Embed Size (px)
Citation preview

Anemia
Clinical PharmacySubmitted to: Ma’am Sobia JawedGroup: 09
Definition of Anemia Deficiency in the oxygen-carrying capacity
of the blood due to a diminished erythrocyte mass.
Anemia is classified as: Regenerative: In a regenerative anemia, the bone
marrow responds appropriately to the decreased red cell mass by increasing RBC production and releasing reticulocytes.
Non regenerative: In a non-regenerative anemia, the bone marrow responds inadequately to the increased need for RBC.
Measurements of Anemia Hemoglobin = grams of hemoglobin per 100 mL of whole
blood (g/dL) Hematocrit = percent of a sample of whole blood occupied by
intact red blood cells RBC = millions of red blood cells per microL of whole blood MCV = Mean corpuscular volume
If > 100 → Macrocytic anemia If 80 – 100 → Normocytic anemia If < 80 → Microcytic anemia
RDW = Red blood cell distribution width = (Standard deviation of red cell volume ÷ mean
cell volume) × 100 Normal value is 11-15% If elevated, suggests large variability in sizes of
RBCs
Laboratory Definition of Anemia
Hgb: Women: <12.0 Men: < 13.5
Hct: Women: < 36 Men: <41
Symptoms of Anemia Decreased oxygenation
Exertional dyspnea Dyspnea at rest Fatigue Bounding pulses Lethargy, confusion
Decreased volume Fatigue Muscle cramps Postural dizziness syncope
Classification on Etiology Decrease in the total circulating red cell mass (hematocrit, hemoglobin concentration) Classification: A. Underlying mechanism
blood loss increased destruction decreased production
B. Morphology of erythrocytes size (micro-, macro-, normocytic) shape (spherocytosis, stomato-,...) color (degree of hemoglobinization: normo- hypo-,
hyperchromic)
Special Considerations in Determining Anemia Acute Bleed
Drop in Hgb or Hct may not be shown until 36 to 48 hours after acute bleed (even though patient may be hypotensive)
Acute Blood Loss – non-regenerative, then moderately regenerative 3-7 days later
Chronic Blood Loss – marked regeneration
Symptoms of Anemia
Acute Blood loss Clinical signs depend on the
degree of anemia, the duration (acute or chronic), and the underlying cause. In acute blood loss, the patient usually presents with tachycardia, pale mucous membranes, bounding or weak pulses, and hypotension.
Chronic Blood loss Patients with chronic anemia
have had time to adjust, and their clinical presentation is usually more indolent with vague signs of lethargy, weakness, and anorexia.
These patients will have similar physical examination findings, pale mucous membranes, tachycardia, and possibly splenomegaly or a new heart murmur, or both.
Causes of Anemia -- Erythrocyte Loss
May be due to: Erythrocyte loss (bleeding) Decreased Erythrocyte production
low erythropoietin Decreased marrow response to erythropoietin
Increased Erythrocyte destruction (hemolysis) The cause of the blood loss may be obvious, eg, trauma. If no evidence of external bleeding is
found, a source of internal or occult blood loss must be sought, eg, a ruptured splenic tumor, other neoplasia, coagulopathy, GI ulceration, or parasites.
Chronic bleeding (long-term bleeding) is often undetected for a long time. The patient gradually loses blood, which means a loss of red blood cells and hemoglobin.
Acute bleeding (not long term), can also reduce red blood cell count. Excessive blood loss can be caused by:
Stomach ulcers. Hemorrhoids. Inflammation of the stomach (gastritis). NSAIDS (nonsteroidal anti-inflammatory drugs) Menstruation - women who have very heavy periods (menorrhagia) have a higher
risk of developing anemia. Surgery and Trauma which results in bleeding, such as a car accident. Blood donations - some regular blood donors may develop anemia.
Anemia Due to Excessive Bleeding or Trauma
• Excessive bleeding is the most common cause of anemia. When blood is lost, the body quickly pulls water from tissues outside the bloodstream in an attempt to keep the blood vessels filled. As a result, the blood is diluted, and the hematocrit (the percentage of red blood cells in the total blood volume) is reduced. Eventually, increased production of red blood cells by the bone marrow may correct the anemia. However, over time, bleeding reduces the amount of iron in the body, so that the bone marrow is not able to increase production of new red blood cells to replace those lost.
• The symptoms may be severe initially, especially if anemia develops rapidly from a sudden loss of blood, such as from an injury, surgery, childbirth, or a ruptured blood vessel. Losing large amounts of blood suddenly can create two problems:
• Blood pressure falls because the amount of fluid left in the blood vessels is insufficient.
• The body's oxygen supply is drastically reduced because the number of oxygen-carrying red blood cells has decreased so quickly.
• Either problem may lead to a heart attack, stroke, or death.
Acute Blood Loss Acute Ulcer
Non-steroidal anti-inflammatory drugs (NSAIDs)Non-steroidal anti-inflammatory drugs (NSAIDs) can cause bleeding in the stomach. Ibuprofen and aspirin are two commonly prescribed NSAIDs.Stomach ulcersThe acid in your stomach (which helps your body to digest food) can sometimes eat into your stomach lining. When this happens, the acid forms an ulcer (an open sore). This is also known as a stomach ulcer (or a peptic ulcer). Stomach ulcers can cause your stomach lining to bleed, which leads to anaemia. In some cases, this blood loss can cause you to vomit blood or pass blood in your stools faecesAngio-dysplasiaGastrointestinal bleeding can also be caused by a condition called angiodysplasia. This is due to abnormal blood vessels in the gastrointestinal tract, which can cause bleeding.
Less common acute ulcersBleeding ulcerInternal bleeding is caused by a peptic ulcer which has been left untreated. When this happens, it is now referred to as a bleeding ulcer - this is the most dangerous type of ulcer. Esophageal ulcerThis type of ulcer occurs in the lower end of your esophagus. Esophageal ulcers are often associated with a bad case of acid reflux, or GERD as it is commonly called (short for gastro esophageal reflux disease).Stress ulcerStress ulcers are a group of lesions (or lacerations) found in the esophagus, stomach or duodenum. These are normally only found in critically ill or severely stressed patients.Refractory ulcerRefractory ulcers are simply peptic ulcers that have not healed after at least 3 months of treatment.
Chronic Ulcers A chronic ulcer is an ulcer that does not heal in an orderly set of stages and in a
predictable amount of time the way most ulcer do; ulcer that do not heal within three months are often considered chronic. Chronic ulcer seem to be detained in one or more of the phases of wound healing. For example, chronic ulcer often remain in the inflammatory stage for too long. In acute ulcer, there is a precise balance between production and degradation of molecules such as collagen; in chronic ulcer this balancee is lost and degradation plays too large a role
Classification The vast majority of chronic ulcer can be classified into three categories: venous
ulcers, diabetic, and pressure ulcers. A small number of ulcer that do not fall into these categories may be due to causes such as radiation poisoning or ischemia.
Venous and arterial ulcersVenous ulcers, which usually occur in the legs, account for about 70% to 90% of chronic ulcer and mostly affect the elderly. They are thought to be due to venous hypertension caused by improper function of valves that exist in the veins to prevent blood from flowing backward. Ischemia results from the dysfunction and, combined with reperfusion injury, causes the tissue damage that leads to the ulcer.Diabetic ulcersAnother major cause of chronic ulcer, diabetes, is increasing in prevalence. Diabetics have a 15% higher risk for amputation than the general population due to chronic ulcers. Diabetes causes neuropathy, which inhibits nociception and the perception of pain. Thus patients may not initially notice small ulcer to legs and feet, and may therefore fail to prevent infection or repeated injury. Further, diabetes causes immune compromise and damage to small blood vessels, preventing adequate oxygenation of tissue, which can cause chronic ulcer. Pressure also plays a role in the formation of diabetic ulcers.
Pressure ulcersAnother leading type of chronic ulcer is pressure ulcers, which usually occur in people with conditions such as paralysis that inhibit movement of body parts that are commonly subjected to pressure such as the heels, shoulder blades, and sacrum. Pressure ulcers are caused by ischemia that occurs when pressure on the tissue is greater than the pressure in capillaries, and thus restricts blood flow into the area. Muscle tissue, which needs more oxygen and nutrients than skin does, shows the worst effects from prolonged pressure. As in other chronic ulcers, reperfusion injury damages tissue.
Diagnosis
Chronic ulcer may affect only the epidermis and dermis, or they may affect tissues all the way to the fascia. They may be formed originally by the same things that cause acute ones, such as surgery or accidental trauma, or they may form as the result of systemic infection, vascular, immune, or nerve insufficiency, or comorbidities such as neoplasias or metabolic disorders. The reason a wound becomes chronic is that the body’s ability to deal with the damage is overwhelmed by factors such as repeated trauma, continued pressure, ischemia, or illness.
Ischemia Ischemia is an important factor in the formation and persistence of ulcer, especially
when it occurs repetitively (as it usually does) or when combined with a patient’s old age. Ischemia causes tissue to become inflamed and cells to release factors that attract neutrophils such as interleukins, chemokines, leukotrienes, and complement factors.
Pathophysiology
Bacterial colonizationSince more oxygen in the wound environment allows white blood cells to produce ROS to kill bacteria, patients with inadequate tissue oxygenation, for example those who suffered hypothermia during surgery, are at higher risk for infection. The host’s immune response to the presence of bacteria prolongs inflammation, delays healing, and damages tissue. Infection can lead not only to chronic ulcer but also to gangrene, loss of the infected limb, and death of the patient.Growth factors and proteolytic enzymesChronic ulcer also differ in makeup from acute ulcer in that their levels of proteolytic enzymes such as elastase and matrix metalloproteinases (MMPs) are higher, while their concentrations of growth factors such as Platelet-derived growth factor and Keratinocyte Growth Factor are lower.
Pathophysiology
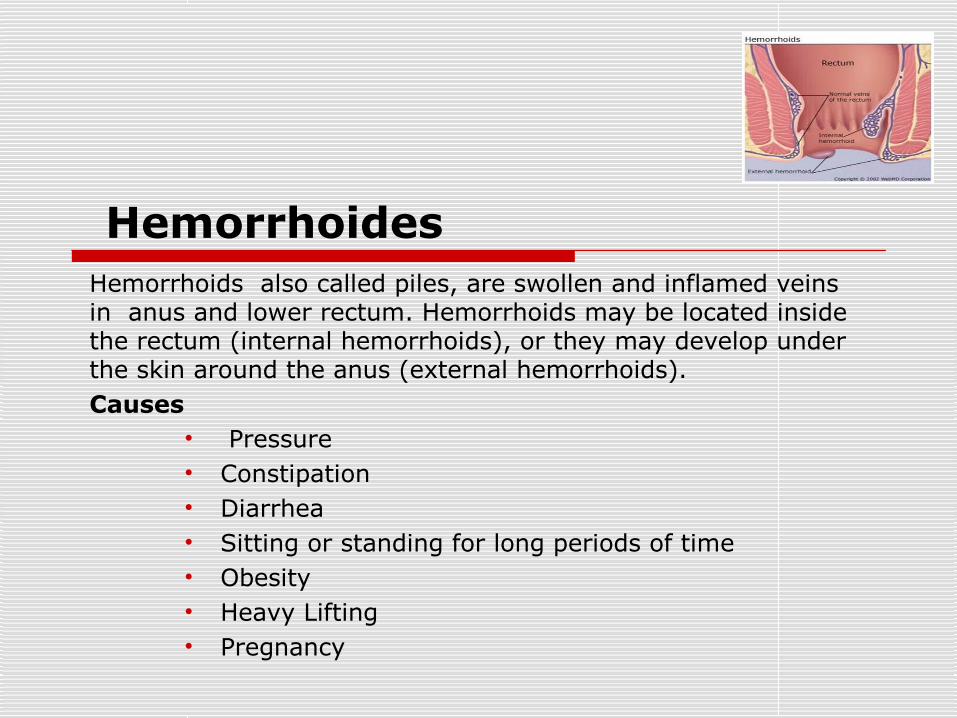
HemorrhoidesHemorrhoids also called piles, are swollen and inflamed veins in anus and lower rectum. Hemorrhoids may be located inside the rectum (internal hemorrhoids), or they may develop under the skin around the anus (external hemorrhoids).Causes
• Pressure• Constipation • Diarrhea• Sitting or standing for long periods of time• Obesity• Heavy Lifting• Pregnancy
pathophysiology
Pile mass descends – gripped by the sphincters – more engorgement. Mucosal gathering in relation to the three branches of superior rectal arteries – called anal cushions – necessary for completer continence. They slide down and internal haemorrhoids develop in the prolapsing tissues. Dilated capillaries beneath epithelium.
Symptoms
• Rectal Bleeding• Bright red blood in stool• Pain during bowel
movements• Anal Itching• Rectal Prolapse• Thrombus
Chronic Vaginal Bleeding vaginal bleeding is abnormal bleeding from the vagina
that is due to changes in hormone levels or abnormal bleeding in the absence of intracavitary or uterine pathology.
Most menstrual cycles occur every 22 to 35 days. Normal menstrual flow lasts 3 to 7 days, with most blood loss occurring within the first 3 days.
The menstrual flow amounts to 35 mL and consists of effluent debris and blood. Patients with menorrhagia lose more than 80 mL of blood with each menstrual cycle and often develop anemia.
Although approximately 16 mg of iron are lost with each menstrual cycle, this rarely results in anemia in women with adequate intake of dietary iron.
Prevalence and symptoms
Approximately 9% to 30% of reproductive-age women have menstrual irregularities requiring medical evaluation. 20% of cases occur in adolescent girls, and more than 50% occur in women older than 45.
Involve more blood loss (loss of more than about 3 ounces of blood or periods that last more than 7 days) but occur at regular intervals (menorrhagia)
Involve more blood loss and occur frequently and irregularly between menses (menometrorrhagia)
A woman may feel tired or have fatigue if she loses too much blood over time. This is a symptom of anemia.
If bleeding continues, women may develop iron deficiency and anemia.
Diagnosis:During the general examination, clinicians should look for signs of anemia (eg, conjunctival pallor).Blood tests include CBC if bleeding is unusually heavy or has lasted at least several days or if findings suggest anemia or hypovolemia. If anemia is identified and is not obviously due to iron deficiency (e.g, based on microcytic, hypochromic RBC indices), iron studies are done.
TSH, prolactin , and progesterone levels are also measured. The serum ferritin level, which reflects body iron stores, is measured if
women have chronic, heavy bleeding.Review of systems should seek symptoms of possible causes, including missed menses, breast swelling, and nausea (pregnancy-related bleeding); abdominal pain, light-headedness, and syncope (ectopic pregnancy or ruptured ovarian cyst); chronic pain and weight loss (cancer); and easy bruising and excessive bleeding due to tooth brushing or venipuncture (a bleeding disorder).Imaging includes transvaginal ultrasonography if women have any of the following:
Age > 35 Risk factors for endometrial cancer Bleeding that continues despite use of empiric hormone therapy
Treatment for Anemia caused by Vaginal bleeding
Folic acid dose: 400 to 800 mcg orally, intramuscularly, subcutaneously or IV once a day
Vitamin C dose: 75-150 mg per day Vitamin B-12 dose: 2-10
micrograms of vitamin B12 daily combined with iron and/or folic acid for up to 16 weeks and other vitamins that help build red blood cells.

Lab Findings
Serum Iron LOW (< 60 micrograms/dL)
Total Iron Binding Capacity (TIBC) HIGH ( > 360 micrograms/dL)
Serum Ferritin LOW (< 20 nanograms/mL) Can be “falsely”normal in inflammatory
states

Diagnosis Medical and Family HistoriesLet your doctor know about any medicines you take, what you typically eat (your diet), and whether you have family members who have anemia or a history of it.Physical ExamListen to your heart for a rapid or irregular heartbeatListen to your lungs for rapid or uneven breathingFeel your abdomen to check the size of your liver and spleenYour doctor also may do a pelvic or rectal exam to check for common sources of blood loss.Diagnostic Tests and ProceduresYou may have various blood tests and other tests or procedures to find out what type of anemia you have and how severe it is.

Complete Blood Count(CBC) CBC results include measurements of hemoglobin, hematocrit,
and mean corpuscular volume. Hematocrit. Hematocrit is the percentage of blood composed
of red blood cells. People with a high volume of plasma (the liquid portion of blood) may be anemic even if their blood count is normal because the blood cells have become diluted. 33% for children 6 months - 5 years 35% for children 5 - 12 years 36% for children 12 - 15 years 39% for adult men 36% for adult non-pregnant women 33% for adult pregnant women

Hemoglobin. Anemia is generally considered when hemoglobin concentrations fall below 11 g/dL for pregnant women, 12 g/dL for non-pregnant women, and 13 g/dL for men. Mild anemia is considered when hemoglobin is between 9.5 - 13.0
g/dL Moderate anemia is considered when hemoglobin is between 8.0 -
9.5 g/dL Severe anemia is considered for hemoglobin concentrations below
8.0 g/dL Mean Corpuscular Volume. Mean corpuscular volume (MCV) is a
measurement of the average size of red blood cells. The MCV increases when red blood cells are larger than normal (macrocytic) and decreases when red blood cells are smaller than normal (microcytic). Macrocytic cells can be a sign of anemia caused by vitamin B12 deficiency, while microcytic cells are a sign of iron-deficiency anemia.

Other Tests Serum Iron. Serum iron measures the amount of iron in the blood. A normal
serum iron is 60 - 170 mcg/dL. Lower levels may indicate iron-deficiency anemia or anemia of chronic disease, while higher levels may indicate hemolytic anemia or vitamin B12 deficiency.
Total Iron Binding Capacity. Total iron binding capacity (TIBC) measures the level of transferrin in the blood. Transferrin is a protein that carries iron in the blood. TIBC calculates how much or how little the transferrin in the body is carrying iron. A higher than normal TIBC is a sign of iron-deficiency anemia. A lower than normal level may indicate anemia of chronic disease, sickle cell, pernicious anemia, or hemolytic anemia.
Reticulocyte Count. Reticulocytes are young red blood cells, and their count reflects the rate of red blood cell production. The upper normal limit is about 100,000/mL. A low count, when bleeding isn't the cause, suggests production problems in the bone marrow. An abnormally high count indicates that red blood cells are being destroyed in high numbers and indicates hemolytic anemia. Recent research suggests that the reticulocyte hemoglobin content (CHr) test may be more accurate than a standard hemoglobin test for detecting iron deficiency in infants.

Complications of Anemia Pregnancy: Pregnant women who are severely anemic have a significant risk of
complications, especially when they give birth and afterwards. Giving birth often involves losing blood; being anemic already and then losing blood can result in serious complications. If a mother is severely anemic her baby is much more likely to be born prematurely and underweight. Babies born to mothers with anemia are much more likely to have problems with anemia themselves later on in infancy.
Fatigue: Fatigue may have a considerable impact on the quality of life of the patient. If the anemia is severe the patient may feel too tired to work, or carry out essential daily tasks. Long-term fatigue may eventually lead to clinical depression.
Susceptibility to illness and infection: People with untreated anemia are more susceptible to illness and infection, compared to healthy people.
Heart Problems: The heart needs to pump more blood to make up for the lack of oxygen and nutrients if you are anemic. This can eventually lead to congestive heart failure.

Treating Acute Blood LossTreating Acute Blood Loss
Stop the Bleeding
Replace fluid loss
Oxygen support
Treat underlying disorder

Stop the Bleeding
1. Assess coagulation status
2. External arterial bleeder Temporary
Cautery - silver nitrate, Kwik Stop, electrocautery
Epinephrine Permanent
Excise abnormal tissue for biopsy Reveal normal artery and ligate

Stop the Bleeding
3. Abdominal bleeder exploratory surgery as soon as vascular volume and
oxygen carrying capacity restored
4. GI bleeder Sucralfate PO – 1-3g in a slurry Barium PO – 3-5 ml/lb Endoscopic cautery surgery

Replace fluid loss
crystalloids 10 ml/lb bolus and then reassess 1-2 ml/lb/hr when hypovolemia replaced
Colloids Hetastarch
10 ml/kg over 5-15 minutes repeat once if needed
Oxyglobin 3-5 ml/kg added to fluids running at 0.5-2ml/lb/hr Or 10 ml/kg/hr for up to 3 hours
If IV access is difficult, try intraosseous

Oxygen support
Transfusion – RBC or whole blood
Oxyglobin Oxygen – nasal, flow-by, mask,
intubate

Oral iron salts Ferrous sulfate – 325 mg po Q Day
Side effects: constipation, black stools, positive hemmoccult test
Vitamin C can facilitate iron absorption.
Treat underlying disorder

Transfusion PCV threshold higher for acute blood loss
20-25% with signs of hypoxia Or if going to surgery
Improves oxygen carrying capacity May improve hemostasis
Normally, transfusion of 10 ml/lb whole blood is given over a minimum of 2 hours Pretreat with dexamethasone Give as fast as is tolerated
Collect blood from the abdomen, pass through filter and re-administer (use anticoagulant) No limitation on administration rate

Chronic Blood Loss AnemiaThe chronic diseases that are associated with this process include:Certain cancers. Examples include lymphomas and Hodgkin's disease.Autoimmune diseases. Examples include rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel disease, and polymyalgia rheumatica.Long-term infections. Examples include chronic or recurrent urinary tract infections, osteomyelitis, HIV/AIDS, hepatitis C.Liver disease. Cirrhosis can reduce the production of red blood cells. Gastrointestinal bleeding may also contribute to blood loss.Heart failure. Many patients with heart failure also have anemia. Anemia is associated with a higher risk of death in patients with heart failure. However, it is unclear whether anemia actually causes or worsens heart failure. Recent research suggests it may actually be a sign (marker) of heart failure. Iron deficiency in heart failure can be due to a number of factorsChronic kidney disease. The hormone erythropoietin (EPO) is produced in the kidneys and stimulates the bone marrow production of red blood cells. Diseased kidneys do not release sufficient amounts of EPO. Anemia can result and is universal in end-stage renal disease (kidney failure). Chronic kidney disease is a common complication of diabetes.

Chronic Blood Loss AnemiaCertain chronic diseases ulcerative colitisCancer, including lymphoma Hodgkin diseaseBreast cancerChronic kidney diseaseLong-term infections, such as bacterial endocarditis, osteomyelitis (bone infection)HIV/AIDS, hepatitis B or hepatitis C.

39
Pathogenesis Shortened red cell life span, moderately 20-30%
(from 120 to 60-90 days) Relative bone marrow(erythropoiesis) failure
- Cytokines released from inflammatory cells (TNF-α, IL-1, IFN-γ) affects erythropoiesis by inhibiting the growth of erythroid progenitors
- Serum erythropoietin levels in patiens with ACD are normal when compared to healthy subjects but much lower than levels in non-ACD anemic patients

40
Pathogenesis
ABNORMAL IRON METABOLISM• Activation of the reticuloendothelial system with increased
iron retention and storage within it• impaired release of iron from macrophages to circulating
transferrin (impaired reutilization of iron)• Reduced concentration of transferrin
(decreased production, increase sequestration in the spleen and in the foci of inflammation, increase loss )

41
Anemia of chronic disease (ACD) - symptoms
Symptoms of the underlying disease ( malignancy or chronic inflammatory disease)
Symptoms of the anemia

42
Laboratory features
The anemia is usually mild or moderate ( Hb 7-11g/dl)- lower values are observed in 20-30% of patients
The anemia is most often normochromic and normocytic (MCHC and MCV are normal)- MCV 70-80 fl in 5-40% of patients with ACD - MCHC 26-32 g/dl in 40-70%
Erythrocyte sedimentation rate (ESR) - usually rapid
Retikulocytes - most often normal or slightly decreased number, increased count is rarely

43
Laboratory features Iron metabolism
1. Serum Iron - decreased (it is necessary for the diagnosis of ACD)
2. TIBC - reduced or low-normal (N) 3. Transferrin saturation(TS) - moderately decreased ( higher than in iron-deficiency anemia), usually > 10% 4. Serum Ferritin-increased or normal 5. Serum Transferrin Receptor (sTR)-Normal 6. Sideroblasts in the bone marrow-reduced (5-20%)

Treating Chronic Blood LossTreating Chronic Blood Loss
Correct Anemia - Transfusion
Treat underlying disorder
Correct Iron Deficiency

Correct Anemia – Transfusion
Anemia severe enough to cause clinical signs (PCV <15-20%)
Or preparing for corrective surgery Conservative transfusion volume to avoid
precipitating CHF Volume overload more of a problem in cats than
in dogs Use packed cells
Correction of anemia results in resolution of cardiomegaly within several weeks

Treat Underlying Disorder
Deworm/deflea after patient is stabilized If GI Bleeding confirmed
Abdominal US Endoscopy Exploratory Laparotomy
Confirm blood loss has resolved by monitoring reticulocyte count < 40,0000/ul Retics more sensitive than anemia for chronic
blood loss

Correct Iron Deficiency
Ferrous sulfate 5 mg/lb/day PO Give with a meal Continue for weeks to months Serology to confirm iron stores are replete
TIBC – falls back to normal Transferrin – 20-60% saturated Iron – 60-230 ug/dl