Embed Size (px)
Citation preview

BASIC AIRWAY BASIC AIRWAY MANAGEMENTMANAGEMENT

Problems with airwaysProblems with airways
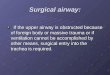
Snoring, indrawing of the supraclavicular, Snoring, indrawing of the supraclavicular, suprasternal and intercostal spaces, use suprasternal and intercostal spaces, use of the accessory muscles or paradoxical of the accessory muscles or paradoxical respiratory movement (see-saw respiratory movement (see-saw respiration) suggest that manual airway respiration) suggest that manual airway maneuvers (head tilt and jaw thrust)or maneuvers (head tilt and jaw thrust)or using oropharyngeal or nasopharyngeal using oropharyngeal or nasopharyngeal airway methods are failing to maintain a airway methods are failing to maintain a patent airway.patent airway.

Other problems with these techniques include:Other problems with these techniques include:
• • Inability to maintain a good seal between the patient’s Inability to maintain a good seal between the patient’s face and the mask, particularly in those without teeth;face and the mask, particularly in those without teeth;
• • Fatigue, when holding the mask for prolonged periods;Fatigue, when holding the mask for prolonged periods;• • The risk of aspiration, due to the loss of upper airway The risk of aspiration, due to the loss of upper airway
reflexes;reflexes;• • The anesthetist not being free to deal with any other The anesthetist not being free to deal with any other
problems that may arise.problems that may arise.
The laryngeal mask airway or tracheal intubation may be The laryngeal mask airway or tracheal intubation may be used to overcome these problems used to overcome these problems

Laryngeal mask airway (LMA)Laryngeal mask airway (LMA)
Laryngeal masks are used in anesthesia and in Laryngeal masks are used in anesthesia and in emergency medicine for airway management. They emergency medicine for airway management. They consist of a tube with an inflatable cuff that is inserted consist of a tube with an inflatable cuff that is inserted into the pharynx. They cause less pain and coughing into the pharynx. They cause less pain and coughing than an endotracheal tube, and are much easier to than an endotracheal tube, and are much easier to insert.insert. However, unlike an endotracheal tube, a laryngeal However, unlike an endotracheal tube, a laryngeal mask cannot protect the airway or lungs from mask cannot protect the airway or lungs from aspiration of regurgitated material making them aspiration of regurgitated material making them unsuitable for patients at risk for this complication, and unsuitable for patients at risk for this complication, and deep (subglottic) suctioning cannot be performed deep (subglottic) suctioning cannot be performed through the mask.through the mask.

Laryngeal mask airway (LMA)Laryngeal mask airway (LMA)
The device is useful in situations where a The device is useful in situations where a patient is trapped in a sitting position, patient is trapped in a sitting position, suspected of trauma to the cervical spine suspected of trauma to the cervical spine (where tilting the head to maintain an open (where tilting the head to maintain an open airway is contraindicated), or when airway is contraindicated), or when intubation is unsuccessful. It is not inserted intubation is unsuccessful. It is not inserted as far as an endotracheal tube (it sits tightly as far as an endotracheal tube (it sits tightly over the top of the larynx, and thus does not over the top of the larynx, and thus does not need to be inserted into the trachea), and need to be inserted into the trachea), and supports both spontaneous and artificial supports both spontaneous and artificial ventilation. It is popular in day case surgery.ventilation. It is popular in day case surgery.

Guide to useGuide to use
The cuff is deflated and the mask lightly lubricated , a The cuff is deflated and the mask lightly lubricated , a head tilt is performed, the patient’s mouth opened fully head tilt is performed, the patient’s mouth opened fully and the tip of the mask inserted along the hard palate and the tip of the mask inserted along the hard palate with the open side facing but not touching the tongue. with the open side facing but not touching the tongue. The mask is further inserted, using the index finger to The mask is further inserted, using the index finger to provide support for the tube. Eventually, resistance will provide support for the tube. Eventually, resistance will be felt at the point where the tip of the mask lies at the be felt at the point where the tip of the mask lies at the upper esophageal sphincter upper esophageal sphincter The cuff is now fully inflated using an air-filled syringe The cuff is now fully inflated using an air-filled syringe attached to the valve at the end of the pilot tube, air entry attached to the valve at the end of the pilot tube, air entry is confirmed by listening for air entry into the lungs with a is confirmed by listening for air entry into the lungs with a stethoscope, or by presence of end tidal carbon dioxide.stethoscope, or by presence of end tidal carbon dioxide.. • The laryngeal mask is secured either by a length of . • The laryngeal mask is secured either by a length of bandage or adhesive strapping attached to the bandage or adhesive strapping attached to the protruding tubeprotruding tube



Tracheal intubationTracheal intubation
This is the best method of providing and securing a This is the best method of providing and securing a clear airway in patients during anesthesia and clear airway in patients during anesthesia and resuscitation, but success requires abolition of the resuscitation, but success requires abolition of the laryngeal reflexes.laryngeal reflexes. During anesthesia, this is usually achieved by the During anesthesia, this is usually achieved by the administration of a muscle relaxant. Deep inhalational administration of a muscle relaxant. Deep inhalational anesthesia or local anesthesia of the larynx can also be anesthesia or local anesthesia of the larynx can also be used, but these are usually reserved for patients where used, but these are usually reserved for patients where difficulty with intubation is anticipated, for example in the difficulty with intubation is anticipated, for example in the presence of airway tumors or immobility of the cervical presence of airway tumors or immobility of the cervical spine.spine.

Common indications for tracheal intubationCommon indications for tracheal intubation
1-To maintain patent airway1-To maintain patent airway • •Unconscious (GCS<8)Unconscious (GCS<8) • • Where the position of the patient would make airway maintenance difficult, for Where the position of the patient would make airway maintenance difficult, for
example the lateral or prone position.example the lateral or prone position. • •Where there is competition between surgeon and anesthetist for the airway (e.g. Where there is competition between surgeon and anesthetist for the airway (e.g.
operations on the head and neck).operations on the head and neck). • • In those patients in whom the airway cannot be satisfactorily maintained by any In those patients in whom the airway cannot be satisfactorily maintained by any
other technique e.g. obese patient, beard patientother technique e.g. obese patient, beard patient • • During cardiopulmonary resuscitationDuring cardiopulmonary resuscitation 2-To allow ventilation 2-To allow ventilation • • Where muscle relaxants are used to facilitate surgery (e.g. abdominal and Where muscle relaxants are used to facilitate surgery (e.g. abdominal and
thoracic surgery), thereby necessitating the use of mechanical ventilation.thoracic surgery), thereby necessitating the use of mechanical ventilation. • • Where controlled ventilation is utilized to improve surgical access (e.g. Where controlled ventilation is utilized to improve surgical access (e.g.
neurosurgeryneurosurgery • •Patient with respiratory failure Patient with respiratory failure • • To minimize the dose of volatile agent and /or allow large doses of narcoticsTo minimize the dose of volatile agent and /or allow large doses of narcotics 3-To prevent aspiration3-To prevent aspiration • • In patients with a full stomach, (emergency operation, Caesarian section, uremic, In patients with a full stomach, (emergency operation, Caesarian section, uremic,
diabetic gastroparesis, obese) to protect against aspiration.diabetic gastroparesis, obese) to protect against aspiration. 4-Allow bronchial suction4-Allow bronchial suction

Observation of the patient’s anatomyObservation of the patient’s anatomy
Look for:Look for: • • Limitation of mouth opening;Limitation of mouth opening; • • A receding mandible;A receding mandible; • • Position, number and health of teeth;Position, number and health of teeth; • • Size of the tongue;Size of the tongue; • • Soft tissue swelling at the front of the neck;Soft tissue swelling at the front of the neck; • • Deviation of the larynx or trachea;Deviation of the larynx or trachea; • • Limitations in flexion and extension of the cervical spine.Limitations in flexion and extension of the cervical spine. Finding any of these suggests that intubation may be more Finding any of these suggests that intubation may be more
difficult. However, it must be remembered that all of difficult. However, it must be remembered that all of these are subjective.these are subjective.

Simple bedside testsSimple bedside tests
• • Mallampati criteria Mallampati criteria The patient, sitting upright, is asked to open The patient, sitting upright, is asked to open his mouth and maximally protrude his tongue. The view of the his mouth and maximally protrude his tongue. The view of the pharyngeal structures is noted and graded I–IV pharyngeal structures is noted and graded I–IV
Grades III and IV suggest difficult intubation.Grades III and IV suggest difficult intubation. • • Thyromental distance Thyromental distance With the head fully extended on the With the head fully extended on the
neck, the distance between the bony point of the chin and the neck, the distance between the bony point of the chin and the prominence of the thyroid cartilage is measured. A distance of prominence of the thyroid cartilage is measured. A distance of less than 7 cm suggests difficult intubation.less than 7 cm suggests difficult intubation.
None of these tests, alone or in combination, predicts all None of these tests, alone or in combination, predicts all difficult intubations. A Mallampati grade III or IV with a difficult intubations. A Mallampati grade III or IV with a thyromental distance of <7cm predict 80% of difficult thyromental distance of <7cm predict 80% of difficult intubations.intubations.
If problems are anticipated, anesthesia should be planned If problems are anticipated, anesthesia should be planned accordingly.accordingly.
If intubation proves to be difficult, it must be recorded in a If intubation proves to be difficult, it must be recorded in a prominent place in the patient’s notes and the patient informed.prominent place in the patient’s notes and the patient informed.



Routes for IntubationRoutes for Intubation
OrotrachealOrotracheal
NasotrachealNasotracheal
TracheotomyTracheotomy

Oral IntubationOral Intubation

Equipment for tracheal intubationEquipment for tracheal intubation
The equipment used will be determined by the The equipment used will be determined by the circumstances and by the preferences of the individual circumstances and by the preferences of the individual anesthetist. anesthetist.
The following is a list of the basic needs for The following is a list of the basic needs for adult oral adult oral intubation.intubation.
• • LaryngoscopeLaryngoscope: with a curved (Macintosh) blade and : with a curved (Macintosh) blade and functioning light.functioning light.
LaryngoscopeLaryngoscope It’s a rigid instrument used to examine the larynx and to It’s a rigid instrument used to examine the larynx and to
facilitate intubation of the trachea.facilitate intubation of the trachea. The laryngoscope is held in your non dominant hand The laryngoscope is held in your non dominant hand
carefully introduce the blade into the right side of the mouth carefully introduce the blade into the right side of the mouth (Never press against the teeth), the tongue is then swept to (Never press against the teeth), the tongue is then swept to the left and up into the flour of pharynx by the bladethe left and up into the flour of pharynx by the blade ’’s s flange and advancing the blade toward the glottic opening flange and advancing the blade toward the glottic opening then pass the tube into the right side of the mouth and then pass the tube into the right side of the mouth and through the vocal cords (using the dominant hand) through the vocal cords (using the dominant hand)

• • Tracheal tubes (cuffed)Tracheal tubes (cuffed): in a variety of sizes. : in a variety of sizes. The internal diameter is expressed in millimeters The internal diameter is expressed in millimeters and the length in centimeters. They may be and the length in centimeters. They may be lightly lubricated.lightly lubricated.
• • For males: 8.0–9.0mm internal diameter, 22–For males: 8.0–9.0mm internal diameter, 22–24cm length24cm length
• • For females: 7.5–8.5mm internal diameter, 20–For females: 7.5–8.5mm internal diameter, 20–22cm length.22cm length.
• • SyringeSyringe: to inflate the cuff once the tube is in : to inflate the cuff once the tube is in place.place.
• • Catheter mountCatheter mount: or ‘elbow’ to connect the tube : or ‘elbow’ to connect the tube to the anesthetic system or ventilator tubing.to the anesthetic system or ventilator tubing.
• • SuctionSuction: switched on and immediately to hand : switched on and immediately to hand in case the patient vomits or regurgitates.in case the patient vomits or regurgitates.

• • StethoscopeStethoscope: to check correct placement : to check correct placement of the tube by listening for breathe sounds of the tube by listening for breathe sounds during ventilationduring ventilation
• • ExtrasExtras: a semi-rigid introducer to help : a semi-rigid introducer to help mould the tube to a particular shape;mould the tube to a particular shape;
Magill’s forceps, designed to reach into Magill’s forceps, designed to reach into the pharynx to remove debris or direct the the pharynx to remove debris or direct the tip of a tube; bandage or tape to secure tip of a tube; bandage or tape to secure the tube.the tube.

Visualization of Vocal CordsVisualization of Vocal Cords

Tracheal tubesTracheal tubes
Mostly manufactured from plastic (PVC), and for single use Mostly manufactured from plastic (PVC), and for single use to eliminate cross-infection to eliminate cross-infection
They are available in 0.5mm diameter intervals, and long They are available in 0.5mm diameter intervals, and long enough to be used orally or nasally. A standard 15mm enough to be used orally or nasally. A standard 15mm connector is provided to allow connection to the connector is provided to allow connection to the breathing system.breathing system.
In adult anesthesia, a tracheal tube with an inflatable cuff In adult anesthesia, a tracheal tube with an inflatable cuff is used to prevent leakage of anesthetic gases back past is used to prevent leakage of anesthetic gases back past the tube when positive pressure ventilation is used. This the tube when positive pressure ventilation is used. This also helps prevent aspiration of any foreign material into also helps prevent aspiration of any foreign material into the lungs.the lungs.
The cuff is inflated by injecting air via a pilot tube, at the The cuff is inflated by injecting air via a pilot tube, at the distal end of which is a one-way valve to prevent distal end of which is a one-way valve to prevent deflation and a small ‘balloon’ to indicate when the cuff is deflation and a small ‘balloon’ to indicate when the cuff is inflated.inflated.

A wide variety of specialized tubes have been A wide variety of specialized tubes have been developeddeveloped
• • Reinforced tubes Reinforced tubes are used to prevent kinking and subsequent are used to prevent kinking and subsequent
obstruction as a result of the positioning of the patient’s head obstruction as a result of the positioning of the patient’s head • • Preformed tubes Preformed tubes are used during surgery on the head and are used during surgery on the head and
neck, and are designed to take the connections away from the neck, and are designed to take the connections away from the surgical field surgical field
• • Double lumen tubes Double lumen tubes are effectively two tubes welded together are effectively two tubes welded together side-by-side, with one tube extending distally beyond the other.side-by-side, with one tube extending distally beyond the other.
They are used during thoracic surgery, and allow one lung to They are used during thoracic surgery, and allow one lung to be deflated whilst ventilation is maintained via the bronchial be deflated whilst ventilation is maintained via the bronchial portion in the opposite lung portion in the opposite lung
• • Uncuffed tubes Uncuffed tubes are used in children up to approximately 10 are used in children up to approximately 10 years of age as the narrowing in the subglottic region provides years of age as the narrowing in the subglottic region provides a natural seal a natural seal

Endotracheal TubeEndotracheal Tube



The technique of oral intubationThe technique of oral intubation
PreoxygenationPreoxygenation
All patients who are to be intubated are asked to All patients who are to be intubated are asked to breathe 100% oxygen via a close-fitting breathe 100% oxygen via a close-fitting facemask for 2–3 mins (‘preoxygenation’). This facemask for 2–3 mins (‘preoxygenation’). This provides a reservoir of oxygen in the patient’s provides a reservoir of oxygen in the patient’s lungs, reducing the risk of hypoxia if difficulty is lungs, reducing the risk of hypoxia if difficulty is encountered with intubation. Once this has been encountered with intubation. Once this has been accomplished, the appropriate drugs will be accomplished, the appropriate drugs will be administered to render the patient unconscious administered to render the patient unconscious and abolish laryngeal reflexes.and abolish laryngeal reflexes.

PositioningPositioning
The patient’s head is placed on a small The patient’s head is placed on a small pillow with the neck flexed and the head pillow with the neck flexed and the head extended at the atlanto-occipital joint, the extended at the atlanto-occipital joint, the ‘sniffing the morning air’ position. The ‘sniffing the morning air’ position. The patient’s mouth is fully opened using the patient’s mouth is fully opened using the index finger and thumb of the index finger and thumb of the right right hand in hand in a scissor action.a scissor action.

Patient PositioningPatient PositioningGoalGoal
Align 3 planes of Align 3 planes of view, so vocal view, so vocal cords are most cords are most visiblevisible
T - tracheaT - trachea
P - PharynxP - Pharynx
O - OropharynxO - Oropharynx

Patient PositioningPatient Positioning


LaryngoscopeLaryngoscope
The laryngoscope is held in the leftThe laryngoscope is held in the left hand and hand and the blade introduced into the mouth along the the blade introduced into the mouth along the right side of the tongue, displacing it to the left. right side of the tongue, displacing it to the left. The blade is advanced until the tip lies in the The blade is advanced until the tip lies in the gap between the base of the tongue and the gap between the base of the tongue and the epiglottis, the vallecula. Force is then applied in epiglottis, the vallecula. Force is then applied in the direction in which the handle of the the direction in which the handle of the laryngoscope is pointinglaryngoscope is pointing. . The effort comes The effort comes from the upper arm not the wrist, to lift the from the upper arm not the wrist, to lift the tongue and epiglottis to expose the larynx, tongue and epiglottis to expose the larynx, seen as a triangular opening with the apex seen as a triangular opening with the apex interiorly and the whitish coloured true cords interiorly and the whitish coloured true cords laterallylaterally

LaryngoscopeLaryngoscope

Curved bladeCurved blade

Straight bladeStraight blade

IntubationIntubation
The tracheal tube is introduced into the right The tracheal tube is introduced into the right side of the mouth, advanced and seen to pass side of the mouth, advanced and seen to pass through the cordsthrough the cords until the cuff lies just below until the cuff lies just below the cords. The tube is then held firmly and the the cords. The tube is then held firmly and the laryngoscope is carefully removed, and the cuff laryngoscope is carefully removed, and the cuff is inflated sufficiently to prevent any leak during is inflated sufficiently to prevent any leak during ventilation. Finally the position of the tube is ventilation. Finally the position of the tube is confirmed and secured in place. confirmed and secured in place.

For nasotracheal intubation a well-lubricated For nasotracheal intubation a well-lubricated tube is introduced, usually via the right nostril tube is introduced, usually via the right nostril along the floor of the nose with the bevel along the floor of the nose with the bevel pointing medially to avoid damage to the pointing medially to avoid damage to the turbinates. It is advanced into the oropharynx, turbinates. It is advanced into the oropharynx, where it is usually visualized using a where it is usually visualized using a laryngoscope in the manner described above. laryngoscope in the manner described above. It can then either be advanced directly into the It can then either be advanced directly into the larynx by pushing on the proximal end, or the larynx by pushing on the proximal end, or the tip picked up with Magill’s forceps (which are tip picked up with Magill’s forceps (which are designed not to impair the view of the larynx) designed not to impair the view of the larynx) and directed into the larynx. The procedure and directed into the larynx. The procedure then continues as for oral intubation.then continues as for oral intubation.

Nasal IntubationNasal Intubation

Confirming the position of the tracheal tubeConfirming the position of the tracheal tube
This can be achieved using a number of This can be achieved using a number of techniques:techniques:
• • Measuring the carbon dioxide in expired gas Measuring the carbon dioxide in expired gas (capnography)(capnography)::
Less than 0.2% indicates esophageal intubation.Less than 0.2% indicates esophageal intubation.
• • Direct visualizationDirect visualization: of the tracheal tube passing : of the tracheal tube passing between the vocal cords.between the vocal cords.
• • FoggingFogging: on clear plastic tube connectors during : on clear plastic tube connectors during expiration.expiration.

Less reliable signs areLess reliable signs are
• • Diminished breath sounds on auscultation;Diminished breath sounds on auscultation;• • decreased chest movement on ventilation;decreased chest movement on ventilation;• • gurgling sounds over the epigastrium and gurgling sounds over the epigastrium and
‘Burping’ sounds as gas escapes;‘Burping’ sounds as gas escapes;• • A decrease in oxygen saturation detected by A decrease in oxygen saturation detected by
pulse oximetry. This occurs late, particularly if pulse oximetry. This occurs late, particularly if the patient has been preoxygenated.the patient has been preoxygenated.

Complications of tracheal intubationComplications of tracheal intubation
The following complications are the more common ones, not The following complications are the more common ones, not an attempt to cover all occurrences.an attempt to cover all occurrences.
HypoxiaHypoxia Due to:Due to: • • Unrecognized Unrecognized eesophageal intubationsophageal intubation If there is any doubt about the position of the tube it should If there is any doubt about the position of the tube it should
be removed and the patient ventilated via a facemask.be removed and the patient ventilated via a facemask. • • Failed intubation and inability to ventilate the patientFailed intubation and inability to ventilate the patient This is usually a result of abnormal anatomy or airway This is usually a result of abnormal anatomy or airway
pathology. Many cases are predictable at the preoperative pathology. Many cases are predictable at the preoperative assessment assessment
• • Failed ventilation after intubationFailed ventilation after intubation Possible causes include the tube becoming kinked, Possible causes include the tube becoming kinked,
disconnected, or inserted too far and passing into one main disconnected, or inserted too far and passing into one main bronchus; severe bronchospasm and tension pneumothorax.bronchus; severe bronchospasm and tension pneumothorax.

• • Aspiration Aspiration Regurgitated gastric contents can cause blockage Regurgitated gastric contents can cause blockage
of the airways directly, or secondary to laryngeal of the airways directly, or secondary to laryngeal spasm and bronchospasm. spasm and bronchospasm.
Cricoid pressure can be used to reduce the risk of Cricoid pressure can be used to reduce the risk of regurgitation prior to intubationregurgitation prior to intubation
TraumaTrauma
• • Direct Direct During laryngoscope and insertion of the During laryngoscope and insertion of the tube, damage to lips, teeth, tongue, pharynx, larynx, tube, damage to lips, teeth, tongue, pharynx, larynx, trachea, and nose and nasopharynx during nasal trachea, and nose and nasopharynx during nasal intubation; causing soft tissue swelling or bleeding.intubation; causing soft tissue swelling or bleeding.
• • Indirect Indirect To the recurrent laryngeal nerves, and the To the recurrent laryngeal nerves, and the cervical spine and cord, particularly where there is cervical spine and cord, particularly where there is pre-existing degenerative disease or trauma.pre-existing degenerative disease or trauma.

Reflex activityReflex activity • • Hypertension and arrhythmias Hypertension and arrhythmias Occurs in response to Occurs in response to
laryngoscope and intubation. May jeopardize patients with laryngoscope and intubation. May jeopardize patients with coronary artery disease coronary artery disease
In patients at risk, specific action is taken to attenuate the In patients at risk, specific action is taken to attenuate the response; for example pretreatment with beta blockers or response; for example pretreatment with beta blockers or potent analgesics (fentanyl, remifentanil).potent analgesics (fentanyl, remifentanil).
• • Vomiting Vomiting This may be stimulated when laryngoscopy is This may be stimulated when laryngoscopy is attempted in patients who are inadequately anaesthetized. It is attempted in patients who are inadequately anaesthetized. It is more frequent when there is material in the stomach; for more frequent when there is material in the stomach; for example in emergencies when the patient is not starved, in example in emergencies when the patient is not starved, in patients with intestinal obstruction, or when gastric emptying is patients with intestinal obstruction, or when gastric emptying is delayed, as after opiate analgesics or following trauma.delayed, as after opiate analgesics or following trauma.
• • Laryngeal spasm Laryngeal spasm Reflex adduction of the vocal cords as a Reflex adduction of the vocal cords as a result of stimulation of the epiglottis or larynxresult of stimulation of the epiglottis or larynx