Embed Size (px)
Citation preview

Is Bone Loss Important?
2
1. Yes
2.No
www.wrightington.com
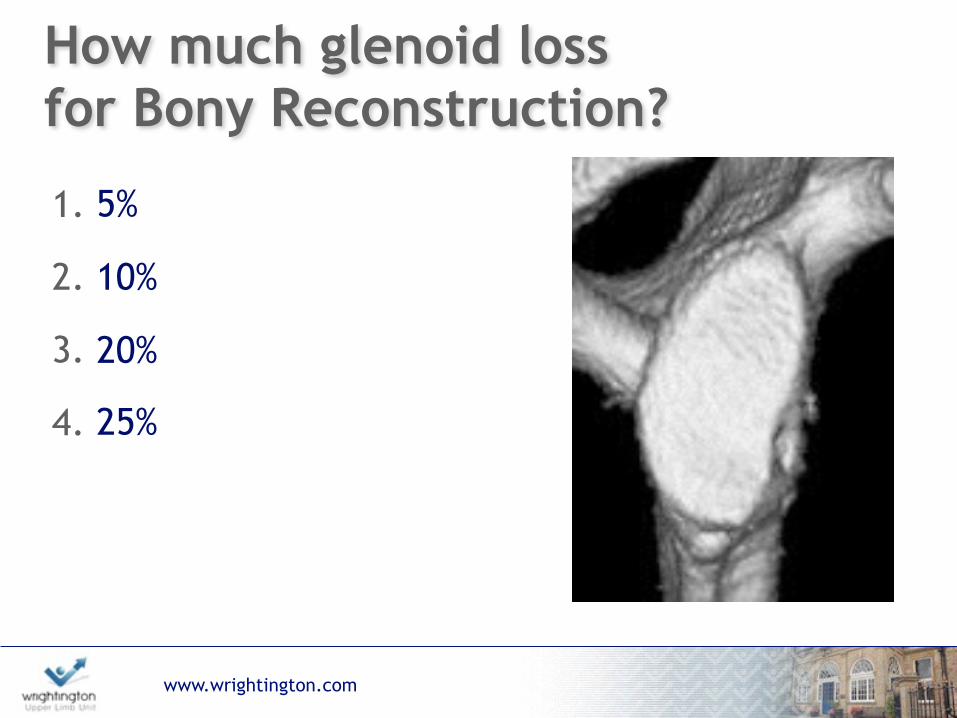
How much glenoid loss for Bony Reconstruction?
1. 5%
2. 10%
3. 20%
4. 25%

www.wrightington.com
What is a significant Hill-Sachs Lesion?
1. 12.5% humeral head surface
2. 20% humeral head surface
3. 40% humeral head surface
4. Engaging at Arthroscopy

www.wrightington.com
How do you assess Bone Loss?
1. X-Rays
2. MRI
3. CT
4. Arthroscopy
5
www.wrightington.com
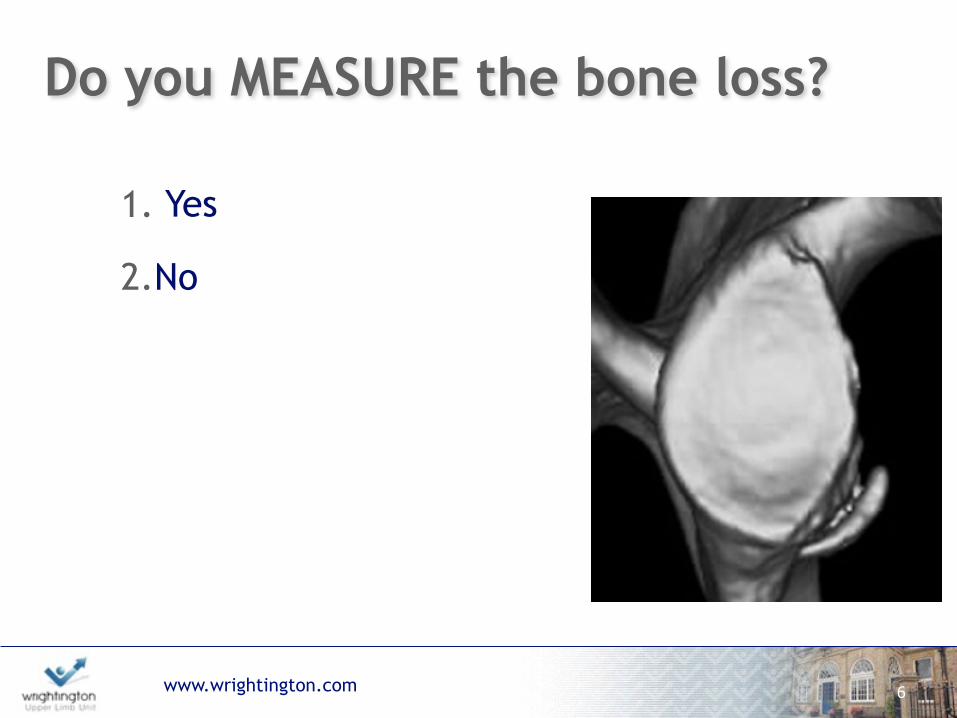
Do you MEASURE the bone loss?
1. Yes
2.No
6
www.wrightington.com
“The extent to which beliefsare based on evidence is very much less than believers suppose”
7
Bertrand Russell The Skeptical Essays, 1928
www.wrightington.com
The problem with ‘Evidence’
8
www.wrightington.com
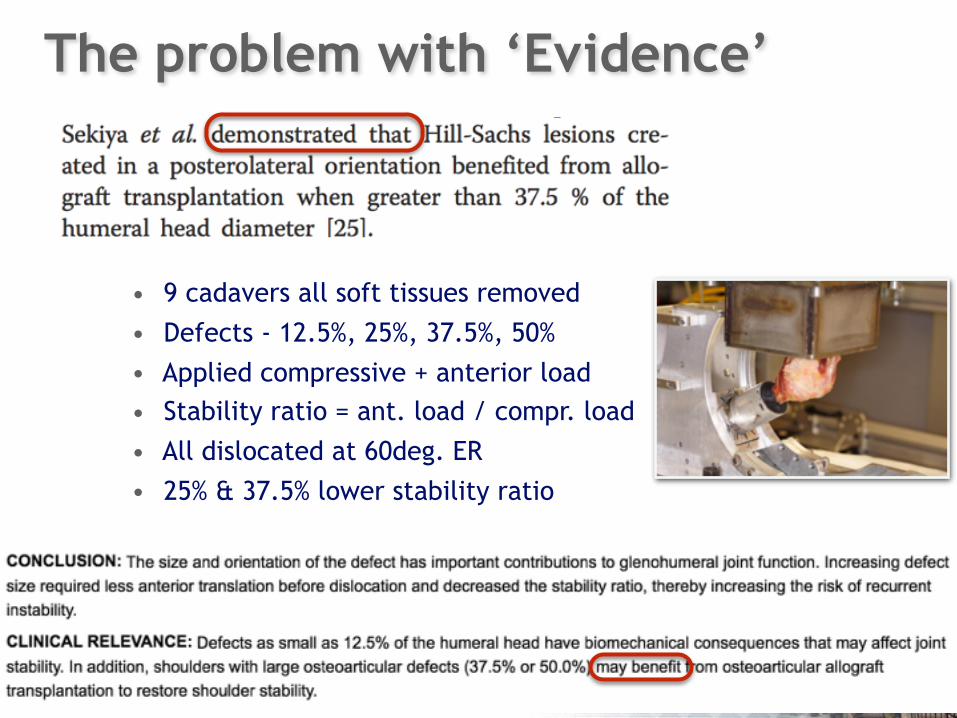
• 9 cadavers all soft tissues removed • Defects - 12.5%, 25%, 37.5%, 50% • Applied compressive + anterior load • Stability ratio = ant. load / compr. load
• All dislocated at 60deg. ER • 25% & 37.5% lower stability ratio
The problem with ‘Evidence’
www.wrightington.com
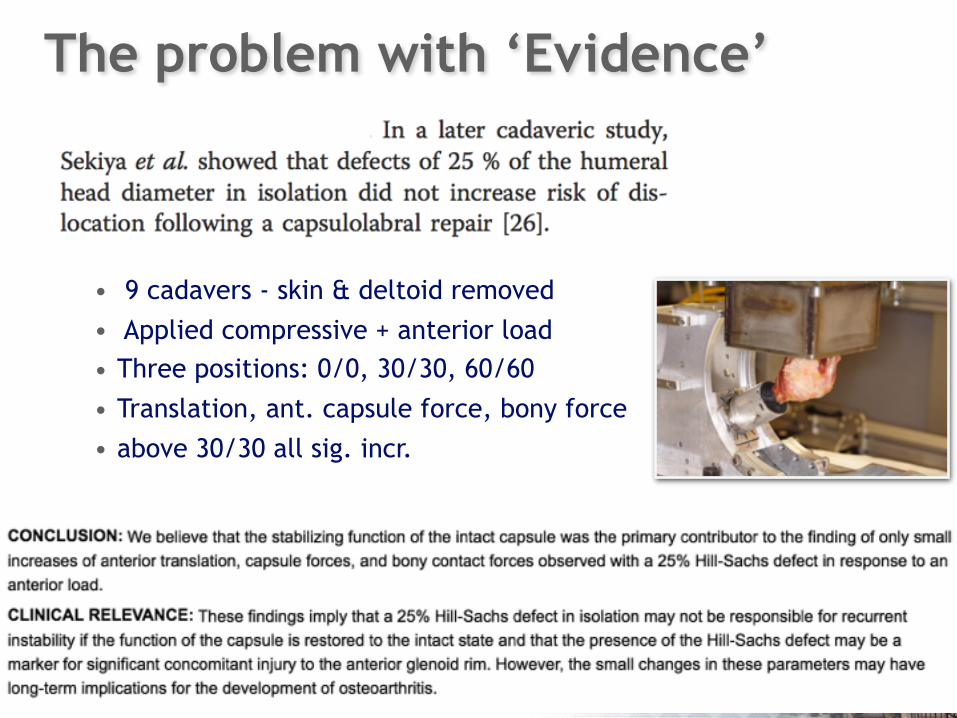
• 9 cadavers - skin & deltoid removed • Applied compressive + anterior load • Three positions: 0/0, 30/30, 60/60
• Translation, ant. capsule force, bony force • above 30/30 all sig. incr.
The problem with ‘Evidence’
www.wrightington.com
“The extent to which beliefsare based on evidence is very much less than believers suppose”
11
Bertrand Russell The Skeptical Essays, 1928
GLENOID BONE LOSS
12
www.wrightington.com
How much?
www.wrightington.com
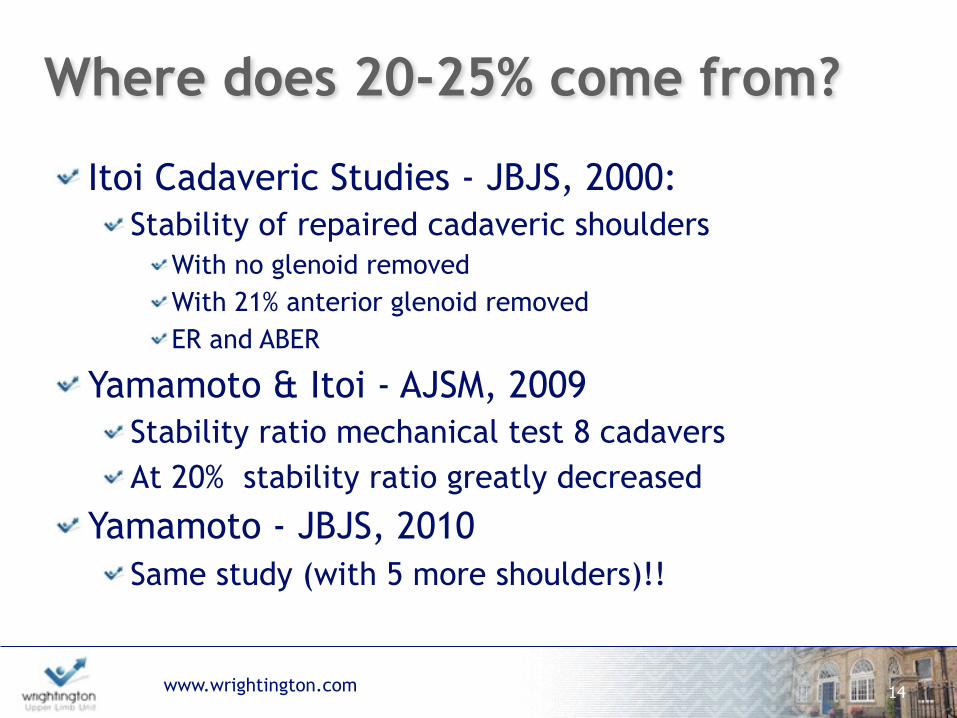
Where does 20-25% come from?
Itoi Cadaveric Studies - JBJS, 2000: Stability of repaired cadaveric shoulders
With no glenoid removed With 21% anterior glenoid removed ER and ABER
Yamamoto & Itoi - AJSM, 2009 Stability ratio mechanical test 8 cadavers At 20% stability ratio greatly decreased
Yamamoto - JBJS, 2010 Same study (with 5 more shoulders)!!
14
www.wrightington.com
Pear
15
Inverted Pear
www.wrightington.com 16
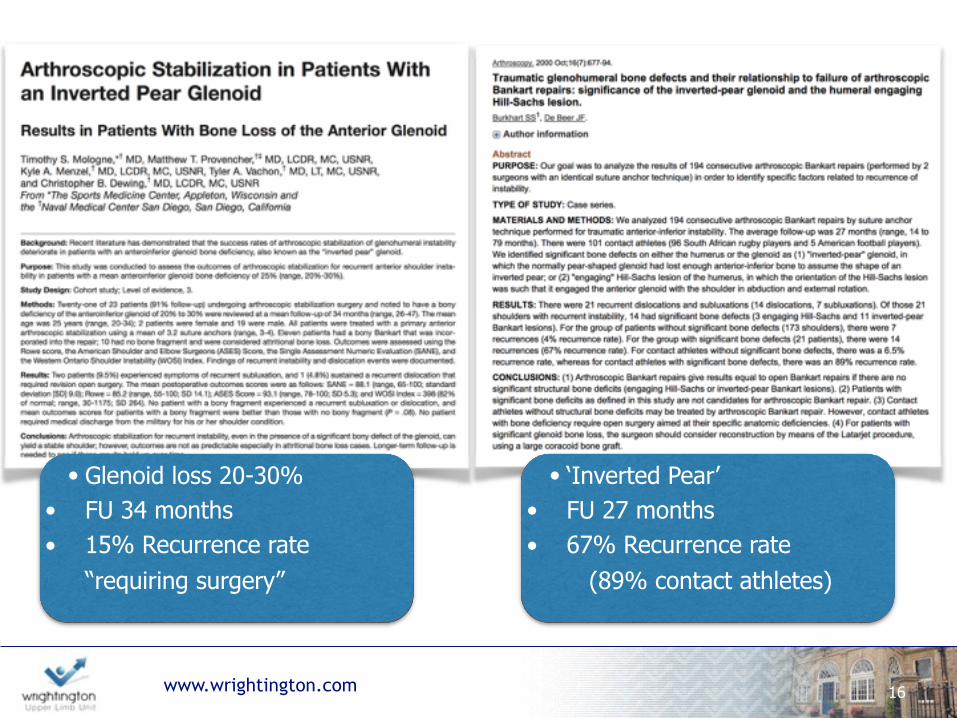
• Glenoid loss 20-30% • FU 34 months • 15% Recurrence rate
“requiring surgery”
• ‘Inverted Pear’ • FU 27 months • 67% Recurrence rate
(89% contact athletes)
www.wrightington.com
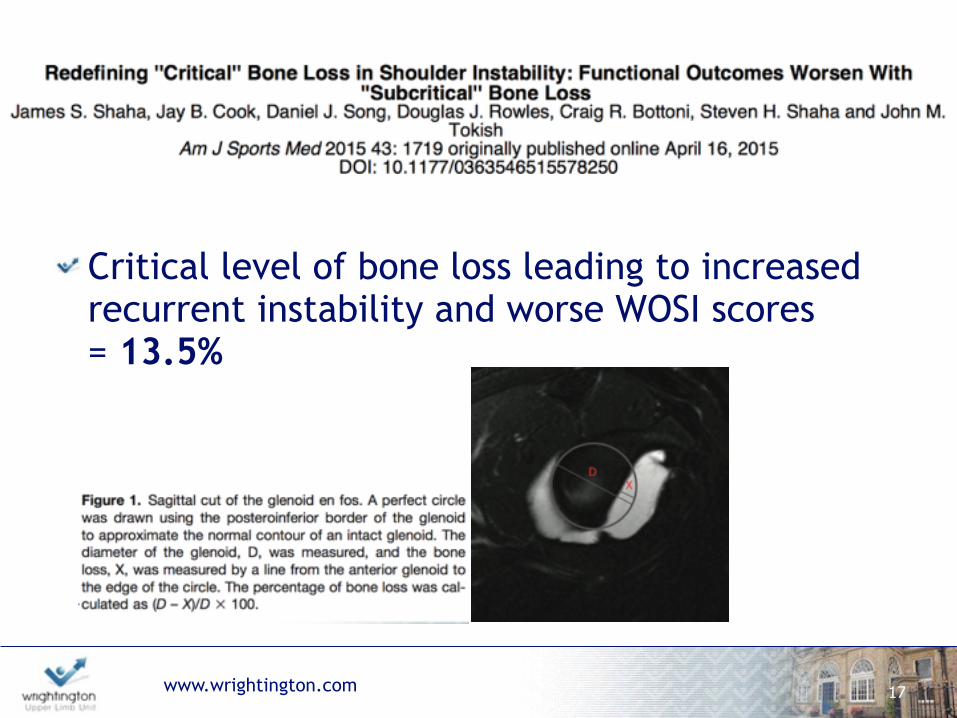
Critical level of bone loss leading to increased recurrent instability and worse WOSI scores = 13.5%
17
www.wrightington.com
How much?

www.wrightington.com
CT Scan reliable?Griffith Method: AJR 2008
‘En face’ CT compared to opp. normal glenoid in 218 anterior instability cases
High inter- and intra-observer reliability
19
BUT: Only one study validating side-side reliability in Normals… 10 patients! Same authors and Journal: AJR, 2003
www.wrightington.com
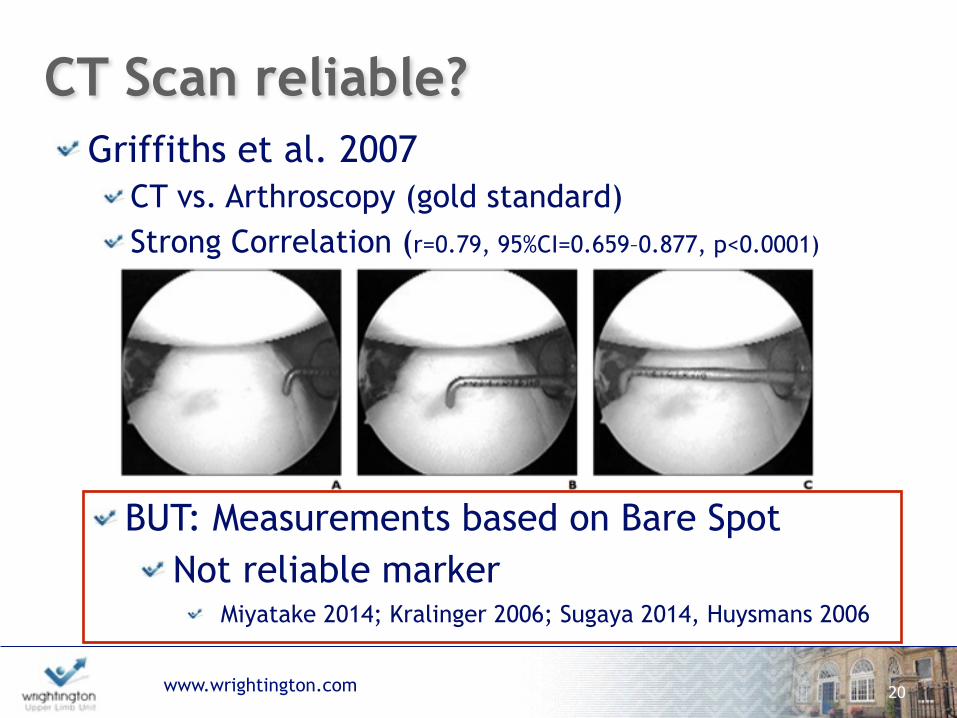
CT Scan reliable?Griffiths et al. 2007
CT vs. Arthroscopy (gold standard) Strong Correlation (r=0.79, 95%CI=0.659–0.877, p<0.0001)
20
BUT: Measurements based on Bare Spot Not reliable marker
Miyatake 2014; Kralinger 2006; Sugaya 2014, Huysmans 2006
www.wrightington.com
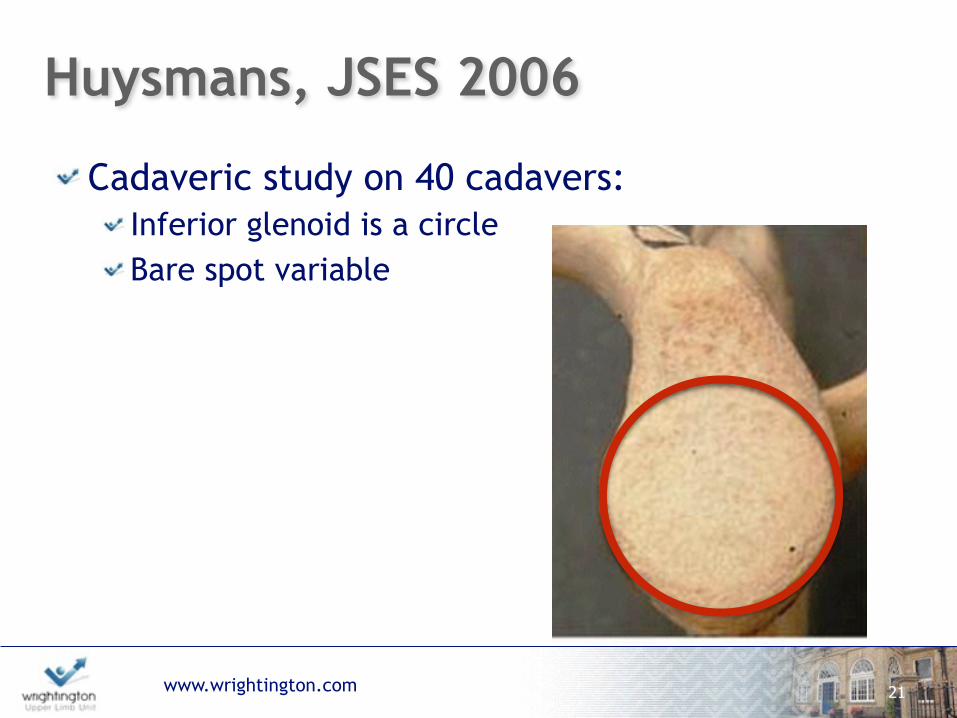
Huysmans, JSES 2006
Cadaveric study on 40 cadavers: Inferior glenoid is a circle Bare spot variable
21

www.wrightington.com
CT Reliable?‘Pico’ Method: Skeletal Radiol, 2009
40 shoulders compared opp. side ICC values 0.9-0.98
22
BUT: Two observers, only one intra-observer Reformatting done prior to observers.
www.wrightington.com
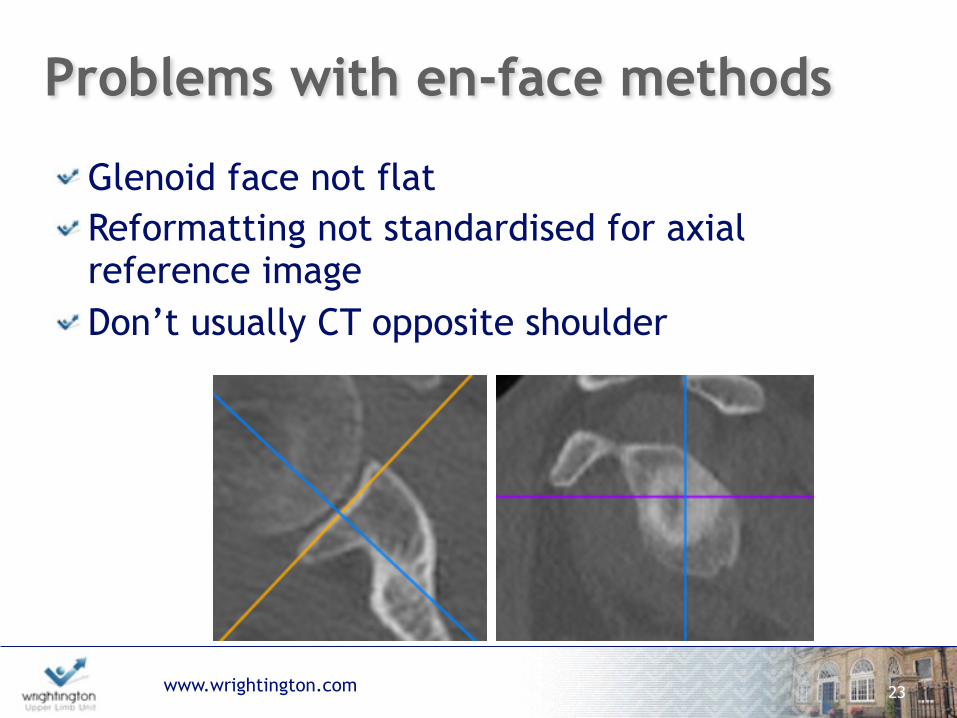
Problems with en-face methods
Glenoid face not flat Reformatting not standardised for axial reference image Don’t usually CT opposite shoulder
23

www.wrightington.com
What about MRI?MRI vs CT:
24
Lee et al. 2013 vs. 2D CT r=0.83 YES
Moroder 2013 vs. 3D CT 35% sensitive
100% specific NO
Gyftopoulous 2012 vs. 2DCT & 3DCT
percent error :3DCT 2.17-3.5 %, 2DCT 2.22-17.1 %, MRI 2.06- 5.94 %
YES
All different methodology & statistical analysis

www.wrightington.com
Glenoid Summary
No clear evidence on critical degree of bone loss
Discrepancy in outcomes
Arthroscopy not reliable gold standard
En-face measurements ? reproducible
If you do measure - ? need to CT opposite
‘normal’ side
25

HUMERAL HEAD BONE LOSS
26
www.wrightington.com
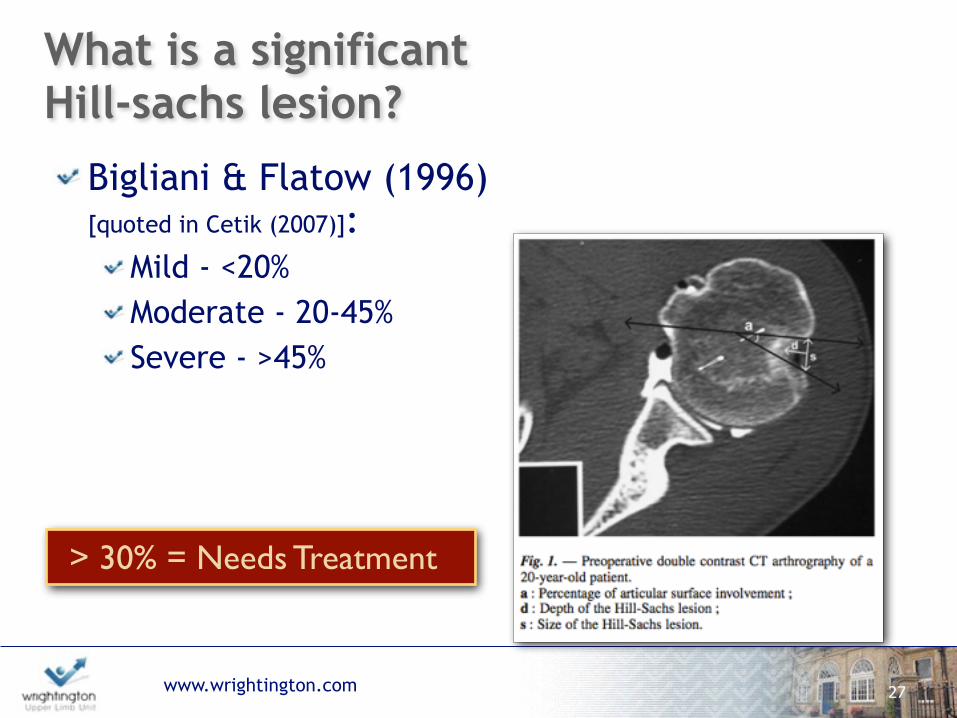
What is a significant Hill-sachs lesion?
Bigliani & Flatow (1996) [quoted in Cetik (2007)]:
Mild - <20% Moderate - 20-45% Severe - >45%
27
> 30% = Needs Treatment
www.wrightington.com
Biomechanical Studies
5/8 radius in ABER; 7/8 radius neural ER (Kaar, 2010)
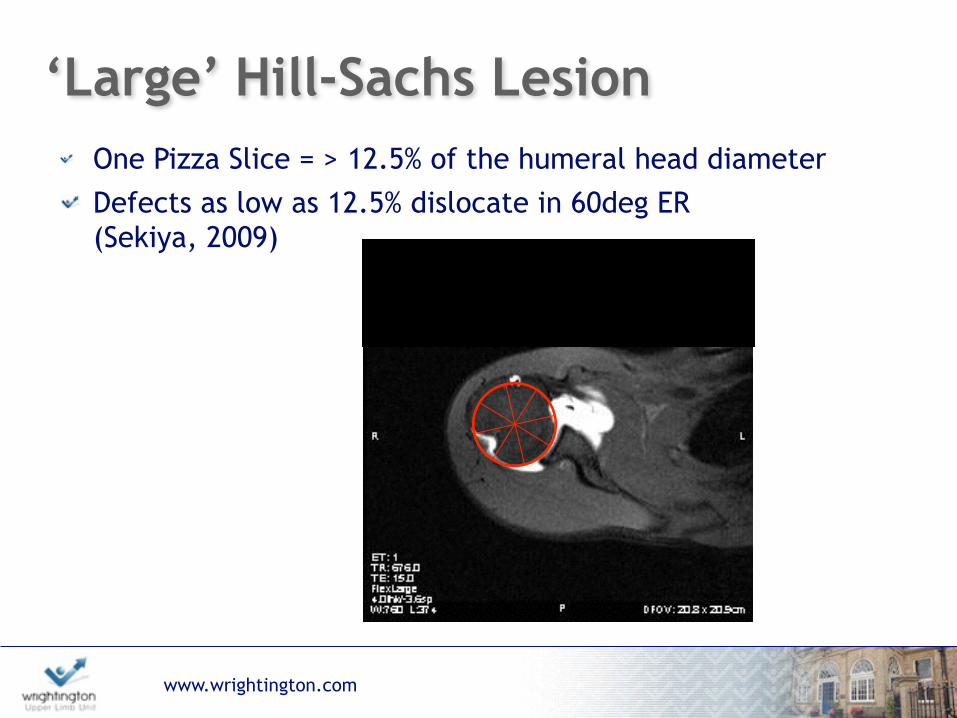
Defects as low as 12.5% dislocate in 60deg ER(Sekiya, 2009)
28
www.wrightington.com
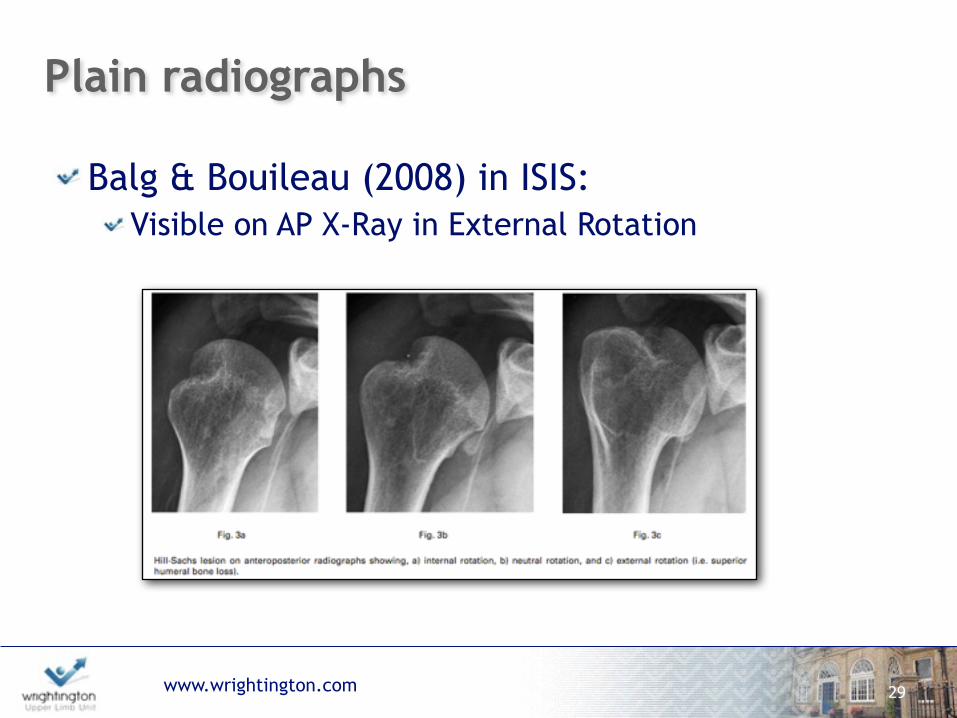
Plain radiographs
Balg & Bouileau (2008) in ISIS: Visible on AP X-Ray in External Rotation
29
www.wrightington.com
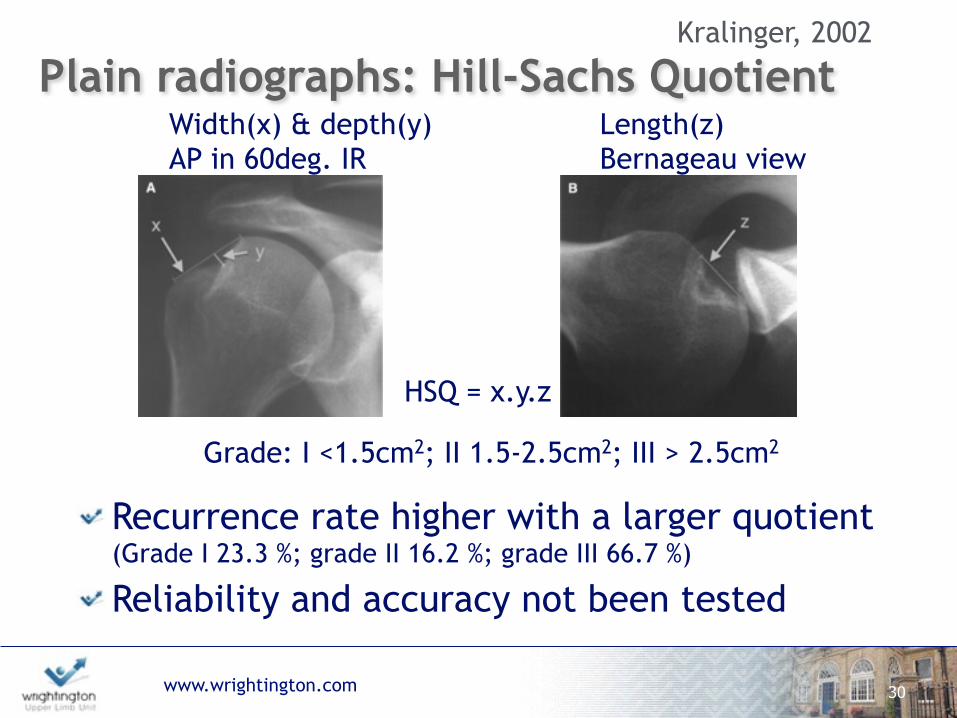
Width(x) & depth(y) AP in 60deg. IR
30
Plain radiographs: Hill-Sachs Quotient
Recurrence rate higher with a larger quotient (Grade I 23.3 %; grade II 16.2 %; grade III 66.7 %) Reliability and accuracy not been tested
Length(z) Bernageau view
HSQ = x.y.z
Grade: I <1.5cm2; II 1.5-2.5cm2; III > 2.5cm2
Kralinger, 2002

www.wrightington.com 31
Plain radiographs: Radius Technique
Recurrence rate higher with a larger ratio (Sommaire):
d/R >20% = 40% recurrence d/R < 20% = 10% recurrence
Arth Stab failure rate (Hardy): d/R >15% = 60% failure d/R <15% = 15% failure
Hill-Sachs depth(d)/Humeral head radius(R)- AP in IR
Charrouset, 2010

www.wrightington.com
CT
Hardy, 2012: Larger Width, depth & length = lower Duplay score, but not tested for reliability
Saito, 2009 & Cho, 2011: Good intra- & inter-reliability for depth & width on 2DCT
Kodali, 2011: Moderate reliability on 2DCT With percentage error of 13.6+/-8.4%
32
www.wrightington.com
MRI & Arthroscopy
No reliability studies for MRI!
Kirkley, 2003: MRI = Arthroscopy in detecting Hill-Sachs lesions (16 patients; no blinding)
33

www.wrightington.com
Funky Pizza Method
34
www.wrightington.com
‘Large’ Hill-Sachs LesionOne Pizza Slice = > 12.5% of the humeral head diameter Defects as low as 12.5% dislocate in 60deg ER(Sekiya, 2009)
Combined Glenoid + Humeral Head
Methods
36
www.wrightington.com
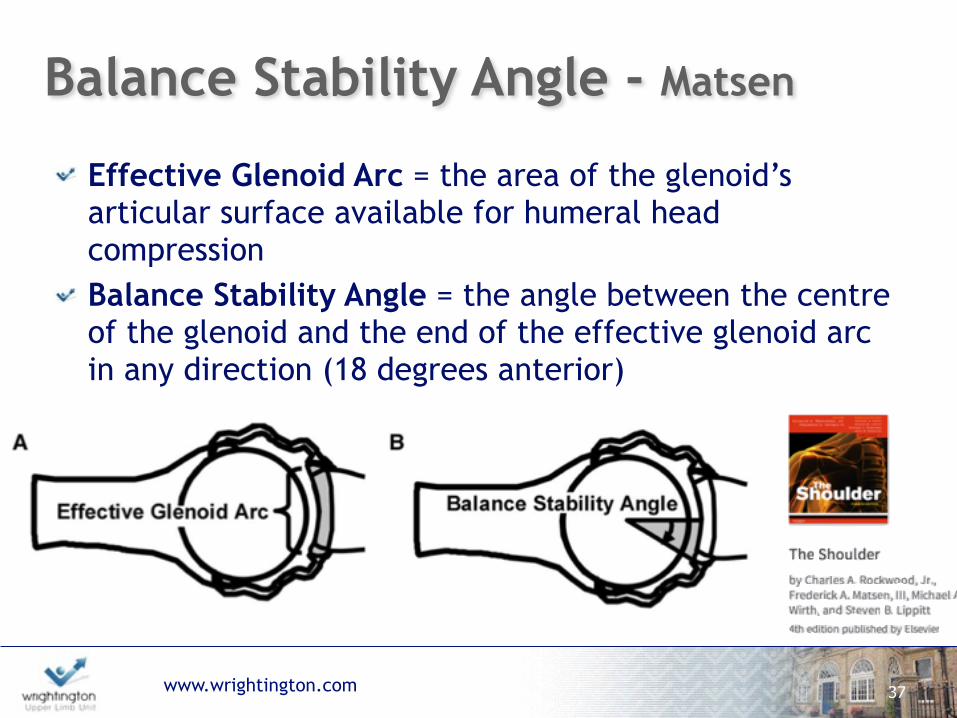
Balance Stability Angle - Matsen
Effective Glenoid Arc = the area of the glenoid’s articular surface available for humeral head compression Balance Stability Angle = the angle between the centre of the glenoid and the end of the effective glenoid arc in any direction (18 degrees anterior)
37
www.wrightington.com
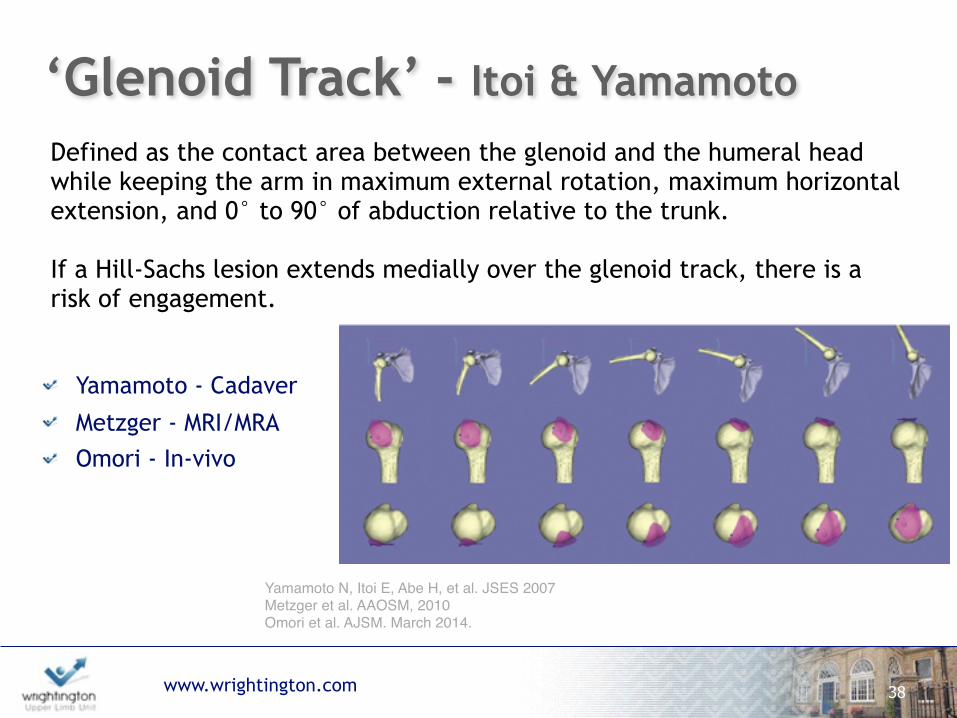
‘Glenoid Track’ - Itoi & Yamamoto
Yamamoto - Cadaver
Metzger - MRI/MRA Omori - In-vivo
38
Yamamoto N, Itoi E, Abe H, et al. JSES 2007 Metzger et al. AAOSM, 2010 Omori et al. AJSM. March 2014.
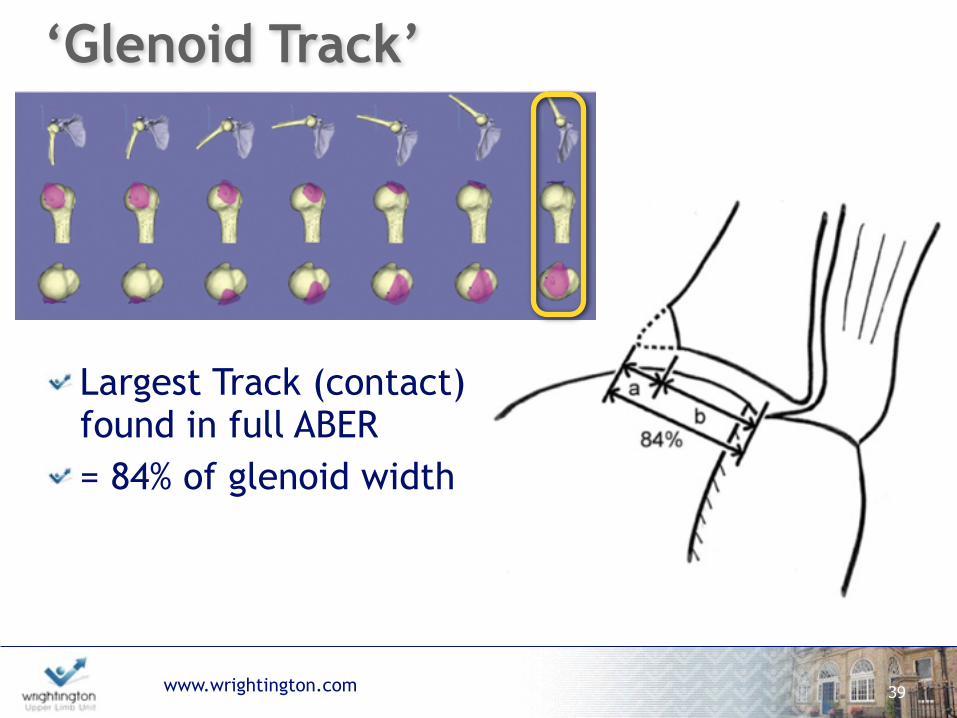
Defined as the contact area between the glenoid and the humeral head while keeping the arm in maximum external rotation, maximum horizontal extension, and 0° to 90° of abduction relative to the trunk.
If a Hill-Sachs lesion extends medially over the glenoid track, there is a risk of engagement.
www.wrightington.com
Largest Track (contact) found in full ABER = 84% of glenoid width
39
‘Glenoid Track’
www.wrightington.com 40
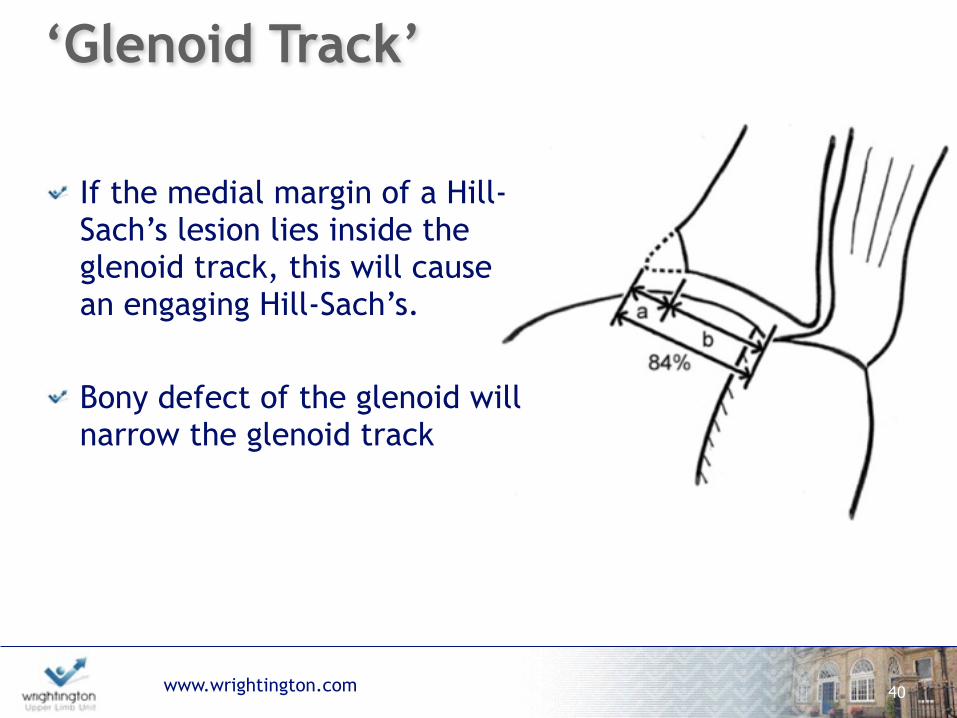
‘Glenoid Track’
If the medial margin of a Hill-Sach’s lesion lies inside the glenoid track, this will cause an engaging Hill-Sach’s.
Bony defect of the glenoid will narrow the glenoid track

www.wrightington.com
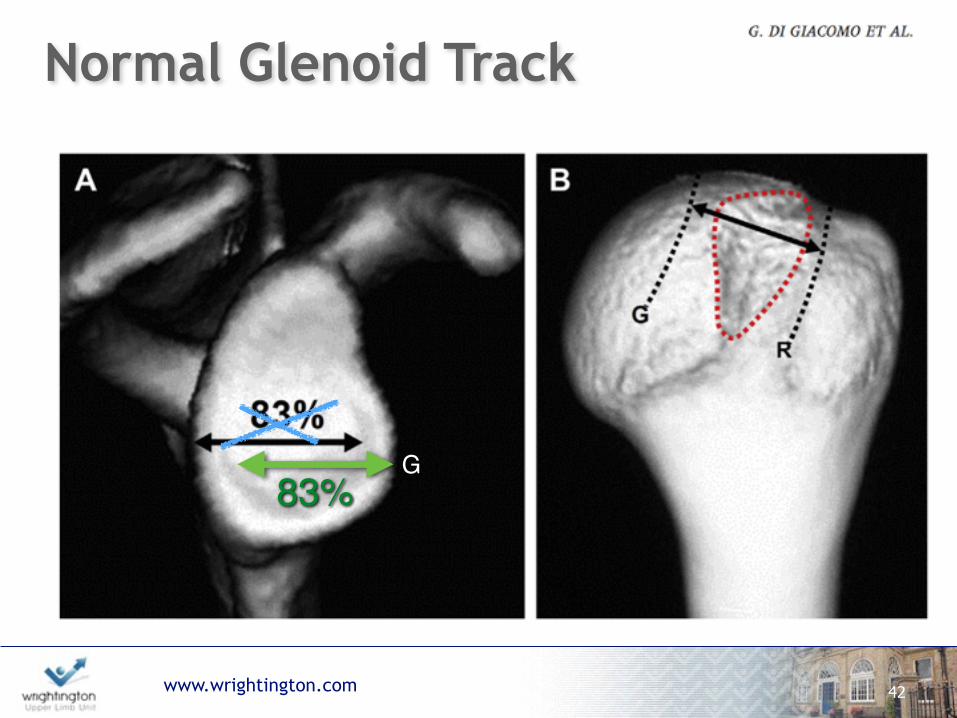
1. Measure the diameter (D) of the inferior glenoid, either by arthroscopy or from 3D CT scan.
2. Determine the width of the anterior glenoid bone loss (d). 3. Calculate the width of the glenoid track (GT) by the following
formula: GT=0.83D-d 4. Calculate the width of the HSI, which is the width of the Hill-
Sachs lesion (HS) plus the width of the bone bridge (BB) between the rotator cuff attachments and the lateral aspect of the Hill-Sachs lesion: HSI = HS + BB.
5. If HSI > GT, the HS is off track, or engaging. If HSI < GT, the HS is on track, or non-engaging.
41
www.wrightington.com
Normal Glenoid Track
42
83%G
www.wrightington.com
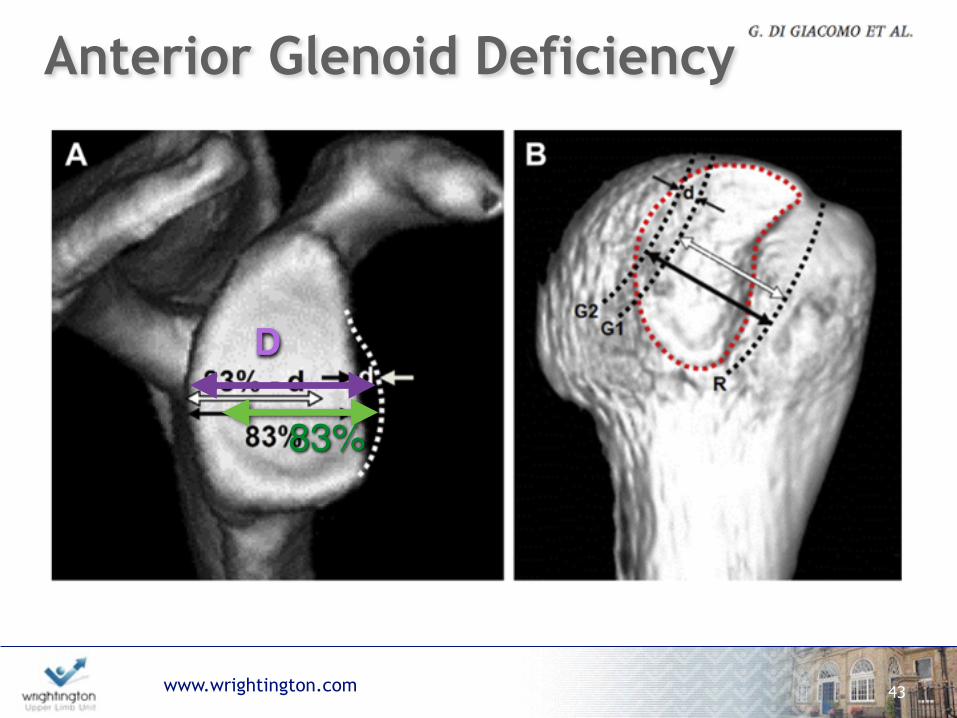
Anterior Glenoid Deficiency
43
D
83%
www.wrightington.com
The Formula:
44
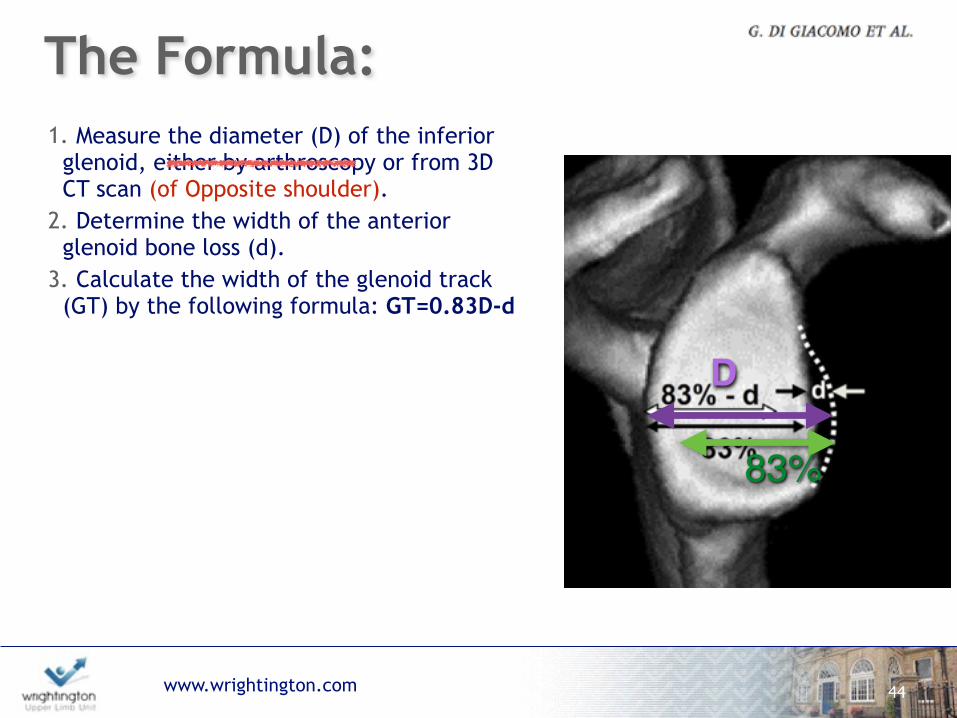
1. Measure the diameter (D) of the inferior glenoid, either by arthroscopy or from 3D CT scan (of Opposite shoulder).
2. Determine the width of the anterior glenoid bone loss (d).
3. Calculate the width of the glenoid track (GT) by the following formula: GT=0.83D-d
4. Calculate the width of the HSI, which is the width of the Hill-Sachs lesion (HS) plus the width of the bone bridge (BB) between the rotator cuff attachments and the lateral aspect of the Hill-Sachs lesion: HSI = HS + BB.
5. If HSI > GT, the HS is off track, or engaging. If HSI < GT, the HS is on track, or non-engaging.
D
83%
www.wrightington.com
The Formula:
45
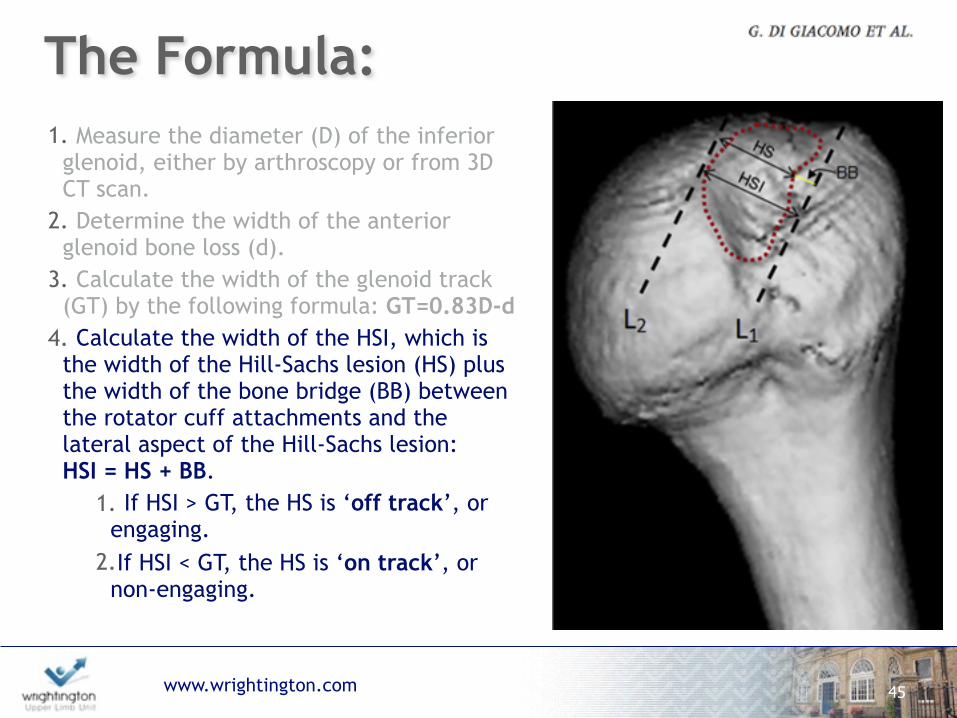
1. Measure the diameter (D) of the inferior glenoid, either by arthroscopy or from 3D CT scan.
2. Determine the width of the anterior glenoid bone loss (d).
3. Calculate the width of the glenoid track (GT) by the following formula: GT=0.83D-d
4. Calculate the width of the HSI, which is the width of the Hill-Sachs lesion (HS) plus the width of the bone bridge (BB) between the rotator cuff attachments and the lateral aspect of the Hill-Sachs lesion: HSI = HS + BB.
1. If HSI > GT, the HS is ‘off track’, or engaging.
2.If HSI < GT, the HS is ‘on track’, or non-engaging.
www.wrightington.com
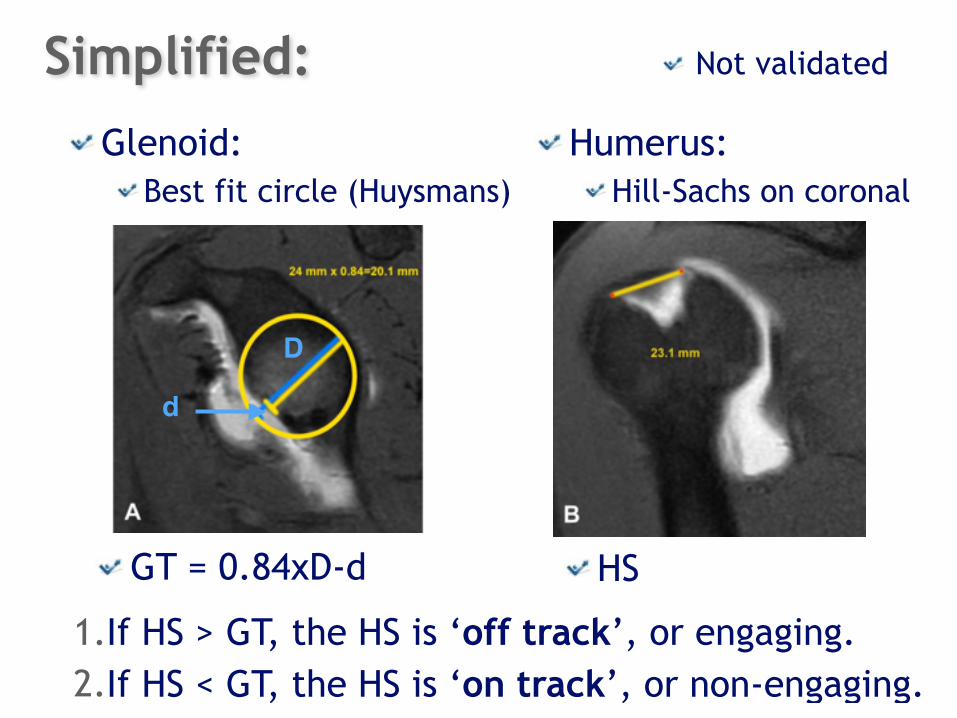
Glenoid: Best fit circle (Huysmans)
46
Humerus: Hill-Sachs on coronal
GT = 0.84xD-d HS
D
d
1.If HS > GT, the HS is ‘off track’, or engaging. 2.If HS < GT, the HS is ‘on track’, or non-engaging.
Simplified: Not validated
www.wrightington.com
Two year period of 57 Bankart repairs On-track (49) - recurrence 4% Off-track (8) - recurrence 75%
PPV for Glenoid Track = 75% PPV for Glenoid loss >20% = 43%
47
www.wrightington.com
Summary:Radiography:
Insufficient accuracy Not sufficient for pre-op planning Useful for screening
CT: Most reliable, but need opposite shoulder Radiation exposure
MRI & Arthroscopy: No sufficient validation
ALSO: No consensus measuring technique No clarity on what a clinically significant lesion is!
48
www.wrightington.com
Thank You
49