Embed Size (px)
DESCRIPTION
Citation preview

Benign & Malignant Benign & Malignant Diseases Of The Diseases Of The
ProstateProstate
By:By: Dr. Saud Al-Subaie Dr. Saud Al-Subaie
Moderator:Moderator: Dr.E.O.Kehinde Dr.E.O.Kehinde

OutlineOutline
IntroductionIntroduction
BPHBPH
Prostate cancerProstate cancer
Prostatitis Prostatitis 1.1. Acute bacterial prostatitisAcute bacterial prostatitis
2.2. Chronic bacterial prostatitisChronic bacterial prostatitis
3.3. Chronic pelvic pain (CPP) syndrome (Chronic pelvic pain (CPP) syndrome ( inflammatory/non-inflammatory)inflammatory/non-inflammatory)

IntroductionIntroduction BPH & prostate adenocarcinoma are the 2 major BPH & prostate adenocarcinoma are the 2 major neoplasms affecting the human prostate.neoplasms affecting the human prostate.
The prostate is a complex organ consisting of epithelial, The prostate is a complex organ consisting of epithelial, stromal, & muscular element.stromal, & muscular element.
Anatomically the prostate gland is the shape of a Anatomically the prostate gland is the shape of a compressed inverted cone, residing in the true pelvis.compressed inverted cone, residing in the true pelvis.
Arterial blood supply: inferior vesical+ middle rectal a.Arterial blood supply: inferior vesical+ middle rectal a.
Venous drainage: Dorsal venous plexes Venous drainage: Dorsal venous plexes


The normal prostate measures between 3-4cm at its The normal prostate measures between 3-4cm at its widest portion; it is 4-6cm in length & 2-3cm in thickness.widest portion; it is 4-6cm in length & 2-3cm in thickness.
Weight 17-25 gmWeight 17-25 gm
In the early 1970’s McNeal proposed a concept of zonal In the early 1970’s McNeal proposed a concept of zonal anatomy.anatomy.
According to this concept, the glandular portion of the According to this concept, the glandular portion of the prostate is composed of a large peripheral & a small prostate is composed of a large peripheral & a small central zone, which together constitute about 95% of the central zone, which together constitute about 95% of the gland. gland.

The other 5% is formed by the transition zone which is The other 5% is formed by the transition zone which is located just outside the urethra & is composed of the located just outside the urethra & is composed of the periurethral glands, which presumably are responsible periurethral glands, which presumably are responsible for all of the BPH.for all of the BPH.
60-70% of prostatic CA occurs in the peripheral zone, 60-70% of prostatic CA occurs in the peripheral zone, 10-20% in the transition zone, & 5-10% in the central 10-20% in the transition zone, & 5-10% in the central zone.zone.

Benign Prostatic Benign Prostatic hypertrohy (hypertrohy (BPHBPH))

Incidence & EpidemiologyIncidence & Epidemiology
The term BPH is a misnomer because the actual The term BPH is a misnomer because the actual change is a hyperplasia & not hypertrophy.change is a hyperplasia & not hypertrophy.
The initiation of BPH may not be environmental The initiation of BPH may not be environmental or genetically influenced.or genetically influenced.
It is also suggested that the prevalence of BPH It is also suggested that the prevalence of BPH increases with age in all male populations.increases with age in all male populations.

EtiologyEtiology
The etiology of BPH is unclear.The etiology of BPH is unclear.
Two factors necessary for BPH to occur are:Two factors necessary for BPH to occur are:
(1) endocrine control (DHT)(1) endocrine control (DHT)
(2) aging(2) aging
The relative roles of androgen & estrogen in inducing The relative roles of androgen & estrogen in inducing BPH, however , are complex & not completely BPH, however , are complex & not completely understood.understood.


PathogenesisPathogenesis
Stromal – epithelial interaction Stromal – epithelial interaction normal 2:1, BPH 3 or 4:1normal 2:1, BPH 3 or 4:1
major change is connective tissuemajor change is connective tissue
The differential representation of the histologic The differential representation of the histologic components of BPH explains the potential components of BPH explains the potential responseviness to medical therapyresponseviness to medical therapy

Pathophysiology Of SymptomsPathophysiology Of Symptoms
Symptoms of BPH:Symptoms of BPH:1) obstructive 1) obstructive
decrease in force & caliber of the stream:decrease in force & caliber of the stream: due to urethral due to urethral compression is one of the early & constant features of BPH.compression is one of the early & constant features of BPH.
Hesitancy: Hesitancy: occurs because the detrusor takes a longer time to occurs because the detrusor takes a longer time to generate the initial increased pressure to overcome the urethral generate the initial increased pressure to overcome the urethral resistance. resistance.
Intermittency: Intermittency: occurs because the detrusor is unable to sustain occurs because the detrusor is unable to sustain the increased pressure until the end of voiding.the increased pressure until the end of voiding.
Terminal dribbling of urine & incomplete sense of bladder Terminal dribbling of urine & incomplete sense of bladder emptyingemptying

Pathophysiology Of SymptomsPathophysiology Of Symptoms
2) Irritative symptoms:2) Irritative symptoms:
Frequency:Frequency: - Incomplete emptying during each void results in shorter - Incomplete emptying during each void results in shorter
intervals between voids. intervals between voids. - The presence of enlarged prostate provokes the bladder to - The presence of enlarged prostate provokes the bladder to
trigger a voiding response more frequently than in normal trigger a voiding response more frequently than in normal individuals, especially if the prostate is growing intravesically.individuals, especially if the prostate is growing intravesically.
Nocturia:Nocturia: normal cortical inhibitors are lessened and also because normal cortical inhibitors are lessened and also because the normal urethral and sphincteric tone is reduced during sleep.the normal urethral and sphincteric tone is reduced during sleep.
urgency & dysuria:urgency & dysuria: uncommon. uncommon.

Pathophysiology Of SymptomsPathophysiology Of Symptoms
Obstructive symptoms are common with Obstructive symptoms are common with enlarged prostates. Predominance of enlarged prostates. Predominance of
irritative should suggest voiding irritative should suggest voiding dysfunction.dysfunction.

Pathophysiology Of SymptomsPathophysiology Of SymptomsSystemic symptoms related to the UT:Systemic symptoms related to the UT:
- Vesicoureteral reflux- Vesicoureteral reflux - Dilatation & hydronephrosis- Dilatation & hydronephrosis - Renal failure & symptoms of uremia- Renal failure & symptoms of uremia
Symptoms unrelated to the UT:Symptoms unrelated to the UT: - hernias, hemorrhoids and vesical calculus- hernias, hemorrhoids and vesical calculus - change in the caliber of bowl movements- change in the caliber of bowl movements
Symptoms related to complications:Symptoms related to complications: - cystitis- cystitis - pyelonephritis- pyelonephritis - bladder calculi - bladder calculi - micro or gross hematuria.- micro or gross hematuria.


Signs of BPHSigns of BPH
If the disease is advanced & has resulted in renal failure. If the disease is advanced & has resulted in renal failure. Signs of renal failure include elevated BP, rapid pulse & Signs of renal failure include elevated BP, rapid pulse & respiration, uremic fetor, pericarditis & pallor of nail beds.respiration, uremic fetor, pericarditis & pallor of nail beds.
Abdominal examination may reveal palpable kidney or Abdominal examination may reveal palpable kidney or flank tenderness if there is hydronephrosis or flank tenderness if there is hydronephrosis or pyelonephritis.pyelonephritis.
A distended bladder may be noted on palpation or A distended bladder may be noted on palpation or percussion.percussion.

Signs of BPHSigns of BPH
Rectal examination may reveal an enlarged prostate.Rectal examination may reveal an enlarged prostate.
The distinction between right & left lobes of the prostateThe distinction between right & left lobes of the prostate
is usually lost in BPH.is usually lost in BPH.
Median sulcus always present.Median sulcus always present.

Laboratory FindingsLaboratory FindingsUrinalysis & microscopic examination:Urinalysis & microscopic examination: to R/O infection to R/O infection or the presence of hematuria.or the presence of hematuria.
serum U/E & creatinine:serum U/E & creatinine: to provide baseline information to provide baseline information on renal function & metabolic status.on renal function & metabolic status.
Uroflowmetry: Uroflowmetry: At a volume of 125-150ml, normal At a volume of 125-150ml, normal individuals have average flow rates of 12ml/sec & peak individuals have average flow rates of 12ml/sec & peak flow close to 20ml/sec.flow close to 20ml/sec.
Mild 11-15 ml/secMild 11-15 ml/sec Moderate Moderate 7 and 7 and 10 ml/sec 10 ml/sec Severe Severe 7ml/sec 7ml/sec
Residual Urine: Residual Urine: estimated by U/S or catheterizations. estimated by U/S or catheterizations. Volumes >150 ml are considered significant since they Volumes >150 ml are considered significant since they constitute approximately one-third of normal bladder constitute approximately one-third of normal bladder volume.volume.

ImagingImaging
Ultrasonography:Ultrasonography:
In BPH, it is most useful for measuring bladder & In BPH, it is most useful for measuring bladder & prostate volume as well as residual urine.prostate volume as well as residual urine.
Estimation of prostatic size is important because most Estimation of prostatic size is important because most urologists prefer to perform TURP for glands under urologists prefer to perform TURP for glands under 100g.100g.
TRUS must be used as it is more accurate. TRUS must be used as it is more accurate.
IVP:IVP:
For UTI & complications of BPHFor UTI & complications of BPH

TreatmentTreatment
Because BPH is not invariably progressive, the timing of Because BPH is not invariably progressive, the timing of intervention for each patient is variable.intervention for each patient is variable.
Absolute indications for treatment include severe Absolute indications for treatment include severe obstructive symptoms & renal insufficiency.obstructive symptoms & renal insufficiency.
Relative indications include moderate symptoms of Relative indications include moderate symptoms of prostatism, recurrent UTI and hematuria.prostatism, recurrent UTI and hematuria.
Until recently, surgery was the mainstay of therapy for Until recently, surgery was the mainstay of therapy for BPH. In the last decade or so , there has been a BPH. In the last decade or so , there has been a tremendous resurgence of interest in non surgical tremendous resurgence of interest in non surgical therapies.therapies.

Medical TreatmentMedical Treatment
Obstruction secondary to BPH occurs because Obstruction secondary to BPH occurs because of 2 factors:of 2 factors:
a. Dynamic component:a. Dynamic component: a result of a result of contraction of smooth muscles of the prostate contraction of smooth muscles of the prostate & prostatic urethra mediated mostly by & prostatic urethra mediated mostly by adrenergic receptors.adrenergic receptors.
b. Mechanical component:b. Mechanical component: related to the related to the presence of a mass which compresses & presence of a mass which compresses & narrows the urethral lumen.narrows the urethral lumen.

Alpha-1 adrenergic antagonistsAlpha-1 adrenergic antagonistsIdeally suited for the treatment of the dynamic component of Ideally suited for the treatment of the dynamic component of BOO because they can selectively reduce resistance along the BOO because they can selectively reduce resistance along the bladder outlet without impairing detrusor contractility.bladder outlet without impairing detrusor contractility.Example:Example:
- Tamsulosin- Tamsulosin 0.4mg0.4mg ODOD- Alfuzosin XL- Alfuzosin XL 10mg10mg ODOD- Doxazosin- Doxazosin 4mg 4mg TIDTID
Indication: Prostate size < 40 gmIndication: Prostate size < 40 gm
S/E are related to their antihypertensive effects and include S/E are related to their antihypertensive effects and include dizziness and lightheadedness, Tachycardia, palpitation, dizziness and lightheadedness, Tachycardia, palpitation, tiredness, weakness & nasal congestion.tiredness, weakness & nasal congestion.
Retrograde ejaculation may occur due to relaxation of the Retrograde ejaculation may occur due to relaxation of the bladder neck.bladder neck.
Alpha blockers also have beneficial S/E including lowering of Alpha blockers also have beneficial S/E including lowering of serum cholesterol & triglycerides.serum cholesterol & triglycerides.

55 alpha- reductase inhibitoralpha- reductase inhibitor
Agents that selectively blockade androgens at the Agents that selectively blockade androgens at the prostate cellular level are termed anti-androgens.prostate cellular level are termed anti-androgens.
the prostate normally requires conversion of the prostate normally requires conversion of testosterone to dihydrotestosterone by the enzyme 5 testosterone to dihydrotestosterone by the enzyme 5 alpha-reductase.alpha-reductase.
Proscar is an anti-androgen that blocks this enzyme. Proscar is an anti-androgen that blocks this enzyme.
In long term clinical trials, proscar has been shown to In long term clinical trials, proscar has been shown to decrease prostatic size & improve urine flow rates & decrease prostatic size & improve urine flow rates & symptoms of BPH.symptoms of BPH.

55 alpha- reductase inhibitoralpha- reductase inhibitor
Another approach to blocking androgen uptake by Another approach to blocking androgen uptake by prostatic cells is to prevent androgen binding to nuclear prostatic cells is to prevent androgen binding to nuclear androgen receptors ( e.g. Flutamide). androgen receptors ( e.g. Flutamide).
There are also anti-androgens that block both LH and There are also anti-androgens that block both LH and nuclear androgen uptake.nuclear androgen uptake.
In BPH patients, this has been demonstrated to improve In BPH patients, this has been demonstrated to improve flow rates & voiding symptoms.flow rates & voiding symptoms.
Indication: Prostate size > 40 gmIndication: Prostate size > 40 gm
S/E include impotence, decreased libido & lowers serum S/E include impotence, decreased libido & lowers serum PSA by approximately 50% within 6 months of use.PSA by approximately 50% within 6 months of use.

Conventional Surgical TherapyConventional Surgical Therapy
1) TURP1) TURPThe principles of TURP are to remove the obstructing The principles of TURP are to remove the obstructing adenomatous portion of the prostate via the urethra.adenomatous portion of the prostate via the urethra.
Overall morbidity: 18%.Overall morbidity: 18%.Current mortality: 0.2%.Current mortality: 0.2%.
One preventable complication is One preventable complication is TUR syndromeTUR syndrome
Immediate complications:Immediate complications: failure to void, post op. failure to void, post op. haemorrhage, clot retention, & UTI.haemorrhage, clot retention, & UTI.
Late complications:Late complications: impotence, incontinence, impotence, incontinence, uretheral stricture and retrograde ejaculation.uretheral stricture and retrograde ejaculation.

Conventional Surgical TherapyConventional Surgical TherapyTUR syndromeTUR syndrome
Because irrigating fluid under pressure is used during Because irrigating fluid under pressure is used during resection, there is a certain amount of absorption via the resection, there is a certain amount of absorption via the venous sinuses.venous sinuses.
It results in hypervolemia & hyponatremia which leads to It results in hypervolemia & hyponatremia which leads to cerebral oedema & seizures.cerebral oedema & seizures.
Other S/E include visual disturbance & Other S/E include visual disturbance & hyperammonemia or hemolysis.hyperammonemia or hemolysis.
The incidence is approximately 2%.The incidence is approximately 2%.
Preventive measures include suprapubic drainage during Preventive measures include suprapubic drainage during TURP, continuous flow resectoscopes & diuretics.TURP, continuous flow resectoscopes & diuretics.




Conventional Surgical TherapyConventional Surgical Therapy
2) TUIP2) TUIP
It is indicated in patients with obstructive symptoms & It is indicated in patients with obstructive symptoms & normal or small prostates in whom TURP is considered normal or small prostates in whom TURP is considered excessive surgery to obtain relief of symptoms.excessive surgery to obtain relief of symptoms.

Conventional Surgical TherapyConventional Surgical Therapy
3) Open prostatectomy3) Open prostatectomyOpen prostatectomy can be done either Open prostatectomy can be done either TranvesicalTranvesical, , perinealperineal or or RetropupicRetropupic prostatectomy. prostatectomy.
In recent years the suprapubic & retropubic approaches In recent years the suprapubic & retropubic approaches for BPH have been limited to approximately 10% of for BPH have been limited to approximately 10% of patients.patients.
Indications for suprapubic prostatectomy are a gland Indications for suprapubic prostatectomy are a gland size greater than 100g, cystolithotomy or diverticulum size greater than 100g, cystolithotomy or diverticulum excision.excision.
Most post op complications are similar to TURP, Most post op complications are similar to TURP, however, wound infection & thromboembolism are however, wound infection & thromboembolism are additional complications. additional complications.


Minimally Invasive TherapyMinimally Invasive Therapy
1) Laser prostatectomy1) Laser prostatectomy
advantages over TURP: technical simplicity, lack of advantages over TURP: technical simplicity, lack of complications & shorter hospital stay.complications & shorter hospital stay.
Laser energy works by thermal destruction of tissue.Laser energy works by thermal destruction of tissue.
disadvantages: lack of tissue availability for pathologic disadvantages: lack of tissue availability for pathologic examination, longer postop cathitarization time, more examination, longer postop cathitarization time, more irritative voiding complain, & high costsirritative voiding complain, & high costs

Minimally Invasive TherapyMinimally Invasive Therapy
2) Transurethral needle ablation2) Transurethral needle ablation
High frequency radio waves to cause thermal injury to High frequency radio waves to cause thermal injury to the prostate.the prostate.
3) High-intensity focused Ultrasound3) High-intensity focused Ultrasound

Minimally Invasive TherapyMinimally Invasive Therapy
4) Prostate stents4) Prostate stentsIn recent years, metallic spirals & stents have been used In recent years, metallic spirals & stents have been used as permanent indwelling prostheses .as permanent indwelling prostheses .
These stents may be placed endoscopically & under These stents may be placed endoscopically & under radiologic guidance. radiologic guidance.

Minimally Invasive TherapyMinimally Invasive Therapy
5) Transurethral balloon dilatation5) Transurethral balloon dilatationIt involves the use of non compliant balloons to dilate the It involves the use of non compliant balloons to dilate the prostate under pressure.prostate under pressure.
This pressure is maintained for 15 min.This pressure is maintained for 15 min.
The exact mechanism is unclear.The exact mechanism is unclear.
6) Thermotherapy6) Thermotherapy

Prostate CancerProstate Cancer

IncidenceIncidenceprostate cancers is the 2prostate cancers is the 2ndnd most common cause of cancer deaths in most common cause of cancer deaths in USA.USA.
Autopsy studies demonstrate that there is an increasing incidence Autopsy studies demonstrate that there is an increasing incidence starting around 30% in men at 50 increasing to 75% in men at 75 starting around 30% in men at 50 increasing to 75% in men at 75 years.years.
USAUSA (blacks)(blacks) 137/100,000 per year 137/100,000 per year
GermanyGermany 45/100,000 per year45/100,000 per year
KuwaitKuwait 6.5/100,000 per year (1998-2002) 6.5/100,000 per year (1998-2002)KuwaitKuwait 12.8/100,000 per year (2002-2005) 12.8/100,000 per year (2002-2005)
ChinaChina 1/100,000 per year1/100,000 per year

EtiologyEtiology
* * Genetic predisposition, racial origin.Genetic predisposition, racial origin.Autosomal dominant inheritance of Autosomal dominant inheritance of rarely yet highly penetrant gene.rarely yet highly penetrant gene.
* * Hormonal influences.Hormonal influences.
* * Dietary & environmental factors.Dietary & environmental factors.
* Infectious agents.* Infectious agents.
* Sexual habits, multiple sexual partner.* Sexual habits, multiple sexual partner.
* Idiopathic* Idiopathic

PathogenesisPathogenesisMost prostate cancers are Most prostate cancers are adenocarcinomasadenocarcinomas arising arising from prostatic acinar cells.from prostatic acinar cells.
Prostate normally atrophies between the 5Prostate normally atrophies between the 5thth & 7 & 7thth decades of life with some atypical and hyperplastic decades of life with some atypical and hyperplastic changes.changes.
Among dysplastic changes, prostatic intraepithelial Among dysplastic changes, prostatic intraepithelial neoplasia neoplasia (PIN)(PIN) considered premalignant lesion found in considered premalignant lesion found in 30% of patients with prostate cancers.30% of patients with prostate cancers.
70% of prostate cancers arise in the peripheral zone of 70% of prostate cancers arise in the peripheral zone of the prostate; 15-20% arise in the central zone; 10-15% the prostate; 15-20% arise in the central zone; 10-15% arise in the transition zone.arise in the transition zone.
Most prostate cancers are Most prostate cancers are multicentricmulticentric..

Grading of Prostatic CancerGrading of Prostatic Cancer
Gleason grading system is the most Gleason grading system is the most widely used. It’s based on glandular widely used. It’s based on glandular differentiation:differentiation:
* Gleason Score 2-4 * Gleason Score 2-4 well differentiatedwell differentiated
5-7 5-7 moderately moderately differentiateddifferentiated
8-10 8-10 poorly differentiatedpoorly differentiated

Stages of Prostatic CancerStages of Prostatic Cancer

Pattern of ProgressionPattern of ProgressionLocal Metastasis:Local Metastasis:
Cancers arising in close proximity are prone to spread Cancers arising in close proximity are prone to spread early to the urethra, periprostatic tissues, bladder and early to the urethra, periprostatic tissues, bladder and seminal vesicles.seminal vesicles.
Spread to seminal vesicles indicates ominous prognosis Spread to seminal vesicles indicates ominous prognosis with 50% of patients developing distant metastasis.with 50% of patients developing distant metastasis.
Rectal invasion is rare, ? Due to the tough Denonvilliers’ Rectal invasion is rare, ? Due to the tough Denonvilliers’ fascia in between.fascia in between.
Ureteral invasion by direct extension can occur but late, Ureteral invasion by direct extension can occur but late, usually lymph node and distant metastasis present at usually lymph node and distant metastasis present at this time.this time.

Pattern of ProgressionPattern of Progression
Distant MetastasisDistant Metastasis
Osseous metastases is most common form of Osseous metastases is most common form of hematogenous metastases and occur in 85% of patients hematogenous metastases and occur in 85% of patients dying from prostate cancerdying from prostate cancer
Frequent sites: lumbar spines, pelvis, proximal femur, Frequent sites: lumbar spines, pelvis, proximal femur, thoracic spines, ribs, sternum and skull.thoracic spines, ribs, sternum and skull.
Extension to the axial skeleton vai the Batson’s plexus of Extension to the axial skeleton vai the Batson’s plexus of presacral veins which communicate with the pre & presacral veins which communicate with the pre & periprostatic venous complex.periprostatic venous complex.


Clinical FindingsClinical FindingsSymptomsSymptoms
Most prostate cancers are discovered because of Most prostate cancers are discovered because of elevated PSA or with incidental finding on rectal elevated PSA or with incidental finding on rectal examination.examination.
prostate cancers rarely cause symptoms but may prostate cancers rarely cause symptoms but may present with bladder outlet obstruction, acute urinary present with bladder outlet obstruction, acute urinary retention, hematuria or incontinenceretention, hematuria or incontinence
SignsSignsirregular firm or hard prostatic nodule during rectal irregular firm or hard prostatic nodule during rectal examination.examination.
Median sulcus is absentMedian sulcus is absent

Tumor MarkersTumor MarkersProstate Specific Antigen (PSA)Prostate Specific Antigen (PSA)
– Glycoprotein secreted in the cytoplasm of the prostatic Glycoprotein secreted in the cytoplasm of the prostatic cells and function normally in liquefaction of the cells and function normally in liquefaction of the semen, normal value in young adult 0-4 ng/dL.semen, normal value in young adult 0-4 ng/dL.
– PSA elevation is proportional to the size of the PSA elevation is proportional to the size of the transitional zone. 1g of prostate cancer will ↑PSA by transitional zone. 1g of prostate cancer will ↑PSA by 0.3 ng/dL.0.3 ng/dL.
– PSA production by the malignant cell depends on the PSA production by the malignant cell depends on the degree of differentiation, well diff. gland will give moredegree of differentiation, well diff. gland will give more
– Prostate cancer with poor differentiation have normal Prostate cancer with poor differentiation have normal PSAPSA

Tumor Markers (PSA)Tumor Markers (PSA)
– PSA rises by 0.04 per year in individual without PSA rises by 0.04 per year in individual without cancercancer upper limit of PSA for upper limit of PSA for
- 40-49 yrs is 2.5- 40-49 yrs is 2.5 ng/dLng/dL- 50-59 yrs is 3.5- 50-59 yrs is 3.5 ng/dLng/dL- 60-69 yrs is 4.5- 60-69 yrs is 4.5 ng/dLng/dL- 70-79 yrs is 6.5- 70-79 yrs is 6.5 ng/dL.ng/dL.
– PSA density (PSA level/prostate volume) level PSA density (PSA level/prostate volume) level between 0.1-0.15 associated with 15% incidence of between 0.1-0.15 associated with 15% incidence of cancer, level above 0.15 associated with 60%.cancer, level above 0.15 associated with 60%.
– New studies showed two types of PSA,New studies showed two types of PSA,a. complex PSA associated with cancera. complex PSA associated with cancerb. free PSA goes with BPH.b. free PSA goes with BPH.

Tumor MarkersTumor Markers
Other Tumor MarkersOther Tumor Markers
– DNA ploidy recently reported to be useful in predicting DNA ploidy recently reported to be useful in predicting prognosis in prostate cancer.prognosis in prostate cancer.
– Low grade tumors associated with diploidy and high Low grade tumors associated with diploidy and high grade tumors with aneuploidy.grade tumors with aneuploidy.
– Patients with deploid tumors do well with expectant Patients with deploid tumors do well with expectant therapy while those with aneuploidy do poorly.therapy while those with aneuploidy do poorly.

Prostate BiopsyProstate Biopsy
Diagnosis of prostate cancers is confirmed by Diagnosis of prostate cancers is confirmed by needle and core biopsy.needle and core biopsy.
Ultrasound guided systematic sampling of the Ultrasound guided systematic sampling of the prostate in 4 quadrants provides the most prostate in 4 quadrants provides the most accurate information for staging and grading the accurate information for staging and grading the cancer.cancer.

ImagingImaging1)1) Trans-rectal U/STrans-rectal U/S
– Can identify Can identify 60% of cancers even if non-palpable.60% of cancers even if non-palpable.
– By allowing precise placement of biopsy needle in By allowing precise placement of biopsy needle in various quadrants, adequate sampling achieved.various quadrants, adequate sampling achieved.
– More accurate than DRE at detecting extra-capsular More accurate than DRE at detecting extra-capsular extension.extension.
– Allow biopsy of seminal vesicles which improve Allow biopsy of seminal vesicles which improve staging accuracy.staging accuracy.
– Disadvantage of TRUS include the inability to look Disadvantage of TRUS include the inability to look at the pelvic lymph nodes.at the pelvic lymph nodes.


ImagingImaging2) CT:2) CT:
used only when extensive L.N. disease is used only when extensive L.N. disease is suspected and it is based only on the size of the nodes suspected and it is based only on the size of the nodes thus false +ve and –ve are common.thus false +ve and –ve are common.
3) MRI:3) MRI:not useful because of the cost and the overlap in not useful because of the cost and the overlap in
the appearance of benign & malignant processes, but its the appearance of benign & malignant processes, but its more accurate than TRUS for staging extracapsular more accurate than TRUS for staging extracapsular extension and seminal vesicle involvement.extension and seminal vesicle involvement.
4) Bone scanning:4) Bone scanning:– most common way to assess systemic metastasis. most common way to assess systemic metastasis. – False +ve rate is less than 2%. False +ve rate is less than 2%. – Diagnosis is confirmed by plain radiographs, thin section CT or Diagnosis is confirmed by plain radiographs, thin section CT or
MRI and bone biopsyMRI and bone biopsy


Management of Localized DiseaseManagement of Localized Disease
The current therapy of patients with low stage disease The current therapy of patients with low stage disease (stage T1 and T2) is radical prostatectomy & (stage T1 and T2) is radical prostatectomy & radiotherapy to the prostate.radiotherapy to the prostate.
Treatment mortality is under 1%.Treatment mortality is under 1%.
For patients For patients 75 years of age, treatment is “watchful 75 years of age, treatment is “watchful waiting”waiting”


Radical ProstatectomyRadical Prostatectomy
Retropubic approachRetropubic approach allow simultaneous access to allow simultaneous access to the prostate and the pelvic LN, but it is often associated the prostate and the pelvic LN, but it is often associated with a greater amount of blood loss from the dorsal vein with a greater amount of blood loss from the dorsal vein complex.complex.
Perineal approachPerineal approach requires separate incision for requires separate incision for pelvic LN, associated with minimal blood loss and it is pelvic LN, associated with minimal blood loss and it is preferred for obese individuals.preferred for obese individuals.
5 yrs disease free survival for Stage T1 is 92% and for 5 yrs disease free survival for Stage T1 is 92% and for stage T2 is 86%stage T2 is 86%


Complication of Surgical TherapyComplication of Surgical Therapy
Intra-operatively:Intra-operatively:– bleeding and injury to the obturator nerve, bleeding and injury to the obturator nerve,
ureter or rectum ureter or rectum
Post-operatively:Post-operatively:– DVT & PE.DVT & PE.– Symptomatic pelvic lymphadenocele.Symptomatic pelvic lymphadenocele.– Wound infections & UTIWound infections & UTI
The long term :The long term :– Incontinence and impotence. Incontinence and impotence.

Radiation TherapyRadiation Therapy
All modern techniques use CT scans for accurate localization All modern techniques use CT scans for accurate localization of the prostate.of the prostate.
Generally, prostate is subjected to 6800-7000 rads and the Generally, prostate is subjected to 6800-7000 rads and the pelvic LNs are subjected to 4500-5000 rads.pelvic LNs are subjected to 4500-5000 rads.
Total treatment duration is 6-7 weeks.Total treatment duration is 6-7 weeks.
5 yrs disease free survival rate for Stage T1 is 83% and for 5 yrs disease free survival rate for Stage T1 is 83% and for Stage T2 is 72%.Stage T2 is 72%.
PSA level is useful for assessing the response to RTPSA level is useful for assessing the response to RT
Rising PSA or PSA level persistently more than 30 ng/dL Rising PSA or PSA level persistently more than 30 ng/dL indicate poor response to RT.indicate poor response to RT.


Complication of Radiation TherapyComplication of Radiation Therapy
Intestinal sequelae:Intestinal sequelae:– Rectal bleeding, tenesmus, mucous discharge, Rectal bleeding, tenesmus, mucous discharge,
diarrhea, fecal incontinence, intestinal obstruction and diarrhea, fecal incontinence, intestinal obstruction and rectal strictures.rectal strictures.
Urological sequelae:Urological sequelae:– Frequency, dysurea, cystitis, hematuria and urethral Frequency, dysurea, cystitis, hematuria and urethral
stricturestricture
Edema of the extremities and impotenceEdema of the extremities and impotence
Majority of these complications are minor and persist Majority of these complications are minor and persist less than 6 monthsless than 6 months

Neoadjuvant Hormonal TherapyNeoadjuvant Hormonal Therapy
LHRH agonists and antiandrogensLHRH agonists and antiandrogens
Studies showed that hormonal therapy will not down-Studies showed that hormonal therapy will not down-stage the cancer in patient with stage T3, however, in stage the cancer in patient with stage T3, however, in patient with stage T2 the hormonal therapy will reduce patient with stage T2 the hormonal therapy will reduce the size and the incidence of positive marginsthe size and the incidence of positive margins

Manegment of patients with Margin-Positive Manegment of patients with Margin-Positive Disease / Extracapsular ExtensionDisease / Extracapsular Extension
60% of positive margins are at postlateral areas, 60% of positive margins are at postlateral areas, 30% are posterior30% are posterior
In stage T1 cancers, 40% of positive margins In stage T1 cancers, 40% of positive margins are anterior.are anterior.
Adjuvant radiation in these patients controls Adjuvant radiation in these patients controls local recurrence but whether it reduces systemic local recurrence but whether it reduces systemic recurrences is unclear.recurrences is unclear.
Adjuvant hormones & more recently intermittent Adjuvant hormones & more recently intermittent adjuvant hormones appears to reduce PSA.adjuvant hormones appears to reduce PSA.

Management of locally extensive Management of locally extensive diseasedisease
Stage T3,T4 or C prostate cancer are advised to Stage T3,T4 or C prostate cancer are advised to have radiation therapy. Surgery is not have radiation therapy. Surgery is not
recommended.recommended.


Management of distant metastatic diseaseManagement of distant metastatic disease
The standard treatment is androgen ablation therapy to lower The standard treatment is androgen ablation therapy to lower serum testosterone.serum testosterone.
Methods of lowering testosterone include:Methods of lowering testosterone include:(1) Bilateral subcapsular orchiectomy(1) Bilateral subcapsular orchiectomy
(2) LHRH(2) LHRH agonist agonist By downregulating pituitary LH production.By downregulating pituitary LH production.
(3) Estrogen(3) Estrogen e.g. diethylstilbestrol which create negative feedback to e.g. diethylstilbestrol which create negative feedback to the pituitary. the pituitary.
S/E include impotence, breast tenderness, & hot flushesS/E include impotence, breast tenderness, & hot flushes

Prognostic Factors in Ca prostatePrognostic Factors in Ca prostateStageStage 1&2 1&2 65 - 98% 5-yrs survival rate 65 - 98% 5-yrs survival rate
3 3 60% 5-yrs survival rate 60% 5-yrs survival rate 4 4 30% 5yrs survival rate 30% 5yrs survival rate
GradeGrade
Tumor VolumeTumor Volume– < 0.5 ml < 0.5 ml →→ no capsular penetration no capsular penetration– < 4 ml < 4 ml →→ less SV invasion & LN metastasis less SV invasion & LN metastasis

Prostatitis Prostatitis

NIH Consensus Conference on ProstatitisNIH Consensus Conference on Prostatitis (1995)(1995)
Category ICategory I: Acute Bacterial Prostatitis = Acute : Acute Bacterial Prostatitis = Acute infection of the prostate glandinfection of the prostate gland
Category IICategory II: Chronic Bacterial Prostatitis = : Chronic Bacterial Prostatitis = Recurrent infection of the prostate.Recurrent infection of the prostate.
Category IIICategory III: Chronic Abacterial : Chronic Abacterial Prostatitis/CPPS: No demonstrable infectionProstatitis/CPPS: No demonstrable infection
– Category IIIACategory IIIA: Inflammatory CPPS = WBCs in : Inflammatory CPPS = WBCs in semen/EPS/VB3semen/EPS/VB3
– Category IIIBCategory IIIB: Noninflammatory CPPS = No WBCs in : Noninflammatory CPPS = No WBCs in semen/EPS/VB3semen/EPS/VB3
Category IVCategory IV: Asymptomatic Inflammatory : Asymptomatic Inflammatory ProstatitisProstatitis

Acute bacterial prostatitisAcute bacterial prostatitis
EtiologyEtiology• Is mainly caused by aerobic gram negative rods. Is mainly caused by aerobic gram negative rods. (E-coli and Pseudomonas aerigenosa)(E-coli and Pseudomonas aerigenosa)
• Common in people with “uptight personality”Common in people with “uptight personality”
The possible routes of infection include:The possible routes of infection include: 1)1) Ascent from the urethra. Ascent from the urethra. 2)2) Reflux of infected urine into prostatic ducts that empty into the Reflux of infected urine into prostatic ducts that empty into the
posterior urethra. posterior urethra. 3)3) Direct extension (lymphatogenous spread): from the rectum. Direct extension (lymphatogenous spread): from the rectum.
Ascending infection and reflux of infected urine into prostatic ducts Ascending infection and reflux of infected urine into prostatic ducts are probably the most common routes of prostatic infection.are probably the most common routes of prostatic infection.

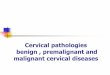
Leukocytic infiltration of stroma and glandular lumina during acute bacterial prostatitis

Acute bacterial prostatitisAcute bacterial prostatitisClinical FindingsClinical Findings
A. SymptomsA. SymptomsAcute febrile illness characterized by chills, low back and perineal Acute febrile illness characterized by chills, low back and perineal pain, urinary urgency and frequency, nocturia, dysuria, and pain, urinary urgency and frequency, nocturia, dysuria, and varying degrees of bladder outlet obstruction.varying degrees of bladder outlet obstruction.Both myalgia and arthralgia are common.Both myalgia and arthralgia are common.
B. SignsB. SignsModerate or high grade fever.Moderate or high grade fever.Rectal palpation: tender, swollen, indurated, boggy and warm to Rectal palpation: tender, swollen, indurated, boggy and warm to be touched. be touched. Since acute cystitis often accompanies acute bacterial prostatitis, Since acute cystitis often accompanies acute bacterial prostatitis, the urine may be cloudy. the urine may be cloudy. Initial, terminal, or even total gross hematuria may be observed Initial, terminal, or even total gross hematuria may be observed occasionally.occasionally.

Acute bacterial prostatitisAcute bacterial prostatitisC. Laboratory FindingsC. Laboratory Findings
Voided urine usually shows significant pyuria, microscopic Voided urine usually shows significant pyuria, microscopic hematuria, and bacilluria. hematuria, and bacilluria.
The prostatic expressate is purulent and yields the infecting The prostatic expressate is purulent and yields the infecting pathogen in heavy growth on culture plates.pathogen in heavy growth on culture plates.
Because massage of an acutely infected prostate is painful for the Because massage of an acutely infected prostate is painful for the patient and can produce bactermia, prostatic massage is generally patient and can produce bactermia, prostatic massage is generally contraindicated. Except under anaesthesia and antibiotic cover.contraindicated. Except under anaesthesia and antibiotic cover.
D. Instrumental ExaminationD. Instrumental ExaminationTransurethral instrumentation should be avoided during the acute Transurethral instrumentation should be avoided during the acute
stage of bacterial prostatitis.stage of bacterial prostatitis.

Acute bacterial prostatitisAcute bacterial prostatitis
ComplicationsComplications
• Acute urinary retention.Acute urinary retention.• Acute bacterial cystitis.Acute bacterial cystitis.• Acute pyelonephritis.Acute pyelonephritis.• Unilateral or bilateral acute bacterial epididymitis.Unilateral or bilateral acute bacterial epididymitis.• bactermia with possible septic shock.bactermia with possible septic shock.
1)1) Rarely meningitis, spread of infection via Batesan’s Rarely meningitis, spread of infection via Batesan’s veinous plexusveinous plexus
2)2) Prostate abcessProstate abcess

Acute bacterial prostatitisAcute bacterial prostatitis
Prostatic AbscessProstatic Abscess
More recently, about 70% of prostatic abscesses have been caused More recently, about 70% of prostatic abscesses have been caused by coliform bacteria, mostly E-coli. by coliform bacteria, mostly E-coli.
Although the pathogenesis remains unclear, most cases of prostatic Although the pathogenesis remains unclear, most cases of prostatic abscesses are probably complications of acute bacterial prostatitis. abscesses are probably complications of acute bacterial prostatitis.
The signs and symptoms of prostatic abscess can mimic those of The signs and symptoms of prostatic abscess can mimic those of bacterial prostatitis; Fluctuation is an important diagnostic clue. bacterial prostatitis; Fluctuation is an important diagnostic clue.
Once the diagnosis of prostatic abscess is made preferred Once the diagnosis of prostatic abscess is made preferred treatment consists of surgical drainage combined with appropriate treatment consists of surgical drainage combined with appropriate antimicrobial therapy. antimicrobial therapy.
With proper diagnosis and therapy, the overall prognosis is good.With proper diagnosis and therapy, the overall prognosis is good.

Acute bacterial prostatitisAcute bacterial prostatitisTreatmentTreatment
• Fluoroquinolone Fluoroquinolone • Ciprofloxacin Ciprofloxacin • Trimethoprim-sulfamethoxazole Trimethoprim-sulfamethoxazole • Alternatively, initial therapy with Gentamicin or Alternatively, initial therapy with Gentamicin or
Amikacin or Tobraminycin, 3-5 mg/kg/d divided into 3 Amikacin or Tobraminycin, 3-5 mg/kg/d divided into 3 intravenous or intramuscular doses, plus ampicillen, intravenous or intramuscular doses, plus ampicillen, 2 g intravenously every 6 hours, is recommended 2 g intravenously every 6 hours, is recommended until the results of culture and sensitivity tests are until the results of culture and sensitivity tests are known.known.
Transurethral instrumentation is contraindicated Transurethral instrumentation is contraindicated during acute infection.during acute infection.

Acute bacterial prostatitisAcute bacterial prostatitis
PrognosisPrognosis
• Unless the patient develops septicemia and septic Unless the patient develops septicemia and septic shock, the prognosis generally is good with prompt shock, the prognosis generally is good with prompt and appropriate therapy.and appropriate therapy.

Chronic Bacterial ProstatitisChronic Bacterial Prostatitis
Etiology:Etiology:
Is a non acute infection of the prostate caused by one or Is a non acute infection of the prostate caused by one or more specific bacteria.more specific bacteria.
The possible routes of infection are the same The possible routes of infection are the same in acute and chronic bacterial prostatitis.in acute and chronic bacterial prostatitis.

Chronic Bacterial ProstatitisChronic Bacterial Prostatitis
Clinical FindingsClinical FindingsA. SymptomsA. Symptoms• Asymptomatic; most have varying degrees of irritative voiding Asymptomatic; most have varying degrees of irritative voiding
dysfunction and low back or perineal pain and discomfort. dysfunction and low back or perineal pain and discomfort. • Occasionally, myalgia and arthralgia accompany the other Occasionally, myalgia and arthralgia accompany the other
symptoms.symptoms.
B. SignsB. Signs• On rectal examination, the prostate may feel normal (rarely), On rectal examination, the prostate may feel normal (rarely),
boggy, or very tender focally indurated.boggy, or very tender focally indurated.
• Crepitation may be felt when large prostatic stones are present or Crepitation may be felt when large prostatic stones are present or if infection is due to gas forming organisms commenly seen in if infection is due to gas forming organisms commenly seen in diabetic patients. diabetic patients.
• Secondary epididymitis sometimes is associated with chronic Secondary epididymitis sometimes is associated with chronic bacterial prostatitis.bacterial prostatitis.

Chronic Bacterial ProstatitisChronic Bacterial Prostatitis
C. Laboratory findingsC. Laboratory findings• The Prostatic secretions obtained by prostatic massage typically The Prostatic secretions obtained by prostatic massage typically
show excessive numbers of inflammatory cells. show excessive numbers of inflammatory cells.
• The presence of large numbers of lipid laden macrophages in The presence of large numbers of lipid laden macrophages in prostatic fluid correlates particularly well with the presence of prostatic fluid correlates particularly well with the presence of prostatic inflammation. prostatic inflammation.
D. X-Ray findingsD. X-Ray findings• normal unless there are complications (eg, prostatic calculi, normal unless there are complications (eg, prostatic calculi,
prostatic enlargement, urethral stricture, renal infection).prostatic enlargement, urethral stricture, renal infection).
E. Instrumental ExaminationE. Instrumental Examination• Cystoscopy and urethroscopy may reveal normal findings or Cystoscopy and urethroscopy may reveal normal findings or
erythema and edema of the prostatic urethra, with or without erythema and edema of the prostatic urethra, with or without inflammatory polyps.inflammatory polyps.

Chronic Bacterial ProstatitisChronic Bacterial Prostatitis
ComplicationsComplications
• Relapsing recurrent UTI.Relapsing recurrent UTI.
• Ascending bacterial infection of the upper urinary tract Ascending bacterial infection of the upper urinary tract and bacterial epididymitis.and bacterial epididymitis.
• Bladder outlet obstruction.Bladder outlet obstruction.

Chronic Bacterial ProstatitisChronic Bacterial Prostatitis
TreatmentTreatment
General MeasuresGeneral Measures
Symptoms can be relieved by the liberal use of hot sits Symptoms can be relieved by the liberal use of hot sits baths. baths.
Irritative voiding discomfort and pain often respond to the Irritative voiding discomfort and pain often respond to the use of anti-inflammatory agents ( eg, indomethacin, use of anti-inflammatory agents ( eg, indomethacin, ibuprofen) and anticholinergic drugs.ibuprofen) and anticholinergic drugs.

Chronic Bacterial ProstatitisChronic Bacterial Prostatitis
TreatmentTreatment
Surgical MeasuresSurgical Measures
Radical prostatovesiculectomy is curative; unfortunately, the Radical prostatovesiculectomy is curative; unfortunately, the sequels of this operation ( sexual impotence and possible urinary sequels of this operation ( sexual impotence and possible urinary incontinence) seldom make this a desirable choice.incontinence) seldom make this a desirable choice.
Transurethral prostatectomy can be curative provided all infective Transurethral prostatectomy can be curative provided all infective stones and tissues are successfully removed; unfortunately, this stones and tissues are successfully removed; unfortunately, this may be difficult to achieve, especially since the peripheral zone of may be difficult to achieve, especially since the peripheral zone of the prostate usually contains the most foci of the infection.the prostate usually contains the most foci of the infection.

Chronic Bacterial ProstatitisChronic Bacterial Prostatitis
PrognosisPrognosis
Chronic bacterial prostatitis is difficult to cure Chronic bacterial prostatitis is difficult to cure permanently, but its symptoms and tendency to cause permanently, but its symptoms and tendency to cause recurrent UTIs generally can be controlled by recurrent UTIs generally can be controlled by suppressive antimicrobial therapy. suppressive antimicrobial therapy.

Chronic Abacterial ProstatitisChronic Abacterial Prostatitis EtiologyEtiology
Is the most common of the prostatitis syndromes; its Is the most common of the prostatitis syndromes; its cause is unknown. cause is unknown.
There has been much speculations but little proof that There has been much speculations but little proof that chlamydial infection is responsible for many cases of chlamydial infection is responsible for many cases of apparent nonbacterial prostatitis.apparent nonbacterial prostatitis.
Like wise, there is little evidence that infection due to U Like wise, there is little evidence that infection due to U urealyticum plays an important role in this prostatitis. urealyticum plays an important role in this prostatitis.
Some researchers believe that non bacterial prostatitis is Some researchers believe that non bacterial prostatitis is an autoimmune disease of the prostate.an autoimmune disease of the prostate.

Chronic Abacterial ProstatitisChronic Abacterial Prostatitis
Pathogenesis and PathologyPathogenesis and Pathology
The cause of the pathogenesis of nonbacterial prostatitis The cause of the pathogenesis of nonbacterial prostatitis are unknown. are unknown.
The histopathologic findings are non specific and The histopathologic findings are non specific and resemble those seen in chronic bacterial prostatitis.resemble those seen in chronic bacterial prostatitis.

Chronic Abacterial ProstatitisChronic Abacterial Prostatitis
Clinical FindingsClinical Findings
The signs and symptoms are similar except that The signs and symptoms are similar except that documented UTI almost never occurs in former.documented UTI almost never occurs in former.
ComplicationsComplications
Non bacterial prostatitis causes no known organic Non bacterial prostatitis causes no known organic complicationscomplications

Chronic Abacterial ProstatitisChronic Abacterial Prostatitis
TreatmentTreatment
• Antimicrobial therapy should be tried for at least 4 weeks.Antimicrobial therapy should be tried for at least 4 weeks.
• Therapy must be directed toward control of the symptoms. Therapy must be directed toward control of the symptoms.
• Symptomatic flare ups often respond to anti-inflammatory agents. Symptomatic flare ups often respond to anti-inflammatory agents.
• Like most patients with prostatodynia, most patients with non Like most patients with prostatodynia, most patients with non bacterial prostatitis respond favorably to therapy using an alpha bacterial prostatitis respond favorably to therapy using an alpha blocking agent. blocking agent.
• Most authorities agree that prostatectomy is not indicated. Most authorities agree that prostatectomy is not indicated.

THANK YOU THANK YOU