low probability for PE
» CT chest: no abnormalities
» Event monitor: sinus brady with occasional
junctional escape during episodes of
dyspnea, lightheadedness
• On night of admission, had 30-second
syncopal episode

Electrocardiogram

Chest Radiography

• Right heart catheterization:
» RA 0-1, RV 20/0, PA 20/3 (11), PCWP 5
» Ao 110/67 (85); CO 4.2 (TD), 4.54 (Fick)
» Sats: Ao 98%, PA 68%
62 y.o. woman s/p OHT with syncope

Coronary Angiography

Coronary Angiography

Coronary Angiography

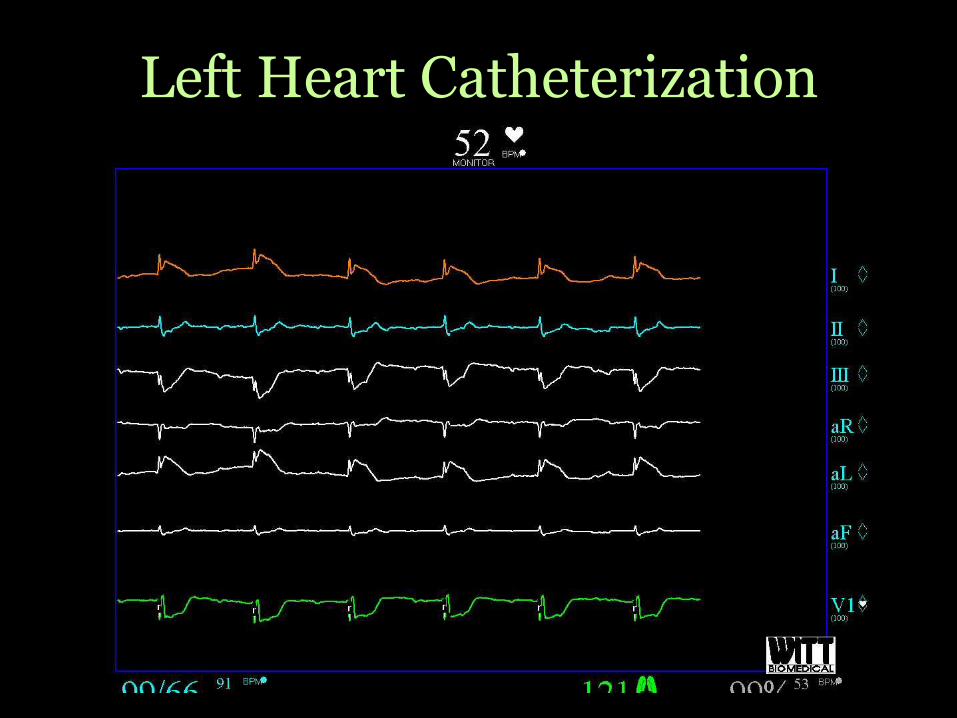
Left Heart Catheterization
• Just after the contrast injection into the
left main coronary artery…
» Patient became progressively bradycardic
» ST elevations seen on monitor
Left Heart Catheterization

What is the most likely coronary
pathophysiology?
A. Plaque rupture
B. Allograft vasculopathy
C. Coronary vasospasm
D. Cellular rejection

What is the most likely coronary
pathophysiology?
A. Plaque rupture
B. Allograft vasculopathy
C. Coronary vasospasm
D. Cellular rejection

A diagnostic procedure was performed…

Coronary Angiography
PRE POST
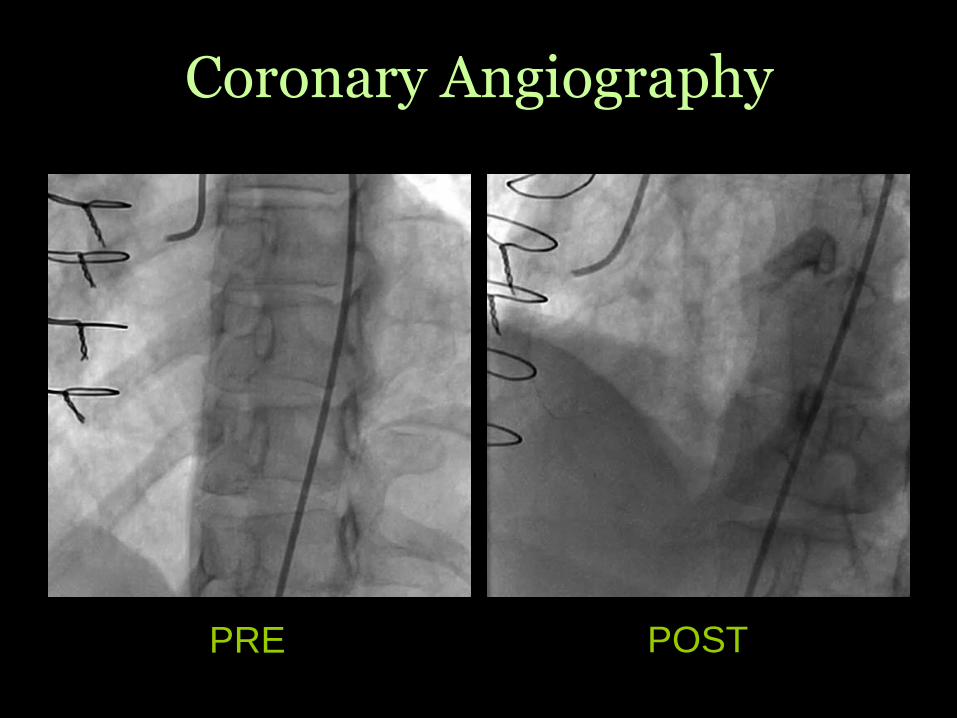
Coronary Angiography
PRE POST
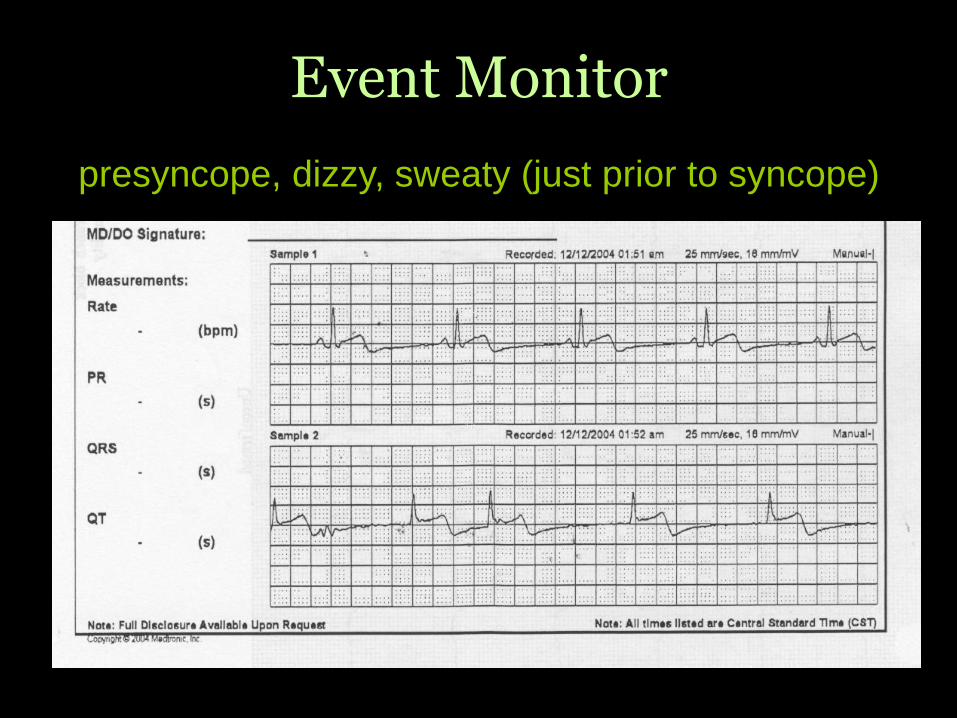
Event Monitor
presyncope, dizzy, sweaty (just prior to syncope)

Event Monitor
“felt like passing out” “chest tightness”
Coronary vasospasm s/p OHT
• Rare: occurs in <5%
• Usually begins 1-3 years post-transplant
• “Triple-vessel” spasm very rare
• Spasm carries a poor prognosis
• Possibly associated with accelerated
arteriosclerosis and diffuse lymphocytic
coronary endothelialitis

Cardiac allograft vasculopathy (CAV)
• Prevalence ~54% in survivors at 10 years
after OHT:
» Diffuse intimal hyperplasia, likely results
from cumulative endothelial injury
• Early diagnosis of CAV is challenging:
» Typical symptoms of ischemia lacking
» Coronary angiography can underestimate
» Early recognition important:
—Rapid CAV progression can occur bad outcomes

• Associated with traditional cardiac RFs
• Other risk factors:
» Acute rejection, anti-HLA antibodies
» Cytomegalovirus (CMV)
» Nephrotoxicity post-transplant
» New-onset diabetes post-transplant
• Typically affects distal coronary arteries
Cardiac allograft vasculopathy (CAV)

• Diagnosis:
» Coronary angiography, IVUS,
dobutamine stress echocardiography
• Prevention/Treatment:
» Everolimus, sirolimus
» Lipid-lowering
» Percutaneous coronary intervention
» Re-transplantation
Cardiac allograft vasculopathy (CAV)
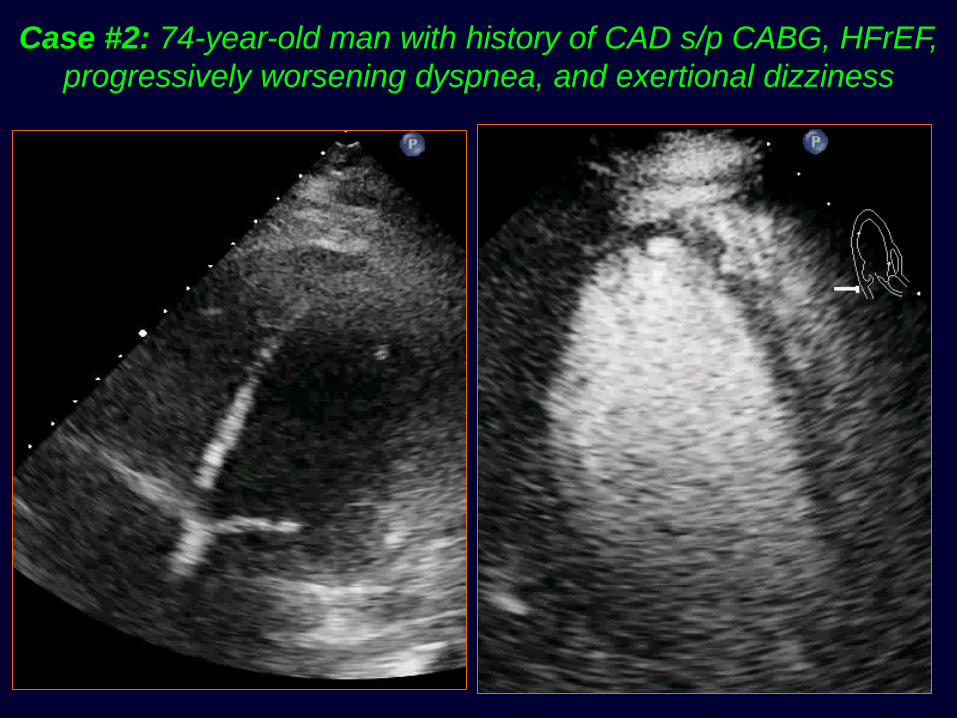
Case #2: 74-year-old man with history of CAD s/p CABG, HFrEF,
progressively worsening dyspnea, and exertional dizziness

74-year-old man with HFrEF
• ACE-I and beta-blocker stopped
• Diuresed 5L, feels much better
• Attending switches on day of discharge
» “Start guideline-directed medical therapy”
» Low-dose ACE-I and beta-blocker started
» Pt has syncope while walking in room, develops
subdural hematoma…

Case #2: 74-year-old man with history of CAD s/p CABG, HFrEF,
progressively worsening dyspnea, and exertional dizziness


74-year-old man with HFrEF
• Constrictive pericarditis diagnosed
• Underwent pericardial stripping
• Still with mild HFrEF but now NYHA class II
and no further syncopal events
1. If creatinine goes up during IV diuresis,
differentiate hemoconcentration from
worsening renal function
2. Remember to measure hemodynamics
(especially PCWP) at end-expiration
3. Exercise oscillatory breathing: poor
prognostic sign in HF
Advanced HFrEF pearls

5. Echo: cannot yet replace routine biopsy
surveillance for transplant rejection
6. Coronary vasospasm in the setting of
cardiac transplantation: consider
coronary allograft vasculopathy
7. When treating HFrEF: get with the
guidelines, but don’t stop using your
noggin’!
Advanced HFrEF pearls

thank you!