Embed Size (px)
Citation preview

Oral anticoagulant therapy in AF – which one is best?
Dr. Pavankumar P Rasalkar

Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia.
The estimated number of individuals with AF globally in 2010 was 33∙5 million 20∙9 million males and 12∙6 million females .
Prevalence: 596.7/100000 in males 373.1/100000 in females Incidence: 77.5/100000 in males 59.5/100000 in females
Introduction
Sumeet S.Chugh etal CIRCULATIONAHA.113.005119 December 17, 2013,

AF is associated with a 5-fold increased risk of stroke
AF is also associated with a 3-fold risk of HF
2-fold increased risk of both dementia and mortality
HF : Heart Failure

Types of AFFirst diagnosed episode of AF
Paroxysmal (<7 days)
Persistent (>7 days to
12m)
Long standing
persistent (>1year)
Permanent (accepted)

Management strategy
Atrial fibrillation
Anticoagulation Assess TE riskNOACOAC
Aspirin or none
Rate and rhythm control AF type symptoms
Rate control+/- Rhythm control
Ablation

ANTICOAGULATION

CHADS2
C congestive cardiac
failure
H Hypertension
AAge more than 75
D
Diabetes
S2 Previous Stroke or
TIA
Thromboembolic risk
Gage BF, Waterman AD et. al. JAMA 2001;285:2864–2870

CHADS2Age 65-74
Vascular diseaseFemale
CHA2DS2-VASc

Risk Profile Class / LevelCHA2DS2-VASc = 0 No antithrombotic therapy
Class IIa
CHA2DS2-VASc = 1
No antithrombotic therapy Or
AsprinOr
Oral anticoagulation Class IIb
CHA2DS2-VASc ≥ 2 Oral anticoagulationClass I
Indication for anticoagulation in non valvular AF patients

Risk of bleedingH- HypertensionA- Abnormal renal or liver function
(1 point each)S- StrokeB- BleedingL- Labile INRE- Elderly, Age >65D- Drugs or alcohol (1 point each)
INR . international normalized ratio

VKA

Warfarin

Warfarin
Kinetics Absorption Oral: Rapid, complete
Distribution 0.14 L/kgMetabolism Hepatic, primarily via CYP2C9;
minor pathways include CYP2C8, 2C18, 2C19, 1A2, and 3A4
Excretion Urine (92%, primarily as metabolites)
Half-life 20-60 hours

Warfarin Onset of action:
◦ 5-7 days ◦ May requiring bridging
Antidote: ◦ Vitamin K, FFP, PRBC
Interactions:◦ Foods with high vitamin K content

Warfarin
Medications ◦ Amiodarone◦ Antiplatelets ◦ Azole antifungals
(fluconazole)◦ 2nd/3rd-gen Cephalosporins◦ Fluoroquinolones
(ciprofloxacin)◦ Griseofulvin◦ Isoniazid◦ Macrolides (clarithromycin)◦ Metronidazole◦ NSAIDs
◦ Penicillins (nafcillin)◦ Prednisone ◦ Rifampin ◦ SSRIs◦ Sulfonamides (Bactrim)◦ Tetracyclines (Doxycycline )
Herbals ◦ Ginger◦ Gingko ◦ Fenugreek◦ Chamomile◦ St. John’s Wort

Warfarin ADRs
◦ Bleeding/Hemorrhage/Hematuria◦ Vasculitis◦ Dermatitis, pruritus, urticaria◦ Abdominal pain, N/V/D ◦ Anemia◦ Skin necrosis, gangrene, “purple toes” syndrome

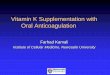
Hart R, et al. Ann Intern Med 1999;131:492
WarfarinBetter
ControlBetter
AFASAK
SPAFBAATAF
CAFA
SPINAF
EAFT
100% 50% 0 -50% -100%
Aggregate
Warfarin in atrial fibrillation

VKA
Similar to Warfarin
Lesser pharmacogenimic interaction (VKORC1 and CYP2C9)
Lesser food and drug interactions
Higher potency and longer half life
Acitrom

Difficulties with warfarin use Requires monitoring Numerous drug and diet interactions Narrow therapeutic range Difficult to control – takes time to get in or out of
the system
Role for new anticoagulants?

New anticoagulants
Leung, The Hematologist, 2011

New anticoagulants Ideal anticoagulant:
◦ Equally efficacious◦ Equally safe◦ No monitoring◦ Fewer interactions◦ Oral◦ Reversible

New anticoagulants Direct thrombin inhibitors
◦ Dabigatran
Factor Xa inhibitors◦ Rivaroxaban◦ Apixaban◦ Edoxaban

Absorption and metabolism of NOACDabigatran Apixaban Rivaroxaban
Bioavailability 3-7% 50% 66% (w/o food) ~100% with food
Prodrug yes no no
Clearance: non-renal/renal of adsorbed dose if normal renal function
20%/80% 73%/27% 65%/35%
Liver metabolism: CYP3A4 no yes (elimination; minor CYP3A4) yes (elimination)
Absorption with food no effect no effect +39%
Intake with food? no no mandatory
Absorption with H2B/PPI plasma level -12 to -30% no effect no effect
Asian ethnicity plasma level +25% no effect no effect
GI tolerability dyspepsia 5-10% no problem no problem
Elimination half-life 12-17h 12h 5-9h (young)/11-13h (elderly)16
www.escardio.org/EHRA

Mechanisms underlying DDIs in NOACs
P-glycoprotein transporter involved in absorption and renal clearance – plasma levels may be affected by P-gp inducers or inhibitors1
Cytochrome P450 CYP3A4 involved in hepatic
clearance of rivaroxaban and apixaban – plasma levels may be affected by CYP3A4 inducers of inhibitors2
17
1. Gnoth et al, J Pharmacol Exp Ther 2011;338:372-80 2. Mueck et al, Br J Clin Pharmacol 2013

Action to be taken in case of DDIsThree levels of alert: Red – contraindicated/not recommended for use Orange – adapt NOAC dose
◦ dabigatran: 150 mg to 110 mg BID◦ rivaroxaban: 20 mg to 15 mg QD◦ apixaban: 5 mg to 2.5 mg BID
Yellow – consider dose reduction if two concomitant yellow interactions
Where no data available, NOACs not recommended yet
18
www.escardio.org/EHRA

Possible drug-drug interactions – Effect on NOAC plasma levels
Dabigatran Apixaban Edoxaban Rivaroxaban
Atorvastatin P-gp/ CYP3A4 +18% no data yet no effect no effect
Digoxin P-gp no effect no data yet no effect no effect
Verapamil P-gp/ wk CYP3A4 +12–180% no data yet
+ 53% (slow release) minor effect
Diltiazem P-gp/ wk CYP3A4 no effect +40% No data minor effect
Quinidine P-gp +50% no data yet +80% +50%
Amiodarone P-gp +12–60% no data yet no effect minor effect
Dronedarone P-gp/CYP3A4 +70–100% no data yet +85% no data yet
Ketoconazole; itraconazole; voriconazole; posaconazole;
P-gp and BCRP/ CYP3A4 +140–150% +100% no data yet up to +160%
19
www.escardio.org/EHRA
Red – contraindicated; orange – reduce dose; yellow – consider dose reduction if another yellow factor present; hatching – no data available; recommendation made from pharmacokinetic considerations

Possible drug-drug interactions – Effect on NOAC plasma levels
Dabigatran Apixaban Edoxaban Rivaroxaban
Atorvastatin P-gp/ CYP3A4 +18% no data yet no effect no effect
Digoxin P-gp no effect no data yet no effect no effect
Verapamil P-gp/ wk CYP3A4 +12–180% no data yet
+ 53% (slow release) minor effect
Diltiazem P-gp/ wk CYP3A4 no effect +40% No data minor effect
Quinidine P-gp +50% no data yet +80% +50%
Amiodarone P-gp +12–60% no data yet no effect minor effect
Dronedarone P-gp/CYP3A4 +70–100% no data yet +85% no data yet
Ketoconazole; itraconazole; voriconazole; posaconazole;
P-gp and BCRP/ CYP3A4 +140–150% +100% no data yet up to +160%
19
www.escardio.org/EHRA
Red – contraindicated; orange – reduce dose; yellow – consider dose reduction if another yellow factor present; hatching – no data available; recommendation made from pharmacokinetic considerations

Possible drug-drug interactions – Effect on NOAC plasma levels
Interaction Dabigatran Apixaban Rivaroxaban
Fluconazole CYP3A4 no data no data +42%Cyclosporin; tacrolimus P-gp no data no data +50%Clarithromycin; erythromycin P-gp/ CYP3A4 +15–20% no data +30–54%
HIV protease inhibitors
P-gp and BCRP/ CYP3A4 no data strong increase up to +153%
Rifampicin; St John’s wort; carbamezepine; phenytoin; phenobarbital
P-gp and BCRP/ CYP3A4/CYP2J2 -66% -54% up to -50%
Antacids GI absorption -12-30% no data no effect
20
www.escardio.org/EHRARed – contraindicated; orange – reduce dose; yellow – consider dose reduction if another yellow factor present;hatching – no data available; recommendation made from pharmacokinetic considerations

Factors associated with raised plasma levels of NOACs
Dabigatran Apixaban RivaroxabanAged ≥ 80 years Increased plasma level
Aged ≥ 75 years Increased plasma level
Weight ≤ 60 kg Increased plasma level
Renal function Increased plasma level
21
Other increased bleeding risk
Pharmacodynamic interactions – antiplatelet drugs, NSAIDs Systemic steroid therapy Other anticoagulantsRecent surgery on critical organ (brain, eye)Thrombocytopenia (e.g. chemotherapy)HAS-BLED ≥ 3
Orange – reduce dose; yellow – consider dose reduction if another yellow factor present;hatching – no data available; recommendation made from pharmacokinetic considerations

Clinical Evidence

RE-LY ROCKET-AF ARISTOTLE
Dabigatran 150mg
BID vs. warfarin
Rivaroxaban 20mg daily
vs. warfarinApixaban5mg BID
vs. warfarinStudy Design
Trial design RCT Open blinded assessment RCT DB DD RCT DB DD
Sample size (n) 18,000+ 14,000+ 18,000+
Inclusion criteria AF and selected risk factor(s) for embolization
AF and CHADS2 ≥2
AF or flutter and CHADS2 ≥1
Key exclusion criteria
Valvular AFUse of ASA ≥100 mg/dayCrCl <30 ml/min
Valvular AF;Use of ASA >100 mg/dayCrCl <30 ml/min
Valvular AFNeed for ASA >165 mg/daySCr >2.5mg/dL or CrCl <25ml/min
Follow-up (mean) 2 yr 1.9 yr 1.8 yrOutcome Definitions
Primary Efficacy Composite of systemic embolism and stroke (ischemic or hemorrhagic)Major Bleeding ISTH: fatal/critical organ bleed; decrease ≥2g/dL Hbg or transfusion of ≥2U bloodMortality All causes
Baseline CharacteristicsAge (years) 71 (mean) 73 (median) 70 (median) Female (%) 36.4% 39.7% 35.2 %CHADS2 (mean) 2.1 3.5 2.1Previous embolic episode (%)
20% (stroke or TIA only)
55%(stroke,TIA, systemic
embolism)19%
(stroke, TIA, systemic embolism)
TTR (%) (Standard 60-65%) 64% 55% 62%

Comparison of Efficacy Results RE-LY ROCKETAF ARISTOTLE
Outcome (%/year)Dabigatran 150mg BID
vs. warfarin
p Value
Rivaroxaban 20mg
daily vs.
warfarin
p ValueApixaban 5mg BID
vs. warfarin
p Value
Primary OutcomeStroke or systemic embolism
1.1 vs. 1.7%
p<0.001 NNT 88
2.1 vs. 2.4% p=0.12 1.3 vs.
1.6%
p=0.01
NNT 167
Stroke 1.0 vs. 1.6%
p<0.001NNT 88
1.65 vs. 1.96% p=0.09 1.2 vs.
1.5%
p=0.01
NNT 175
Ischemic stroke 0.9 vs. 1.3%
p=0.03NNT 132 1.3 vs. 1.4 p=0.58 0.97 vs.
1.05%p=0.4
2
Hemorrhagic stroke 0.1vs0.4% p<0.001
NNT 1820.26 vs. 0.44%
p=0.02NNT 333
0.24 vs. 0.47%
p<0.001
NNT 238
All cause death 3.6 vs. 4.1% p=0.051 4.5 vs.
4.9% p=0.15 3.5 vs. 3.9p=0.0
47NNT 132
MI/ACS 0.7 vs. 0.5%
p=0.048NNH 239
0.9 vs. 1.1% p=0.12 0.5 vs.
0.6%p=0.3
7

Comparison of Safety Results
RE-LY ROCKETAF ARISTOTLE
Major bleed 3.1 vs. 3.36% p=0.31 3.6 vs.
3.4% p=0.58 2.1 vs. 3.1%
p<0.001NNT 67
Intracranial bleed
0.3 vs. 0.74%
p<0.001
NNT 116
0.5 vs. 0.7%
p=0.02NNT 250
0.3 vs. 0.8%
p<0.001NNT 128
GI bleed 1.5 vs. 1.0%
p<0.001
NNH 100
3.2 vs. 2.2%**
p=0.001NNH 100
0.76 vs. 0.86% 0.37

Factor Xa inhibitor
Doses 60mg and 30mg OD
Engage AF trial(November 2013, NEJM)◦ Versus Warfarin, RCT DD ◦ More than 20000 subjects◦ Non inferior◦ Less major bleed
Edoxaban

Boxed warning: Less effective in pateints with CrCl >95ml/min, as it was associated with more thromboembolic complications compared to warfarin. Also contraindicated if CrCl < 15ml/mim
Was FDA approved in January 2015
Approved by European union in June 2015
Savaysa (USA), Lixiana(Europe)
Edoxaban

All major trials excluded Valvular AF
Re-Align AF◦ RCT, Nejm 2013◦ Dabigatran vs Warfarin in prosthetic heart valve◦ Significantly increased bleeding◦ Significantly increased thromboembolism◦ Stopped prematurely
NOAC’S in valvular AF

NOAC’s Vs Warfarin which one is better?

Wafarin
Advantages Disadvantages
Cheap: 2rs/5mg Antidote available Robust data(Class IA) Time tested
Narrow TI/Non target INR
Frequent INR monitoring
Numerous drug-drug and drug-food interactions
Slow onset and offset of action/ Requires bridging

NOAC’S
Advantages Disadvantages
Quick onset/offset of action
Few drug-drug and drug-food interactions
No need of monitoring
Cost◦ Dabigatran
(Pradaxa:71.8rs/150 or 110mg)
◦ Apixaban (Equilis: 72.5 rs)
◦ Rivaroxaban (Xarelto: 240rs)
No antidote
Less robust data (Class IB)

Patient not willing for regular INR
Patient preferance
Target INR not achieved with warfarin
NOAC’S considered in

Atrial Fibrillation
Valvular AF?
Non Valvular AF?
Warfarin IB
Undergoing Procedure
CHA2DS2-VASc IB1In patients with AF, antithrombotic therapy should be individualized based on shared decision making after discussion of the absolute and RRs of stroke and bleeding, and the patient’s values and preferences. IC2. Selection of antithrombotic therapy should be based on the risk of thromboembolism irrespective of whether the AF pattern is paroxysmal, persistent, or permanent IB.
Among patients treated with warfarin, the INR should be determined at least weekly during initiation of antithrombotic therapy and at least monthly when anticoagulation (INR in range) is stable IA
Bridging therapy with unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) is recommended for patients with AF and a mechanical heart valve undergoing procedures that require interruption of warfarin. Decisions regarding bridging therapy should balance the risks of stroke and bleeding. IC
The direct thrombin inhibitor, dabigatran, should not be used in patients with AF and a mechanical heart valve IIIB

Non Valvular AF?
Warfarin Direct thrombin ,Factor Xa inhibitors
Renal function should be evaluated prior to initiation of direct thrombin or factor Xa inhibitorsand should be re-evaluated when clinically indicated and at least annually IB
For patients with nonvalvular AF unable to maintain a therapeutic INR level with warfarin, use of a direct thrombin or factor Xa inhibitor (dabigatran, rivaroxaban, or apixaban) is recommended. IC
For patientwith a CHA2DS2-VASc score of 2 and who have endstage CKD (creatinine clearance [CrCl] <15 mL/min) or are on hemodialysis, it is reasonable to prescribe warfarin (INR 2.0 to 3.0) for oral anticoagulation IIaBThe direct thrombin inhibitor, dabigatran, and
the factor Xa inhibitor, rivaroxaban, are not recommended in patients with AF and end-stage CKD or on hemodialysis because of the lack of evidence from clinical trials regarding the balance of risks and benefits IIIC



Practical scenerios

Bleeding management

Warfarin Warfarin
◦ Give vitamin K 5-10 mg◦ Fresh frozen plasma◦ Octaplex
Prothrombin complex concentrate Works within 1 hour More effective than plasma at reversing INR Small volume 40 ml usually enough for most patients $$$$$

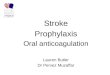
Reversal of new anticoagulants No specific monitoring test available
No reversal agents for new anticoagulants

Measuring the anticoagulant effect of NOACs Dabigatran Apixaban Rivaroxaban
Plasma peak 2h after ingestion 1-4h post ingestion 2-4h after ingestion
Plasma trough 12-24h after ingestion 12-24h after ingestion 16-24h after ingestion
PT cannot be used cannot be used prolonged: may indicate excess bleeding risk but local calibration required
INR cannot be used cannot be used cannot be used
aPTT at trough >2x ULN suggests excess bleeding risk
cannot be used cannot be used
dTT At trough >200ng/ml ≥ 65s: excess bleeding risk
cannot be used cannot be used
Anti-FXa assays n/a no data yet quantitative; no data on threshold values for bleeding or thrombosis
Ecarin clotting time at trough >2x ULN: excess bleeding risk
not affected; cannot be used
not affected; cannot be used12

Circulation, 2011

Reversal using PCC Randomized, double-blind, placebo controlled
study 12 healthy male volunteers received rivaroxaban
20mg BID or dabigatran 150 mg BID for 2.5 days Followed by bolus of 50IU/kg PCC (Cofact) or
saline Procedure then repeated with the other
anticoagulant treatment

Reversal using PCC Rivaroxaban:
◦ Prolonged the PT◦ Immediately reversed by PCC completely◦ Endogenous thrombin potential inhibited◦ Also completely normalized with PC
Dabigatran:◦ Affected PTT, ecarin clotting time, and thrombin time◦ Not reversed by PCC



Antidote to Dabigatran NEJM 6th august 2015 (REVERSE AD TRIAL) IV 5g dose Rapidly reversed anticoagulant effecs in
minutes Pending approval
Idarucizumab

Possible measures to take in case of bleeding
37
Van Ryn et al Am J Med 2012;125:417

Switching between anticoagulant regimens
VKA to NOAC INR <2.0: immediateINR 2.0–2.5: immediate or next day INR >2.5: use INR and VKA half-life to estimate time to INR <2.5
Parenteral anticoagulant to NOAC: Intravenous unfractioned heparin (UFH) Low molecular weight heparin (LMWH)
Start once UFH discontinued (t½=2h). May be longer in patients with renal impairmentStart when next dose would have been given
NOAC to VKA Administer concomitantly until INR in appropriate rangeMeasure INR just before next intake of NOACRe-test 24h after last dose of NOACMonitor INR in first month until stable values (2.0–3.0) achieved
NOAC to parenteral anticoagulant Initiate when next dose of NOAC is due
NOAC to NOAC Initiate when next dose is due except where higher plasma concentrationsexpected (e.g. renal impairment)
Aspirin or clodiprogel to NOAC Switch immediately, unless combination therapy needed22
www.escardio.org/EHRA

How to deal with dosing errors
Missed dose: BID: take missed dose up to 6 h after scheduled intake. If not possible skip dose and take next scheduled dose.QD: take missed dose up to 12 h after scheduled intake. If not possible skip dose and take next scheduled dose.
Double dose: BID: skip next planned dose and restart BID after 24 h.QD: continue normal regimen.
Uncertainty about intake: BID: continue normal regimen.QD: take another dose then continue normal regimen.
Overdose: Hospitalization advised.
25

When to stop NOACs before a planned surgical intervention
Dabigatran Apixaban Edoxaban * RivaroxabanNo important bleeding risk and/or local haemostasis possible: perform at trough
level (i.e. ≥12h or 24h after last intake)
Low risk High risk Low risk High risk Low risk High risk Low risk High
risk
CrCl ≥80 ml/min ≥24h ≥48h ≥24h ≥48hno
data yet
no data yet ≥24h ≥48h
CrCl 50–80 ml/min ≥36h ≥72h ≥24h ≥48h
no data yet
no data yet ≥24h ≥48h
CrCl 30–50 ml/min § ≥48h ≥96h ≥24h ≥48h
no data yet
no data yet ≥24h ≥48h
CrCl 15–30 ml/min §
not indicate
dnot
indicated ≥36h ≥48hno
data yet
no data yet ≥36h ≥48h
CrCl <15 ml/min no official indication for use
40
www.escardio.org/EHRA
Last intake of drug before elective surgical intervention
*no EMA approval yet.; Low risk: surgery with low risk of bleeding. High risk: surgery with high risk of bleeding § many of these patients may be on the lower dose of dabigatran (i.e. 2x110 mg/d) or apixaban (i.e. 2x2.5 mg/d), or have to be on the lower dose of rivaroxaban (15 mg/d).

When to restart NOACs after a planned surgical intervention
Procedures with immediate and complete haemostasis:
Atraumatic spinal/epidural anethesia Clean lumbar puncture
Resume 6–8 h after surgery
Procedures associated with immobilization:
Procedures with post-operative risk of bleeding:
Initiate reduced venous or intermediate dose of LMWH 6–8 h after surgery if haemostasis achieved.
Restart NOACs 48–72h after surgery upon complete haemostasis
Thromboprophylaxis (e.g. with LMWH) can be initiated 6-8 h after surgery
41
www.escardio.org/EHRA

Patients undergoing an urgent surgical
intervention Discontinue NOAC. Try to defer surgery at least 12 h and ideally 24 h after last dose. Urgent surgery associated with much higher rates of bleeding than
elective procedures, but lower than VKA-treated patients. 1
Coagulation tests can be considered (classical test or specific tests) but strategy based on these results has never been evaluated. Therefore such strategy cannot be recommended and should not be used routinely.
43
1. Healey et al, Circulation 2012:126;343-8

No data
Currently contraindicated
Pregnancy and lactation

Warfarin has been the benchmark since long
But, limitations with warfarin have paved way for NOAC’S
NOAC’S have their own limitations
One not superior over other
Decide case to case basis
Conclusion


thank you…