- 1.Biological options in AVNfemur Dr. Sushil Paudel
2. Avascular necrosis (also osteonecrosis,bone
infarction,aseptic necrosis,ischemic bone necrosis,and AVN) Disease
where there is cellular deathof bone components due tointerruption
of the blood supply 3. The LEV enters the femoral head within a
1-cm-wide zone between the cartilage of the femoralhead and the
cortical bone of the femoralneck. Supply the lateral and central
thirds of thefemoral head When patent, the artery of the
ligamentumteres (ALT) supplies the medial third of thefemoral head
4. Etiology and pathophysiology 5. AVN : areas of dead trabecular
bone andmarrow extending to involve the subchondralplate.
Anterolateral aspect of the femoral head, theprincipal
weightbearing region typicallyinvolved, but any region of the
femoral headmay be involved. Involved segment usually never
fullyrevascularizes, and collapse of the femoralhead usually occurs
6. Elderly persons at decreased risk Fat cells become smaller,
space between fatcells fills with a loose reticulum and mucoid
fluid,which are resistant AVN. Condition is termed gelatinous
marrow. Even in the presence of increasedintramedullary pressure,
interstitial fluid escapesinto the blood vessels, leaving the
spaces free toabsorb additional fluid. 7. Clinical picture
nonspecific Presenting symptom unilateral hip pain, whichmay be
followed by a limp and a decreasedrange of motion (ROM). Young
adults between the ages of 30 and 40most frequently affected
Bilateral in more than 50% of patients 8. Sequelae of avascular
necrosis Minimal AVN - If the vascular area is small and isnot
adjacent to an articular surface, the patientmay be asymptomatic;
healing may occurspontaneously, or the disease may remainundetected
or be discovered incidentallyduring workup for other conditions. 9.
More severe AVN : repair begins at the interfacebetween viable bone
and necrotic bone. Dead bone reabsorbed only partially. Reactive
and reparative bone laid down on deadtrabeculae, resulting in a
sclerotic margin ofthickened trabeculae within an advancing front
ofhyperemia, inflammation, bone resorption, andfibrosis. Incomplete
resorption of dead bone has a mixedsclerotic and cystic appearance
on radiographs.Necrosis and repair are ongoing in various stages
ofevolution within a single lesion. 10. Mechanical failure - In the
subchondral regionmicrofractures do not heal Progression of the
microfractures results in adiffuse subchondral fracture,
seenradiographically as the crescent sign Following subchondral
fracture and progressiveweightbearing, collapse of the
articularcartilage occurs Continued fracture, necrosis, and
furtherweightbearing may progress to degenerativejoint disease
(DJD) and joint dissolution 11. IMAGING MODALITIES AP and lateral
radiographs of both hips Initially within normal limits because it
takes aperiod of weeks to months after the initiatingevent for
changes to appear on radiographs The first changes to be noted are
areas ofradiolucency and sclerosis within the femoralhead, usually
in the anterior superior quadrant 12. If osteonecrosis suspected
despite normal-appearing plain radiographs, MRI of both hipsshould
be obtained because more than 50% ofcases are bilateral 13. MRI
Help guide interventional procedures such ascore decompression,
Demonstrate response of the femoral head totreatment Noninvasive
means of evaluating articularcartilage congruity Sequential
evaluation of asymptomatic lesionsundetectable on plain
radiographs. 14. I DDPlain film radiographs Malignancy
Osteomyelitis Transient osteoporosis of the hip Bone sarcoma
Advanced Degenerative joint disease Insufficiency fractures
Epiphyseal dysplasia Bone metastases 15. Bone scintigrams Infection
Plasma cell myeloma Skeletal metastasis Hemangioma Radiation
therapy Arthritis Sympathetic dystrophy Bone marrow edema syndrome
Bone metastases 16. CT scans Degenerative disease Insufficiency
fracture Malignancy Infection Plasma cell myeloma Bone metastases
17. MRIs Transient osteoporosis of the hip Transient bone marrow
syndrome Bone bruise Epiphyseal stress fracture Infection
Infiltrative neoplasm Insufficiency fracture Bone metastases 18.
Ficat and Arlet Radiographic StagingSystem for AVN Stage 0
(preclinical and preradiologic) Avascular necrosis (AVN) can be
suggestedonly if it has already been diagnosed in thecontralateral
hip. 19. Stage 1 (preradiologic)Defined by normal findings on
radiographs andpositive findings on MRI or bone scintigraphy. Early
resorptive stage, Late in this stage, plain radiographs may
showminimal osteoporosis and/or blurring and poordefinition of the
bony trabeculae 20. Stage 2 (reparative) Demineralization evident;
first manifestation ofthe reparative stage, represents resorption
ofdead bone, and may be generalized or patchyor appear in the form
of small cysts within thefemoral head 21. Anteroposterior view of
thepelvis in a patient withbilateral avascular necrosisof the
femoral head. Mildflattening to the superioraspect of the right
femoralhead (open arrow)indicates stage 3 disease.The left femoral
head has anormal contour, indicatingstage 2 disease. 22. Stage 3
(early collapse of the femoralhead ) Linear subcortical lucency,
representing a fracture line,present immediately beneath the
articular cortex andmay extend into the articular cartilage at
thesuperolateral aspect of the femoral head. Crescent sign ; best
demonstrated on a frogleg view Subarticular cortex remain attached
to the cartilageand is separated from the underlying femur by soft
tissue,termed the eggshell sign. The femoral head initially
preserves its roundappearance, but later, it demonstrates
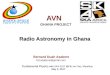
collapse,indicated by joint-space widening. 23. Frogleg lateral
view of the right hip in a patient with avascular necrosis shows
thecrescent sign, indicating subchondral fracture. 24. Stage 4
(progressive degenerative disease) Further flattening of the
femoral head with lossof its smooth convex contour Ultimately, the
superior femoral fragment,representing the articular surface and
theimmediate subchondral bone becomeseparated from the underlying
femoral head ordepressed and compacted into the femoralhead.
Fragments of bone and cartilage may separatefrom the underlying
femur, become loosebodies. 25. Severe collapse anddestruction of
the femoralhead leads to progressivedegenerative jointdisease (DJD)
with joint-space narrowing,marginal osteophyteformation,
andsubchondral cystformation 26. Steinberg et als Staging System
for AVN Steinberg et al proposed a 6-stage classificationsystem
based on that of Ficat and Arlet andincluded radiologic clinical
classificationfindings 27. Stage 0 - both preclinical and
preradiologic,identified when imaging is performed to evaluateAVN
in the contralateral hip or to exclude otherdiseases. Abnormal MRI
findings, normalradiographic findings, and normal bone scanfindings
Stage 1 - normal radiographic findings or minimaldemineralization
or blurred trabeculae,Pain in theanterior groin or thigh ,Limited
ROM in the hip Stage 2 - Osteoporosis, groin pain, and
mottledsclerotic and/or cystic area 28. Stage 3 - crescent sign
(subchondral fracture) ,pain with subchondral fracture activity,
and nofemoral head flattening Stage 4 - marked collapse and
fractureinvolving the articular surface, Segmentalflattening, pain
with femoral head activity, noacetabular involvement, and normal
joint space Stage 5 - joint space narrowing, resting pain,and
acetabular degeneration (DJD) 29. AVN Classification per Central
Avascular SegmentSignal Alterations 30. Class A - Central
osteonecrotic focus signal analogous to that of fat arenoted.
Increased signal is demonstrated on T1WIs, and intermediate tohigh
signal is demonstrated on T2WIs 31. Class B - The presence of
central osteonecrotic focus signal analogous to that of blood is
observed. Increasedsignal is demonstrated on both T1WIs and T2WIs
32. Class C - Central osteonecrotic focus signal analogous to that
of fluid is present. Decreased signal isdemonstrated on T1WIs, and
increased signal is demonstrated on T2WIs 33. Class D - The
presence of central osteonecroticfocus signal analogous to that of
fibrous tissue isnoted. Decreased signal is demonstrated onboth
T1WIs and T2WIs 34. University of PennsylvaniaSystem 35. To
determine the most appropriate treatment,consider the following
aspects: age of the patient, stage of the disease (early
orlate),location and amount of boneaffected (small or large
area),underlying causeof AVN (with ongoing causes such
ascorticosteroid or alcohol use, treatment may notwork unless use
of the substance is stopped) 36. Conservative management Restricted
weight-bearing Pharmacological agentslipid-lowering drugs,
anticoagulants,vasodilators, and bisphosphonates External,
biophysical, nonoperative modalitiesPulsed electromagnetic field
stimulationExtracorporeal shockwave therapyhyperbaric oxygen (HBO)
37. Restricted weight-bearing Advised with the expectation of
preventing femoralhead collapse during the healing Only 5 studies
with reference to weight bearing astreatment modality Factors
related to resolution : early, asymptomaticdisease (ARCO stage I)
and small lesion size (amodified index of necrotic extent of <
25). Hernigou et al, observed that clinical andradiographic signs
of the disease in asymptomatichips with a very small asymptomatic
lesion progressmore slowly than do signs in hips with a
largesymptomatic stage-II lesion 38. Agarwal et al studied 60
patients with AVN of the hip (100 hips ). Allpatients were treated
with alendronate 10 mg/day (or 70 mg/week)along with 500-1000 mg of
daily calcium and vitamin D supplements,and were advised to avoid
weight-bearing. NSAIDs and analgesicswere permitted as needed and
were recorded. CONCLUSION: Alendronate reduces pain, improves
function and retards AVNprogression. Early surgical intervention
can be avoided in mostpatients.Rheumatology (Oxford) 2005 Efficacy
of alendronate, a bisphosphonate, in the treatment of AVN ofthe
hip. A prospective open-label study. Agarwala S, Jain D Joshi
VR,Sule A P. D. Hinduja Hospital, Mahim, Mumbai 400 016, India. 39.
Operative intervention 1. Core decompression 2. Core decompression
with bone graftingPhemister type fibular graftingCancellous iliac
bone graftingMeyers Quardatus femoris muscle graftingSartorious
muscle pedicle graftingTensor fascia lata pedicle graftingGluteus
medius pedicle graftingVascularized muscle pedicle bone grafting
40. 3. Osteotomy 4. Surface arthroplasty 5. Total hip arthroplasty
41. Core decompression 2 methods of core decompression:
large-diameter trephines and small-diameter drills. Themost common
method, the 8 to 10-mmtrephine, is completed under fluoroscopy
withthe core track either being left open or filled inwith bone
graft 42. Complications e.g., articular cartilage damageand
subchondral fractures associated with thelarge-diameter technique,
Kim et al. developed the multiple small-diameter core decompression
technique. In their initial cohort of patients treated with
thistechnique, they reported a lower rate ofcollapse (14.3%) as
compared with the ratereported with the traditional trephine method
Kim SY, Kim DH, Park IH, Park BC, Kim PT, Ihn JC. Multiple drilling
compared withstandard core decompression for the treatment of
osteonecrosis of the femoralhead [abstract]. J Bone Joint Surg Br.
2004; 43. After core decompression 44. Stulberg et al. compared
core decompressionalone with conservative treatment in
aprospective, randomized study of 55hips. Onthe basis of Harris hip
scores, operativetreatment was successful in approximately 70%of
hips with Ficat Stage-I, II, or III osteonecrosis. Incontrast,
nonoperative treatment was successfulfor 20% of hips with Ficat
Stage-I disease, 0% withStage-II,and 10% with Stage-III Stulberg
BN, Davis AW, Bayer TW, Levine M,Easley K. Osteonecrosis of the
femoral head.Aprospective randomized treatment protocol Clin
Orthop. 45. Smith et al. reviewed twelve articles, publishedbetween
1979 and 1991, that included a total of702 hips with an average
duration of followup ofthirty-eight months. Using the University
ofPennsylvania staging system, they reported asuccessful result in
78% of the Ficat Stage-I hips,62% of the Stage-II hips, and 41% of
the Stage- IIIhips. Smith SW, Fehring TK, Griffin WL, Beaver
WB.Core decompression of theosteonecrotic femoral head. J Bone
Joint Surg Am 46. USE OF OSTEOINDUCTIVE SUBSTANCES ALONGWITH CORE
DECOMPRESSION 47. Mont et al used a modified trapdoor techniqueand
bone morphogenetic protein enriched bonegraft substitute through a
window at the femoralhead-neck junction in 23 patients. Successful
clinical results (a Harris hip score of 80points or greater and no
additional procedures) in18 of 21 hips (86%) at a minimum follow up
of 36months (mean, 48 months; range, 3655 months) Extensive
dissection required and, technically moredifficult than a standard
core decompression Mont MA, Etienne G, Ragland PS. Outcome of
nonvascularized bone graftingfor osteonecrosis of the femoral head.
Clin Orthop Relat Res. 2003 48. Lieberman et all retrospectively
evaluated 15 patients (17 hips) withAVN hip treated with core
decompression combined with anallogeneic, antigen-extracted,
autolyzed fibula allograft and 50 mgof partially purified human
bone morphogenetic protein andnoncollagenous proteins Clinical
success in 14 of 15 hips (93%; 13 patients) with Stage IIAdisease.
3 of 17 hips had radiographic progress and converted to total
hipreplacements. Only 1of seven hips with 50% or less involvement
of the femoral headdeveloped radiographic progression of the
femoral head No radiographic progression in the 3 hips with less
than 1/3involvement of the weight bearing surface of the femoral
head. Concluded further evaluation of the potential efficacy of
bonemorphogenetic protein required in randomized trials.Treatment
of osteonecrosis of the femoral head with core decompression and
human bone morphogenetic protein.Lieberman JR 49. Mesenchymal stem
cells (MSC) from adult bonemarrow are multipotent that can
differentiateinto fibroblastic, osteogenic, myogenic,adipogenic and
reticular cells.These cells mayalso provide a potential therapy for
bone repair Procedure of autologous stem celltransplantation has
been standardized with theguidelines that these should be instilled
inconcentration of 2X106 stem cells in non-traumatic pre-collapse
stage of avascularnecrosis femur head. 50. Effectiveness of bone
marrow mononuclear cellsrelated to the availability of stem cells
endowedwith osteogenic properties Injected marrow stromal cells
secrete angiogeniccytokines, resulting in increased angiogenesis
Bone marrow contains the bone morphogeneticproteins such as BMP-2
Supplementation of bone marrow stromal cellscultures with FGF-2
resulted in prolonged lifespan ofbone marrow stromal cells to more
than 70doublings and maintained their differentiationpotential
accompanied by an increase of theirtelomerase size 51. Yan et al
treated 44 hips in 28 patients with AVN at early stageby
percutaneous multiple holes decompression followed byautologous
BMCs infusion. Autologous BMCs wereconcentrated from bone marrow
that was taken from theposterior iliac crest of the patient.
Patients were followed up atleast 2 years. The results were
determined by the changes inthe Harris hip score and the
progression in the radiograghicstages. They concluded ercutaneous
multiple holes decompressioncombined with autologous BMCs is a new
way to treatavascular necrosis of the femoral head. Treatment of
osteonecrosis of the femoral head by percutaneousdecompression and
autologous bone marrow mononuclear cell infusion.Yan ZQ, Chen YSLi
, Yang Y Huo JZ Chen ZR Shi JHGe JB Source Department
ofOrthopaedics, Zhongshan Hospital of Fudan University, Shanghai
200032,China. [email protected] 52. Valerie et al studied
the implantation of autologous bone-marrow mononuclear cells in a
necrotic lesion of the femoralhead along with core decompression.
After twenty-four months, significant reduction in pain (p =0.021)
and in joint symptoms within the bone-marrow-graftgroup
Implantation of autologous bone-marrow mononuclear cellsappears to
be a safe and effective treatment for early stagesof osteonecrosis
of the femoral head. Treatment of Osteonecrosis of the Femoral Head
with Implantation of Autologous Bone-Marrow CellsValrie Gangji,
MD1; Jean-Philippe Hauzeur, MD, PhD J Bone Joint Surg Am. 2005 53.
Deltro et al, published their experience in 8 patientswhere they
assessed the efficacy and safety ofautologous bone-marrow
mononuclear cells (BMMC)implantation in necrotic lesions of the
femoral head inpatients with sickle cell disease. After 8 months, 7
of the eight patients reportedimprovement from symptoms Concluded
autologous bone-marrow mononuclear cellsimplantation is a safe and
effective treatment for earlystages of femoral head osteonecrosis
in patients withsickle cell disease Daltro GC, Fortuna VA, Salvino
de Arajo SA, FerrazLessa PI, SobrinhoUA, Borojevic R. Femoral head
necrosis treatment with autologousstem cells in sickle cell
disease. Acta Orthop Bras. 2008; 54. Use of a tantalum implant
reported in 2 studies Tantalum is a light metal that has a high
yield to stress. Inthese studies, porous tantalum rods used to
potentiallyallow bone growth to occur while providing support.While
the short-term results in these studies comparedfavorably to other
core decompression techniqueslonger follow-up is needed to more
fully assess theefficacy of this procedure. Tsao AK, Roberson JR,
Christie MJ, Dore DD, Heck DA, Robertson DD, Poggie
RA.Biomechanical and clinical evaluations of a porous tantalum
implant for thetreatment of early-stage osteonecrosis. J Bone Joint
Surg Am. 2005;87 Suppl 2: 22-7.8722 2005 Veillette CJ, Mehdian H,
Schemitsch EH, McKee MD. Survivorship analysis andradiographic
outcome following tantalum rod insertion for osteonecrosis of
thefemoral head. J Bone Joint Surg Am. 2006;88 Suppl 3: 48-55.8848
2006 55. Bone-grafting procedures can be divided intotwo general
categories: non-vascularized andvascularized 56. 3 approaches to
introduce bone graft into thefemoral head a core tract window in
the femoral neck (a lightbulbprocedure) a trapdoor made through the
articularcartilage in the femoral head 57. Cortical strut-grafting,
a procedure popularizedby Phemister, Boettcher et al., and
Bonfiglio etal. not commonly used today Technique involves the
removal of an 8 to 10-mm-diameter cylindrical core of bone from
thefemoral head and neck. This core tract is thenfilled with
cortical strut grafts harvested from theilium,fibula, or tibia.
Postoperatively,protected weight-bearing forthree to six months 58.
Grafting using an intact fibular allograft 59. Lightbulb procedure
The term lightbulb procedure introduced byRosenwasser et al.
Cortical window lifted from the femoral head-neckjunction,
cancellous bone graft from the iliac crestused to fill the defect
in the femoral head aftercomplete evacuationof the necrotic bone.
In their series, thirteen of fifteen hips wereasymptomatic at a
mean of twelve years (range,ten to fifteen years) Rosenwasser MP,
Garino JP, Kiernan HA, MichelsenCB. Long termfollowup of thorough
debridement and cancellous bone graftingofthe femoral head for
avascular necrosis. ClinOrthop. 1994 60. Trapdoor 61. Muscle
pedicle grafting 62. Meyers (1978) reported that fresh
autologousiliac bone chips combined with a muscle-pedicle bone
graft gave good results in stages 1and 2 necrosis, but was
unsatisfactory in stages3 and 4. 63. Technique for performing
muscle-pedicle bonegrafting to the femoral head, modified after
Meyerset al 64. Baksi(1991) reported his results at 3 to 12
years(mean, 7 years) follow-up in treating 61 patients(68 hips)
with a variety of muscle pedicle bonegrafts. Tensor fascia lata
anteriorly and the quadratusfemoris posteriorly preferred. As many
as 83% of the patients, obtained goodor excellent results at
follow-up.Baksi DP. Treatment of osteonecrosis of the femoral head
by drilling andmuscle-pedicle bone grafting. J Bone Joint Surg Br.
1991; 65. Vascularized fibular grafting 66. The rationale for
management of osteonecrosis ofthe femoral head with a free
vascularized fibulargraft based on five principles: (1)
decompression of the femoral head, (2) removal of the necrotic
bone, (3) replacement with fresh autogenous cancellousbone, (4)
support of the subchondral bone with a viable strong bone strut,
(5) revascularization and osteogenesis of thefemoral head. 67.
INDICATIONS: Symptomatic patients younger than fifty years ofage
with stage- II, III, or IV Patients younger than 20 of age who
havestage-V disease and a good range of motion ofthe hip 68. A
15-cm incision is made on the lateral aspect of the leg between
thelateral and posteriorcompartments. The incision is begun 10 cm
distal to the fibular head (PF)and ends10 cm proximal to the tip of
the lateral malleolus (LM). 69. The yellow arrow is pointing to the
anterior intermuscular septum. The black arrow ispointing to the
fibula, on which a small cuff of muscle and periosteum has
beenpreservedthe so-called marbleizing technique 70. The
interosseous membrane (IOM) is divided with a specially
designedright-angle Beaverblade (white arrow). The close proximity
of the deep peroneal nerve andanterior tibial artery(black arrow)
can be seen in this photograph 71. The fibular osteotomy is
performed once the pediclehas been isolated distally and
proximallyand protected with malleable retractors 72. The proximal
stump of the peroneal artery is ligated with the hemostaticclips
(arrow) justas it branches from the posterior tibial artery,
ensuring at least a 4 to 5-cmpedicle 73. Cancellous bone harvested
from the greater trochantericarea is inserted into the cavity
formedby removal of the necrotic bone. The fibulargraft is inserted
into the core tract and stabilizedwith a 0.62-mm Kirschner wire
(K). Theperoneal veins and artery are anastomosed tothe ascending
branches of the lateral femoralcircumflex artery (LFCA) and vein
74. Urbaniak reviewed the results in 1523 hips treated with a
freevascularizedfibular graft for osteonecrosis between 1979 and
October1, 2000 Best results obtained in the patients who had had no
collapse of thesubchondral bone or articularcartilage
preoperatively. Of the hips that had not had preoperative
subchondral or articularcollapse, 91% had a successful result after
six months to twenty-twoyears of follow-up. If collapse had been
present, the success rate was 85%, and if therehad also been
joint-space narrowing, it was 65% Urbaniak JR, Coogan PG, Gunneson
EB, Hunley JA. Treatment of osteonecrosis of thefemoral head with
free vascularized fibular grafting. A long-term follow-up study of
onehundred and three hips. J Bone Joint SurgAm. 1995 75.
Vascularized iliac crestgrafting 76. OSTEOTOMY To rotate the
necrotic or collapsing segment ofthe hip out of the weight bearing
zone,replacing it with a segment of articular cartilageof the
femoral head supported by healthyviable bone. In addition to the
biomechanical effect,osteotomy reduce venous hypertension
anddecrease intramedullary pressure. 77. Utilized for both pre- and
postcollapse lesions, butnot be performed if there is acetabular
involvement Work best when the lesions are small or mediumsized
with a combined necrotic angle of less than200 or with less than
30% of femoral headinvolvement. For varus osteotomies, there should
be at least 20 ofthe superolateral femoral head not involved
withdisease, because this area of cartilage will beshifted into
weight bearing after the osteotomy. 78. Valgus osteotomy requires
normal bone andcartilage in the central or medial aspect of
thehead. Extension can be added when the necroticsegment is
posterior Flexion can be added if the lesion is anterior 79. The
angular measurements of the lesion on theAP and lateral radiographs
are added togetherto give the combined necrotic angle,as described
by Kerboul et al. (From Kerboul M,Thomine J, Postel M, Merle
DAubign R. TheConservative Surgical Treatment of IdiopathicAseptic
Necrosis of the Femoral Head. J BoneJoint Surg Br 1974 80.
Radiographs of a hip that underwent a varusosteotomy for
osteonecrosis 81. Rotational osteotomy indicated in early
tointermediate stages in which the acetabularcartilage is
relatively unaffected Must be sufficient normal bone and cartilage
inthe femoral head so that after rotation theintact segment
occupies at least 36% of theweight-bearing surface of the
acetabulum. Contraindications include whole-head
necrosis,significant degenerative changes in the femoralhead or
acetabulum, and poor general health 82. Rotational Osteotomies In
1973, Sugioka reported transtrochantericanterior rotation osteotomy
More than 500 of these procedures wereperformed since 1972, and
Sugiokas results,especially in hips treated before
significantfemoral head collapse, were quite gratifying
Unfortunately, these results could not beconsistently duplicated by
other investigators 83. Schematic of the Sugioka
transtrochantericrotational osteotomy of the femoral head. 84.
Transposition of necrotic focus of femoral head
anteroinferiorlyaway from weight-bearing area as a result of
anterior rotation ofthe femoral head. (A) before rotation and (B)
after rotation. (FromSugioka Y, Mohtai M. Osteonecrosis of the
Femoral Head 85. Zhang et alExperimentenly injected intravenous
bonemarrow mesenchymal cells in rabbit and resultsrevealed
intravenously implanted MSCs couldmigrate into the femoral head of
hosts, andespecially migrate directionally and survive in
thenecrotic femoral heads. Thus, it is feasible andsafe to treat
femoral head necrosis by intravenoustransplantation of allogeneic
MSCs Intravenous transplantation of allogeneic bone marrow
mesenchymal stemcells and its directional migration to the necrotic
femoral head Zhang-hua LiInternational Journal of Medical Sciences
2011 86. Total hip replacement is recommended forpatients over the
age of fifty years who haveany degree of symptomatic osteonecrosis
orpatients over the age of forty years who haveadvancedstage-IV
disease or involvement of>50% of the femoral head with limited
hipmotion.